
Abstract
Introduction
Glaucoma is a known complication of uveitis, and may require glaucoma tube shunt implantation for intraocular pressure (IOP) control. The success of glaucoma tube shunt implantation in the setting of a local ocular steroid depot in uveitic glaucoma remains unknown. The purpose of this study was to determine whether patients who underwent combined glaucoma tube shunt (Ahmed) and fluocinolone acetonide (Retisert™, Bausch + Lomb, Bridgewater, NJ, USA) implantation have superior outcomes compared to patients with Ahmed implants only in the setting of uveitic glaucoma.
Methods
All participants were studied retrospectively and underwent Ahmed implantation alone or with existing/concurrent Retisert implantation (combined group) at a single academic institution. The main outcome measures were IOP, visual acuity (VA), number of IOP-lowering medications, and adverse events at 6 months after Ahmed implantation. Secondary outcome measures included adverse events and surgical success at 6 months after Ahmed implantation.
Results
Mean IOP at 6 months after Ahmed implantation was 15.3 ± 4.8 and 15.1 ± 4.9 mm Hg in the Ahmed only group (n = 17) and the combined group (n = 17), respectively (p = 0.89). The mean number of IOP-lowering medications at 6 months after Ahmed implantation was 1.7 ± 1.0 and 1.8 ± 1.0 in the Ahmed only group and the combined group, respectively (p = 0.86). Mean VA at 6 months after Ahmed implantation was 0.35 ± 0.29 and 0.42 ± 0.33 log mean angle of resolution in the Ahmed only group and the combined group, respectively (p = 0.50). No significant differences in surgical success or adverse events were noted between the two groups.
Conclusion
At 6 months, no significant differences in mean IOP, mean number of IOP-lowering medications, VA, surgical success, or adverse events were noted between Ahmed implantation alone or combined Ahmed and Retisert implantation in patients with uveitic glaucoma.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The Ahmed glaucoma tube shunt, introduced in 1993 [1], is used in the management of elevated intraocular pressure (IOP) and glaucoma [2, 3]. The Ahmed design incorporates a flow restrictive device, thus reducing the incidence of postoperative hypotony [4] and making the Ahmed of particular utility in uveitic glaucoma [5]. After Ahmed implantation, the device progresses through predictable phases, including a hypertensive phase coinciding with encapsulation and bleb formation over the Ahmed plate. This phase is generally associated with an increase in IOP to greater than 21 mmHg [6]. Excessive inflammatory response after Ahmed implantation appears to be associated with higher failure rates and elevated IOP [7, 8]. Studies have demonstrated the importance of permeability of the capsule overlying the Ahmed plate in determining the long-term control of IOP [9, 10]. Anti-inflammatory agents have been shown to be associated with thinner-walled capsules and lower IOP in certain patient populations [11, 12]. Indeed, recent studies using long-term topical steroid tapers, as well as aqueous suppressants after Ahmed implantation appear to show a reduction in the degree of IOP elevation during the ocular hypertensive phase, as well as an improvement in the long-term IOP control [13].
Given the above observations of capsule formation limiting Ahmed function and the potential benefit of anti-inflammatory agents in preventing excessive capsule formation, we hypothesized that patients with the long-term intravitreal steroid depots in the form of fluocinolone acetonide (Retisert™, Bausch + Lomb, Bridgewater, NJ, USA) implants undergoing Ahmed implantation might have superior IOP control relative to eyes receiving Ahmed implant alone. This hypothesis was further supported by a recent publication showing a trend towards lower IOP in uveitic patients who underwent combined Ahmed and Retisert implant relative to patients with primary open angle glaucoma who underwent Ahmed implant alone [14].
Methods
Study Population
After institutional review board approval from Oregon Health and Science University (OHSU), a retrospective analysis of electronic medical records from 2004 to 2015 at OHSU was conducted. Patients with an established diagnosis code of uveitis, as well as surgical billing codes corresponding to Retisert implantation prior to, or concurrent with Ahmed glaucoma tube shunt (model S2, New World Medical, Cucamonga, CA, USA) implantation were identified. The surgeries were performed by five glaucoma surgeons and three vitreoretinal surgeons during the study period. All patients had the diagnoses of uveitis and uncontrolled IOP in the eye undergoing Ahmed implantation. All patients had 6 months of follow-up with the following exceptions: one patient from the combined Ahmed and Retisert group relocated out of state 3 months after Ahmed implantation, while one patient from the Ahmed only group chose to follow up with a local provider 1 month after Ahmed implantation. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (OHSU IRB) and with the Helsinki Declaration of 1964, as revised in 2013. This article is based on previously performed procedures and does not involve any new studies of human or animal subjects performed by any of the authors.
Study Design and Outcome Measures
For both the groups, the data were collected immediately prior to Ahmed implantation and at the following time intervals after Ahmed implantation: 1 day, 1 week, 1 month, 3 months, and 6 months. Primary clinical outcomes included visual acuity (VA) converted to the log of the mean angle of resolution (logMAR), IOP, and the number of topical IOP-lowering medications. LogMAR values of 2.3, 2.9, 3.2, and 3.5 were assigned to counting fingers, hand motion, light perception, and no light perception visions, respectively, according to the grading scheme of the World Glaucoma Association [15]. In addition, the presence of active inflammation was defined as any eye with any of the following findings within 3 months prior to Ahmed implantation: anterior chamber cell grade greater than zero, active cystoid macular edema, active leakage on fluorescein angiography, or vitreous haze grade greater than zero. The need for clinically active inflammatory control was defined as any eye requiring a new or additional inflammatory control therapy within 3 months prior to Ahmed implantation. A secondary outcome measure of surgical success was defined as IOP between 5 and 18 mmHg and greater than 20% reduction of IOP at two consecutive visits, without loss of light perception, or need for additional IOP-lowering procedures. Postoperative complications were also noted, including sustained postoperative ocular hypotension (IOP <5 mmHg on 2 or more consecutive follow-up visits), need for additional IOP-lowering procedures, need for Ahmed implant removal, or drop in VA to light perception or worse.
Statistical Analysis
The statistical analysis was performed using the Microsoft Excel and GraphPad Prism 6 software (La Jolla, California, USA). A Student t test was performed to determine whether there was significant difference in measured outcomes between the two groups at baseline and at 6 month post-Ahmed surgery. The duration of surgical success was compared between the two groups using Kaplan–Meier curves and the log-rank test. A multivariate regression analysis was performed to evaluate the relationship between surgical success and multiple variables. P values less than 0.05 were considered statistically significant.
Results
Baseline Characteristics
Seventeen eyes of 13 participants were studied in the combined Ahmed and Retisert group. The comparison group included 17 eyes of 12 age-matched participants with a diagnosis of uveitis that underwent Ahmed implantation alone. Baseline patient characteristics in the Ahmed only group included a mean patient age at the time of Ahmed placement of 50.9 ± 14.4 years. Mean VA at baseline prior to Ahmed implantation was 0.55 ± 0.74 logMAR. Mean IOP at baseline was 39.9 ± 13.8 mmHg, and the mean number of IOP-lowering medications at baseline was 3.0 ± 0.7. Within 3 months prior to Ahmed surgery, 52.9% of eyes in the Ahmed only group had clinically active inflammation and 17.6% needed anti-inflammatory therapy (Table 1).
Baseline patient characteristics in the combined Ahmed and Retisert group at the time of Ahmed placement included a mean age of 49.8 ± 14.2 years. Mean VA at baseline before Ahmed placement was 0.42 ± 0.33 logMAR. Mean IOP at baseline was 30.1 ± 10.8 mmHg, and the mean number of IOP-lowering medications at baseline was 2.9 ± 1.1. Within three months prior to Ahmed surgery, 29.4% of eyes in the combined group had clinically active inflammation and 11.8% needed anti-inflammatory therapy. In the combined group, all Retisert implants were placed prior to, or concurrent with, Ahmed implantation. Three of 17 eyes (17.6%) in the combined group underwent concurrent Ahmed and Retisert implantation (on the same surgical day), while 14 of 17 eyes (82.4%) underwent Ahmed implantation at some point after the Retisert implantation surgery (Table 1). The overall mean interval time between Retisert and Ahmed implantation was 1.1 ± 1.3 years.
A small portion (11.8%) of patients in the Ahmed only group received an increase in steroid medications pre-operatively compared to none in the combined group (p = 0.15). Some patients received additional intraoperative steroid injections beyond the routine subconjunctival dexamethasone injection (29.4% in the Ahmed only group vs. 5.9% in the combined group, p = 0.08). In the Ahmed only group, this included four patients who received intravenous methylprednisolone (125 mg) and one patient who received peribulbar triamcinolone (40 mg). In the combined Ahmed and Retisert group, this included one patient who received peribulbar triamcinolone (40 mg). More patients in the Ahmed only group underwent systemic steroid therapy (in the form of oral prednisone) beyond topical steroid taper after Ahmed implantation compared to the combined group (64.7% vs 0%, p ≤ 0.01). Of note, a significantly smaller portion of eyes in the combined Ahmed and Retisert group was on systemic immunosuppressive therapy at baseline, relative to the Ahmed only group (Table 1). Three of 17 eyes (17.6%) in each group underwent concurrent cataract surgery and intraocular lens placement at the time of Ahmed implantation.
Intraocular Pressure
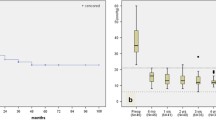
After Ahmed implantation, both the Ahmed only and combined Ahmed and Retisert groups had a significant reduction in mean IOP on postoperative day 1 (Fig. 1). The initial reduction in IOP immediately after Ahmed implantation was followed by a gradual increase in the IOP at the 1 month time point in both the groups, consistent with the hypertensive phase of Ahmed implants (Fig. 1). There was no statistically significant difference in IOP at any time point up to 6 months between the groups post-Ahmed implantation (Fig. 1). The final mean IOP at 6 months was 15.3 ± 4.8 and 15.1 ± 4.9 mm Hg (p = 0.89) in the Ahmed only and combined groups, respectively.

Mean intraocular pressures (IOP, mmHg ± standard deviation) pre- and post- Ahmed implantation for both the Ahmed + Retisert group and Ahmed only group. From left to right, n = 17, 17, 17, 17, 17, 16 for the Ahmed + Retisert group and n = 17, 17, 17, 17, 16, 16 for the Ahmed only group, respectively. Statistically significant difference in mean IOP (p < 0.05) was noted at baseline (time = 0), while no significant difference in mean IOP was noted at any time point after Ahmed implantation
Number of IOP-Lowering Medications
The number of IOP-lowering medications immediately after Ahmed implantation was significantly reduced in both the Ahmed only group and the combined Ahmed and Retisert group (Fig. 2). Both the groups required an increase in IOP-lowering medication at approximately 1 month post-Ahmed implant, consistent with the known ocular hypertensive phase of the Ahmed glaucoma tube shunt. This increase in the need for IOP-lowering medication at 1 month also corresponded to the increase in IOP post-Ahmed implantation at 1 month (Fig. 1). The mean number of IOP-lowering medications at 6 month post-Ahmed implantation were 1.7 ± 1.0 and 1.8 ± 1.0 (p = 0.86) in the Ahmed only and combined Ahmed and Retisert groups, respectively (Fig. 2). No statistically significant difference in the number of IOP-lowering medications was noted between the two groups at any time point in the follow-up period.

Mean intraocular pressure (IOP)-lowering medications (number ± standard deviation) pre- and post-Ahmed implantation for both the Ahmed + Retisert group and the Ahmed only group. From left to right, n = 17, 17, 17, 17, 17, 16 for the Ahmed + Retisert group and n = 17, 17, 17, 17, 16, 16 for the Ahmed only group, respectively. No significant difference in the number of IOP-lowering medication was noted at any time point during follow-up
Visual Acuity
Immediately after Ahmed implantation, a trend towards worsening VA was noted in both the Ahmed only and the combined Ahmed and Retisert groups (Fig. 3). However, the VA in both the groups trended towards an improvement, and reached levels similar to baseline VA prior to Ahmed implantation (Fig. 3). The VA at 6 months after Ahmed placement was 0.35 ± 0.29 logMAR in the Ahmed only group and 0.42 ± 0.33 logMAR in the combined Ahmed and Retisert group (p = 0.50). Both the groups had large variability in single time point analysis, as well as throughout the follow-up period (Fig. 3). No statistically significant difference in VA was noted between the two groups at any time point in the follow-up period. During the 6 month period of follow-up, worsening cataract was noted in the clinical assessment of 3 out of 8 (37.5%) and 1 out of 2 (50%) phakic eyes in the Ahmed only and combined Ahmed and Retisert groups, respectively (p = 0.78). At 6 month post-Ahmed implantation, 53.0% of patients in the Ahmed only group were pseudophakic relative to 88.2% in the combined Ahmed and Retisert group (p = 0.02), which were unchanged from baseline levels (Table 1).

Mean visual acuity (VA, log of the mean angle of resolution, logMAR ± standard deviation) pre- and post-Ahmed implantation for both the Ahmed + Retisert group and the Ahmed only group. From left to right, n = 17, 17, 17, 17, 17, 16 for the Ahmed + Retisert group and n = 17, 17, 17, 17, 16, 16 for the Ahmed only group, respectively. No significant difference in the mean VA was noted at any time point during follow-up
Systemic Immunosuppression and Active Inflammation
Post-Ahmed implant systemic immunosuppression was required in a larger proportion of eyes in the Ahmed only group (52.9, 43.8, and 35.7% at 1, 3, and 6 months, respectively) relative to the combined Ahmed and Retisert group (11.8, 6.2, and 6.7% at 1, 3, and 6 months, respectively). This difference was statistically significant at 1 and 3 months, but not at 6 months (p ≤ 0.01, 0.01, and 0.06, respectively). Of those patients receiving systemic immunosuppression, some received a short (less than 1 month) postoperative oral steroid taper after Ahmed implant at a rate of 64.7% in the Ahmed only group and 0% in the combined Ahmed and Retisert group. The level of active inflammation (as defined by anterior chamber cell grade greater than zero, active cystoid macular edema, active leakage on fluorescein angiography, or vitreous haze grade greater than zero) trended towards a higher level in the Ahmed only group (23.5, 25.0, and 35% at 1, 3, and 6 months) relative to the combined Ahmed and Retisert group (23.5, 17.6, and 18.8% at 1, 3, and 6 months). However, these differences did not reach statistical significance at any time point in the study.
Surgical Success
Using the Kaplan–Meier survival analysis, there appeared to be a trend towards higher surgical success in the combined Ahmed and Retisert group relative to the Ahmed only group, however, we found no statistically significant difference in the duration of surgical success between the two groups (p = 0.32, Fig. 4). The cumulative probability of success at 6 months was 41.2% and 35.2% for the combined Ahmed and Retisert and the Ahmed alone groups, respectively. The principal reason for failure in both groups was sustained ocular hypertension, with the largest drop in surgical success being noted around the 1 month postoperative period (Fig. 4). With multivariate regression analysis, the number of IOP-lowering medication at baseline (prior to Ahmed implantation) significantly and inversely correlates with surgical success (odds ratio 0.48, 95% CI 0.08–0.89, p value 0.025). Other baseline factors, including age, sex, the presence of posterior uveitis diagnosis, VA, IOP, systemic immunosuppressive therapy, active inflammation, need for clinically active inflammatory control, and pseudophakia were evaluated and were not statistically significant.

Kaplan–Meier curves representing cumulative probability of surgical success for Ahmed implantation alone compared to Ahmed and Retisert implantation. Surgical success was defined as intraocular pressure (IOP) between 5 and 18 mmHg and greater than 20% reduction of IOP at two consecutive visits without loss of light perception, or need for an additional IOP-lowering surgical procedure. No statistically significant difference was found between the curves
Adverse Events
Three of the 17 eyes (17.6%) experienced sustained ocular hypotension (IOP <5 mm Hg on two or more consecutive visits) in the combined Ahmed and Retisert group, compared to none in the Ahmed only group (p = 0.08). All the three cases of hypotony were noted between the first day and first week post-Ahmed implantation, and resolved thereafter. The etiology of hypotony was recorded as decreased aqueous production in two patients and leakage from the site of the prior Retisert implant in the third patient. No other adverse events, including the need for additional IOP-lowering surgery, the requirement of Ahmed removal, and a drop of VA to light perception, were noted in either group throughout the 6 month follow-up period.
Discussion
While evidence exists to support the use of anti-inflammatory medications to reduce significant capsule formation and thus failure after Ahmed implant, our study did not find a significant difference in outcomes between combined Ahmed and Retisert implantation versus Ahmed implantation alone in uveitic glaucoma. Our results show no statistically significant difference between the two groups in mean IOP, mean number of IOP-lowering medications, or mean VA at 6 months. We did observe a significant difference in the two studied groups (Ahmed alone vs. combined Ahmed and Retisert) with regard to the need for systemic immunosuppression post-Ahmed implantation. This likely reflects the intended use of local steroid depot delivery to the eye with Retisert implantation in uveitis, which reduces the need for systemic immunosuppression [16, 17]. Of note, the level of active inflammation was not statistically different between the two groups at 1, 3, and 6 month post-Ahmed implantation. Thus, local or systemic immunosuppression in uveitic glaucoma appears to provide similar outcomes with regard to Ahmed implantation up to 6 month post implantation. The trend toward worsening VA immediately after Ahmed implant in both the groups may be related to the early and temporary postoperative changes (including but not limited to, tear film instability, corneal edema, and refractive changes).
Our results are consistent with a retrospective study by Moore et al. of uveitic patients undergoing multiple Ahmed model implantations (S2, S3, FP7, and M4) with or without Retisert implantation, which found no significant difference in the long-term IOP control between these two groups [14]. However, Moore et al. found that the duration of surgical success (defined as IOP between 5 and 18 mm Hg and greater than 20% reduction of IOP at two consecutive visits without loss of light perception, or need for additional IOP-lowering surgical procedures) was significantly greater in the combined Ahmed and Retisert group when compared to Ahmed alone [14]. In addition, Moore et al. noted a higher survival probability in both the Ahmed alone and the combined Ahmed and Retisert groups relative to our study at approximately 6 months [14]. Given the retrospective nature of both the studies, the discrepancy may be explained by potentially different follow-up regimen schedules. As both the studies use the criteria of maintained IOP control on two consecutive visits, the number and frequency of follow-ups in each study patient within each institution may affect whether an ocular hypertensive phase was documented more or less frequently throughout the follow-up period. While the study by Moore et al. and our study have comparable uveitic patient numbers within each group (Ahmed only vs. combined Ahmed and Retisert), the study by Moore et al. reported longer mean follow-up time post-Ahmed implantation, while our study reports outcomes relative to an age-matched population.
Another recent retrospective study by Hennein et al. found that patients who underwent Ahmed implantation in the setting of Retisert implants had lower IOP and were using less IOP-lowering medication relative to Ahmed only controls at 1 year post-Ahmed implant [18]. However, consistent with our results, the study by Hennein et al. found no statistically significant difference in IOP between the two groups at 6 months after Ahmed implantation [18]. In addition, while the study by Hennein et al. included a large number of control patients with Ahmed implantation only (a ratio of three control eyes to one study eye), the control eyes were not age-matched, and only 6 out of 55 control eyes had a diagnosis of uveitic glaucoma [18]. Finally, our study uniquely reports pre- and post-Ahmed implantation inflammatory control in both the combined and control populations, which is an important variable in studies involving uveitic glaucoma.
Our study suggests that the combined Ahmed and Retisert implantation is well-tolerated and no statistically significant difference in adverse outcomes between the two groups was noted, although the Ahmed and Retisert combined group did experience more sustained ocular hypotension (defined as IOP <5 mm Hg) over the 6 month period (however, this difference did not reach statistical significance). No eyes from either group required additional IOP-lowering procedures or removal of the Ahmed implant, and no drop in VA to light perception or worse was noted. These findings agree with the low complication rates in a prior study reporting the safety of the combined Ahmed and Retisert implantation [19].
IOP control at 6 months in our study is in agreement with prior reports of clinical outcomes after Ahmed implantation. In the Ahmed-Baerveldt Comparison study and Ahmed Versus Baerveldt study, mean IOP and mean number of IOP-lowering medications 6 months after Ahmed implantation alone [20, 21] were comparable to this study for both the Ahmed alone and the combined Ahmed and Retisert groups. In a retrospective analysis of patients undergoing concurrent Ahmed and Retisert implant, Malone et al. found that the average IOP 12 months after Ahmed and Retisert implantation was 14.6 mm Hg [19]. These further support the suggestion that the addition of a Retisert implant to the Ahmed implant provides no additional benefit in IOP control versus Ahmed implantation alone in the setting of uveitis. In addition, consistent with prior reports, IOP elevation and need for additional IOP-lowering medication were noted around 1 month post-Ahmed implantation, which is consistent with the known ocular hypertensive phase of Ahmed implants.
This study, however, does have some limitations. The number of patients studied was limited, with the number of patients who underwent Retisert and Ahmed implantation as the limiting factor. Despite sampling patients over a 10 year period at a large, academic eye institute, only 17 eyes were identified in the combined Retisert and Ahmed group. In addition, while care was taken to randomly assign controls (Ahmed only) that were age-matched to the patients receiving combined Ahmed and Retisert implants, this process can introduce an inherent selection bias. Data were analyzed retrospectively, and though every effort was made to achieve accuracy, differences in methods of measurement and inter-observer variability at the time of data documentation could not be controlled. In addition, the follow-up regimen and frequency were variable due to the retrospective nature of the study. The percentage of patients with a diagnosis of posterior uveitis was higher in the combined group, which likely reflects the utility of Retisert implantation to control posterior uveitis [22]. Mean IOP at baseline was higher in the Ahmed only group, relative to the combined Ahmed and Retisert group, which may be due to the ability of Retisert implant to a better control intraocular inflammation, and reduce ocular hypertensive episodes due to uncontrolled inflammation. Indeed, while baseline active inflammation was not statistically significant between the two groups, the Ahmed only group trended towards a higher baseline active inflammation prior to Ahmed implantation. While we found no significant differences in the proportions of patients with active inflammation or clinically active patients in the two groups, other unmeasured contributors to inflammation severity (such as anatomic posterior-predominant site of inflammation, which may be considered more severe than anterior and intermediate forms in some cases) may mask a potentially better outcome of Ahmed implantation in the presence of Retisert implantation.
Conclusion
In this retrospective review that included 34 adults with uveitic glaucoma, no significant differences in mean IOP, mean number of IOP-lowering medications, VA, surgical success, or adverse events were noted between Ahmed implantation alone or combined Ahmed and Retisert implantation at 6 months. Further studies with larger sample sizes, longer follow-up, and prospective evaluation may provide more insight into patient outcomes after Ahmed implantation with or without the presence of a Retisert implant.
References
Coleman AL, Hill R, Wilson MR, et al. Initial clinical experience with the Ahmed glaucoma valve implant. Am J Ophthalmol. 1995;120(1):23–31.
Gedde SJ, Schiffman JC, Feuer WJ, et al. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012;153(5):789–803 e782.
Budenz DL, Barton K, Gedde SJ, et al. Five-year treatment outcomes in the Ahmed Baerveldt comparison study. Ophthalmology. 2015;122(2):308–16.
Ayyala RS, Zurakowski D, Smith JA, et al. A clinical study of the Ahmed glaucoma valve implant in advanced glaucoma. Ophthalmology. 1998;105(10):1968–76.
Papadaki TG, Zacharopoulos IP, Pasquale LR, Christen WB, Netland PA, Foster CS. Long-term results of Ahmed glaucoma valve implantation for uveitic glaucoma. Am J Ophthalmol. 2007;144(1):62–9.
Ayyala RS, Hong C-H, Layden WE. Comparison of double-plate Molteno and Ahmed glaucoma valve in patients with advanced uncontrolled glaucoma. Ophthalm Surg Lasers Imaging Retina. 2002;33(2):94.
Hong CH, Arosemena A, Zurakowski D, Ayyala RS. Glaucoma drainage devices: a systematic literature review and current controversies. Surv Ophthalmol. 2005;50(1):48–60.
Ozdal PC, Vianna RN, Deschenes J. Ahmed valve implantation in glaucoma secondary to chronic uveitis. Eye (London, England). 2006;20(2):178–83.
Wilcox MJ, Barad JP, Wilcox CC, Peebles EL, Minckler DS. Performance of a new, low-volume, high-surface area aqueous shunt in normal rabbit eyes. J Glaucoma. 2000;9(1):74–82.
Minckler DS, Shammas A, Wilcox M, Ogden TE. Experimental studies of aqueous filtration using the Molteno implant. Trans Am Ophthalmol Soc. 1987;85:368–92.
Molteno AC, Straughan JL, Ancker E. Control of bleb fibrosis after glaucoma surgery by anti-inflammatory agents. S Afr Med J. 1976;50(23):881–5.
Molteno A, Dempster A. Methods of controlling bleb fibrosis around draining implants. Paper presented at: Glaucoma. In: Proc 4th Int Symposium of North Eye Institute. Manchester, UK; 1988.
Pakravan M, Rad SS, Yazdani S, Ghahari E, Yaseri M. Effect of early treatment with aqueous suppressants on Ahmed glaucoma valve implantation outcomes. Ophthalmology. 2014;121(9):1693–8.
Moore DB, Stinnett S, Jaffe GJ, Asrani S. Improved surgical success of combined glaucoma tube shunt and Retisert® implantation in uveitic eyes: a retrospective study. Ophthalmol Ther. 2015;4(2):103–13.
Shaarawy T, Sherwood M, Grehn F. Guidelines on design and reporting of glaucoma surgical trials. Amsterdam: Kugler; 2009.
Multicenter Uveitis Steroid Treatment Trial Research G, Kempen JH, Altaweel MM, et al. Benefits of systemic anti-inflammatory therapy versus fluocinolone acetonide intraocular implant for intermediate uveitis, posterior uveitis, and panuveitis: fifty-four-month results of the multicenter uveitis steroid treatment (MUST) trial and follow-up study. Ophthalmology. 2015;122(10):1967–75.
Multicenter Uveitis Steroid Treatment Trial Follow-up Study Research G. Quality of life and risks associated with systemic anti-inflammatory therapy versus fluocinolone acetonide intraocular implant for intermediate uveitis, posterior uveitis, or panuveitis: fifty-four-month results of the multicenter uveitis steroid treatment trial and follow-up study. Ophthalmology. 2015;122(10):1976–86.
Hennein L, Hou J, Stewart JM, et al. Comparison of surgical outcome after ahmed valve implantation for patients with and without fluocinolone intravitreal implant (retisert). J Glaucoma. 2016;25(9):e772–6.
Malone PE, Herndon LW, Muir KW, Jaffe GJ. Combined fluocinolone acetonide intravitreal insertion and glaucoma drainage device placement for chronic uveitis and glaucoma. Am J Ophthalmol. 2010;149(5):800–806 e801.
Budenz DL, Barton K, Feuer WJ, et al. Treatment outcomes in the Ahmed Baerveldt comparison study after 1 year of follow-up. Ophthalmology. 2011;118(3):443–52.
Christakis PG, Kalenak JW, Zurakowski D, et al. The Ahmed versus Baerveldt study: one-year treatment outcomes. Ophthalmology. 2011;118(11):2180–9.
Sangwan VS, Pearson PA, Paul H, Comstock TL. Use of the fluocinolone acetonide intravitreal implant for the treatment of noninfectious posterior uveitis: 3-year results of a randomized clinical trial in a predominantly asian population. Ophthalmol Ther. 2015;4(1):1–19.
Acknowledgments
This work was supported by an American Glaucoma Society Young Clinician Scientist Award (ST), a Glaucoma Research Foundation Shaffer Grant (ST), a Research to Prevent Blindness (RPB) Career Development Award (ST), the National Institute of Health (K08EY024025 to ST and P30EY010572 to CEI/OHSU), and an unrestricted grant from RPB (CEI/OHSU). All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given the final approval to the version to be published. The authors would like to thank the following additional physicians and surgeons, whose patients’ outcomes were retrospectively reviewed as part of this study: Drs. Christine Flaxel, Thomas Hwang, and John Morrison.
Disclosures
Mark Zivney, Phoebe Lin, Beth Edmunds, Mansi Parikh, Hana Takusagawa, and Shandiz Tehrani have nothing to disclose.
Compliance with Ethics Guidelines
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (OHSU IRB) and with the Helsinki Declaration of 1964, as revised in 2013. This article is based on previously performed procedures and does not involve any new studies of human or animal subjects performed by any of the authors.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article, go to http://www.medengine.com/Redeem/5FD6F060144EDD43.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Zivney, M., Lin, P., Edmunds, B. et al. Combined Glaucoma Tube Shunt (Ahmed) and Fluocinolone Acetonide (Retisert™) Implantation Compared to Ahmed Alone in Uveitic Glaucoma. Ophthalmol Ther 5, 223–233 (2016). https://doi.org/10.1007/s40123-016-0066-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40123-016-0066-2