
Abstract
Introduction
High-dose dual therapy (HDDT) can attain acceptable eradication rates provided that the optimal doses, timing and treatment duration are applied. The existing evidence still shows inconsistent reports (< 90%) on HDDT therapy except in some Asian countries. We aimed to assess and compare the efficacy of 14-day HDDT by comparing it to 14-day rabeprazole-containing hybrid therapy (HT) and to investigate the host and bacterial factors predicting the treatment outcomes of eradication therapies.
Methods
In this open-label, randomized controlled trial, we recruited 243 naïve Helicobacter pylori-infected patients from September 1, 2018, to November 30, 2021. They were randomly allocated (1:1) to the HDDT group (rabeprazole 20 mg and amoxicillin 750 mg q.i.d for 14 days, n = 122) and the HT group (rabeprazole 20 mg and amoxicillin 1 g b.i.d. for 7 days, followed by rabeprazole 20 mg, amoxicillin 1 g, clarithromycin 500 mg and metronidazole 500 mg b.i.d. for 7 days, n = 121). Twelve patients were absent during follow-up in the HDDT group and 4 in the HT group, resulting in 110 for the HDDT group and 117 for HT group in the per protocol (PP) study. The outcome was determined by urea breath tests 8 weeks later.
Results
The eradication rates for the HDDT and HT groups were 77.0% (95% confidence interval [CI]: 68.5% to 84.1%) and 94.2% (95% CI: 88.4% to 97.6%) (P < 0.001) in intention-to-treat analysis; 85.5% (95% CI: 77.5% to 91.5%) and 97.4% [95% CI: 92.6% to 99.5%] (P = 0.001) in per protocol analysis. The adverse event rates were 7.3% in the HDDT group and 14.5% in the HT group (P = 0.081). The habit of coffee drinking was the dependent factor for eradication failure in the HDDT group (88.2% vs. 68.8%, P = 0.040), but had no influence in the HT group (97.9% versus 95.0%, P = 0.449) in the univariate analysis.
Conclusion
This study demonstrated that 14-day rabeprazole-containing HDDT did not achieve > 90% eradication rates for first-line H. pylori eradication as 14-day rabeprazole-containing HT did. HDDT is a potentially beneficial combination, which involves only two drugs with mild adverse effects; more precise studies are urged to find answers regarding these failures.
This clinical trial was registered retrospectively on 28 November, 2021, as ClinicalTrials.gov identifier: NCT05152004.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why carry out the study? |
One of the main reasons for the decreasing efficacy of Helicobacter pylori eradication is related to the increasing incidence of clarithromycin-resistant strains of H. pylori. Searching for successful treatment regimens in areas with increasing clarithromycin resistance > 15%, especially those with dual resistance to clarithromycin and metronidazole, is mandatory. |
Fourteen days’ hybrid therapy has been successful in the presence of clarithromycin resistance. It achieves an eradication rate of > 95% by intention-to-treat (ITT) and per-protocol (PP) analysis in areas of high clarithromycin and metronidazole resistance. However, it involves multiple drugs and prescription is complex, involving two stages of different drugs. |
What was learned from the study? |
High-dose dual therapy (proton-pump-inhibitor plus amoxicillin) involves a more potent acid inhibitor that likely enhances the activity of amoxicillin and is a promising alternative that can decrease misuse of antibiotics. HDDT can attain acceptable eradication rates if optimal doses, timing and treatment duration are applied but is still not categorized as strongly recommended in many consensus statements (< 90% eradication rates in many studies). |
This study demonstrated that 14-day rabeprazole-containing HDDT did not achieve > 90% eradication rates for first-line H. pylori eradication as 14-day rabeprazole-containing HT did. HDDT is a potentially beneficial combination, which involves only two drugs with mild adverse effects; more precise studies are urged to find answers regarding these failures. |
Introduction
One of the main reasons for the decline in efficacy of Helicobacter pylori eradication rates is related to the increasing incidence of clarithromycin-resistant strains of H. pylori [1,2,3,4,5,6,7]. Searching for successful treatment regimens in areas with increasing clarithromycin resistance > 15%, especially those with dual resistance to clarithromycin and metronidazole, is mandatory. Fourteen-day hybrid therapy (HT) has been successful in the presence of clarithromycin resistance [1, 8,9,10]. HT consists of a dual therapy with a proton pump inhibitor (PPI) and amoxicillin for 7 days followed by a quadruple regimen with a PPI, amoxicillin, clarithromycin and metronidazole for 7 days. It achieved an eradication rate of > 90% by intention-to-treat (ITT) and per-protocol (PP) analysis in areas of high clarithromycin and metronidazole resistance [10, 11]. However, it requires multiple drugs and prescription is complex, involving two stages of different drugs.
High-dose dual therapy (HDDT, proton-pump-inhibitor plus amoxicillin) and a more potent acid inhibitor that likely enhances the activity of amoxicillin are promising alternatives that could decrease misuse of antibiotics and emerge as a viable strategy for addressing high levels of clarithromycin resistance. Fourteen-day high-dose PPI and amoxicillin dual therapy could also attain > 90% eradication rate in some Asian studies [5, 12,13,14]. This treatment option is simple and involves only two drugs; most importantly, amoxicillin resistance is very low in Taiwan [5, 13]. High-dose PPI has been used in several studies for H. pylori eradication to increase the intragastric PH for optimal eradication but much existing evidence still shows inconsistent reports (< 90%) [15,16,17,18]. Kwack et al. reported a cure rate of 79.3% in the ITT analysis and 82.1% in the PP analysis by using high-dose dual therapy with ilaprazole 40 mg tablets given twice a day and amoxicillin 750 mg tablets given four times a day in Korea [18]. HDDT can attain acceptable eradication rates (< 90% in many studies) if the optimal doses, timing and treatment duration are applied but it is still not categorized as a strong recommendation in many consensus statements. HDDT involves increasing PPI and amoxicillin simultaneously to achieve a satisfactory eradication rate of H. pylori infection. Up to now, there is no standard HDDT, so different researchers have adopted different specific schemes. We therefore conducted this study to further assess the real-world efficacy of high-dose rabeprazole plus amoxicillin dual therapy in Taiwan by comparing it to 14-day rabeprazole-containing hybrid therapy and to investigate the host and bacterial factors predicting the treatment outcomes of eradication therapies.
Methods
Study Population
This randomized controlled trial allotted participants into two groups at 1:1 ratio, and they were prescribed either HDDT or HT. It was conducted at Kaohsiung Chang Gung Memorial Hospital from September 1, 2018, to November, 30, 2021, in Taiwan. The trial was approved and monitored by the institutional review boards of Chang Gung Memorial Hospital (201800871A3). This clinical trial was been registered retrospectively on November 28, 2021, as ClinicalTrials.gov identifier: NCT05152004. All authors had access to the study data and reviewed and approved the final manuscript.
Eligible outpatients > 18 years old with naïve H. pylori infection were included in the invited patient lists (n = 266). These invited patients had (1) endoscopically proven peptic ulcer diseases or (2) gastritis with naive H. pylori infection and had received no prior treatment. However, we excluded patients if they had been prescribed any form of antibiotics or bismuth for any other treatments, proton-pump inhibitors or non-steroidal anti-inflammatory drugs in the last 4 weeks. Another exclusion criterion for these eligible patients was any potential history of allergy to the medications given in the two study groups. Candidates with history of previous gastric surgery or other comorbidities were uninvited. Lastly, currently pregnant participants or those who refused to participate were also not invited. Eventually, we obtained written informed consent from all participants before enrollment.
Randomization
The recruited participants were randomly assigned at a 1:1 ratio to receive HDDT or HT (HDDT, rabeprazole 20 mg and amoxicillin 750 mg q.i.d for 14 days; HT, rabeprazole 20 mg and amoxicillin 1 g b.i.d. for 7 days, followed by rabeprazole 20 mg, amoxicillin 1 g, clarithromycin 500 mg and metronidazole 500 mg b.i.d. for 7 days). Rabeprazole and amoxicillin were taken 1 h before a meal while clarithromycin and metronidazole were taken with food. The randomization process was performed by using a web-based central randomization system with 24 h’ access, with instant and concealed allocation being obtained. Randomization block sizes vary in accordance with the computer-generated provision sequence. When recruitment began, patients were presented to the doctor in a blinded manner by a research assistant. All codes were exposed only at the study completion date.
Study Process Timeline
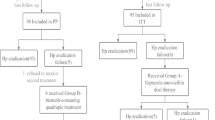
Figure 1 shows the schematic flowchart of the study design timeline including informed consents, screening, enrollment, randomization, performing eradication, each visit and confirmation of eradication (also in Supplementary Fig. 1). Figure 2 shows the patient disposition (also in Supplementary Fig. 2). Each patient completed a standard questionnaire for their complete medical history and provided demographic data. These data included age, sex and history of smoking, alcohol, and coffee and tea consumption habits, etc. In this study, we defined alcohol consumption as taking < 80 g/day or ≥ 80 g/day; smoking habit as consumption of ≥ 1 pack of cigarettes per week; coffee or tea consumption as drinking ≥ 1 cup per day.

Study protocol timeline. HDDT: High-dose dual therapy (rabeprazole 20 mg and amoxicillin 750 mg q.i.d for 14 days); ITT: intention to treat; PP: per protocol; HT: hybrid therapy (rabeprazole 20 mg and amoxicillin 1 g b.i.d. for 7 days, followed by rabeprazole 20 mg, amoxicillin 1 g, clarithro-mycin 500 mg and metronidazole 500 mg b.i.d. for 7 days)

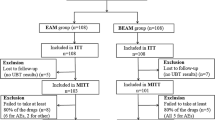
Disposition of patients. HDDT: High-dose dual therapy (rabeprazole 20 mg and amoxicillin 750 mg q.i.d for 14 days); ITT: intention to treat; PP: per protocol; HT:hybrid therapy (rabeprazole 20 mg and amoxicillin 1 g b.i.d. for 7 days, followed by rabeprazole 20 mg, amoxicillin 1 g, clarithromycin 500 mg and metronidazole 500 mg b.i.d. for 7 days)
The participants were requested to return 2 weeks later to our outpatient clinics to report the drug compliance and adverse events. On the return to the outpatient clinics 2 weeks later, participants reported the adverse events using a 4-point scale system: (1) none; (2) mild if they experienced bothersome uneasiness but it did not interfere with their daily life; (3) moderate when these symptoms were bothersome enough to interfere with daily life; (4) severe when they suffered from distress causing them to quit the medication [4]. We checked the unfinished medication at the completion of treatment and defined poor compliance when < 90% of the prescribed medications were taken.
Follow-up urea breath tests were scheduled 8 weeks later. The 13C-urea breath test was performed according to our previous studies [19]. The cutoff value of the urea breath test was set at 4.8‰ of δ13CO2. The staff, who was blind to the H. pylori status, performed the tests.
Outcomes
Primary outcome was the successful eradication of H. pylori. Secondary outcome was adverse events. We defined successful eradication as a negative result of the urea breath test. Finally, the rates of eradication, adverse events and compliance and bacterial factors influencing the efficacy of eradication therapy were analyzed.
Helicobacter pylori culture was performed only for those participants who agreed and had signed additional informed consent to receive endoscopy and biopsy for culture. One antral gastric biopsy specimen was obtained for isolation of H. pylori, using previously described culture methods [5, 19]. The antibiotic susceptibility was tested by E test (AB Biodisck, Solna, Sweden). Helicobacter pylori strain MIC values > 0. 125, > 0.5, > 1, > 1 and > 8 mg/l were considered to be the resistance breakpoints for amoxicillin, clarithromycin, levofloxacin, tetracycline and metronidazole, respectively [20].
Statistical Analysis
All analyses were performed using the Statistical Package for Social Sciences (IBM SPSS®, version 22.0 for Windows). The dataset was analyzed using the SAS statistical package. We assumed the eradication rate in the HDDT group should be at least an acceptable 80% and that the HT group could attain 90% eradication rate, a 10% difference; then, we could reach a statistical power of 80% when recruiting a sample size of 119 participants in each group and have a two-sided P value of 0.05 once 95% had completed the follow-up. The effect variables were the rates of eradication, adverse events and compliance. To compare the major outcomes between groups, chi-square test with or without Yates correction for continuity and Fisher’s exact test were applied when applicable. A P value < 0.05 was considered statistically significant. Eradication rates were evaluated by ITT and PP analyses. We reported all randomized participants into ITT analysis once they took at least one dose of medication. Any participants with unknown infection status following treatment were measured as treatment failures in the ITT analysis. However, the participants with unknown H. pylori status following therapy and those with major protocol violations were excluded in the PP analysis.
Univariate analysis to identify the dependent factors affecting the treatment response was performed. Variables found to be significant by univariate analysis were subsequently calculated by a stepwise logistic regression method to identify factors for eradication outcome.
Results
Eradication Rates and Predisposing Factors
As shown in Fig. 2, 266 eligible participants with endoscopically proven peptic ulcer diseases or gastritis were invited; 243 participants were enrolled (n = 122 in the HDDT group and n = 121 in HT group) in the ITT analysis. Twelve participants missed the appointment date during follow-up in the HDDT group, and 4 in the HT group, and were excluded, resulting in a final number of 110 in the PP study for the HDDT group and 117 for the HT group. The demographic data of the two groups are summarized in Table 1; none of the variables was significantly different between the groups. The eradication rates for HDDT and HT groups were 77.0% (95% confidence interval [CI]: 68.5% to 84.1%) and 94.2% (95% CI: 88.4% to 97.6%) (P < 0.00) in intention-to-treat analysis; 85.5% (95% CI: 77.5% to 91.5%) and 97.4% [95% CI: 92.6% to 99.5%] (P = 0.001) in per protocol analysis (Table 2).
In univariate analysis of the clinical factors influencing the efficacy of H. pylori eradication in each therapy, there were no independent factors influencing eradication in the HT group. Sex and coffee-drinking habit were the influencing clinical factors in the HDDT group (P = 0.045 and P = 0.040, respectively) (Table 3). In univariate analysis, coffee consumption, dual resistance of clarithromycin and metronidazole, and hybrid therapy were the significant factors influencing eradication. In multivariate analysis, hybrid therapy was an independent factor for H. pylori eradication (OR 95% CI: 11.053 [1.234–99.021], P = 0.032) (Table 4).
Adverse Events and Complications
As shown in Table 5, the observed adverse event rate was 7.3%.for participants prescribed HDDT. However, 14.5% of the participants who received HT reported adverse events (P = 0.081). Table 5 summarizes the reported adverse events such as abdominal pain, constipation, diarrhea, dizziness, headache, nausea/vomiting and skin rash. There was 100% drug compliance in both the participant group as all adverse events were mild and tolerable.
Antibiotic Resistance
Samples from 108 participants were cultured for H. pylori, and the positive culture rate was 89.8% (97/108). The antibiotic resistance rates were amoxicillin (2.1%), clarithromycin (16.5%), metronidazole (37.1%) and dual resistance to clarithromycin and metronidazole (5.1%). The drug resistance factors influencing the efficacy of H. pylori eradication in each therapy are shown in Table 3. The H. pylori eradication rates for the clarithromycin-susceptible but metronidazole-resistant strains were 87.5% (14/16) compared to 82.4% (14/17) for both clarithromycin and metronidazole-susceptible strains in the HDDT group, P = 0.680. The H. pylori eradication rates for the clarithromycin-susceptible but metronidazole-resistant strains were 100% (15/15) compared to 97.1% (33/34) for both clarithromycin and metronidazole-susceptible strains in the HT group, P = 0.502. The H. pylori eradication rates for the metronidazole-susceptible but clarithromycin-resistant strains were 75.0% (3/4) compared to 66.7% (2/3) for the dual resistance to both clarithromycin and metronidazole in the HDDT group, P = 0.809. The H. pylori eradication rates for the metronidazole-susceptible but clarithromycin-resistant strains were 100% (6/6) compared to 100% (2/2) for the dual resistance to both clarithromycin and metronidazole in the HT group. In short, the H. pylori eradication rates for dual resistance to both clarithromycin and metronidazole were 100% (2/2) in HT group and 66.7%(2/3) in the HDDT group, P = 1.000 in Fisher’s exact test.
Discussion
Although HDDT has been reported to achieve a high eradication rate in many studies especially in areas with high clarithromycin resistance (> 15%), it is acknowledged in Maastricht VI as a “potentially” useful regimen for eradicating naïve H. pylori infection with the advantage that it bypasses clarithromycin and metronidazole resistances [21]. This issue was also raised in the Italian guidelines, which recommend HDDT in areas that have high clarithromycin resistance for better contextualization [22]. To date, many studies have attained only acceptable eradication rates, provided that the optimal doses, timing and treatment durations are applied. Consequently, the treatment was not categorized as a strong recommendation in Maastricht VI.
Realistically, the evidence from meta-analysis supporting the use of HDDT as first-line or rescue treatment for H. pylori infection was neither significantly inferior nor superior to the recommended regimens such as triple therapy, bismuth quadruple therapy and non-bismuth quadruple therapy. Additionally, the frequency of adverse events for HDDT was significantly lower than for other regimens (RR: 0.48, 95% CI: 0.37–0.64, P < 0.001) [23, 24]. Among these reviewed studies, the regimens with rabeprazole 20 mg q.i.d and amoxicillin 750 mg q.i.d for 14 days achieved excellent success rates ranging from 94.0 to 96.4% in the first-line treatment for H. pylori eradication in PP analysis [13, 25]. However, in this study, the rabeprazole-containing HDDT was inferior to 14-day rabeprazole-containing HT for first-line H. pylori eradication (85.5% vs. 97.4%, P = 0.001) in PP analysis. In the univariate analysis, we observed that the habit of coffee drinking was a dependent factor for eradication failure in the HDDT group (88.2% vs. 68.8%, P = 0.040), but it had no influence in the HT group (97.9% versus 95.0%, P = 0.449). The HDDT regimen seems to be more susceptible to coffee drinking than the HT regimen. In animal and human studies, caffeine stimulates gastrin secretion in preparations of pure rat gastrin cells that are present in the stomach and duodenum and secrete gastrin [26]. Theoretically, caffeinated coffee stimulates more effective gastrin secretion than decaffeinated coffee in patients with gastroesophageal reflux disease [27, 28]. This might be associated with the decrease in ability to maintain a constant high intragastric pH, which determined success or failure of these HDDTs. However, this hypothesis needs more solid evidence to support it.
Moreover, the effect of amoxicillin is time- and intragastric pH-dependent. Oral amoxicillin is a time-dependent semi-synthetic penicillin, and plasma levels in excess of the minimum inhibitory concentrations are maintained for 6 to 8 h. Therefore, maintaining plasma concentrations of amoxicillin can only be attained by constantly keeping a high intragastric pH. Gastric pH value is associated with the dose of PPI, dosing frequency and drug type. At intragastric pH < 6, amoxicillin becomes unstable and ineffective [29]. A multiple antibiotic component regimen, such as hybrid eradication therapy, would overcome the lower acid environment.
To date, there have been inconsistent and conflicting reports on the efficacy of HDDT from different study groups. For example, an ITT analysis conducted in the US demonstrated that a 14-day dual therapy consisting of esomeprazole (40 mg, 3 times daily) and amoxicillin (750 mg, 3 times daily) had an eradication rate of 72.2% (95% CI: 56%–84%) in treatment-naive patients; the low cure rate was mainly attributed to a high frequency of unfavorable CYP2C19 gene polymorphisms [14]. It has been shown that in patients with CYP2C19-poor metabolizers, HDDT could reliably cure > 90% of H. pylori infections [30].
The success of H. pylori eradication depends on the presence of antimicrobial resistance. The antibiotic resistance rates were amoxicillin (2.1%), clarithromycin (16.5%), metronidazole (37.1%) and dual resistance to clarithromycin and metronidazole (5.1%). The H. pylori eradication rates for the clarithromycin- and metronidazole-susceptible strains were 97.1% (33/34) in the HT group and 82.4% (14/17) in the HDDT group. Notably, the antibiotic resistance rates for amoxicillin were low at 2.1%, according to the MIC value > 0.125 with 2018 EUCAST breakpoints, and the eradication rates for amoxicillin-resistant strains were 100% (2/2) in the HDDT group. In a meta-analysis study assessing the impact of amoxicillin resistance on the efficacy of amoxicillin-containing regimens for H. pylori eradication, the breakpoint of amoxicillin resistance was found to be 0.125 mg/l (kappa coefficient 0.298), where the resistance rate was 11.1%. Interestingly, combination regimens still had a positive effect in the presence of amoxicillin resistance [31].
In the current study the adverse event rates were 7.3% in the HDDT group and 14.5% in the HT group but compliance was 100% in both groups. The probability of side effects in HDDT seems to be half that of other first-line regimens in the systemic review [22, 25]. In our experience, if a consultation phone number is provided to patients, this is helpful and increases patient compliance. This was done during the present study, and none of the patients discontinued treatment as a result of poor compliance caused by adverse events during eradication therapy. It was also because all the adverse events encountered in this study were mild and tolerable. A benefit of the role of probiotics in addition to H. pylori regimens is that probiotics have been reported to increase H. pylori eradication rates and reduce the potential adverse events in many studies [32]. However, the reports were controversial in some studies [33]. To date, the level of evidence is still classified as low until more high-quality studies emerge [22, 33].
The reasons for the failures could be multifactorial but the use of different PPIs in terms of optimal doses, timing and treatment duration applied was a key factor. The main limitation is that our laboratory could not perform CYP2C19 genotyping, so we could not determine the difference in PPI metabolic effect in the two groups. It is generally accepted that CYP2C19 genotype status influences gastric acid suppression by PPIs but the influence decreases when PPI dosage and dosing frequency are increased [13, 34]. However, at least two studies have reported that PPIs (rabeprazole 10 mg or esomeprazole 20 mg) given four times daily could maintain the high intragastric pH > 6. [35, 36]. Vonoprazan has a stronger and more lasting effect on inhibiting gastric acid compared with PPIs [37]. It may be able to reduce the impact of CYP2C19 genotyping differences and optimize the dual therapy again, but more data need to be gathered in the future. The strength of our study is that we showed that 14-day rabeprazole-containing HDDT eradication rate was < 90%. Despite previous successful reports of HDDT especially in some Asian countries, heterogeneous reports still exist. HDDT involves only two drugs, and amoxicillin resistance is generally low globally; it is theoretically expected to be effective in high clarithromycin resistance areas (> 15%) or areas with high dual resistance to clarithromycin and metronidazole. However, 14-day rabeprazole-containing HDDT did not achieve > 90% eradication rates in this study, just like many other studies.
Conclusions
This study demonstrated that 14-day rabeprazole-containing HDDT did not achieve > 90% eradication rates for first-line H. pylori eradication as 14-day rabeprazole-containing HT did. HDDT is a potentially beneficial combination which involves only two drugs with mild adverse effects. More precise studies are needed to solve the issues related to these failures.
References
Update on the first-line treatment of Helicobacter pylori infection in areas with high and low clarithromycin resistances. Therap Adv Gastroenterol. 2022; 15: 17562848221138168.
Boyanova L, Hadzhiyski P, Gergova R, Markovska R. Evolution of Helicobacter pylori resistance to antibiotics: a topic of increasing concern. Antibiotics (Basel). 2023;12(2):332.
Quach DT, Mai BH, Tran MK, Dao LV, Tran HV, Vu KT. Vietnam Association of Gastroenterology (VNAGE) consensus on the management of Helicobacter pylori infection. Front Med (Lausanne). 2023;9:1065045.
Ma TL, Tai WC, Loke SS, Yao CC, Liang CM, Chuah SK. Efficacy and safety of 7-day non-bismuth concomitant quadruple therapy for first-line Helicobacter pylori eradication in the elderly. Drugs Aging. 2023;40(1):71–9.
Tai WC, Liang CM, Kuo CM, Huang PY, Wu CK, Yang SC, et al. A 14-day esomeprazole- and amoxicillin-containing high dose dual therapy achieves high eradication rate in the first line anti-helicobacter pylori treatment in Taiwan: a Prospective Randomized Trial. J Antimicrob Chemother. 2019;74(6):1718–24.
Doctor S, Abraham P, Desai D, Dhoble P, Gupta T, Joshi A. Ten-day concomitant and sequential therapy for Helicobacter pylori effective in region with high antibiotic resistance rates. Indian J Gastroenterol. 2022;41(6):627–33.
Huang TH, Yang SC, Tai WC, Liang CM, Kuo CM, Yao CC, et al. The efficacies of non-bismuth containing quadruple therapies in the treatment of first-line anti-Helicobacter pylori across 4-year time interval with changing antibiotics resistance. Biomed J. 2021; 44(6 Supple 2): S275–81.
Hsu PI, Lin PC, Graham DY. Hybrid therapy for Helicobacter pylori infection: a systemic review and meta-analysis/. World J Gastroenterol. 2015;21(45):12954–62.
Hybrid therapy versus sequential therapy for eradication of Helicobacter pylori: a randomized controlled trial. J Pharmacol Pharmacother 2017; 8(2): 62–7.
Hsu PI, Wu DC, Wu JY, Graham DY. Modified sequential Helicobacter pylori therapy: proton pump inhibitor and amoxicillin for 14 days with clarithromycin and metronidazole added as a quadruple (hybrid) therapy for the final 7 days. Helicobacter. 2011;16(2):139–45.
Hybrid vs sequential therapy for eradication of Helicobacter pylori in Taiwan: A prospective randomized trial. World J Gastroenterol 2015; 21(36): 10435–42.
Ren L, Lu H, Li HY, Zhu LY, Xu XQ, Gu LY, et al. New dual therapy for primary treatment of Helicobacter pylori infection: a prospective randomized study in Shanghai. Chin J Dig Dis. 2014;15(11):622–7.
Yang JC, Lin CJ, Wang HL, Chen JD, Kao JY, Shun CT, et al. High-dose dual therapy is superior to standard first-line or rescue therapy for Helicobacter pylori infection. Clin Gastroenterol Hepatol. 2015;13(5):895–905.
Yang Q, He C, Hu Y, Hong J, Zhu Z, Xie Y, et al. 14-day pantoprazole- and amoxicillin-containing high-dose dual therapy for Helicobacter pylori eradication in elderly patients: a prospective, randomized controlled trial. Front Pharmacol. 2023;14:1096103.
Graham DY, Javed SU, Keihanian S, Abudayyeh S, Opekun AR. Dual proton pump inhibitor plus amoxicillin as an empiric anti-H. pylori therapy: studies from the United States. J Gastroenterol. 2010; 45(8): 816–20.
Bayerdörffer E, Miehlke S, Mannes GA, Sommer A, Höchter W, Weingart J, et al. Double-blind trial of omeprazole and amoxicillin to cure Helicobacter pylori infection in patients with duodenal ulcers. Gastroenterology. 1995;108(5):1412–7.
Miehlke S, Kirsch C, Schneider-Brachert W, Haferland C, Neumeyer M, Bästlein E, et al. A prospective, randomized study of quadruple therapy and high-dose dual therapy for treatment of Helicobacter pylori resistant to both metronidazole and clarithromycin. Helicobacter. 2003;8(4):310–9.
Kwack W, Lim Y, Lim C, Graham DY. High dose ilaprazole/amoxicillin as first-line regimen for Helicobacter pylori infection in Korea. Gastroenterol Res Pract. 2016;2016:1–7.
Chuah SK, Liang CM, Lee CH, Chiou SS, Chiu YC, Hu ML, et al. A randomized control trial comparing two levofloxacin-containing second-line therapies for Helicobacter pylori eradication. Medicine (Baltimore). 2016;95(19): e3586.
European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 8.1; (2018) http://www.eucastorg/clinical_breakpoints. 2018.
Malfertheiner P, Megraud F, Rokkas T, Gisbert JP, Liou JM, Schulz C, et al. Management of Helicobacter pylori infection: The Maastricht VI/Florence consensus report. Gut. 2022 in press. https://doi.org/10.1136/gutjnl-2022-327745
Romano M, Gravina AG, Eusebi LH, Pellegrino R, Palladino G, Frazzoni L, et al. Management of Helicobacter pylori infection: Guidelines of the Italian Society of Gastroenterology (SIGE) and the Italian Society of Digestive Endoscopy (SIED). Dig Liver Dis. 2022;54(9):1153–61.
Zhu YJ, Zhang Y, Wang TY, Zhao JT, Zhao Z, Zhu JR, et al. High dose PPI-amoxicillin dual therapy for the treatment of Helicobacter pylori infection: a systematic review with meta-analysis. Therap Adv Gastroenterol. 2020;13:1756284820937115.
Gao CP, Zhang D, Zhang T, Zhao JT, Zhao Z, Zhu JR, et al. PPI-amoxicillin dual therapy for Helicobacter pylori infection: An update based on a systematic review and meta-analysis. Helicobacter. 2020;25: e12692.
Hwong-Ruey Leow A, Chang JV, Goh KL. Searching for an optimal therapy for H pylori eradication: High-dose proton-pump inhibitor dual therapy with amoxicillin vs. standard triple therapy for 14 days. Helicobacter. 2020; 25(5): e12723.
Kidd, M., Hauso, Ø., Drozdov, I., Gustafsson, B.I., Modlin, I.M. Delineation of the chemomechanosensory regulation of gastrin secretion using pure rodent G cells. Gastroenterology 2009; 137(1):231–41. e10.
Schubert ML. Functional anatomy and physiology of gastric secretion. Curr Opin Gastroenterol. 2015;31(6):479–85.
Van Deventer G, Kamemoto E, Kuznicki JT, Heckert DC, Schulte MC. Lower esophageal sphincter pressure, acid secretion, and blood gastrin after coffee consumption. Dig Dis Sci. 1992;37(4):558–69.
Scott D, Weeks D, Melchers K, Sachs G. The life and death of Helicobacter pylori. Gut. 1998;43(Suppl 1):S56-60.
Kuo CH, Lu CY, Shih HY, Liu CJ, Wu MC, Hu HM, et al. CYP2C19 polymorphism influences Helicobacter pylori eradication. World J Gastroenterol. 2014;20(43):16029–36.
Chen MJ, Wu MS, Chen CC, Chen CC, Fang YJ, Bair MJ et al. Taiwan Gastrointestinal Disease and Helicobacter Consortium. Impact of amoxicillin resistance on the efficacy of amoxicillin-containing regimens for Helicobacter pylori eradication: analysis of five randomized trials. J Antimicrob Chemother. 2017; 72(12): 3481–89.
McFarland LV, Huang Y, Wang L, Malfertheiner P. Systematic review and meta-analysis: Multi-strain probiotics as adjunct therapy for Helicobacter pylori eradication and prevention of adverse events. United European Gastroenterol J. 2016;4(4):546–61.
Fallone CA, Chiba N, van Zanten SV, Fischbach L, Gisbert JP, Hunt RH, et al. The Toronto Consensus for the Treatment of Helicobacter pylori Infection in Adults. Gastroenterology. 2016;151(51–69): e14.
Ormeci A, Emrence Z, Baran B, Soyer OM, Gokturk S, Evirgen S, et al. Can Helicobacter pylori be eradicated with high-dose proton pump inhibitor in extensive metabolizers with the CYP2C19 genotypic polymorphism? Eur Rev Med Pharmacol Sci. 2016;20(9):1795–7.
Furuta T, Shirai N, Takashima M, Xiao F, Hanai H, Nakagawa K, et al. Effects of genotypic differences in CYP2C19 status on cure rates for Helicobacter pylori infection by dual therapy with rabeprazole plus amoxicillin. Pharmacogenetics. 2001;11(4):341–8.
Sahara S, Sugimoto M, Uotani T, Ichikawa H, Yamade M, Kagami T, et al. Potent gastric acid inhibition over 24 hours by 4-times daily dosing of esomeprazole 20 mg. Digestion. 2015;91(4):277–85.
Echizen H. The first-in-class potassium-competitive acid blocker, vonoprazan fumarate: pharmacokinetic and pharmaco-dynamic considerations. Clin Pharmacokinet. 2016;55(4):409–18.
Acknowledgements
Funding
This work and the journal’s Rapid Service Fee was funded by grants from the Research Foundation of Chang Gung Memorial Hospital (CMRPG8H0631), Taiwan.
Author Contributions
Wei-Chen Tai, Shih-Cheng Yang, Chih-Chien Yao, Cheng-Kun Wu, An-Che Liu, Chen-Hsiang Lee, Yuan-Hung Kuo, Seng-Kee Chuah and Chih-Ming Liang conceived of this study, Wei-Chen Tai participated in its design and coordination, and Seng-Kee Chuah and Chih-Ming Liang performed the statistical analyses. All authors helped to draft the manuscript and read and approved the final manuscript.
Disclosures
The authors (Wei-Chen Tai, Shih-Cheng Yang, Chih-Chien Yao, Cheng-Kun Wu, An-Che Liu, Chen-Hsiang Lee, Yuan-Hung Kuo, Seng-Kee Chuah and Chih-Ming Liang) declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Compliance with Ethics Guidelines
This article is based on new study with human participants performed by the authors. This study was approved by both the Institutional Review Board and Ethics Committee of Chang Gung Memorial Hospital, Taiwan (permit number 201800871A3). None of our patients were minors/children. This study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments.
Data Availability Statement
All data generated or analyzed during this study are included in this published article. Requests to access datasets should be directed to chuahsk@seed.net.tw.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Tai, WC., Yang, SC., Yao, CC. et al. The Efficacy and Safety of 14-day Rabeprazole Plus Amoxicillin High Dose Dual Therapy by Comparing to 14-day Rabeprazole-Containing Hybrid Therapy for the Naïve Helicobacter pylori Infection in Taiwan: A Randomized Controlled Trial. Infect Dis Ther 12, 1415–1427 (2023). https://doi.org/10.1007/s40121-023-00811-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40121-023-00811-3