
Abstract
Introduction
Lutein (L) and zeaxanthin (Z) are carotenoids that are found in the macula of the human eye and are known to improve visual functions. However, poor bioavailability of supplemental L and Z poses a challenge to achieving significant benefits after consumption. We developed a novel patented formulation of L and Z (Ocusorb®) and demonstrated the improved bioavailability in a pharmacokinetic clinical study.
Methods
Ninety adult human volunteers were recruited in this randomized, double-blind, parallel, comparative bioavailability study. Volunteers were randomly assigned to receive single dose of 10 mg lutein and 2 mg zeaxanthin from test (LZO) or reference (LZC) formulations after breakfast. Blood samples were collected pre-dose at − 48, − 24, and 0 h and at 2, 4, 6, 8, 10, 12, 16, 20, 24, 48, and 72 h post-dose. Serum concentrations of L and Z were quantified by using a validated HPLC method. The LZO and LZC formulations were compared for L and Z on the basis of Cmax, AUC0–72, and AUC0–t.
Results
All 90 subjects completed the study. The LZO group demonstrated significantly higher levels of L and Z in serum at several time points as compared to LZC group. The LZO group showed significantly higher bioavailability for lutein (2.5 times higher Cmax, 2.9 times higher AUC0–72, and 3.2 times higher AUC0–t) and zeaxanthin (1.8 times higher Cmax, 2.2 times higher AUC0–72, and AUC0–t) as compared to the LZC group. No safety issues were reported.
Conclusion
The study results show superior bioavailability of lutein and zeaxanthin from our novel LZO formulation as compared to LZC. The enhanced bioavailability from the LZO formulation can be advantageous for individuals looking to quickly improve their L and Z status and enhance their vision performance.
Trial Registration
http://ctri.nic.in/. Identifier: CTRI/2019/11/022082.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Lutein (L) and zeaxanthin (Z), known as macular carotenoids, are found in the macula of the human eye and are known to improve visual functions. |
Poor bioavailability of supplemental L and Z poses a challenge to achieve significant benefits after consumption. |
The study was conducted to evaluate the bioavailability of L and Z from a novel formulation known as Ocusorb® in comparison to the market sample. |
Ocusorb® demonstrated superior bioavailability for lutein—2.5 times higher Cmax, 2.9 times higher AUC0–72, and 3.2 times higher AUC0–t compared to the market sample. |
Ocusorb® demonstrated superior bioavailability for zeaxanthin—1.8 times higher Cmax, 2.2 times higher AUC0–72, and AUC0–t compared to the market sample. |
Enhanced bioavailability from Ocusorb® can be beneficial for individuals looking to quickly improve their L and Z status and enhance their vision performance. |
Introduction
Lutein and zeaxanthin (L and Z) are nutritionally important carotenoids found in several fruits and vegetables. As a result of selective accumulation in the macula of the human retina, L and Z are also known as macular carotenoids [1, 2]. L and Z have antioxidant properties and are known to absorb high energy blue light and protect the retina in the eye. The benefits of L and Z have been extensively researched for their roles in ocular, cognitive, and skin health [1, 3,4,5]. L and Z accumulate in the macula of the human eye and enhance visual performance [3, 5,6,7,8,9,10,11]. L and Z have also been shown to reduce the risk of age-related macular degeneration (AMD) [6, 7]. Choroidal neovascularization (CNV) plays a critical role in the pathogenesis of AMD, and in vivo animal models for neovascular AMD demonstrated significant suppression of the inflammatory process associated with CNV in response to lutein supplementation [12]. Regular intake of carotenoid-rich food has been associated with the reduced risk of several chronic diseases like photosensitivity diseases, cataracts, AMD, and cardiovascular diseases [13, 14].
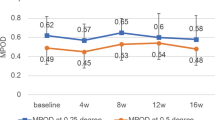
L and Z are isomers with identical chemical formulas. Lutein occurs as a single stereoisomer, while zeaxanthin occurs as a mixture of three stereoisomers, namely (3R,3′R)-zeaxanthin, (3R,3′S)-zeaxanthin, and (3S,3′S)-zeaxanthin. L and Z from the diet reach plasma and subsequently the macula where lutein is also converted to meso-zeaxanthin. Thus, the macular carotenoids responsible for macular pigment optical density (MPOD) are lutein, zeaxanthin, and meso-zeaxanthin at an approximate ratio of 2:1:1 in the retina [15]. Humans cannot synthesize lutein and (3R,3′R)-zeaxanthin and are dependent on dietary sources such as spinach, corn, lettuce, green peas, kale, pepper, orange, zucchini, and egg yolk to support adequate L and Z status [16, 17]. However, the intake of these fruits and vegetables are below the recommendations and dietary L and Z consumption is very low in most parts of the world. Inadequate dietary intakes of L and Z resulting in low serum levels of L and Z are associated with low macular pigment density and increased risk of AMD [18]. Supplementation with L and Z can help to support adequate L and Z status [19,20,21] and have been clinically demonstrated through increased serum levels of L and Z as well as higher deposition in the retina [3, 10]. However, considerable inter-individual variation in serum concentrations and macular pigment density has been reported following supplementation with L and Z [10]. Factors that affect the absorption of carotenoids, such as the matrix of the formulation and the form (i.e., free versus esterified) of the carotenoids determine the amount of L and Z achieved in serum after supplementation [4, 11]. Moreover, L and Z have poor bioavailability due to poor stability and solubility of the crystalline form in an aqueous medium. Hence, there has been considerable effort to develop L and Z formulations with improved stability and enhanced bioavailability to achieve improved health benefits. Various methods that have been used to develop formulations for L and Z include dispersion of crystals in edible oils, encapsulation with biopolymers [22], or mechanochemical complexation [23,24,25,26].
Here we report a novel formulation of L and Z (LZO) with improved bioavailability (patent filed WO 2021/074763 A1) using an optimized marigold and paprika extract as a source of L and Z respectively at a 5:1 ratio as found in nature in the form of natural dietary sources [27]. We used a micronization process to reduce the particle size followed by formation of an oil suspension in medium chain triglyceride (MCT) oil along with a combination of functional oils that helps to improve absorption from the small intestine. We evaluated the bioavailability of LZO in healthy human volunteers after single oral dose as compared to commercially available formulation (LZC) with L and Z at a similar dose.
Methods
The LZO formulation (Ocusorb®) was made using excipients like sunflower lecithin, olive oil, mixed tocopherol, thyme oil, linseed oil, and lime peel extract oil dissolved in MCT oil followed by addition of micronized marigold/paprika oleoresin mixture. This finished formulation was used for preparation of the study capsules. The final preparation was analyzed by HPLC using reference standard to ensure each gram of final product contains 80% of lutein and 16% of zeaxanthin. Each capsule (LZO) contained 10 mg of lutein and 2 mg of 3′R,3R-zeaxanthin. The reference group utilized LZC capsules which contained a blend of commercially available sample of lutein 20% and zeaxanthin 14% to obtain the dose of 10 mg lutein and 2 mg RR-zeaxanthin per capsule.
Study Design and Procedures
This was a double-blind, balanced, randomized, two-treatment, single-period, single-dose, parallel, comparative bioavailability study in healthy, adult, human subjects under fed conditions. The study was initiated after obtaining written approval from an institutional ethics committee, Maarg Independent Ethics Committee (EC registration Number ECR/77/Indt/AP/2013/RR-19), Secunderabad, India on 18 November 2019. The study was carried out in compliance with the requirements of the Indian Council of Medical Research (ICMR) ethical guidelines, International Council for Harmonization (ICH) Guidance on Good Clinical Practice (E6R2), and Declaration of Helsinki. The study was registered with the Clinical Trials Registry of India (CTRI/2019/11/022082).
Informed consent was voluntarily obtained from every participant before enrolling for the study. Subjects were randomly assigned in a 1:1 ratio to receive either LZO or LZC. The randomization schedule was generated by a non-study assigned, independent expert ensuring the treatment balance using SAS® statistical software, version 9.4. Staff who were involved in the investigational product-related activities were not involved in the study-related activities to ensure double blindness of the study.
Subjects stayed at the study center for a total of 6 days, 3 days before dosing and 3 days after dosing. During their stay, subjects were provided standard meals to control lutein and zeaxanthin in the diet. Subjects fasted overnight for at least 10 h and then received a high-fat, high-calorie breakfast comprising of 900 kcal with 57% fats, 27% carbohydrates, and 16% proteins the next day morning and 30 min later were administered a single oral dose of LZO or LZC containing 10 mg L or 2 mg Z along with 240 ± 2 mL of water. The subjects were dosed in a parallel manner to either LZO or LZC in the single period. The study product was administered to the subjects in a sitting posture and they remained in a sitting posture for the first 2 h (except at the time of vitals, natural and medical emergencies) unless clinically indicated. Thereafter, the subjects were allowed to engage only in normal activities while avoiding severe physical exertion. Blood test, vitals, and medical examinations were done for safety analysis.
Fourteen blood samples of 1 × 6 mL were collected from each subject. Three pre-dose blood samples were collected at 48, 24, and 0 h before dosing to establish baseline levels of lutein and zeaxanthin. Post-dose blood samples were collected at 2, 4, 6, 8, 10, 12, 16, 20, 24, 48, and 72 h. The blood sample collection and analysis were carried out under yellow monochromatic light because of the light sensitivity of lutein and zeaxanthin. After sample collection, samples were placed at room temperature for up to 30 min (time required for proper clot formation) and then centrifuged at 4 °C and 4000 rpm for 10 min to separate serum. The samples were placed in a deep freezer maintained at − 70 °C ± 10 °C until completion of serum sample analysis. A bioanalytical method for the estimation of lutein and zeaxanthin in human serum was developed and validated as per regulatory guidelines. Lutein and zeaxanthin were extracted from human serum by a liquid–liquid extraction method. Astaxanthin was used as internal standard for both lutein and zeaxanthin. The separation was achieved using a Kromasil 100-5SIL 250 × 4.6 mm, 5 μm with hexane/ethyl acetate (55:45 v/v) as mobile phase. The measured concentrations for each subject for all the time points were calculated against the calibration curve prepared with known standards. The retention time was 5.85, 6.48, and 3.90 min for lutein, zeaxanthin, and astaxanthin, respectively. Lutein and zeaxanthin were detected at wavelength of 456 nm and their concentrations in human serum samples were quantified using LabSolution 6.86 SP2 with a Shimadzu HPLC–photodiode array detection (PDA) system. The method was linear and validated over a concentration range of 20.92 to 10,434.15 ng/mL for lutein and 20.05 to 9998.85 ng/mL for zeaxanthin.
Study Population and Inclusion/Exclusion Criteria
A total of 90 healthy adult human subjects were enrolled in the study in accordance with the inclusion and exclusion criteria listed in Table 1.
Statistical Analysis
A sample size of 41 subjects per arm (82 subjects for both arms) was sufficient considering the difference in means and standard deviation with a 0.05 as alpha, two-sided significance level, and 90% as power. However, considering the 10% dropouts due to non-compliance or due to personal reasons, 90 subjects were randomized and dosed.
Study conduct and statistical analysis were performed at AnaCipher Clinical Research Organisation, Hyderabad using the SAS system for windows, version 9.4 (SAS institute Inc., Cary NC, USA). Pharmacokinetics parameters (Cmax, AUC0–72, AUC0–t, Tmax, and t1/2) were determined from the serum lutein and zeaxanthin concentrations by using Phoenix WinNonlin Version 8.2.
The arithmetic mean, minimum, maximum, standard deviations, and geometric mean were reported for the pharmacokinetic parameters of untransformed data. The geometric means were reported for AUC0–72, AUC0–t, and Cmax of log-transformed data.
The log-transformed pharmacokinetic parameters (AUC0–72, AUC0–t, and Cmax) were analyzed using an analysis of variance (ANOVA) model with the main effects of treatment. A 5% level of significance was used throughout the analysis. Each analysis of variance included calculation of least-square means, adjusted differences between treatment means, and the standard error associated with these differences.
For the pharmacokinetic parameters (AUC0–72, AUC0–t, and Cmax), 90% confidence intervals for the ratios of LZO and LZC averages were calculated using the ANOVA output from the analysis of the log-transformed data.
The 90% confidence intervals for the ratio of geometric least squares means between the formulations were calculated, for log-transformed pharmacokinetic parameters—Cmax, AUC0–72, AUC0–t for lutein and zeaxanthin.
The p values were calculated using the PROC GLM (ANOVA) output from the analysis of the log-transformed data. Probability values less than 0.05 denote statistically significant differences between LZO and LZC.
Safety assessments included monitoring of adverse events, physical examination, vital signs measurements, and laboratory assessments.
Results
Ninety male subjects completed the study with 100% compliance (Fig. 1). Out of the 90 randomized subjects, 45 subjects were allocated to the LZO group and 45 subjects to the LZC group. The demographic characteristics are provided in Table 2. The mean age of subjects was 29.96 ± 6.28 years in the LZO group and 31.00 ± 5.41 years in the LZC group. The mean body mass index (BMI) was 23.76 ± 2.30 in the LZO group and 23.55 ± 2.08 in the LZC group. There was no statistically significant difference between the two groups for age, and BMI at the baseline. Female subjects did not participate in the study because of social reasons associated with long-term housing at the study center.

Flowchart of this randomized, double-blind, comparative bioavailability study of lutein and zeaxanthin formulations
The analysis of pharmacokinetic parameters is presented for lutein and zeaxanthin in Table 3.
Results for Lutein
The LZO group showed significantly (p < 0.05) higher lutein serum concentrations (> 2-fold) at all time points i.e., 2 to 72 h post dose as compared to the LZC group (Fig. 2a).

Lutein and zeaxanthin serum levels versus time. The LZO group showed significantly (p < 0.05) higher serum lutein levels (> 2-fold) at all time points i.e., 2–72 h post dose (a) and higher serum zeaxanthin levels (> 1.5-fold) from 4 to 72 h post dose (b) as compared to the LZC group
The maximum serum concentration (Cmax) was significantly (p < 0.05) higher for LZO as compared to LZC (219.15 vs. 87.01 ng/mL; 90% CI 191.97–330.44%). Similarly, the total systemic exposure measured as area under the curve (AUC) was significantly (p < 0.05) higher for LZO as compared to LZC represented by AUC0–72 (8499.89 vs. 2892.09 h·ng/mL; 90% CI 217.33–397.46%) and AUC0–t (8264.02 vs. 2622.97 h·ng/mL; 90% CI 224.50–442.17%), respectively.
The LZO group showed significantly (p < 0.05) higher absorption for lutein based on 2.5 times higher Cmax, 2.9 times higher AUC0–72, and 3.2 times higher AUC0–t levels compared to the LZC group. (Table 3, Fig. 3).

Pharmacokinetic parameters of lutein in serum for test product (LZO) and reference product (LZC). a Mean serum lutein maximum concentration (Cmax). b Lutein area under the curve (AUC) serum concentration versus time for 0–72 h (AUC0–72) and 0 to last measurable concentration (AUC0–t). Cmax, AUC0–72, and AUC0–t were significantly (p < 0.05) higher for LZO compared to LZC
The median Tmax value for LZO was 20 h and LZC was 16 h for Lutein.
Results for Zeaxanthin
The LZO group showed significantly (p < 0.05) higher serum zeaxanthin concentrations (> 1.5-fold) from 4 to 72 h post dose as compared to the LZC group (Fig. 2b).
The maximum serum concentration (Cmax) was significantly (p < 0.05) higher for LZO as compared to LZC (56.95 vs. 32.55 ng/mL; 90% CI 140.70–217.50%), respectively. Similarly, the total systemic exposure measured as area under the curve (AUC) was significantly (p < 0.05) higher for LZO when compared to LZC represented by AUC0–72 (1929.93 vs. 861.65 h·ng/mL; 90% CI 159.64–314.26%) and AUC0–t (1817.29 vs. 814.17 h·ng/mL; 90% CI 154.35–322.79%), respectively.
The LZO group showed significantly (p < 0.05) higher absorption for zeaxanthin with 1.8 times higher Cmax, 2.2 times higher AUC0–72, and 2.2 times higher AUC0–t levels as compared to the LZC group (Table 3, Fig. 4).

Pharmacokinetic parameters of zeaxanthin in serum for test product (LZO) and reference product (LZC). a Mean serum zeaxanthin maximum concentration (Cmax). b Zeaxanthin area under the curve (AUC) serum concentration versus time for 0–72 h (AUC0–72) and 0 to last measurable concentration (AUC0–t). Cmax, AUC0–72, and AUC0–t were significantly (p < 0.05) higher for LZO compared to LZC
The median Tmax for LZO was 20 h and LZC was 24 h for Zeaxanthin.
The study product was well tolerated and did not show any adverse events.
Discussion
L and Z, also known as macular carotenoids, support visual performance and provide protection from ocular diseases such as AMD and cataract [1, 2, 28, 29]. Multiple human pharmacokinetic studies of L and Z have shown that intake of L and Z through diet or supplementation increases circulating levels of L and Z in the body leading to enhanced deposition in the macula of the eye. However, L and Z in the natural form have low bioavailability after oral intake due to their poor stability and inefficient absorption in the intestine leading to varying plasma concentrations [30]. In the current study we report a highly bioavailable formulation of L and Z that demonstrated significant improvement in absorption leading to increased serum levels after a single oral dose.
We observed a significant (p < 0.05) increase in serum lutein (> 2-fold) and zeaxanthin (> 1.5-fold) concentrations in the case of the LZO formulation at all time points measured post dose as compared to the LZC group. The maximum serum lutein concentration (Cmax) for LZO was 219.15 ng/mL which was 2.5 times higher and statistically significant (p < 0.05) as compared to LZC (Cmax 87.01 ng/mL). Similarly, maximum serum zeaxanthin concentration was 1.8 times higher with a statistically significant (p < 0.05) increase (Cmax 56.95 ng/mL) in the case of LZO as compared to LZC (Cmax 32.55 ng/mL). Further area under the curve (AUC) measurements for both AUC0–72 and AUC0–t, which is the total analyte exposure across time, significantly increased absorption for both L and Z in the case of LZO as compared to the LZC formulation. The LZO group showed 2.9 times higher AUC0–72 and 3.2 times higher AUC0–t levels for lutein and 2.2 times higher AUC0–72 and AUC0–t levels for zeaxanthin as compared to the LZC group.
The time taken for lutein to reach its highest concentration in serum (Tmax) was 20 h in the case of LZO as compared to 16 h in the case of LZC. Similarly, Tmax for zeaxanthin was 20 h in the case of LZO and 24 h for LZC. Overall, we observed an increased serum L and Z levels in the case of the LZO formulation as a result of faster and better absorption after supplementation which may aid better accumulation in the macula and enhance eye protection. Increased serum L and Z levels are known to increase the MPOD and directly improve visual performance [31].
Several studies have reported variable bioavailability of carotenoids due to the type of formulation matrix used, form of the bioactives (free versus esterified), and effects of other nutrients [32]. We micronized marigold and paprika oleoresin (source of L and Z, respectively) to reduce the particle size which in turn is known to improve dissolution rate and enhance oral bioavailability [33, 34]. Lutein in free form is not very stable and hence we used an oil suspension of medium chain triglycerides (MCT). MCT oil is considered as a healthy fatty acid, known to enhance permeability of intestinal mucosal membrane [35], improve absorption of lutein [36], and widely used in the nutraceutical industry [35, 37]. Further, we also incorporated multiple functional oils in the formulation that are known to improve absorption in the gut [38,39,40]. We believe that the cumulative effect of reduced particle size and combination of excipients used in the formulation improved the bioavailability of L and Z in the LZO formulation.
Both free and esterified lutein have been used to study single-dose, pharmacokinetic (PK) properties in human subjects [41,42,43]. Although variables such as intestinal absorption, metabolism, and serum clearance of carotenoids have an impact on circulating serum levels, the dose of L and Z used is also directly correlated with serum levels achieved, with an increased dose resulting in higher serum concentration [41]. Further, at a higher dose, the free form of lutein is better absorbed than lutein esters leading to increased plasma lutein levels [27, 44]. In the current study we observed increased circulating levels of L and Z owing to our improved formulation which is significant as this is achieved without increasing the dose. Higher circulating levels of L and Z are known to increase MPOD levels leading to improved visual protection and performance. The National Eye Institute sponsored the AREDS2 clinical study to evaluate the protective effects of carotenoids on progression of eye diseases. The study reported that 5-year supplementation of 10 mg lutein and 2 mg zeaxanthin leads to 18% reduction in AMD progression [29]. Other studies reported that increased dose of L and Z supplementation leads to increased plasma circulating levels of L and Z and improved MPOD [32] with improved health benefits such as improved contrast sensitivity, disability glare performance, and photo stress recovery [45, 46].
A limitation of the study was that female subjects did not participate because of social reasons associated with long-term housing at the study center. However, gender-specific differences in blood concentrations of L and Z have been reported to be very minimal [47,48,49].
Conclusions
L and Z protects the retina from blue light and provides antioxidant and anti-inflammatory support to retina and choroidal blood vessels that supply blood to the macular region of the retina [12]. Increased intake of L and Z not only increases the MPOD in the macula [28, 32] leading to improved visual acuity, sensitivity, and glare [29, 30, 50,51,52] but also reduces the risk of AMD [28, 53,54,55,56,57,58,59]. We developed an improved formulation of L and Z with significantly improved oral absorption leading to higher blood levels of L and Z which may further help in increased MPOD levels. L and Z supplements are generally considered to be safe [32] and are well tolerated. The enhanced bioavailability of this proprietary formulation can be advantageous for individuals looking to quickly improve their L and Z status and enhance their vision performance. Further, long-term human studies that evaluate MPOD and other related eye health benefits should help in accurate prediction of long-term benefits of our improved formulation.
References
Alves-Rodrigues A, Shao A. The science behind lutein. Toxicol Lett. 2004;150(1):57–83.
Ribaya-Mercado JD, Blumberg JB. Lutein and zeaxanthin and their potential roles in disease prevention. J Am Coll Nutr. 2004;23(sup6):567S-587S.
Whitehead AJ, Mares JA, Danis RP. Macular pigment: a review of current knowledge. Arch Ophthalmol. 2006;124(7):1038–45.
Evans M, Beck M, Elliott J, Etheve S, Roberts R, Schalch W. Effects of formulation on the bioavailability of lutein and zeaxanthin: a randomized, double-blind, cross-over, comparative, single-dose study in healthy subjects. Eur J Nutr. 2013;52(4):1381–91.
Barker FM, Snodderly DM, Johnson EJ, et al. Nutritional manipulation of primate retinas, V: effects of lutein, zeaxanthin, and n-3 fatty acids on retinal sensitivity to blue-light-induced damage. Investig Ophthalmol Vis Sci. 2011;52(7):3934–42.
Buscemi S, Corleo D, Di Pace F, Petroni ML, Satriano A, Marchesini G. The effect of lutein on eye and extra-eye health. Nutrients. 2018;10(9):1321.
Bungau S, Abdel-Daim MM, Tit DM, et al. Health benefits of polyphenols and carotenoids in age-related eye diseases. Oxid Med Cell Longev. 2019;2019:9783429. https://doi.org/10.1155/2019/9783429
Lien EL, Hammond BR. Nutritional influences on visual development and function. Prog Retin Eye Res. 2011;30(3):188–203.
Wong IYH, Koo SCY, Chan CWN. Prevention of age-related macular degeneration. Int Ophthalmol. 2011;31(1):73–82.
Connolly EE, Beatty S, Loughman J, Howard AN, Louw MS, Nolan JM. Supplementation with all three macular carotenoids: response, stability, and safety. Invest Ophthalmol Vis Sci. 2011;52(12):9207–17.
Nwachukwu ID, Udenigwe CC, Aluko RE. Lutein and zeaxanthin: production technology, bioavailability, mechanisms of action, visual function, and health claim status. Trends Food Sci Technol. 2016;49:74–84.
Izumi-Nagai K, Nagai N, Ohgami K, et al. Macular pigment lutein is antiinflammatory in preventing choroidal neovascularization. Arterioscler Thromb Vasc Biol. 2007;27(12):2555–62.
Krinsky NI, Johnson EJ. Carotenoid actions and their relation to health and disease. Mol Asp Med. 2005;26(6):459–516.
Mayne ST. Beta-carotene, carotenoids, and disease prevention in humans. FASEB J. 1996;10(7):690–701.
Thurnham DI. Macular zeaxanthins and lutein—a review of dietary sources and bioavailability and some relationships with macular pigment optical density and age-related macular disease. Nutr Res Rev. 2007;20(2):163–79.
Sommerburg O, Keunen JE, Bird AC, Van Kuijk FJ. Fruits and vegetables that are sources for lutein and zeaxanthin: the macular pigment in human eyes. Br J Ophthalmol. 1998;82(8):907–10.
Perry A, Rasmussen H, Johnson EJ. Xanthophyll (lutein, zeaxanthin) content in fruits, vegetables and corn and egg products. J Food Compos Anal. 2009;22(1):9–15.
Chiu CJ, Taylor A. Nutritional antioxidants and age-related cataract and maculopathy. Exp Eye Res. 2007;84(2):229–45.
Murphy MM, Barraj LM, Herman D, Bi X, Cheatham R, Randolph RK. Phytonutrient intake by adults in the United States in relation to fruit and vegetable consumption. J Acad Nutr Diet. 2012;112(2):222–9.
Tennant DR, Davidson J, Day AJ. Phytonutrient intakes in relation to European fruit and vegetable consumption patterns observed in different food surveys. Br J Nutr. 2014;112(7):1214–25.
Who J, Consultation FE. Diet, nutrition and the prevention of chronic diseases. World Health Organ Tech Rep Ser. 2003;916(i–viii):1–149.
Steiner BM, McClements DJ, Davidov-Pardo G. Encapsulation systems for lutein: a review. Trends Food Sci Technol. 2018;82:71–81.
Li B, Vachali PP, Shen Z, et al. Retinal accumulation of zeaxanthin, lutein, and β-carotene in mice deficient in carotenoid cleavage enzymes. Exp Eye Res. 2017;159:123–31.
Apanasenko IE, Selyutina OY, Polyakov NE, et al. Solubilization and stabilization of macular carotenoids by water soluble oligosaccharides and polysaccharides. Arch Biochem Biophys. 2015;572:58–65.
Olvera RM, Quiroga JT. Absorption and bioavailability of carotenoids, formulations and applications. Google Patents; 2008. Patent number US7435846B2, Patent date October 14, 2008.
Pavlović N, Goločorbin-Kon S, Ðanić M, et al. Bile acids and their derivatives as potential modifiers of drug release and pharmacokinetic profiles. Front Pharmacol. 2018;9:1283.
Thürmann PA, Schalch W, Aebischer JC, Tenter U, Cohn W. Plasma kinetics of lutein, zeaxanthin, and 3-dehydro-lutein after multiple oral doses of a lutein supplement. Am J Clin Nutr. 2005;82(1):88–97.
Sabour-Pickett S, Nolan JM, Loughman J, Beatty S. A review of the evidence germane to the putative protective role of the macular carotenoids for age-related macular degeneration. Mol Nutr Food Res. 2012;56(2):270–86.
Group AREDS 2 (AREDS2) R. Lutein+ zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA. 2013;309(19):2005–15.
Johnson EJ. Role of lutein and zeaxanthin in visual and cognitive function throughout the lifespan. Nutr Rev. 2014;72(9):605–12.
Stringham JM, Hammond BR Jr. Dietary lutein and zeaxanthin: possible effects on visual function. Nutr Rev. 2005;63(2):59–64.
Juturu V, Bowman JP, Stringham NT, Stringhan J. Bioavailability of lutein/zeaxanthin isomers and macular pigment optical density response to macular carotenoid supplementation: a randomized double blind placebo controlled study. New Front Ophthalmol. 2016;2:140–5.
Chaumeil JC. Micronization: a method of improving the bioavailability of poorly soluble drugs. Methods Find Exp Clin Pharmacol. 1998;20(3):211–6.
Oh DM, Curl RL, Yong CS, Amidon GL. Effect of micronization on the extent of drug absorption from suspensions in humans. Arch Pharm Res. 1995;18(6):427–33.
Lindmark T, Kimura Y, Artursson P. Absorption enhancement through intracellular regulation of tight junction permeability by medium chain fatty acids in Caco-2 cells. J Pharmacol Exp Ther. 1998;284(1):362–9.
Yuan X, Liu X, McClements DJ, Cao Y, Xiao H. Enhancement of phytochemical bioaccessibility from plant-based foods using excipient emulsions: impact of lipid type on carotenoid solubilization from spinach. Food Funct. 2018;9(8):4352–65.
Peterson B, Weyers M, Steenekamp JH, Steyn JD, Gouws C, Hamman JH. Drug bioavailability enhancing agents of natural origin (bioenhancers) that modulate drug membrane permeation and pre-systemic metabolism. Pharmaceutics. 2019;11(1):33.
Nidhi B, Mamatha BS, Baskaran V. Olive oil improves the intestinal absorption and bioavailability of lutein in lutein-deficient mice. Eur J Nutr. 2014;53(1):117–26.
Sugasini D, Lokesh BR. Curcumin and linseed oil co-delivered in phospholipid nanoemulsions enhances the levels of docosahexaenoic acid in serum and tissue lipids of rats. Prostaglandins Leukot Essent Fatty Acids. 2017;119:45–52.
Takenaka M, Ohkubo T, Okadome H, Sotome I, Itoh T, Isobe S. Effective extraction of curcuminoids by grinding turmeric (Curcuma longa) with medium-chain triacylglycerols. Food Sci Technol Res. 2013;19(4):655–9.
Kostic D, White WS, Olson JA. Intestinal absorption, serum clearance, and interactions between lutein and beta-carotene when administered to human adults in separate or combined oral doses. Am J Clin Nutr. 1995;62(3):604–10.
Bowen PE, Herbst-Espinosa SM, Hussain EA, Stacewicz-Sapuntzakis M. Esterification does not impair lutein bioavailability in humans. J Nutr. 2002;132(12):3668–73.
Norkus EP, Norkus KL, Dharmarajan TS, Schierle J, Schalch W. Serum lutein response is greater from free lutein than from esterified lutein during 4 weeks of supplementation in healthy adults. J Am Coll Nutr. 2010;29(6):575–85.
Schalch W, Cohn W, Barker FM, et al. Xanthophyll accumulation in the human retina during supplementation with lutein or zeaxanthin–the LUXEA (LUtein Xanthophyll Eye Accumulation) study. Arch Biochem Biophys. 2007;458(2):128–35.
Stringham JM, O’Brien KJ, Stringham NT. Contrast sensitivity and lateral inhibition are enhanced with macular carotenoid supplementation. Investig Ophthalmol Vis Sci. 2017;58(4):2291–5.
Stringham JM, Stringham NT, O’Brien KJ. Macular carotenoid supplementation improves visual performance, sleep quality, and adverse physical symptoms in those with high screen time exposure. Foods. 2017;6(7):47.
Hammond BR Jr, Curran-Celentano J, Judd S, et al. Sex differences in macular pigment optical density: relation to plasma carotenoid concentrations and dietary patterns. Vis Res. 1996;36(13):2001–12.
Olmedilla B, Granado F, Blanco I, Rojas-Hidalgo E. Seasonal and sex-related variations in six serum carotenoids, retinol, and α-tocopherol. Am J Clin Nutr. 1994;60(1):106–10.
Ito Y, Sasaki R, Suzuki S, Aoki K. Relationship between serum xanthophyll levels and the consumption of cigarettes, alcohol or foods in healthy inhabitants of Japan. Int J Epidemiol. 1991;20(3):615–20.
Mares J. Lutein and zeaxanthin isomers in eye health and disease. Annu Rev Nutr. 2016;36:571–602.
Bone RA, Landrum JT, Guerra LH, Ruiz CA. Lutein and zeaxanthin dietary supplements raise macular pigment density and serum concentrations of these carotenoids in humans. J Nutr. 2003;133(4):992–8.
Lamport DJ, Saunders C, Butler LT, Spencer JP. Fruits, vegetables, 100% juices, and cognitive function. Nutr Rev. 2014;72(12):774–89.
Ho L, van Leeuwen R, Witteman JC, et al. Reducing the genetic risk of age-related macular degeneration with dietary antioxidants, zinc, and ω-3 fatty acids: the Rotterdam study. Arch Ophthalmol. 2011;129(6):758–66.
Moeller SM, Parekh N, Tinker L, et al. Associations between intermediate age-related macular degeneration and lutein and zeaxanthin in the Carotenoids in Age-related Eye Disease Study (CAREDS): ancillary study of the Women’s Health Initiative. Arch Ophthalmol. 2006;124(8):1151–62.
Wu J, Cho E, Willett WC, Sastry SM, Schaumberg DA. Intakes of lutein, zeaxanthin, and other carotenoids and age-related macular degeneration during 2 decades of prospective follow-up. JAMA Ophthalmol. 2015;133(12):1415–24.
Ma L, Dou HL, Wu YQ, et al. Lutein and zeaxanthin intake and the risk of age-related macular degeneration: a systematic review and meta-analysis. Br J Nutr. 2012;107(3):350–9.
Liu XH, Yu RB, Liu R, et al. Association between lutein and zeaxanthin status and the risk of cataract: a meta-analysis. Nutrients. 2014;6(1):452–65.
Ma L, Hao ZX, Liu RR, Yu RB, Shi Q, Pan JP. A dose–response meta-analysis of dietary lutein and zeaxanthin intake in relation to risk of age-related cataract. Graefes Arch Clin Exp Ophthalmol. 2014;252(1):63–70.
Liu R, Wang T, Zhang B, et al. Lutein and zeaxanthin supplementation and association with visual function in age-related macular degeneration. Investig Ophthalmol Vis Sci. 2015;56(1):252–8.
Acknowledgements
Funding
The study, and the journal’s Rapid Service Fees, was funded by OmniActive Health Technologies Limited (Mumbai, India).
Other Acknowledgments
The authors would like to acknowledge OmniActive Health Technologies Ltd. for funding the study and providing the study products and thank the participating subjects and the staff of AnaCipher Clinical Research Organization, Hyderabad, India for conducting this study.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Srinivasa Rao Kotagiri, Chirag Khatri, Kalmanoor Babji and Abhijeet Morde designed the study and were involved in the data interpretation. Muralidhara Padigaru and Deshanie Rai provided suggestions on the study design and data interpretation. Srinivasa Rao Kotagiri, Chirag Khatri and Kalmanoor Babji helped in the conduct of the study at their site, volunteer recruitment, study procedures, data collection, statistical analysis, and study report. Mohan Lal developed the study formulation. The manuscript was drafted by Chirag Khatri, Srinivasa Rao Kotagiri, Kalmanoor Babji, Abhijeet Morde and Muralidhara Padigaru. All authors read and approved the final manuscript.
Disclosures
Abhijeet Morde, Muralidhara Padigaru, Deshanie Rai, and Mohan Lal are employees of OmniActive Health Technologies. All named authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Compliance with Ethics Guidelines
Institutional ethics approval was obtained from Maarg Independent Ethics Committee (EC registration Number ECR/77/Indt/AP/2013/RR-19), Secunderabad, India. This study was conducted in compliance with the ethical principles originating in or derived from the Declaration of Helsinki and in compliance with the International Conference on Harmonization (ICH), Good Clinical Practice (GCP) Guidelines, as well as in strict compliance with the “The New Drugs and Clinical Trial Rules-2019”, the Ministry of Health and the Government of India, India GCP guidelines released by Central Drugs Standard Control Organization, India, at all stages of the trial for adherence to protocol and compliance with ethical and regulatory guidelines. The EC was duly apprised of the progress and updates of the trial at regular intervals as per prescribed guidelines.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Kotagiri, S.R., Morde, A., Rai, D. et al. Superior Bioavailability of a Novel Lutein and Zeaxanthin Formulation in Healthy Human Subjects. Ophthalmol Ther 11, 1463–1477 (2022). https://doi.org/10.1007/s40123-022-00522-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-022-00522-x