
Abstract
Corneal endothelium plays an important role in maintaining hydration homeostasis and clarity of the cornea. Fuchs endothelial corneal dystrophy (FECD) affects the corneal endothelium resulting in edema and characteristic excrescences on the Descemet’s membrane known as corneal guttae. Descemet membrane endothelial keratoplasty (DMEK) has evolved to become the standard of care for patients with FECD with excellent visual acuity outcomes. Patients with FECD may have coexisting cataracts and therefore may require a cataract surgery, which increases the risk of corneal decompensation. The presence of FECD may not only influence the choice of intraocular lens but vision outcomes can also be affected by the corneal condition. The ability to combine the surgeries further raises important considerations regarding the timing and sequence of DMEK and cataract extraction for patients with FECD. This review provides a guide for corneal surgeons in choosing between endothelial keratoplasty and cataract surgery—alone, in combination or sequential—in their management of patients with FECD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Fuchs endothelial corneal dystrophy (FECD) affects the corneal endothelium resulting in decreased vision. |
While newer therapeutic options are being investigated, Descemet membrane endothelial keratoplasty (DMEK), which involves replacing the diseased corneal endothelium and Descemet membrane with healthy donor endothelium and Descemet membrane, is the current standard therapeutic option for patients with FECD. |
Patients with FECD may have co-existing cataracts, and both conditions have varying effects on their vision. |
Corneal surgeons’ factor in clinical history, examination, diagnostic tests (e.g., corneal tomography, specular and pachymetry), practice patterns and patient preference to make the decision of offering endothelial keratoplasty and cataract surgery—alone, in combination or sequential. |
A review of the current literature will help corneal surgeons navigate this decision. |
Digital Features
This article is published with digital features, including videos, to facilitate understanding of the article. To view digital features for this article go to https://doi.org/10.6084/m9.figshare.21691958.
Introduction
Fuchs endothelial corneal dystrophy (FECD) was first described more than a century ago in 1910 by Austrian ophthalmologist Ernst Fuchs. He initially called it dystrophia epithelialis corneae because of the epithelial bullae seen in advanced stages of the disease, but it was later realized that the condition primarily affects the corneal endothelium with the characteristic excrescences on Descemet’s membrane known as corneal guttae. The attrition rate of corneal endothelium becomes accelerated in cases of FECD with resulting corneal edema [1, 2]. Currently, approximately 300 million people over the age of 30 years are estimated to be affected by FECD across the globe, and the number is projected to increase to 415 million by 2050 [3]. FECD is usually an inherited condition with a female predilection. FECD may have an early or late onset with a complex interplay of multiple genes [4,5,6]. Epidemiological data on FECD suggest that it also preferentially affects middle-aged individuals and thus is coincident with the time when patients develop cataracts and require cataract surgery. Cataract surgery in turn can result in corneal decompensation in patients with FECD and thus must be approached with care. This review aims to evaluate the most recent management strategies for patients with both FECD and cataracts. This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Evaluation of Patients With FECD
Clinical Presentation of FECD
The diagnosis of FECD is made primarily based on clinical findings and history. The progression of the disease is bilateral but may be asymmetric with four clinical stages over 2 to 3 decades [7]. The first stage is characterized by the hallmark finding of non-confluent corneal guttae, which can be noted on slit-lamp examination. Historically, the Krachmer scale has also been used to clinically grade FECD severity [8]. Krachmer grading is based on central corneal guttae density seen on slit-lamp imaging with specular reflection and retro imaging. It ranges from G0 to G4 + edema with G4 + edema being most severe with central confluent guttae > 5 mm and stromal or epithelial edema. While it has been thought that patients generally have no complaints in the early stages, recent studies suggest that patients may have a lot of glare and color vision defects even in mild stages [9]. Stage two is characterized by confluent guttae with endothelial cell polymegathism, pleomorphism and loss. Patients may report blurry vision particularly in the morning and glare. In stage 3, the endothelial dysfunction results in edema, developing first in the stroma followed by the epithelium. Microcysts of corneal epithelial edema are seen on retro illumination, which later coalesces to form bullae. Patients frequently notice blurred vision, glare and halos. The bullae might rupture causing pain and foreign body sensation and predispose patients to infectious keratitis. The fourth stage consists of vascularization of corneal periphery and formation of subepithelial pannus, scarring and opacification, thereby worsening patient’s vision.
Management of FECD
In early stages, FECD can be observed. However, many patients will develop visual impairment with progression of the disease. Currently, no medical therapy is available to interfere with the progression of FECD. Hyperosmotic drops may temporarily improve symptoms in earlier stages. However, a recent randomized trial has revealed that the drops might not offer much benefit and might result in more adverse events compared to a placebo [10]. Netarsudil, a rho kinase inhibitor, is approved for treatment of glaucoma. Netarsudil was associated with reduction of corneal edema and improvement in scotopic corrected distance vision of FECD patients in a randomized clinical trial on 26 eyes [11]. However, currently for more advanced disease keratoplasty is the main modality for treatment [12].
Evolution of Keratoplasty and Rising Numbers of DMEK
For over a century penetrating keratoplasty (PK) was the main treatment option for FECD [12]. However, the surgical management has evolved from PK to endothelial keratoplasty (EK) beginning with deep lamellar endothelial keratoplasty (DLEK), then Descemet stripping (Automated) endothelial keratoplasty (DSEK/DSAEK) and most recently Descemet membrane endothelial keratoplasty (DMEK) over the past 2 decades. Figure 1 shows the overall rates of different types of keratoplasties in the US according to Eye Bank Association of America (EBAA) in which DMEK numbers are approaching DSAEK numbers [13].

Overall trends of different types of keratoplasty in the US from 2014 to 2021 using EBAA data PK: Penetrating Keratoplasty; DSAEK: Descemet Stripping (Automated) Endothelial Keratoplasty; DLEK: Deep Lamellar Endothelial Keratoplasty; DMEK: Descemet Membrane Endothelial Keratoplasty
While DSEK involves the replacement of the host Descemet membrane (DM) and endothelial cell (EC) layer with a donor lenticule composed of stroma, DM and EC, DMEK is the anatomically correct replacement of host DM and EC with donor DM and EC without additional stroma [14]. The treatment of endothelial cell disorder may ultimately evolve to Descemet’s stripping only (DSO) or cell-based therapies, but currently, EK remains the standard of care [6, 15] (Fig. 2).

Schematic explaining different types of keratoplasty and Descemet stripping only
In 2021, FECD resulted in 35.8% (n = 16,780) of the total keratoplasties in the US and thus remained the number one indication for corneal transplant for the 9th consecutive year [13]; 94.5% of these patients were treated with EK and 5.5% with PK. Similarly, a study from the European Cornea and Cell Transplantation Registry and Australian graft registry 2021–2022 report shows FECD to be the most common and second most common indication for keratoplasty, respectively. EK was the most common treatment modality for FECD in both of these regions with most patients receiving DSAEK followed by DMEK [16, 17]. In general, the improved visual acuity outcomes and lower risk of EK surgery compared to PK have changed the threshold for offering keratoplasty to patients with FECD and a shift in approach to cataract surgery in eyes with FECD.
Surgical Decision Making
Distinguishing the Cause of Vision Loss
When evaluating a patient with both cataract and FECD, it is important to recognize the corneal condition and counsel patients to expect slower visual recovery and possible corneal decompensation that might necessitate a future endothelial transplant or determine if a concurrent EK (triple procedure) would be indicated. The first step in deciding whether to consider a triple procedure is to try to determine if the cause of vision loss is cataract or the corneal disease (Fig. 3). This determination includes assessment of patient history, slit-lamp examination and diagnostic testing. The symptoms of glare, blurry vision and decreased contrast sensitivity may be overlapping between the two, and are often not adequate for distinguishing between FECD and cataract. However, cataracts may additionally be associated with a myopic shift [18]. On the other hand, FECD patients may report blurry vision upon awakening, which improves with deturgescence of the cornea, or foreign body sensation and pain if bullae are present [19]. Slit-lamp examination is important in assessing the stage and density of the cataract, depth of the anterior chamber and also presence of clinically evident corneal edema.

Algorithm describing an approach to Fuchs endothelial corneal dystrophy (FECD) with cataract
Diagnostic testing can be particularly helpful in evaluating patients without clinically evident edema by detecting subclinical edema and identifying eyes that would be higher risk for corneal decompensation. Typically, an endothelial cell density (ECD) of 500/mm2 is required to maintain corneal clarity, and eyes with EC counts < 1000 are more likely to decompensate [20]. However, the cell counts can be difficult to accurately measure in eyes with FECD, and cell counts do not adequately assess function [21]. Seitzman et al. suggested using preoperative pachymetry measurements of > 640 µm to predict the need for PK [22]. They used data from 1990 to 2002 to reach this conclusion, a time when PK used to be the most performed surgery in patients with FECD. This is based on the concept that an increase in central corneal thickness (CCT) occurs with increasing severity of FECD [23]. However, this approach may miss subclinical corneal edema since absolute pachymetry cut-offs do not account for variation in baseline thickness.
In a series of studies, Patel and colleagues have delineated tomographic findings on scheimpflug imaging that can be used to detect subclinical edema [24, 25]. Three features including the irregular isopachs, displacement of the thinnest point of the cornea and obvious focal posterior surface depression can be indicative of subclinical edema in eyes with FECD. They found that eyes with no feature, one to two features and all three features had 7%, 48% and 89% 5-year risk of disease progression. Thus, the use of tomography can help predict which eyes may not benefit from cataract surgery alone or have a higher risk of needing EK in the future. More recently, Arnalich-Montiel et al. used a combination of CCT values and the three tomographic features described above to estimate the risk of needing EK after uncomplicated phacoemulsification in patients with FECD [26]. Their model generated a score out of 8, and the cumulative risk for EK within 2 years of an uncomplicated phacoemulsification ranged from minimal risk ranging from 0.8 to 7.5% for scores < 4 to 96.5% for those with a score of 8.
In a study involving 89 eyes, Cleynenbreugel et al. reported that backscatter at the basal epithelial cell layer measured using in vivo confocal microscopy represents the hydration status of the cornea and therefore may predict the need for EK after cataract surgery. This information may be used to offer combined surgery to these patients; however, confocal microscopy may not be widely available [27]. Using a multivariable model which included preoperative best-corrected visual acuity, CCT, pachymetry readings, anterior chamber depth, backscatter variables derived from scheimpflug imaging and ECD, Arnalich-Montiel et al. reported that anterior layer corneal backscatter values between 0 and 2 mm from the apex and relative increase in CCT using pentacam were significant predictors of EK in patients with FECD [28]. They used their findings to create a RISC (Relative Increase in corneal thickness in the relative pachymetry map and anterior corneal backSCatter) score that included these two variables and had a sensitivity of 96% along with a specificity of 95%. Moreover, they modified the RISC score by removing the backscatter data from the model to create a RIPT (Relative Increase in corneal thickness in the relative pachymetry map and Pupillary corneal Thickness) score. The model performed similarly to the RISC score with corneal thickness at the pupil center by pentacam and relative increase in CCT as significant predictors of EK. Thus, the use of corneal tomography has become increasingly useful in the evaluation of FECD patients.
Phakic DMEK
For young patients with significant FECD, but without a cataract, phakic DMEK might be the preferred approach. In a case series of 1000 eyes (25.6%, 256 phakic) with 85.3% (n = 853) carrying a diagnosis of FECD, Birbal et al. found that the patient’s lens status did not influence DMEK outcomes [29]. Corneal surgeons may be apprehensive about damaging the cornea during a subsequent cataract surgery. However, recent studies show that a subsequent cataract extraction is feasible with minimal EC loss if performed carefully in patients with a DMEK graft [30,31,32,33]. Additionally, the 5-year phacoemulsification rate among FECD patients undergoing phakic DMEK with no cataract is reported to be just 16.9% [34]. It is therefore preferable to preserve the lens of young patients with accommodative power without a cataract. (See video 1 in the online/HTML version of the manuscript or follow the digital features link under the abstract.)
Video 1: Video demonstrating a Descemet membrane endothelial keratoplasty procedure in a phakic eye
Cataract Surgery Alone in FECD
For patients with a visually significant cataract, but without evidence of sub-clinical FECD edema, cataract surgery alone is preferred. In addition, early cataract surgery may be preferred since the increased ultrasound energy needed to remove a dense cataract may result in greater endothelial damage. Surgical techniques to reduce EC loss such as tri-soft shell technique (TSST), Phaco-Chop technique and low-flow irrigation may be considered. TSST uses a thin dispersive ophthalmic viscosurgical device (OVD) shell to protect the corneal endothelium [35]. Phaco-Chop uses the oscillatory handpiece to break up the lens nucleus mechanically to reduce the ultrasonic energy needed [36, 37]. Use of low-flow irrigation has also been found to be effective in reducing EC loss [35, 38]. In terms of intraocular lens (IOL) selection, hydrophobic IOLs are preferred if a future EK is anticipated because of the risk of opacification of hydrophilic IOLs [39]. In a retrospective review of 94 eyes, Chuckpaiwong et al. found that only intraoperative complications were significantly associated with corneal endothelial failure in patients with FECD who underwent phacoemulsification [31]. Therefore, in addition to preoperative risk assessment, efforts to reduce intraoperative complications during cataract surgery are also important to reduce the risk of corneal decompensation.
Cataract Surgery and DMEK in FECD—Triple vs. Sequential Procedure
For patients with both a visually significant cataract and FECD, either a DMEK triple procedure or a staged procedure can be considered. The DMEK triple procedure provides rapid visual recovery and limits the risks and costs associated with two separate procedures. A study looking at 203 eyes reported that the rates of graft dislocation after triple DMEK remain low with no graft failure at 6 months [40]. Visual outcomes, EC loss and rebubbling rates remain comparable between DMEK triple and staged procedures [41, 42]. Shahnazaryan et al. reported that while rates of rebubbling remained low with good visual outcomes, the rates of EC loss at 1 month and 1 year were higher after DMEK triple compared with DMEK alone [43]. Thus, the mixed results in the literature suggest that the decision to perform a staged versus combined procedure should be based on surgeon experience. Analysis of the Intelligent Research in Sight (IRIS) registry found that patients with a history of glaucoma or glaucoma surgery have higher odds of repeat keratoplasty [44]. A retrospective study on 108 DMEK cases reported that eyes with prior trabeculectomy and drainage device may result in very good short-term outcomes [45]. Another comparative case series on 94 eyes of 91 patients who underwent DMEK found that while patients with a history of glaucoma surgery have good early outcomes, longer-term rejection and failure rates are high with a 2-year graft survival probability of only 27% [46]. Thus, patients may be counselled regarding post-surgical prognosis that is tailored to their ocular comorbidities. Other practical considerations including patient preference and financial consideration for reimbursements particularly at ambulatory surgery centers or practice referral patterns may also influence the decision to do staged versus combined surgery.
Surgical modifications when performing a combined procedure include avoiding the use of dilating agents in the irrigation fluid so that the pupil can be constricted during the DMEK. A smaller rhexis that covers the optic edge will improve IOL stability during subsequent manipulation during the keratoplasty. It is important to avoid rupture of the posterior capsule to avoid vitreous loss and enable placement of the IOL in the capsular bag. Finally, the viscoelastic should be carefully removed before graft insertion and using cohesive viscoelastic instead of dispersive may reduce the chances of inadvertent retention of viscoelastic in the interface, which may reduce graft attachment. Surgeons may use either pre-loaded or surgeon-loaded corneal grafts while performing DMEK. A study comparing 200 pre-loaded vs. 200 surgeon-loaded corneal grafts reported comparable outcomes [47]. (See video 2 in the online/HTML version of the manuscript or follow the digital features link under the abstract.)
Video 2: Video showing a combined Descemet membrane endothelial keratoplasty, cataract extraction and intraocular lens insertion procedure
Recent Advancements
Femtosecond Laser-Assisted Cataract Surgery (FLACS)
FLACS has been theorized to reduce corneal damage when making an incision for cataract surgery in patients with Fuchs. However, studies have shown mixed results for patients who underwent FLACS. Koo et al. found no difference in the refractive outcomes for eyes that underwent FLACS compared to the eyes that underwent conventional phacoemulsification [48]. Yong et al. found that FLACS was superior to conventional phacoemulsification in terms of reducing postoperative EC loss especially in patients with moderate-to-dense cataracts [49]. Einan et al. reported that while the best-corrected visual acuity (BCVA) and EC loss were comparable between FLACS and conventional phacoemulsification, eyes that underwent FLACS and DMEK had less graft detachment along with a reduced need for rebubbling [50]. Similar results were reported by another study, which found that FLACS and DMEK had lower detachment, rebubble and cell loss rates compared to conventional phacoemulsification [51].
Refractive Outcomes
A hyperopic shift is seen after DMEK in eyes affected by FECD. This could be explained by the fact that the posterior corneal power decreases (becomes less negative) in later stages of FECD. Moreover, relatively greater horizontal than vertical corneal thickening seen in later stages of FECD can affect posterior toricity. These changes can affect the choice of IOL [52]. Thus, surgeons can purposefully err in the myopic direction during combined cataract surgery and DMEK or when a DMEK is anticipated in the future. A study by Wacker et al. suggests that surgeons should aim similarly in eyes affected by FECD even when DMEK is not anticipated [52]. They found that the mean arithmetic error (the difference between the stable postoperative and the predicted refractive errors) was more hyperopic by 0.25 D in mild FECD, 0.34 D in moderate FECD and 0.37 D in advanced FECD compared with control eyes after phacoemulsification. A study by Campbell et al. compared the outcomes of multiple formulae in DMEK triple cases and found that all of the formulae studied other than the Haigis formula resulted in a hyperopic error [53]. Another study looking at 254 eyes of 127 patients found that the refractive error in the fellow eye that underwent combined DMEK and cataract surgery later followed the refractive shift in the eye that underwent the combined surgery first. They concluded that the refractive shift in the first eye could serve as a reference to optimize refractive outcomes in the second eye [54].
Premium IOLs: Toric, Extended Depth of Focus (EDOF) and Multifocal
Given the improvement in visual acuity outcomes of DMEK, there is greater interest in improving refractive outcomes with greater spectacle independence for patients with FECD undergoing cataract surgery with or without DMEK. However, any of the premium lenses must be used with caution because it is important to recognize that corneal edema and bullae may induce irregular astigmatism and affect keratometry measurements. Similarly, presbyopia-correcting lenses may not provide acceptable visual acuity outcomes in the setting of corneal guttae.
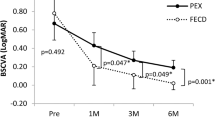
Recently, there have been several small reports on outcomes of toric lenses in patients with FECD who underwent a combined procedure. In a study on four eyes that underwent DMEK triple procedure and toric IOL implant, a decrease in manifest refractive cylinder and improvement in uncorrected and best-corrected vision were seen in all cases [55]. Preoperative corneal astigmatism centroid was 1.72 D @ 2º ± 1.78 D, and 6 months postoperatively, it was 0.09 D @ 125º ± 0.53 D. The uncorrected distance visual acuity (LogMAR) improved from 0.73 ± 0.19 to 0.12 ± 0.04. In another study evaluating 15 eyes of 10 patients who underwent DMEK triple procedure with a toric IOL implant, refractive astigmatism improved significantly from 2.23 ± 1.10 D (range 0.75–4.25 D) preoperatively to 0.87 ± 0.75 D (range 0.00–3.00 D) postoperatively [56]. One of the eyes in this series had rotational misalignment of the toric IOL; therefore, care must be taken to prevent excessive IOL rotation.
The use of presbyopia-correcting IOLs in FECD patients has also been studied. A study by Price et al. reported favorable visual outcomes when cataract surgery and presbyopia-correcting IOL implantation, using either EDOF ± toric or bifocal, were staged after the DMEK [57]. DMEK surgery first helped in clearing corneal edema and resulted in more accurate biometry measurements for the subsequent cataract surgery. Another study looking at nine eyes of nine patients who underwent DMEK after a multifocal IOL implant reported favorable outcomes as well [58].
Light-adjustable IOLs enable postoperative titration in IOL power. In a case series of two patients, light-adjustable IOLs achieved a distance uncorrected visual acuity of 20/20 or better after a DMEK triple procedure [59]. The use of light-adjustable IOLs may be an opportunity to optimize refractive outcomes for FECD patients.
Emerging Treatments
While EK, with its excellent outcomes, remains the standard therapeutic option for patients with FECD, newer modalities are emerging and might be of interest in the near future. These therapies include DSO, rho-associated kinase inhibitor eye drops, synthetic DM transplant, injection cell therapy and gene therapy [6].
Diseased DM in FECD hinders the migration of healthy ECs in addition to scattering light because of the presence of guttae. DSO involves removing the diseased DM, thus allowing healthy ECs to migrate over the central cornea thereby reducing corneal edema. Studies on DSO have shown favorable clinical outcomes [15, 60,61,62]. However, in some cases DSO results in an environment that is not conducive to EC migration and may result in poor or delayed outcomes [63]. In such cases, a synthetic Descemet membrane made of biomimetic materials (e.g., hyaluronic acid hydrogels) may facilitate EC migration and resolution of corneal edema, as shown in rabbit models [64]. Moreover, rho-associated kinase inhibitors can further improve the EC function and can be used in conjunction with DSO with or without synthetic Descemet membrane. Clinical studies on the use of rho-associated kinase inhibitors have shown promising results [11, 65, 66].
DSO relies on healthy corneal ECs on the periphery of the diseased cornea. However, this might not be the case in more advanced FECD. Injection cell therapy via a cell carrier or an intra-cameral injection of laboratory-cultured ECs may prove to be helpful in such cases [67,68,69]. Success of injection cell therapy in preclinical studies represents an exciting opportunity to develop minimally invasive transplant options in the near future [70, 71]. Moreover, increasing understanding of the genes implicated in FECD and the advancement in gene editing tools, e.g., shortening trinucleotide repeats similar to those seen in FECD using CRISPR-Cas nucleases, presents an opportunity to use gene therapy in the treatment of FECD [72].
Conclusion and Summary
Given the high incidence of both FECD and cataracts, patients may present with varying stages of both conditions simultaneously. EK and cataract surgery remain the standard of care for these conditions, respectively. A diagnostic approach based on the patient’s history, clinical examination, and diagnostic modalities (e.g., corneal tomography, specular microscopy and pachymetry, etc.) may assist in differentiating the contribution of either diagnoses to the patient’s visual impairment. This may help corneal surgeons in choosing between EK and cataract surgery—alone, in combination or sequential—thereby optimizing management for these patients.
References
Bourne WM, Nelson LR, Hodge DO. Central corneal endothelial cell changes over a ten-year period. Invest Ophthalmol Vis Sci. 1997;38(3):779–82.
Edelhauser HF. The balance between corneal transparency and edema the proctor lecture. Invest Ophthalmol Vis Sci. 2006;47(5):1755–67. https://doi.org/10.1167/iovs.05-1139.
Aiello F, Gallo Afflitto G, Ceccarelli F, Cesareo M, Nucci C. Global prevalence of fuchs endothelial corneal dystrophy (FECD) in adult population: a systematic review and meta-analysis. J Ophthalmol. 2022. https://doi.org/10.1155/2022/3091695.
Eghrari AO, Riazuddin SA, Gottsch JD. Fuchs corneal dystrophy. Prog Mol Biol Transl Sci. 2015;134:79–97. https://doi.org/10.1016/bs.pmbts.2015.04.005.
Vedana G, Villarreal G, Jun AS. Fuchs endothelial corneal dystrophy: current perspectives. Clin Ophthalmol (Auckland, NZ). 2016;10:321–30. https://doi.org/10.2147/OPTH.S83467.
Soh YQ, Peh GSL, Mehta JS. Evolving therapies for Fuchs’ endothelial dystrophy. Regen Med. 2018;13(1):97–115. https://doi.org/10.2217/rme-2017-0081.
Mark J, Mannis EJH. Cornea-fundamentals, diagnosis and management. 5th ed. Elsevier-OHCE; 2021.
Krachmer JH, Purcell JJ, Young CW, Bucher KD. Corneal endothelial dystrophy. A study of 64 families. ArchOphthalmol (Chicago, Ill: 1960). 1978;96(11):2036–9. https://doi.org/10.1001/archopht.1978.03910060424004.
Watanabe SMD, Oie YMDP, Fujimoto HMDP, et al. Relationship between corneal guttae and quality of vision in patients with mild Fuchs’ endothelial corneal dystrophy. Ophthalmology (Rochester, Minn). 2015;122(10):2103–9. https://doi.org/10.1016/j.ophtha.2015.06.019.
Zander DB, Böhringer D, Fritz M, et al. Hyperosmolar eye drops for diurnal corneal edema in Fuchs’ endothelial dystrophy. Ophthalmology (Rochester, Minn). 2021;128(11):1527–33. https://doi.org/10.1016/j.ophtha.2021.04.015.
Price MO, Price FW. Randomized, double-masked, pilot study of netarsudil 0.02% ophthalmic solution for treatment of corneal edema in Fuchs dystrophy. Am J Ophthalmol. 2021;227:100–5. https://doi.org/10.1016/j.ajo.2021.03.006.
Güell JL, El Husseiny MA, Manero F, Gris O, Elies D. Historical review and update of surgical treatment for corneal endothelial diseases. Ophthalmol Therapy. 2014;3(1–2):1–15. https://doi.org/10.1007/s40123-014-0022-y.
Eye Bank Association of A. 2021 Eye Banking Statistical Report. 2022.
Dapena I, Ham L, Melles GRJ. Endothelial keratoplasty: DSEK/DSAEK or DMEK - the thinner the better? Curr Opin Ophthalmol. 2009;20(4):299–307. https://doi.org/10.1097/ICU.0b013e32832b8d18.
Garcerant D, Hirnschall N, Toalster N, Zhu M, Wen L, Moloney G. Descemetʼs stripping without endothelial keratoplasty. Curr Opin Ophthalmol. 2019;30(4):275–85. https://doi.org/10.1097/ICU.0000000000000579.
Dunker SL, Armitage WJ, Armitage M, et al. Practice patterns of corneal transplantation in Europe: first report by the European Cornea and Cell Transplantation Registry. J Cataract Refract Surg. 2021;47(7):865–9.
Keane M, Coffey N, Jones V, Lawson C, Mills R, Williams K. The Australian corneal graft registry: 2021/22 report. 2022;
Samarawickrama C, Wang JJ, Burlutsky G, Tan AG, Mitchell P. Nuclear cataract and myopic shift in refraction. Am J Ophthalmol. 2007;144(3):457–9. https://doi.org/10.1016/j.ajo.2007.05.003.
Fritz M, Grewing V, Maier P, et al. Diurnal variation in corneal edema in fuchs endothelial corneal dystrophy. Am J Ophthalmol. 2019;207:351–5. https://doi.org/10.1016/j.ajo.2019.08.002.
Joyce NC. Proliferative capacity of corneal endothelial cells. Exp Eye Res. 2012;95(1):16–23. https://doi.org/10.1016/j.exer.2011.08.014.
Seitz B, Hager T. Clinical phenotypes of Fuchs endothelial corneal dystrophy (FECD), disease progression, differential diagnosis, and medical therapy. In: Cursiefen C, Jun AS, editors. Current treatment options for fuchs endothelial dystrophy. Springer International Publishing; 2016. P. 25–50.
Seitzman GD, Gottsch JD, Stark WJ. Cataract surgery in patients with Fuchs’ corneal dystrophy: expanding recommendations for cataract surgery without simultaneous keratoplasty. Ophthalmology. 2005;112(3):441–6. https://doi.org/10.1016/j.ophtha.2004.10.044.
Kopplin LJ, Przepyszny K, Schmotzer B, et al. Relationship of Fuchs endothelial corneal dystrophy severity to central corneal thickness. Arch Ophthalmol (1960). 2012;130(4):433–9. https://doi.org/10.1001/archopthalmol.2011.1626.
Patel SV, Hodge DO, Treichel EJ, Spiegel MR, Baratz KH. Predicting the prognosis of fuchs endothelial corneal dystrophy by using Scheimpflug tomography. Ophthalmology (Rochester, Minn). 2020;127(3):315–23. https://doi.org/10.1016/j.ophtha.2019.09.033.
Sun SY, Wacker K, Baratz KH, Patel SV. Determining subclinical edema in fuchs endothelial corneal dystrophy: revised classification using Scheimpflug tomography for preoperative assessment. Ophthalmology (Rochester, Minn). 2019;126(2):195–204. https://doi.org/10.1016/j.ophtha.2018.07.005.
Arnalich-Montiel F, de de-Arriba-Palomero P, Muriel A, Mingo-Botín D. A risk prediction model for endothelial keratoplasty after uncomplicated cataract surgery in fuchs endothelial corneal dystrophy. Am J Ophthalmol. 2021;231:70–8. https://doi.org/10.1016/j.ajo.2021.04.016.
Van Cleynenbreugel HMD, Remeijer LMDP, Hillenaar TMDP. Cataract surgery in patients with Fuchs’ endothelial corneal dystrophy. Ophthalmology (Rochester, Minn). 2014;121(2):445–53. https://doi.org/10.1016/j.ophtha.2013.09.047.
Arnalich-Montiel F, Mingo-Botín D, De Arriba-Palomero P. Preoperative risk assessment for progression to descemet membrane endothelial keratoplasty following cataract surgery in fuchs endothelial corneal dystrophy. Am J Ophthalmol. 2019;208:76–86. https://doi.org/10.1016/j.ajo.2019.07.012.
Birbal RS, Baydoun L, Ham L, et al. Effect of surgical indication and preoperative lens status on descemet membrane endothelial keratoplasty outcomes. Am J Ophthalmol. 2020;212:79–87. https://doi.org/10.1016/j.ajo.2019.12.011.
Musa FUMBCF, Cabrerizo JMD, Quilendrino RMD, Dapena IMDP, Ham LP, Melles GRJMDP. Outcomes of phacoemulsification after Descemet membrane endothelial keratoplasty. J Cataract Refract Surg. 2013;39(6):836–40. https://doi.org/10.1016/j.jcrs.2012.12.032.
Burkhart ZNMD, Feng MTMD, Price FWMD, Price MOP. One-year outcomes in eyes remaining phakic after Descemet membrane endothelial keratoplasty. J Cataract Refract Surg. 2014;40(3):430–4. https://doi.org/10.1016/j.jcrs.2013.08.047.
Gundlach E, Maier AK-B, Tsangaridou M-A, et al. DMEK in phakic eyes: targeted therapy or highway to cataract surgery? Graefe’s Arch Clin Exp Ophthalmol. 2015;253(6):909–14. https://doi.org/10.1007/s00417-015-2956-8.
Siggel R, Heindl LM, Cursiefen C. Descemet membrane endothelial keratoplasty (DMEK) in phakic eyes with shallow anterior chamber. Graefes Arch Clin Exp Ophthalmol. 2014;253(5):817–9. https://doi.org/10.1007/s00417-014-2850-9.
Birbal R, Ni Dhubhghaill S, Bourgonje V, et al. Five-year graft survival and clinical outcomes of 500 consecutive cases after descemet membrane endothelial keratoplasty. Cornea. 2020;39(3):290–7. https://doi.org/10.1097/ICO.0000000000002120.
Arshinoff SAMDF, Norman RBM. Tri-soft shell technique. J Cataract Refract Surg. 2013;39(8):1196–203. https://doi.org/10.1016/j.jcrs.2013.06.011.
Seitzman G. Cataract surgery in Fuchsʼ dystrophy. Curr Opin Ophthalmol. 2005;16(4):241–5. https://doi.org/10.1097/01.icu.0000172828.39608.7c.
Traish AS, Colby KA. Approaching cataract surgery in patients with fuchs’ endothelial dystrophy. Int Ophthalmol Clin. 2010;50(1):1–11. https://doi.org/10.1097/IIO.0b013e3181c5728f.
Kaup S, Pandey SK. Cataract surgery in patients with Fuchs’ endothelial corneal dystrophy. Community Eye Health J. 2019;31(104):86–7.
Mojzis PMDPF, Studeny PMDP, Werner LMDP, Piñero DPP. Opacification of a hydrophilic acrylic intraocular lens with a hydrophobic surface after air injection in Descemet-stripping automated endothelial keratoplasty in a patient with Fuchs dystrophy. J Cataract Refract Surg. 2016;42(3):485–8. https://doi.org/10.1016/j.jcrs.2016.02.004.
Terry MA, Shamie N, Chen ES, et al. Endothelial keratoplasty for Fuchs’ dystrophy with cataract: complications and clinical results with the new triple procedure. Ophthalmology. 2009;116(4):631–9. https://doi.org/10.1016/j.ophtha.2008.11.004.
Hussien A, Elmassry A, Ghaith A, Goweida M. Descemet’s membrane endothelial keratoplasty and phacoemulsification: combined versus sequential surgery. J Curr ophthalmol. 2021;33(3):277–84. https://doi.org/10.4103/joco.joco_188_20.
Tey KY, Tan SY, Ting DSJ, Mehta JS, Ang M. Effects of combined cataract surgery on outcomes of descemet’s membrane endothelial keratoplasty: a systematic review and meta-analysis. Front Med. 2022;9: 857200. https://doi.org/10.3389/fmed.2022.857200.
Shahnazaryan D, Hajjar Sese A, Hollick EJ. Endothelial Cell loss after descemet’s membrane endothelial keratoplasty for Fuchs’ endothelial dystrophy: DMEK compared to triple DMEK. Am J Ophthalmol. 2020;218:1–6. https://doi.org/10.1016/j.ajo.2020.05.003.
Son H-S, Lum F, Li C, Schein O, Pramanik S, Srikumaran D. Risk factors for repeat keratoplasty after endothelial keratoplasty—an IRIS registry analysis. Am J Ophthalmol. 2022;242:77–87.
Aravena C, Yu F, Deng SX. Outcomes of Descemet membrane endothelial keratoplasty in patients with prior glaucoma surgery. Cornea. 2017;36(3):284.
Sorkin N, Mimouni M, Kisilevsky E, et al. Four-year survival of descemet membrane endothelial keratoplasty in patients with previous glaucoma surgery. Am J Ophthalmol. 2020;218:7–16.
Potts LB, Bauer AJ, Xu DN, et al. The last 200 surgeon-loaded Descemet membrane endothelial keratoplasty tissue versus the first 200 preloaded Descemet membrane endothelial keratoplasty tissue. Cornea. 2020;39(10):1261–6.
Koo EH, Paranjpe V, Feuer WJ, Persad PJ, Donaldson KE. Refractive outcomes in fuchs’ endothelial corneal dystrophy: conventional and femtosecond laser-assisted cataract surgery. Clin Ophthalmol (Auckland, NZ). 2021;15:3419–29. https://doi.org/10.2147/OPTH.S309869.
Yong WWD, Chai HC, Shen L, Manotosh R, Anna Tan WT. Comparing outcomes of phacoemulsification with femtosecond laser-assisted cataract surgery in patients with fuchs endothelial dystrophy. Am J Ophthalmol. 2018;196:173–80. https://doi.org/10.1016/j.ajo.2018.08.006.
Einan-Lifshitz A, Sorkin N, Boutin T, et al. Comparison of femtosecond laser-enabled descemetorhexis and manual descemetorhexis in descemet membrane endothelial keratoplasty. Cornea. 2017;36(7):767–70. https://doi.org/10.1097/ICO.0000000000001217.
Sorkin N, Mednick Z, Einan-Lifshitz A, et al. Three-year outcome comparison between femtosecond laser-assisted and manual descemet membrane endothelial keratoplasty. Cornea. 2019;38(7):812–6. https://doi.org/10.1097/ICO.0000000000001956.
Wacker K, Cavalcante LCB, Baratz KH, Patel SV. Hyperopic trend after cataract surgery in eyes with fuchs’ endothelial corneal dystrophy. Ophthalmology (Rochester, Minn). 2018;125(8):1302–4. https://doi.org/10.1016/j.ophtha.2018.03.060.
Campbell JA, Ladas JG, Wang K, Woreta F, Srikumaran D. Refractive accuracy in eyes undergoing combined cataract extraction and Descemet membrane endothelial keratoplasty. Br J Ophthalmol. 2021;106(5):623–7. https://doi.org/10.1136/bjophthalmol-2020-317247.
Augustin V, Weller J, Kruse F, Tourtas T. Refractive outcomes after descemet membrane endothelial keratoplasty + cataract/intraocular lens triple procedure: a fellow eye comparison. Cornea. 2020;40(7):883–7. https://doi.org/10.1097/ICO.0000000000002602.
Trindade BLC, Garcia JC, Nogueira LR. Toric IOL in combined DMEK and cataract surgery. Informa UK Limited; 2021. p. 1511.
Yokogawa H, Sanchez P, Mayko Z, Straiko M, Terry M. Astigmatism correction with toric intraocular lenses in descemet membrane endothelial keratoplasty triple procedures. Cornea. 2017;36(3):269–74. https://doi.org/10.1097/ICO.0000000000001124.
Price M, Pinkus D, Price F. Implantation of presbyopia-correcting intraocular lenses staged after descemet membrane endothelial keratoplasty in patients with fuchs dystrophy. Cornea. 2020;39(6):732–5. https://doi.org/10.1097/ICO.0000000000002227.
Pereira NC, Diniz ER, Ghanem RC, et al. Descemet membrane endothelial keratoplasty in multifocal pseudophakic eyes. Arq Bras Oftalmol. 2018;81(3):183–7. https://doi.org/10.5935/0004-2749.20180039.
Eisenbeisz HC, Bleeker AR, Terveen DC, Berdahl JP. Descemet Membrane Endothelial Keratoplasty and light adjustable lens triple procedure. Am J Ophthalmol case Rep. 2021;22: 101061. https://doi.org/10.1016/j.ajoc.2021.101061.
Borkar D, Veldman P, Colby K. Treatment of fuchs endothelial dystrophy by descemet stripping without endothelial keratoplasty. Cornea. 2016;35(10):1267–73. https://doi.org/10.1097/ICO.0000000000000915.
Moloney G, Petsoglou C, Ball M, et al. Descemetorhexis without grafting for fuchs endothelial dystrophy—supplementation with topical ripasudil. Cornea. 2017;36(6):642–8. https://doi.org/10.1097/ICO.0000000000001209.
Huang M, Kane S, Dhaliwal D. Descemetorhexis without endothelial keratoplasty versus DMEK for treatment of fuchs endothelial corneal dystrophy. Cornea. 2018;37(12):1479–83. https://doi.org/10.1097/ICO.0000000000001742.
Soh YQ, Peh G, George BL, et al. Predicative factors for corneal endothelial cell migration. Invest Ophthalmol Vis Sci. 2016;57(2):338–48. https://doi.org/10.1167/iovs.15-18300.
Bhogal M, Lwin CN, Seah X-Y, Peh G, Mehta JS. Allogeneic descemet’s membrane transplantation enhances corneal endothelial monolayer formation and restores functional integrity following descemet’s stripping. Invest Ophthalmol Vis Sci. 2017;58(10):4249–60. https://doi.org/10.1167/iovs.17-22106.
Antonini M, Coassin M, Gaudenzi D, Di Zazzo A. Rho-associated kinase inhibitor eye drops in challenging cataract surgery. Am J Ophthalmol Case Rep. 2022;25: 101245. https://doi.org/10.1016/j.ajoc.2021.101245.
Davies E, Jurkunas U, Pineda nR. Pilot study of corneal clearance with the use of a rho-kinase inhibitor after descemetorhexis without endothelial keratoplasty for fuchs endothelial corneal dystrophy. Cornea. 2021;40(7):899–902. https://doi.org/10.1097/ICO.0000000000002691.
Yq S, Gsl P, Js M. Translational issues for human corneal endothelial tissue engineering. J Tissue Eng Regener Med. 2017. https://doi.org/10.1002/term.2131.
Okumura N, Kinoshita S, Koizumi N. Cell-based approach for treatment of corneal endothelial dysfunction. Cornea. 2014. https://doi.org/10.1097/ICO.0000000000000229.
Madathil BK, Anil Kumar PR, Kumary TV. N-isopropylacrylamide-co-glycidylmethacrylate as a thermoresponsive substrate for corneal endothelial cell sheet engineering. Biomed Res Int. 2014. https://doi.org/10.1155/2014/450672.
Okumura N, Matsumoto D, Fukui Y, et al. Feasibility of cell-based therapy combined with descemetorhexis for treating Fuchs endothelial corneal dystrophy in rabbit model. PLoS ONE. 2018;13(1): e0191306.
Rizwan M, Peh GS, Adnan K, et al. In vitro topographical model of Fuchs dystrophy for evaluation of corneal endothelial cell monolayer formation. Adv Healthc Mater. 2016;5(22):2896–910.
Gf R. Shortening trinucleotide repeats using highly specific endonucleases: a possible approach to gene therapy? Trends Genet TIG. 2015. https://doi.org/10.1016/j.tig.2015.02.003.
Acknowledgements
Funding
No funding or sponsorship was received for this study or publication of this article.
Author Contributions
Muhammad Ali: Concept and design, drafting the manuscript, review, and editing. Kyongjin Cho: Concept and design, drafting the manuscript, review, and editing. Divya Srikumaran: Concept and design, drafting the manuscript, review, and editing.
Disclosures
Muhammad Ali and Kyongjin Cho have no disclosures. Divya Srikumaran: Eye Bank Association of America: Grant Support; AAO Hoskins Center: Grant Support; National Eye Institute: Grant Support; Johns Hopkins ICTR/NCATS: Grant Support; ABMS-REF: Grant Support; Alcon: Consultant; Expert Testimony: Legal Fees.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Data Availability
This article is based on previously conducted studies referenced throughout the text. Additional datasets were not analyzed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Ali, M., Cho, K. & Srikumaran, D. Fuchs Dystrophy and Cataract: Diagnosis, Evaluation and Treatment. Ophthalmol Ther 12, 691–704 (2023). https://doi.org/10.1007/s40123-022-00637-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-022-00637-1