
Abstract
Introduction
Amorolfine 5% lacquer is an established topical treatment for fungal infection of the nails. The success of topical therapy for onychomycosis depends on whether the permeated drug concentration in the deep nail bed is retained above the effective antifungal minimum inhibitory concentration (MIC). We compared the penetration profile of amorolfine and a new topical formula of terbinafine in human mycotic toenails using matrix-assisted laser desorption ionization mass spectrometry imaging–Fourier transform ion cyclotron resonance (MALDI-FTICR) imaging.
Methods
Amorolfine 5% lacquer and terbinafine 7.8% lacquer were applied to mycotic nails (n = 17); nail sections were prepared, and MALDI-FTICR analysis was performed. Based on the MICs of amorolfine and terbinafine needed to kill 90% (MIC90) of Trichophyton rubrum, the fold differences between the MIC90 and the antifungal concentrations in the nails (the multiplicity of the MIC90) were calculated overall and for the keratin-unbound fractions.
Results
Both amorolfine and terbinafine penetrated the entire thickness of the nail. The mean concentration across the entire nail section 3 h following terbinafine treatment was 1414 μg/g of tissue (equivalent to 4.9 mM) compared with 780 μg/g (2.5 mM) following amorolfine treatment (not significantly different; p = 0.878). The median multiplicity of the MIC90 was significantly higher in amorolfine- than terbinafine-treated nails overall (191 vs. 48; p = 0.010) and for the keratin-unbound fractions only (7.4 vs. 0.8; p = 0.002).
Conclusion
In this ex vivo study, MALDI-FTICR demonstrated that, although amorolfine 5% and terbinafine 7.8% had similar distribution profiles, both penetrating from the surface to the nail bed, the concentration of amorolfine in the nail was significantly higher than that of terbinafine relative to their respective MIC90 values. Clinical studies are required to determine whether these effects translate to a clinical difference in treatment success.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
The success of topical therapy for onychomycosis depends on whether the permeated drug concentration deep in the nail bed is retained above the antifungal minimum inhibitory concentration. |
In this study, matrix-assisted laser desorption ionization mass spectrometry imaging–Fourier transform ion cyclotron resonance (MALDI-FTICR) imaging was used to compare the penetration profile of amorolfine and terbinafine. |
What was learned from the study? |
Despite similar distribution profiles, amorolfine attained a significantly higher multiple of its minimum inhibitory concentration toward Trichophyton rubrum compared with terbinafine. |
MALDI-FTICR was successfully used to evaluate the penetration of amorolfine and terbinafine into the nail plate. |
Clinical trials are needed to evaluate whether the observed differences in effective concentration in the nail translate to a clinical difference in treatment efficacy between amorolfine and terbinafine. |
Introduction
Toenail onychomycosis is a common problem and the most difficult superficial fungal infection to cure [1]. The majority of cases are caused by Trichophyton rubrum, which invades the nail bed under the nail plate [1, 2], leading to discoloration of the nail plate, brittleness, and nail thickening [3]. In more severe cases, this can result in loss of the nail plate altogether. More widespread fungal lesions that spread to other nails and other parts of the body such as the skin and scalp, as well as to other family members, may also occur as a result of onychomycosis [3, 4].
Treatment approaches include oral and/or topical treatments [1]. Oral treatment is associated with adverse systemic side effects, long treatment times, and low levels of drug distribution to the site of infection as a result of limited local blood circulation [1, 2]. Topical treatment has, therefore, gained attention in recent years [1].
Drug penetration into the nail plate is not, however, straightforward, and it is a significant factor limiting the effectiveness of these topical treatments [1]. Several variables can affect drug penetration, including its molecular weight and hydrophilicity/lipophilicity, the pH and nature of the vehicle transporting the drug, and the solute charge [5]. Evidence also points to the influence of keratin, which binds many antifungal agents and limits their antifungal activity [2].
Matrix-assisted laser desorption ionization–mass spectrometry imaging (MALDI-MSI) has shown that amorolfine has a more homogeneous distribution and a better penetration profile in infected nails than ciclopirox or naftifine [6]; however, to our knowledge, there have been no similar comparisons between amorolfine and terbinafine. Therefore, the present study aimed to quantify the distribution and penetration profile of terbinafine compared with amorolfine after topical application in mycotic human toenails, using MALDI–Fourier transform ion cyclotron resonance (MALDI-FTICR) imaging.
Methods
Samples
The samples used in these studies were sourced and deidentified via Tissue Solutions Ltd., a subsidiary of BioIVT LLC which is accredited for the collection, storage, and commercial distribution of biospecimens by the Office for Human Research Protections (OHRP) of the United States Department of Health. The use of publicly available biospecimens from an accredited supplier is not considered to fall under research in human subjects, and as such, institutional review board (IRB) approval or exemption was not required. Before analysis, the toenails (n = 17), which had been frozen for storage, were thawed for 10 min at room temperature, immersed for 1 min in 70% (v/v) ethanol, and washed twice by vortexing with deionized water. The thickness of each toenail sample was measured in five different areas with an Oditest caliper (Kroeplin GmbH, Schlüchtern, Germany) prior to treatment.
Sample Treatment
The antifungal compounds tested were amorolfine (Loceryl® 5% lacquer) and terfenadine (Terbinafine-1A Pharma®, 7.8% equivalent). For treatment, each toenail was laid on gauze moistened with sterile water in a petri dish. One antifungal was applied at 10 µL/cm2 within a 1-cm2 pre-marked zone on the nail surface. The nails were then air-dried for 30 min at 24 °C in a humid cell incubator, after which the toenail surfaces were cleaned with five cotton swabs wetted with acetone. The samples were then stored at −80°C.
Sample Sectioning and Mounting
Nails stored at −80°C were placed inside a cryostat maintained at −20°C, and 10-µm nail sections were prepared for each sample. The midline cross sections of the toenails (region of interest) were mounted onto adhesive tape and placed on a MALDI plate. The mounted nail sections were then placed in a desiccator prior to matrix deposition to ensure the sections were dry. An optical image of the plate was acquired with a scanner to synchronize positions of the nail sections with the laser target.
Preparation of the Antifungal Dilution Series
Stock solutions of amorolfine and terbinafine were prepared in ethanol/water 50:50 (v:v). A dilution series of each antifungal was then prepared by diluting the stock solutions in a 1:1 (v:v) solution of ethanol and water; 1.0 μL of each dilution was spotted directly onto adhesive tape and placed in a desiccator for 15 min before MALDI matrix deposition. A spot of pure solvent was included as a negative control. The spotted calibration series was later placed onto the slides near the sections for image calibration.
MALDI-FTICR Analysis
For MALDI-FTICR analysis, 2,5-dihydroxybenzoic acid matrix (DHB; 40 mg/mL in 1:1 methanol/water + 1% trifluoroacetic acid) was sprayed over the toenail sections with an automatic sprayer system (TM-Sprayer; HTX Technologies, Chapel Hill, NC, USA). The nail sections were then analyzed with a 7 T MALDI-FTICR instrument (SolariX; Bruker, Billerica, MA, USA) in the continuous accumulation of selected ions (CASI) positive mode centered on a mass range (m/z) at a spatial resolution of either 70 μm to cover the entire nail section or 200 μm for the dilution series to generate the calibration curves. All MSI acquisitions were performed with data reduction set between 0.30 and 0.50 (this was kept consistent between images of nails treated with the same antifungal), and one image was acquired per nail.
For comparison of the amorolfine and terbinafine distribution profiles after 3 h, 16 nails (n = 8 per antifungal agent) were evaluated, and one control sample was used as a reference. The control nails were used to evaluate the tissue extinction coefficients (TEC) [7] of the antifungals for normalization. For this purpose, each antifungal was sprayed at a concentration of 5 μM on the top of a control nail section and next to the nail section (directly onto the adhesive tape). Signals detected in the nail section were then compared to the signal beside the tissue section to determine the TEC.
Data Analysis
The MALDI-FTICR data were analyzed with the FlexImaging v.5.0 (Bruker), DataAnalysis v.5.0 (Bruker), and Multimaging v1.2 (Aliri, Loos, France) software packages. When evaluating antifungal distribution, the intensity scale was adjusted to eliminate the background noise (by increasing the lower threshold) and enable optimal visualization (by decreasing the upper threshold). Convolution of the signal distributions was performed on the original images using a normalized uniform kernel that averaged the values around a position. The kernel size was manually optimized for the analysis to minimize background noise.
The MSI datasets obtained from the nail sections and the dilution series were used for the absolute quantification of the antifungals within the nail sections. The TEC-based method in the Multimaging software was applied to these data to correct the signal in each region of interest and obtain the concentrations in μg/g of tissue.
To quantitatively evaluate the penetration of the test item through the nail samples, penetration profiles were generated for each treated nail section. The methodology was based on the following workflow: (1) the molecular distribution of the test item was first obtained by MSI as described above; (2) the region of interest for the penetration profile was selected (this was generally the entire region of acquisition, unless undesired features present, such as contamination, bad histology, or folding of the sections, would significantly impact the results; (3) each pixel in the region of interest was re-aligned to define a common 0-μm position on the top of the nail section; (4) the mean concentration per raw pixel was calculated according to the quantitative MSI results, and the depth was determined based on the spatial resolution for the acquisition (70 μm for each pixel); and (5) penetration profiles were then generated using the quantification and depth data.
Based on published data on the minimum inhibitory concentration (MIC) required to inhibit 50% and 90% (MIC50 and MIC90) of Trichophyton rubrum, the fold differences between the MIC and the antifungal concentrations in the nails (termed the multiplicity of MIC) were calculated for each. The published MIC50 and MIC90 values (in µM) used for these calculations were 0.79 and 12.60 for amorolfine, and 0.11 and 54.90 for terbinafine, respectively [8]. Antifungal concentrations in the nail were normalized based on published drug-free (keratin unbound) ratios of 3.9% for amorolfine and 1.8% for terbinafine [2].
Statistical Analysis
The Shapiro–Wilk test was used to check the assumption of normality of data within groups. The Kruskal–Wallis H test was used to test for statistically significant differences across groups. When testing for statistically significant differences between groups two by two, the Student t test was used where data were normally distributed, and the Mann–Whitney U test was used where data were not normally distributed. A p value of < 0.05 was considered statistically significant. Python v3.8 (Python Software Foundation, Beaverton, OR, USA) was used for all statistical analyses.
Results
Distribution and Penetration of Amorolfine and Terbinafine
Not accounting for the different concentrations of the two antifungal agents applied to the nails, the mean absolute concentration within the toenails at 3 h was 1414 μg/g of tissue for terbinafine (equivalent to 4.9 mM) and 780 μg/g for amorolfine (equivalent to 2.5 mM; Table 1). One nail (nail 7 in Table 1 [mean thickness 5.0 mm]) was brittle and exhibited a substantially more homogeneous distribution and the deepest penetration of terbinafine in the nail bed compared with other samples. The difference between the mean concentrations of terbinafine and amorolfine was not significant (p = 0.878; Fig. 1).

Total amorolfine and terbinafine concentrations (mM) across entire nail plate sections (n = 8 each) 3 h after application of 5.0% and 7.8% lacquer, respectively, as detected by MALDI-FTICR. Boxplots indicate the median (horizontal bars), mean (crosses), and interquartile range (25th to 75th percentile), and the whiskers show the maximum and minimum, excluding the outlier for terbinafine (terbinafine nail #7). MALDI-FTICR, matrix-assisted laser desorption ionization–Fourier transform ion cyclotron resonance
Multiplicity of MIC90 of Amorolfine and Terbinafine in the Nail Following Treatment
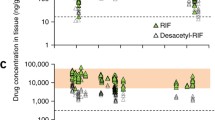
Relative to their respective MIC50 values, the median concentrations of amorolfine and terbinafine in the nail were 3039- and 23,817-fold, whereas the median concentrations of amorolfine and terbinafine were 191-fold and 48-fold relative to their MIC90 values, respectively. Figure 2 shows the mean concentrations of amorolfine and terbinafine in human toenails in a cross-section of the nail plate normalized by their MIC90 (a), keratin-binding percentage (b), or MIC90 and keratin-binding percentage (c). Amorolfine and terbinafine penetrated the entire thickness of the toenails from the top to the bed of the nail.

Mean concentrations of amorolfine and terbinafine in mycotic nail sections (n = 8 each) at various depths of the nail plate 3 h after the application of 5.0% and 7.8% lacquer, respectively, as determined by MALDI-FTICR and normalized by the a MIC90, b keratin-binding percentage, or c MIC90 and keratin-binding percentage of these compounds. MALDI-FTICR, matrix-assisted laser desorption ionization–Fourier transform ion cyclotron resonance; MIC90, minimum inhibitory concentration required to inhibit the growth of 90% of Trichophyton rubrum
At 3 h, the overall median tissue exposure relative to the MIC90 was significantly higher for amorolfine than for terbinafine (191 vs. 48; p = 0.010) (Fig. 3a) and when adjusted according to the keratin unbound fraction (7.4 vs. 0.9; p = 0.002) (Fig. 3b).

Nail tissue exposure 3 h after treatment with amorolfine and terbinafine (n = 8 sections each), based on the fold difference between the concentration of each antifungal reached in the nail and its MIC90 for the a overall fraction or b keratin-unbound drug fraction only. Boxplots indicate the median (horizontal bars), mean (crosses), and interquartile range (25th to 75th percentile), and the whiskers show the maximum and minimum. MIC90, minimum inhibitory concentration required to inhibit the growth of 90% of Trichophyton rubrum
Discussion
This study is, to our knowledge, the first time that the MALDI-FTICR imaging technique has been used to compare the penetration and distribution profiles of amorolfine 5.0% lacquer with terbinafine 7.8% lacquer. Both amorolfine and terbinafine penetrated the entire thickness of the toenail from the top to the bed of the nail. However, previous data have shown that the MIC90 of terbinafine is higher than that of amorolfine (16 vs. 4 µg/mL or 54.9 vs. 12.6 µM), but the MIC50 is lower (0.03 vs. 0.25 µg/mL or 0.11 vs. 0.79 µM) [8]. Thus, although the absolute median concentration of terbinafine was similar to that of amorolfine, relative to their respective MIC90 values, amorolfine levels in the nail were shown here to be significantly higher than those of terbinafine, including when normalized by the keratin-binding percentage.
Although a concentration exceeding their respective MIC90 values may yield a high multiple, effectively treating onychomycosis remains challenging. Oral systemic antifungal treatments are generally more effective than topical treatments, but they are associated with higher risks of adverse events and drug–drug interactions, and these therapies do not fully penetrate the entirety of the nail plate from the blood vessel network beneath the nail bed to the superficial layers of the nail [9]. Therefore, oral agents are largely reserved for patients whose conditions have not responded after 6 months of topical therapy or when at least 50% of the distal nail plate, the nail matrix, or multiple nails (more than three or four) are involved [9].
With topical drug administration, drug penetration into the nail plate through to the nail bed is complex. Drug-related factors impacting drug delivery into human nail tissue include drug molecular size, surface charge, lipophilicity, and polarity [1, 10]. Recent findings suggest that factors present in the natural environment or in situ behavior of the pathogens may influence the effectiveness of a drug differently compared with controlled laboratory conditions [11, 12]. During onychomycosis treatment, the keratin matrix that composes the dorsal plate of the nail is considered an obstacle to nail plate penetration. Binding of the drug to keratin in the nail plate reduces the free (active) drug, lessening the concentration gradient and limiting drug permeation into deeper tissues [2]. Terbinafine free-drug levels after its incubation in human nail keratin suspensions (1.8%) have been shown to be lower than those of amorolfine free-drug levels (3.9%), suggesting that terbinafine has a higher affinity toward human nail keratin [2]. An earlier in vitro study was one of the first to demonstrate the fungistatic and fungicidal activity of amorolfine in a nail keratin-based culture onychomycosis model [13]. More recently, Ghannoum et al. demonstrated that a single application of amorolfine 5% nail lacquer, but not terbinafine 10% nail lacquer, resulted in antifungal efficacy within the nail plate in an ex vivo study [5].
The efficacy of once-weekly amorolfine nail lacquer has been established for several decades [14]. With the lacquer, the volatile vehicle evaporates, leaving an occlusive film on the surface of the nail [15]. This film acts as a drug depot, simultaneously increasing hydration of the nail and positively impacting drug penetration. As a result of the formulation, re-application of amorolfine nail lacquer is only required once to twice weekly. Attempts to develop a topical product based on terbinafine for treating nail fungal infections have been more challenging. In a recent phase 3 study of patients with mild to moderate distal subungual onychomycosis, the proportion of patients with a complete cure (mycological cure and an absence of clinical disease involvement) was not significantly different after 52 weeks of treatment with a topical 10% solution of terbinafine or vehicle [16]. Results with a terbinafine 10% nail lacquer have been more promising, although participants received daily treatment for the first 4 weeks, before weekly treatment was evaluated [17].
The MALDI-FTICR technique for the simultaneous generation of high-resolution images and drug quantification has not been used previously to compare amorolfine and terbinafine. Acknowledging that this was an ex vivo study with a limited sample size, it was further noted that the one nail sample showing the most homogeneous distribution and deepest penetration of terbinafine was particularly thick and brittle and may not, therefore, reflect the standard penetration of terbinafine. In the present study, the variability observed in the thickness of the nails highlighted the heterogeneity of the samples and may have contributed to the observed differences in drug concentration in the nail bed. Also, in addition to the different concentrations of terbinafine and amorolfine in the lacquers, the results do not account for any possible differences in the amount of compound removed by the cleaning of the toenail surface at the end of the treatment period, which was not evaluated in this study.
Conclusion
This is the first study to report the use of MALDI-FTICR for the quantitative analysis of the distribution and penetration profiles of amorolfine compared with terbinafine in human toenails. Amorolfine and terbinafine had similar distribution patterns, and both penetrated the entire thickness of the toenail from the top to the bed of the nail. However, relative to their respective MIC90 values, the concentration of amorolfine in the nail was higher than that of terbinafine.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Aslam R, Hussain T, Yousaf AM, et al. Onychomycosis: current understanding and strategies for enhancing drug delivery into human nail tissue. Curr Drug Res Rev. 2021;13(1):25–35.
Matsuda Y, Sugiura K, Hashimoto T, Ueda A, Konno Y, Tatsumi Y. Efficacy coefficients determined using nail permeability and antifungal activity in keratin-containing media are useful for predicting clinical efficacies of topical drugs for onychomycosis. PLoS ONE. 2016;11(7): e0159661.
Daniel RC. Onychomycosis: burden of disease and the role of topical antifungal treatment. J Drugs Dermatol. 2013;12(11):1263–6.
Thomas J, Jacobson G, Narkowicz C, Peterson G, Burnet H, Sharpe C. Toenail onychomycosis: an important global disease burden. J Clin Pharm Ther. 2010;35(5):497–519.
Ghannoum M, Long L, Kunze G, Sarkany M, Osman-Ponchet H. A pilot, layerwise, ex vivo evaluation of the antifungal efficacy of amorolfine 5% nail lacquer vs other topical antifungal nail formulations in healthy toenails. Mycoses. 2019;62(6):494–501.
Pinto F, Bagger C, Kunze G, et al. Visualisation of penetration of topical antifungal drug substances through mycosis-infected nails by matrix-assisted laser desorption ionisation mass spectrometry imaging. Mycoses. 2020;63(8):869–75.
Hamm G, Bonnel D, Legouffe R, et al. Quantitative mass spectrometry imaging of propranolol and olanzapine using tissue extinction calculation as normalization factor. J Proteomics. 2012;75(16):4952–61.
Adimi P, Hashemi S, Mahmoudi M, et al. In-vitro activity of 10 antifungal agents against 320 dermatophyte strains using microdilution method in Tehran. Iran J Pharm Res. 2013;12(3):537–45.
Gupta AK, Paquet M, Simpson FC. Therapies for the treatment of onychomycosis. Clin Dermatol. 2013;31(5):544–54.
Phan K, Kaur K, Wright K, et al. The penetrance of topical nail therapy: limitations and current enhancements. Clin Podiatr Med Surg. 2021;38(4):535–40.
Ke W, Xie Y, Chen Y, Ding H, Ye L. Fungicide-tolerant persister formation during cryptococcal pulmonary infection. Cell Host Microbe. 2024;32(2):276-289.e7.
Chen L, Tian X, Zhang L, Wang W, Hu P. Brain glucose induces tolerance of Cryptococcus neoformans to amphotericin B during meningitis. Nat Microbiol. 2024;9(2):346–58.
Schaller M, Borelli C, Berger U, et al. Susceptibility testing of amorolfine, bifonazole and ciclopiroxolamine against Trichophyton rubrum in an in vitro model of dermatophyte nail infection. Sabouraudia. 2009;47(7):753–8.
Lauharanta J. Comparative efficacy and safety of amorolfine nail lacquer 2% versus 5% once weekly. Clin Exp Dermatol. 1992;17:41–3.
Marty J-PL. Amorolfine nail lacquer: a novel formulation. J Eur Acad Dermatol Venereol. 1995;4:S17–21.
Gupta AK, Surprenant MS, Kempers SE, Pariser DM, Rensfeldt K, Tavakkol A. Efficacy and safety of topical terbinafine 10% solution (MOB-015) in the treatment of mild to moderate distal subungual onychomycosis: a randomized, multicenter, double-blind, vehicle-controlled phase 3 study. J Am Acad Dermatol. 2021;85(1):95–104.
Blume-Peytavi U, Tosti A, Falqués M, et al. A multicentre, randomised, parallel-group, double-blind, vehicle-controlled and open-label, active-controlled study (versus amorolfine 5%), to evaluate the efficacy and safety of terbinafine 10% nail lacquer in the treatment of onychomycosis. Mycoses. 2022;65(4):392–401.
Acknowledgements
Medical Writing and Editorial Support
Medical writing and editorial support for the preparation of this manuscript, under the guidance of the authors, was provided by Hazel Gwarinda, PhD, of ApotheCom, UK, and was funded by Galderma SA, Lausanne, Switzerland, in accordance with Good Publication Practice (GPP) standards (Ann Intern Med 2022;175:1298–1304).
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Funding
This study and the journal’s Rapid Service Fee were sponsored by Galderma SA, Lausanne, Switzerland.
Author information
Authors and Affiliations
Contributions
Nicolas Joly-Tonetti was responsible for and involved in the study conception and design. Raphael Legouffe, Aurore Tomezyk, Clémence Gumez, Mathieu Gaudin, and David Bonnel were responsible for the acquisition of the cadaver samples and data. All authors were involved in the data analysis and interpretation. All authors also reviewed the manuscript and approved the final version for submission.
Corresponding author
Ethics declarations
Conflict of Interest
Nicolas Joly-Tonetti is an employee of Galderma SA, Lausanne, Switzerland. Clémence Gumez, Aurore Tomezyk, Raphael Legouffe, Mathieu Gaudin and David Bonnel are employees of Aliri (formerly ImaBiotech), Loos, France. Martin Schaller is an advisory board member for Galderma and Marpinion; a speaker for AbbVie, Bayer Healthcare, Galderma, and La Roche-Posay; a recipient of research grants from Galderma and Bayer HealthCare; and an investigator for GSK and Galderma.
Ethical Approval
The samples used in these studies were sourced and deidentified via Tissue Solutions Ltd., a subsidiary of BioIVT LLC which is accredited for the collection, storage, and commercial distribution of biospecimens by the Office for Human Research Protections (OHRP) of the United States Department of Health. The use of publicly available biospecimens from an accredited supplier is not considered to fall under research in human subjects, and as such, IRB approval or exemption was not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Joly-Tonetti, N., Legouffe, R., Tomezyk, A. et al. Penetration Profile of Terbinafine Compared to Amorolfine in Mycotic Human Toenails Quantified by Matrix-Assisted Laser Desorption Ionization–Fourier Transform Ion Cyclotron Resonance Imaging. Infect Dis Ther 13, 1281–1290 (2024). https://doi.org/10.1007/s40121-024-00979-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40121-024-00979-2