
Abstract
Introduction
Nonsteroidal antiinflammatory drugs (NSAIDs) are commonly used for pain disorders such as low back pain and exist in multiple formulations; however, no systemically acting transdermal formulations are available for low back pain. Transdermal formulations can be safely administered even to patients with trouble swallowing or at risk of aspiration, and without regard to the effect of food on drug absorption. Unlike locally acting formulations, systemically acting transdermal formulations need not be applied at the target site, so dosing is simple and the burden is not on one area of the skin. A patch with the systemically acting NSAID diclofenac sodium is approved in Japan for treatment of cancer-related pain, and we hypothesized that it would be useful for controlling low back pain.
Methods
This randomized, double-blind, placebo-controlled study aimed to evaluate the efficacy and safety of diclofenac sodium patch in Japanese patients with low back pain. Eligible patients were randomized to receive diclofenac sodium patch 75 mg or 150 mg or placebo once daily for 2 weeks. The primary endpoint was pain intensity assessed on a visual analog scale (VAS).
Results
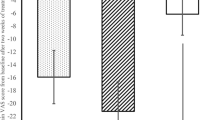
Primary analysis of the primary endpoint showed that both doses of the diclofenac sodium patch (150 mg and 75 mg) were superior to placebo in terms of absolute change from baseline in mean 3-day VAS score after 2 weeks’ treatment; the mean difference between the active and placebo treatments in this variable was −5.67 [95% confidence interval (CI) −9.34 to −2.00] mm in the 150 mg group and −5.68 (95% CI −9.34 to −2.01) mm in the 75 mg group. Most adverse events were mild. No serious adverse events occurred.
Conclusion
In Japanese patients, diclofenac sodium patch is effective for the relief of low back pain and is well tolerated.
Trial Registration
JPRN number, JPRN-JapicCTI-205134.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Why carry out this study? |
Nonsteroidal antiinflammatory drugs (NSAIDs) are available in multiple formulations (e.g., oral, suppository, and transdermal) for the control of various pain disorders such as low back pain |
No systemically acting transdermal formulations of NSAIDs are available for the control of low back pain |
Systemically acting diclofenac sodium patch 75 mg and 150 mg was hypothesized to be superior to a placebo patch and to be safe |
What was learned from the study? |
This study demonstrated the superiority of diclofenac sodium patch 75 mg and 150 mg over placebo in controlling low back pain in Japanese patients, and showed that the patch is effective even when not applied to the target site, unlike locally acting formulations, so dosing is simple and the burden is not on one area of the skin |
There were no significant safety concerns, such as gastrointestinal toxicity or skin irritation, with diclofenac sodium patch |
Introduction
Nonsteroidal antiinflammatory drugs (NSAIDs) are commonly used as a pain control treatment for pain disorders such as low back pain [1,2,3,4]. They are available in multiple formulations (e.g., oral, suppository, and transdermal) [5,6,7]. Oral formulations can be administered by simple procedures, although the timing of dosing in relation to meals should be considered; it is often recommended to avoid consumption without food intake [8]. In addition, because of muscular weakness, older people often have trouble in swallowing, which may contraindicate the use of oral formulations in this population [9, 10]. Rectal suppositories enable rapid drug absorption (via the rectal mucosa) that is unaffected by food intake and can be used safely even in older patients [11]. However, they are not suitable for people with diarrhea because the suppository needs to be kept in place for several minutes to allow the drug to be released and absorbed [11]. In addition, some patients, especially those who are older or otherwise have reduced activities of daily living, often need someone else’s help to insert rectal suppositories and may thus experience distress because they perceive themselves as a burden to others. Transdermal formulations eliminate the effect of food on drug absorption and can be administered even in patients who have difficulty taking drugs by mouth [7]. All existing transdermal formulations of NSAIDs have a much lower potential of causing gastrointestinal and other toxicities compared with oral formulations; however, they act locally and always need to be applied to the target site, potentially causing physical skin irritation (e.g., contact dermatitis) due to their repeated application and, in case of the patch, removal [12].
To date, systemically acting transdermal NSAID formulations have not been available for controlling pain such as low back pain. Recently, a new systemically acting, once-daily transdermal formulation of diclofenac sodium (diclofenac sodium patch) was approved for the control of cancer-related pain in Japan. The NSAID diclofenac sodium exerts analgesic and antiinflammatory effects by inhibiting cyclooxygenase [13].
Therefore, we hypothesized that a systemically acting diclofenac sodium patch would also be useful in controlling low back pain and evaluated its efficacy in low back pain in a randomized controlled study. In a phase III study, Japanese patients with low back pain were randomized to receive a 75 mg or 150 mg diclofenac sodium patch or placebo once daily for 2 weeks. The primary efficacy endpoint was visual analog scale (VAS) score. Safety was also evaluated by assessing adverse events. The diclofenac sodium patch used in this study is a matrix patch formulation containing 75 mg of diclofenac sodium per 70 cm2 (7 × 10 cm).
The diclofenac sodium patch enables transdermal absorption of the drug and therefore can be administered even in patients who have difficulty swallowing or are at risk of aspiration, and without regard to the effect of food on its absorption. This formulation allows the drug to be distributed via the systemic circulation to the location where an analgesic effect is required. Therefore, unlike locally acting formulations, the patch need not be applied to the target site, so dosing is simple and the burden is not on one area of the skin. These advantages of the diclofenac sodium patch, which are lacking in existing NSAID formulations, may make it a novel systemic NSAID option for the control of pain disorders such as low back pain.
Methods
This randomized, double-blind, placebo-controlled, parallel-group, multicenter study was conducted from February 2020 to September 2020 at 75 Japanese institutions (72 of which formally enrolled participants). The study ended after inclusion of the planned number of participants.
The study was performed in compliance with the Declaration of Helsinki of 1964 and its later amendments, and the Good Clinical Practice (GCP) guidelines. The 75 participating institutions acquired approval of the protocol from one of the following institutional review boards: Shinagawa East One Medical Clinic Institutional Review Board; Sugiura Clinic Institutional Review Board; and Jimbo Orthopedics Institutional Review Board. Prior to enrollment, all participants provided written informed consent to participate in the study. Throughout the study period, no ethical problems or medical malpractice occurred, and the participants’ identities were kept confidential. The study was registered with the Japan Primary Registries Network (JPRN) as JPRN-JapicCTI-205134.
Patients
Japanese patients aged 20 years or older were eligible for the study if they had been diagnosed with low back pain at least 12 weeks before giving informed consent and had received any NSAID or acetaminophen for pain control without any dose modification for at least 4 weeks. Those with low back pain related to any organic disease, fracture, trauma, infection, rheumatoid arthritis, or neoplasm were ineligible for the study. Other main exclusion criteria included the following: (1) prior or scheduled surgery for low back pain by the end of the treatment period; (2) any underlying condition associated with radiating pain, numbness, or paralysis extending to the knee(s); (3) presence of pain related to any concomitant illness that would preclude proper assessment of low back pain; (4) significant blood dyscrasia, liver disease, renal disease, hypertension, cardiac dysfunction, or any other clinically significant concomitant illness; (5) any malignancy; (6) peptic ulcer; (7) presence or history of aspirin-induced asthma; (8) history of allergy to NSAIDs; (9) confirmed or potential pregnancy, postpartum state, or breastfeeding; (10) known skin allergy to external medicines or tapes such as plasters; (11) frequent sunbathing or skin abnormality, tattoo, or nevi that would prevent the application of patches.
Study Design
An overview of the study design is shown in Fig. 1. The study consisted of a 1-week washout period, a 1-week observation period, and a 2-week treatment period. After a 1-week washout of the prior analgesic treatment (NSAID or acetaminophen), during the observation period patients applied two placebo patches once daily for 1 week in a single-blind manner. Acceptable sites of application included the chest, abdomen, upper arm, upper and mid back, low back, and thigh. In principle, a different site from that used on the previous day was to be used. Patients assessed their low back pain daily from the start of the washout period until the end of the study by using a 100-mm VAS. The study protocol did not include the use of rescue medication for pain during the study.

Overview of study design
At the end of the observation period, each patient was assessed for eligibility by the investigator. Those confirmed to be eligible by the investigator and the participant enrollment center were formally enrolled and randomized by dynamic allocation in a 1:1:2 ratio to receive diclofenac sodium patch 75 mg, diclofenac sodium patch 150 mg, or placebo patch, respectively. All patches were provided by Hisamitsu Pharmaceutical Co., Inc, Tokyo, Japan. The participant enrollment center performed randomization by its pseudorandom number generator-based allocation system with dynamic allocation procedures that balanced treatment arms for mean pain VAS score over the 3 days immediately before starting the treatment period. During the treatment period, patients applied diclofenac sodium patch 75 mg, diclofenac sodium patch 150 mg, or placebo patch once daily for 2 weeks in a double-blind manner. To maintain blindness, those allocated to receive diclofenac sodium patch 75 mg (75 mg group) applied one diclofenac sodium patch plus one placebo patch; those allocated to receive diclofenac sodium patch 150 mg (150 mg group), two diclofenac sodium patches; and those allocated to receive placebo, two placebo patches. The patches were the same size and were identical in terms of appearance and smell. All patients, investigators, monitors, and the study sponsor were blinded to treatment allocation until the end of the study.
Efficacy and Safety Assessments
The primary endpoint was pain intensity assessed as the score on the VAS. Patients recorded the daily mean intensity of their pain at the site of interest (low back) on the VAS. The primary analysis variable was absolute change from baseline (start of the treatment period) in mean 3-day pain VAS score after 2 weeks of treatment. Secondary analysis variables were absolute change from baseline in mean 3-day pain VAS score after 1 week of treatment, proportion of patients achieving a reduction in mean 3-day pain VAS score of at least 50% from baseline, and day-by-day changes in pain VAS score. Secondary endpoints of the study included absolute change in Roland–Morris Disability Questionnaire (RDQ) score [14], degree of patient satisfaction, and global improvement rating. To determine the degree of patient satisfaction, patients rated how satisfied they were with the analgesic treatment for their low back pain in the past week by using five categories: “very satisfied,” “satisfied,” “neither satisfied nor unsatisfied,” “unsatisfied,” and “very unsatisfied.” Global improvement rated by the investigator by using five categories: “much improved,” “improved,” “unchanged,” “aggravated,” and “very aggravated”; the rating was based on a combined assessment of changes from baseline in pain VAS score and RDQ score, the degree of patient satisfaction, and physical findings.
Safety measures included adverse events (AEs), safety laboratory data, vital sign measurements, and 12-lead electrocardiography (ECG) findings.
Statistical Analyses
The planned sample size of this study was 480 patients in total (formally enrolled in the treatment period), including 240 in the placebo group and 120 in each diclofenac sodium patch dose group. This sample size would provide a power of 80% to simultaneously show the superiority of both doses of the active treatment over placebo at a two-tailed alpha error rate of 5% by using the two-sample t-test, as calculated from the Monte Carlo simulation of 1000 runs with the following assumptions: for the absolute change from baseline in mean 3-day pain VAS score after 2 weeks of treatment, the difference from the placebo group was assumed to be −6 mm for the 75 mg group and the difference from the 75 mg group was assumed to be −1 mm for the 150 mg group, with a standard deviation of 18 mm in all groups. These assumptions were based on the results of a previous, unpublished double-blind, placebo-controlled study on diclofenac sodium patch in Japanese patients with low back pain (JPRN-JapicCTI-153012). In that study, in which values for dropouts were imputed as those observed at the end of the washout period, analysis of covariance (ANCOVA) with treatment as a factor and baseline mean 3-day pain VAS score as a covariate showed a treatment difference of −7.30 mm [95% confidence interval (CI) −11.04 to −3.55 mm] in absolute change in mean 3-day pain VAS score after 2 weeks of treatment with diclofenac sodium patch 75 mg with a standard deviation of 17.7 mm for the diclofenac sodium patch group and 15.4 mm for the placebo group.
The full analysis set (FAS) was used to analyze efficacy and comprised all patients enrolled in the study apart from those who were noncompliant with GCP and those with no assessable efficacy data at baseline or after randomization. The safety analysis set comprised all patients who received at least one dose of the study drug.
In the primary analysis of the primary endpoint, which evaluated whether diclofenac sodium patch 75 mg and 150 mg were superior to placebo, data on absolute change from baseline in mean 3-day pain VAS score after 2 weeks of treatment were analyzed by an ANCOVA model that included treatment and baseline mean 3-day pain VAS score as explanatory variables. Mean 3-day pain VAS score was calculated as the mean of the VAS scores on the 3 days immediately before each specified visit. Missing values for dropouts were imputed as the mean 3-day pain VAS score immediately before the end of the washout period. Comparisons were made within each pair of active and placebo treatments at a two-tailed alpha error rate of 5%. First, a fixed sequence procedure was used for a paired comparison between the 150 mg group and the placebo group; then, if this comparison revealed a statistically significant difference, the 75 mg group was compared with the placebo group.
As a secondary analysis, absolute change from baseline in mean 3-day pain VAS score after 1 week of treatment was analyzed by a similar method to that used for the primary analysis. Multiplicity adjustments with fixed sequence procedures were not performed. With regard to the proportion of patients achieving a reduction from baseline of greater than or equal to 50% in mean 3-day pain VAS score, treatment difference and 95% CI were calculated by Wilson’s score method. Day-to-day changes in pain VAS score were analyzed with a mixed-effect model for repeated measures (MMRM) with an unstructured covariance matrix that included treatment, time, and treatment-by-time interaction as fixed effects and baseline mean 3-day pain VAS score as a covariate.
Statistical analyses were performed with SAS ver. 9.4. AEs were coded with system organ classes (SOCs), and preferred terms (PTs), with MedDRA Ver. 23.1.
Results
Patient Disposition and Baseline Characteristics
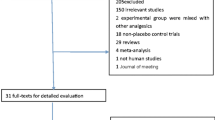
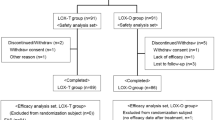
Of 974 patients screened, 538 were enrolled in the treatment period and randomized to the 75 mg group (n = 136), 150 mg group (n = 135), or placebo group (n = 267). All randomized patients received at least one dose of the study drug, but four of them (two in the 75 mg group and two in the placebo group) discontinued the study. The remaining 534 patients (134 in the 75 mg group, 135 in the 150 mg group, and 265 in the placebo group) completed the treatment period (Fig. 2). All 538 randomized patients were included in the FAS and safety analysis set in their original assigned group.

Patient disposition
In the FAS, the three treatment groups were well balanced with regard to demographic and baseline characteristics (Table 1). Among the acceptable sites of drug application (chest, abdomen, upper arm, upper and mid back, low back, and thigh), the low back (where pain intensity was assessed) was chosen as the application site in 983 of 3762 patches (26.1%) in the 75 mg group, 888 of 3763 patches (23.6%) in the 150 mg group, and 1756 of 7383 patches (23.8%) in the placebo group.
Efficacy
Table 2 summarizes the efficacy results in the FAS. The primary analysis of the primary endpoint (pain VAS score) showed the superiority of diclofenac sodium patch 150 mg over placebo: The difference between the 150 mg and placebo groups in terms of least-squares (LS) mean absolute change from baseline in mean 3-day pain VAS score after 2 weeks of treatment was −5.67 mm (95% CI −9.34 to −2.00 mm; p = 0.0025, ANCOVA). The analysis also showed superiority of diclofenac sodium patch 75 mg over placebo in terms of this efficacy variable: The treatment difference in LS mean was −5.68 mm (95% CI −9.34 to −2.01 mm; p = 0.0024, ANCOVA).
Secondary analyses also revealed greater reductions from baseline in mean 3-day pain VAS score after 1 week of treatment in both the 75 mg and 150 mg groups than in the placebo group (Table 2). Figure 3 shows the mean 3-day pain VAS scores at baseline and weeks 1 and 2. For the proportion of patients achieving a reduction in mean 3-day pain VAS score greater than or equal to 50% from baseline, after 2 weeks of treatment the between-group difference (95% CI, calculated by Wilson’s score method) compared with placebo was 8.4% (0.4–17.2%) in the 75 mg group and 14.9% (6.3–24.0%) in the 150 mg group (Table 2). Day-to-day changes in pain VAS score over time are shown in Fig. 4. The between-group comparison of day-to-day changes in pain VAS score from baseline revealed that the 75 mg and 150 mg groups differed from the placebo group by −2.69 mm (95% CI −5.02 to −0.36 mm) and −3.46 mm (95% CI −5.79 to −1.12 mm), respectively, at day 2 (p = 0.0235 and p = 0.0038, respectively, MMRM) and by −4.84 mm (95% CI −8.86 to −0.82 mm) and −5.51 mm (95% CI −9.51 to −1.51 mm), respectively, at day 14 (p = 0.0184 and p = 0.0070, respectively, MMRM). Thus, the 75 mg and 150 mg groups achieved significantly greater reductions in pain VAS score as compared with the placebo group every day from the second through the 14th day of treatment.

Time course plot of the 3-day mean pain visual analog scale score. Data are mean ± SD. VAS visual analog scale. ◆ 75 mg diclofenac sodium patch group, ● 150 mg diclofenac sodium patch group, ○ Placebo patch group

Time course plot of change in the daily pain visual analog scale score from baseline by mixed-effect model for repeated measures. Data are mean ± SD. VAS visual analog scale. ◆ 75 mg diclofenac sodium patch group, ● 150 mg diclofenac sodium patch group, ○ Placebo patch group
Compared with the placebo group, both diclofenac sodium patch dose groups achieved better results with regard to secondary efficacy endpoints, i.e., absolute change in RDQ score, the proportion of patients who were “very satisfied” or “satisfied” with their analgesic treatment, and the proportion of patients with a global improvement rating of “much improved” or “improved” (Table 2).
Safety
AEs occurred in 37/136 patients (27.2%) in the 75 mg group, 40/135 patients (29.6%) in the 150 mg group, and 75/267 patients (28.1%) in the placebo group (Table 3). These AEs were treatment related in 19/136 patients (14.0%), 17/135 patients (12.6%), and 51/267 patients (19.1%) in the respective treatment groups. Blood in the urine (reported in 3.7% of patients in the 75 mg group, 4.4% of patients in the 150 mg group, and 1.5% of patients in the placebo group) was the only AE that occurred at a higher frequency (≥ 2%) in the active treatment (75 mg or 150 mg) group than in the placebo group. Most of the AEs reported were of mild intensity, and no serious AEs occurred.
Application site AEs occurred in 9/136 patients (6.6%) in the 75 mg group, 4/135 patients (3.0%) in the 150 mg group, and 39/267 patients (14.6%) in the placebo group. All application-site AEs were considered to be treatment related but all of them were of mild intensity.
Descriptive statistics of safety laboratory data and vital sign measurements showed no marked changes from baseline at any specified time in any treatment group. The proportion of patients with any abnormal 12-lead ECG finding was similar at all specified times as compared with baseline in all treatment groups.
Discussion
This study demonstrated that diclofenac sodium patch, a systemic transdermal formulation of diclofenac sodium, was effective and safe for the control of low back pain. At both the 75 mg and 150 mg doses, diclofenac sodium patch significantly relieved low back pain as compared with placebo, i.e., it resulted in greater changes from baseline in pain intensity assessed on a pain VAS score (primary endpoint) after 2 weeks of treatment. Compared with placebo, both doses of this new formulation were also shown to significantly relieve low back pain in terms of absolute change from baseline in pain VAS score after 1 week of treatment. The day-by-day changes in pain VAS score were also greater with both doses of the active treatment than with placebo from the second day of treatment onward, indicating rapid pain relief after the start of administration of diclofenac sodium patch. Although this study was not designed to directly compare the two doses of diclofenac sodium patch, changes from baseline in pain VAS score indicated a slightly greater pain relief after 1 week of treatment at 150 mg/day than at 75 mg/day. In the early phase of treatment, the changes from baseline in pain VAS score over time (Fig. 4) were slightly greater at 150 mg/day than at 75 mg/day, suggesting a tendency towards a dose-dependent pain relief. Compared with patients treated with placebo, a numerically (but not significantly) higher proportion of patients treated with 75 mg/day diclofenac sodium and a considerably higher proportion of patients treated with 150 mg/day diclofenac sodium achieved a reduction from baseline of greater than or equal to 50% in pain VAS score after 2 weeks of treatment. For the secondary endpoints (RDQ score, patient satisfaction, and global improvement rating), results were generally better with diclofenac sodium patch than with placebo, supporting the primary endpoint results. Thus, from the aspect of efficacy, diclofenac sodium patch is useful for the control of low back pain at both 75 mg and 150 mg once daily dosages.
Concerning safety, no AEs were much more frequent in patients treated with the diclofenac sodium patch at either dose than in those receiving the placebo patch. All of the administration site reactions were characteristic for the use of patches and were of mild intensity. Diclofenac sodium patch is a systemically acting formulation of diclofenac sodium that need not always be applied at the target site, unlike locally acting formulations. Because it can be applied randomly to accessible skin sites, occurrence of administration site reactions is less likely to require discontinuation of its use. The other AEs reported in patients treated with diclofenac sodium patch were AEs that are known from existing formulations of diclofenac sodium. Gastrointestinal, hepatic, renal, and cardiovascular AEs that are of special concern with NSAID use [15,16,17] were not more frequent (i.e., not ≥ 2% more frequent) in patients treated with diclofenac sodium patch at 75 or 150 mg/day than in those receiving placebo. Most of the reported AEs were of mild intensity, and no serious AEs occurred. These results indicate that there are no clinically significant safety concerns with daily treatment with diclofenac sodium patch for 2 weeks.
A pharmacokinetic study of diclofenac sodium patch showed that the steady-state Cmax during repeated daily administration at 225 mg/day, a higher dose than used in this study, was lower than that achieved with repeated oral doses of 25 mg diclofenac sodium (the minimum dose that can be administered orally as tablets) [18]. In that study, the relative bioavailability of the drug achieved after administration of diclofenac sodium patch 150 mg was estimated to be about 59% of that achieved after oral administration of 100 mg diclofenac sodium (the maximum dose that can be administered orally as tablets). Even though the achievable Cmax was lower with diclofenac sodium patch than with orally administered diclofenac sodium, in the present study the systemically acting transdermal patch formulation was shown to be effective for the control of low back pain. This effect may be associated with pharmacokinetic advantages of systemically acting transdermal patches over oral formulations, such as a slower elevation of blood drug levels, a smaller peak-to-trough ratio, and more sustained effective plasma drug levels [19, 20]. Although its clinical safety should be evaluated further, diclofenac sodium patch may not be associated with higher risks for gastrointestinal, hepatic, renal, or cardiovascular AEs, effects that are of special concern with NSAID use because of the lower Cmax and smaller area under the curve achieved as compared with oral formulations. A long-term study of diclofenac sodium patch in patients treated with 150 mg/day for low back pain for up to 52 weeks found no tendency towards a higher overall incidence of AEs in patients treated for longer [21]. No individual AEs, including those of special concern with NSAID use (e.g., gastrointestinal AEs), became more frequent as the duration of treatment increased. Serum creatinine level, an important parameter of renal function, did not change considerably over time during treatment with diclofenac sodium patch.
Diclofenac sodium patch, which is designed to enable transdermal absorption of the drug, may cause fewer gastrointestinal AEs oral formulations because, unlike oral formulations, the drug is not taken up into gastrointestinal mucosa. The way in which different routes of administration affect the incidence of gastrointestinal toxicities remains to be studied in the future.
This study has several limitations of generalizability. First, the cohort may have been enriched for those with pain that is more responsive to analgesics because to be eligible for enrollment in the study, patients had to have gained some pain control with any NSAID or acetaminophen. Second, this study evaluated the efficacy and safety of diclofenac sodium patch administered for only 2 weeks and did not provide evidence for its efficacy or safety in patients treated on a long-term basis. Nonetheless, another study evaluated long-term use of the patch and confirmed its safety and efficacy after administration for 52 weeks [21].
Conclusion
In Japanese patients with low back pain, diclofenac sodium patch 75 mg and 150 mg administered once daily for 2 weeks has an adequate analgesic effect and is well tolerated. This systemically acting patch can be safely administered even to patients with trouble swallowing or who are at risk of aspiration without regard to the effect of food on drug absorption. Unlike locally acting formulations, the patch need not always be applied to the target site, so dosing is simple and the burden is not on one area of the skin. These advantages of the diclofenac sodium patch may make it a novel systemic NSAID option for pain control in low back pain.
References
Koes BW, van Tulder M, Lin CW, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur Spine J. 2010;19(12):2075–94.
Oliveira CB, Maher CG, Pinto RZ, et al. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. Eur Spine J. 2018;27(11):2791–803.
Wong JJ, Cote P, Sutton DA, et al. Clinical practice guidelines for the noninvasive management of low back pain: a systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Eur J Pain. 2017;21(2):201–16.
Price MR, Cupler ZA, Hawk C, Bednarz EM, Walters SA, Daniels CJ. Systematic review of guideline-recommended medications prescribed for treatment of low back pain. Chiropr Man Ther. 2022;30(1):26.
Altman R, Bosch B, Brune K, Patrignani P, Young C. Advances in NSAID development: evolution of diclofenac products using pharmaceutical technology. Drugs. 2015;75(8):859–77.
Lipscomb GR, Rees WD. Gastric mucosal injury and adaptation to oral and rectal administration of naproxen. Aliment Pharmacol Ther. 1996;10(2):133–8.
Leppert W, Malec-Milewska M, Zajaczkowska R, Wordliczek J. Transdermal and topical drug administration in the treatment of pain. Molecules. 2018;23(3):681.
Martinez MN, Amidon GL. A mechanistic approach to understanding the factors affecting drug absorption: a review of fundamentals. J Clin Pharmacol. 2002;42(6):620–43.
Aslam M, Vaezi MF. Dysphagia in the elderly. Gastroenterol Hepatol. 2013;9(12):784–95.
Kappelle WF, Siersema PD, Bogte A, Vleggaar FP. Challenges in oral drug delivery in patients with esophageal dysphagia. Expert Opin Drug Deliv. 2016;13(5):645–58.
De Boer AG, De Leede LG, Breimer DD. Drug absorption by sublingual and rectal routes. Br J Anaesth. 1984;56(1):69–82.
Ball AM, Smith KM. Optimizing transdermal drug therapy. Am J Health Syst Pharm. 2008;65(14):1337–46.
Gan TJ. Diclofenac: an update on its mechanism of action and safety profile. Curr Med Res Opin. 2010;26(7):1715–31.
Smeets R, Koke A, Lin CW, Ferreira M, Demoulin C. Measures of function in low back pain/disorders. Arthritis Care Res. 2011;63(Suppl 11):S158–73.
Marcén B, Sostres C, Lanas A. NSAID and gastrointestinal risk. Aten Primaria. 2016;48(2):73–6.
Cooper C, Chapurlat R, Al-Daghri N, et al. Safety of oral non-selective non-steroidal anti-inflammatory drugs in osteoarthritis: what does the literature say? Drugs Aging. 2019;36(Suppl 1):15–24.
Prescott LF. Liver damage with non-narcotic analgesics. Med Toxicol. 1986;1(Suppl 1):44–56.
Uchida E, Terahara T, Okawa K, Takahashi E. Pharmacokinetics of diclofenac sodium patch (HP-3150) for relief of cancer pain. Jpn J Med Pharm Sci. 2021;78:741–58 (translated from Japanese).
Shingade GM, Aamer Q, Sabale PM, et al. Review on: Recent trend on transdermal drug delivery system. J Drug Deliv Ther. 2012;2(1):66–75.
Margetts L, Sawyer R. Transdermal drug delivery: principles and opioid therapy. Contin Educ Anaesth Crit Care Pain. 2007;7(5):171–6.
Taguchi T, Yamaguchi S, Terahara T, Okawa K, Inakura H, Nohara Y. Safety of long-term administration of a systemic-acting diclofenac sodium patch (HP-3150) in Japanese patients with low back pain. Jpn Pharmacol Ther. 2022;50(2):213–27.
Acknowledgements
The authors would like to thank the patients who participated in this study, their families, and the staff at all study sites.
Funding
This study and the journal’s Rapid Service Fee were funded by the Hisamitsu Pharmaceutical Co., Inc., Tokyo, Japan.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Toshihiko Taguchi and Shigeki Yamaguchi, who are medical advisers, gave advice with the study design, conduct of the study, and interpretation of the data. Takaaki Terahara, Koji Okawa and Hiroshi Inakura contributed to the study concept and design, the conduct of the study, and data analysis and interpretation. All authors approved the version of the manuscript to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy of integrity of any part of the work are appropriately investigated and resolved.
Disclosures
Toshihiko Taguchi and Shigeki Yamaguchi received medical consultant fees from Hisamitsu Pharmaceutical Co., Inc. Shigeki Yamaguchi received honoraria from The Nakatomi Foundation. Takaaki Terahara, Koji Okawa and Hiroshi Inakura are employees of Hisamitsu Pharmaceutical Co., Inc., Tokyo, Japan.
Compliance with Ethics Guidelines
This study was conducted in compliance with the Declaration of Helsinki of 1964 and its later amendments and Good Clinical Practice guidelines. The 75 participating institutions acquired approval of the protocol from one of the following institutional review boards: Shinagawa East One Medical Clinic Institutional Review Board; Sugiura Clinic Institutional Review Board; and Jimbo Orthopedics Institutional Review Board. Prior to enrollment, all participants provided written informed consent to participate in the study. Throughout the study period, no ethical problems or medical malpractice occurred, and the participants’ identities were kept confidential. The study was registered with the Japan Primary Registries Network (JPRN) as JPRN-JapicCTI-205134.
Data Availability
The datasets generated during and/or analyzed during the current study are not publicly available because the data are confidential and proprietary to Hisamitsu Pharmaceutical Co., Inc.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Taguchi, T., Yamaguchi, S., Terahara, T. et al. Systemically Acting Diclofenac Sodium Patch for Control of Low Back Pain: A Randomized, Double-Blind, Placebo-Controlled Study in Japan. Pain Ther 12, 529–542 (2023). https://doi.org/10.1007/s40122-023-00478-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40122-023-00478-1