
Abstract
Introduction
Multiple sclerosis (MS) is a disabling disease with unpredictable clinical manifestations. As clinical assessments may not fully capture the impact of MS on quality of life, they can be complemented by patient-reported outcome (PRO) measures to provide a more comprehensive picture of MS disease state and impact. The objectives of this study were to explore the experiences of people with relapsing–remitting MS, including symptoms and impacts on daily life, and to provide a conceptual model of MS outcomes.
Methods
A literature review of studies that evaluated the experiences of people with MS was completed and combined with semi-structured concept elicitation interviews conducted with 14 people with relapsing–remitting MS in the USA.
Results
The average age of the 14 participants was 43.9 (range 25–64) years, most were White (78.6%) and female (78.6%), and the mean duration since diagnosis was 6.6 (2–10) years. The most bothersome symptoms identified included fatigue (n = 9), cognitive dysfunction (n = 5), mobility/difficulty with walking (n = 3), and vision problems (n = 3). The most commonly reported impacts on daily life were balance problems/instability (n = 13), work life/productivity (n = 12), difficulty walking (n = 11), daily activities/household chores (n = 11), and leisure activities (n = 10).
Conclusion
There was a high frequency of concepts associated with physical function, fatigue, and sensory-motor actions. A conceptual model was developed that captures the disease symptoms, impairments, and impacts identified in the interviews as well as known processes and symptoms identified in the literature search. This model underpins the appropriateness of PRO instruments, such as the PROMIS Fatigue (MS) 8a and PROMIS Physical Function (MS) 15a, which evaluate symptoms and impacts that matter most to people with MS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Through interviews with people with relapsing–remitting multiple sclerosis and a literature search, we developed a novel conceptual model for multiple sclerosis that captures the processes, symptoms, functional impairments, and psychosocial impacts of the disease. |
The concepts identified are key to the development of targeted patient-reported measures for multiple sclerosis that support the evaluation of disease course and the assessment of symptoms that matter most to people with multiple sclerosis. |
Future patient-reported measures should consider all aspects of the conceptual model to ensure that the experiences and perspectives of people with multiple sclerosis are adequately considered and assessed in clinical trials and practice. |
Introduction
Multiple sclerosis (MS) is a disabling disease of the central nervous system (CNS; brain and spinal cord) in which the flow of information between the brain and the body is disrupted, leading to neurological dysfunction [1,2,3]. Disease processes include inflammatory activity, demyelination, and progressive neurodegeneration [1, 3]. The etiology of MS is complex and heterogeneous, with multifactorial processes involved including genetic, environmental, immunological, and infectious factors [1]. The most common disease course is relapsing–remitting MS (RRMS), experienced by 85% of people with MS (PwMS) [1]. RRMS is characterized by acute occurrences of symptoms, known as relapses, followed by periods of full or partial recovery when symptoms may lessen or disappear completely. Typically, the frequency and intensity of symptoms increase over time, referred to as disease progression, to a point where disability is permanently present, irrespective of additional relapse activity [1].
The clinical manifestations of MS are unpredictable [4, 5], but symptoms commonly experienced by PwMS include difficulties walking, fatigue, numbness/tingling, muscle weakness, spasticity, vision problems, cognitive impairment, bladder/bowel problems, sexual problems, emotional changes, and depression [1, 3, 6, 7]. At present, there is no cure for MS; treatment is lifelong and includes both disease-modifying and symptom management therapies, rehabilitation, psychological support, and social care [8].
Clinical evaluations have demonstrated that during remitting phases of RRMS, PwMS may experience so-called silent progression or progression independent of relapse activity, leading to ongoing disability accumulation from the earliest stages of the disease [3, 9]. The progressive accumulation of neural tissue damage via a smoldering pathological process may affect the entire CNS and involve neurodegeneration that may be downstream or independent of focal inflammatory lesions, including demyelination, slowly expanding lesions (magnetic resonance imaging [MRI] marker of chronic active lesions [demyelinated lesions with ongoing microglia/macrophage activity]), axonal loss, and brain atrophy [9,10,11,12,13,14]. Clinical studies indicate that 80–90% of accumulated disability may occur independent of relapse activity; therefore, disability accumulation can occur during RRMS both related and unrelated to relapses [15, 16].
Capturing impairment of physical and cognitive function, and symptoms such as fatigue, early in the disease course may benefit treatment and intervention strategies for PwMS [17]. In this context, early self-reporting by PwMS plays an important role in illuminating different aspects of disease progression. Improving the assessment of symptoms and functional limitations experienced by PwMS prior to clinical confirmation of disease progression or increased disease activity may help drive innovation in earlier management of MS symptoms and greater understanding of progression independent of relapse activity. Self-reported symptoms captured daily using a digital app were found to correlate with scores recorded using traditional patient-reported outcomes (PROs) [18]. By tracking symptoms and medication use in this way, PwMS may be able to monitor both their disease management and progression more accurately and provide more detailed and valuable information to their physician, supporting treatment strategy assessments [18].
To explore the symptoms and impacts of MS reported by PwMS, along with evaluating the breadth of methods used to understand the experiences of PwMS, we reviewed and summarized published literature relating to the experiences of PwMS (Supplementary Table 1). The methodologies used across these publications comprised a combination of interviews and focus groups, PRO questionnaires, and surveys; it should be noted that the way study participants described their experiences may be sensitive to the methodologies used for elicitation. The symptoms and impacts experienced by PwMS are diverse, complex, and may co-occur with comorbidities [4, 6, 7, 19, 20]. Impaired physical and cognitive functioning, along with fatigue and pain, was frequently identified as being severe and having the greatest impact on quality of life by PwMS [4, 6, 7, 20, 21].
One key insight from our literature search (Supplementary Table 1) is the importance of capturing the experiences of PwMS in addition to gathering data from established clinician-reported outcomes such as EDSS [22] and imaging outcomes such as MRI [12, 23]. While clinician-reported outcomes and imaging provide valuable metrics to diagnose and assess change in disease state [24], PRO measures can complement clinical assessments and provide a more comprehensive picture of disease progression and its perceived impact on a person’s life [25]. In addition, PRO measures are the primary approach for assessing important concepts such as fatigue [26, 27], depression, anxiety, and emotional dysregulation [28] that are not easily evaluated using other types of clinical assessments, as well as providing a population-level understanding of symptom frequency [6, 21]. Health authorities including the European Medicines Agency (EMA) and US Food and Drug Administration (FDA) have published guidance on standards for PRO instruments used in the registration of clinical trials [29, 30]. There are ongoing efforts, internationally, to improve PRO assessment in MS, including use of this information in clinical practice, healthcare systems, and research—in the hope that building a patient-centric approach to care will lead to better management of MS [31, 32].
This study aimed to characterize the symptoms and impacts of MS that are important to PwMS through in-depth concept elicitation interviews (CEIs) with PwMS. The specific objectives were (1) to explore the experiences of people with RRMS, including their symptoms and the impacts of the disease on their daily lives; (2) to develop a conceptual model of MS outcomes, outlining key disease symptoms and impact concepts, and their interrelationships to support the development of fit-for-purpose PRO instruments. The CEIs were conducted in the initial phase of a research program to develop novel, MS-specific PRO measures and the results ultimately supported the development of MS-specific PRO measures of physical function [33] and fatigue [27] that have been included in the phase 3 evolutionRMS 1 and 2 trials (NCT04338022, NCT04338061) of evobrutinib in people with relapsing MS (RRMS or secondary progressive MS [SPMS] with superimposed relapses).
Methods
CEIs were conducted in person by RTI Health Solutions (NC, USA) in September 2017 to elicit the symptoms and impacts of MS that are most important to PwMS. Medical recruiters from two sites in the USA (Detroit, MI; Raleigh, NC) contacted individuals within their databases who were interested in participating in qualitative research. Participants received $200 for their involvement and provided written informed consent. Ethical approval was obtained from RTI’s Institutional Review Board (ID number 14206). The research was performed in accordance with a protocol, the provisions of the International Conference on Harmonisation, the Declaration of Helsinki, and applicable local regulatory requirements and laws.
The study design specified the inclusion of 14 people matching the following inclusion criteria: aged 18–65 years; diagnosed with RRMS for less than 10 years; and able to provide completed diagnosis form, with clinician signature to confirm MS subtype and severity. The severity of MS was classified by the clinician as mild, moderate, or severe. Current or recent (last 30 days) participation in a clinical trial was an exclusion criterion (see Fig. 1). To confirm their MS diagnosis, subtype, and severity level, each participant had to provide a completed diagnosis verification form that was signed by a clinician.

Flowchart of the recruitment process, inclusion and exclusion criteria, and recruitment targets. MI Michigan, MS multiple sclerosis, NC North Carolina, PwMS people with multiple sclerosis, RRMS relapsing–remitting multiple sclerosis
The initial intention was to also interview people with primary progressive MS (PPMS). However, information gathered from the literature and clinical experts at the time of the study indicated there were no significant differences in the key symptoms or impacts by MS subtype (i.e., RRMS or PPMS), and interviews were limited to people with RRMS.
The recruitment targets for the total sample of 14 PwMS were four participants with a high school diploma or less; four non-White participants; four male participants; at least four participants for each severity rating (Fig. 1). These targets were included in an attempt to increase the diversity of the study sample with regard to self-reported race and educational attainment [34, 35]. In addition, it was hoped to reduce the overrepresentation of college-educated individuals by including those with a range of communication abilities and perceptions. Interviews were approximately 60 min and followed a semi-structured interview guide developed by the authors from RTI Health Solutions and Merck Healthcare KGaA, Darmstadt, Germany (see Supplementary Table 2 for an illustrative excerpt of the interview guide). Each interview was audio recorded and verbatim transcripts were created.
During the interviews, the interviewer provided each participant with an overview of the study and asked general questions intended to get them talking about their experiences with MS. The impact of MS on their daily lives was discussed. Participants were asked about the most important symptoms and effects of MS. If common symptoms or impacts were not reported by a participant, the interviewer confirmed whether the participant had experienced them. Both spontaneously reported and prompted symptoms and impacts were collected and are collated together when reported in the results.
Results
Demographics
A total of 14 PwMS (seven each from Detroit, MI and Raleigh, NC), with an average age of 43.9 years (range 25–64 years), took part in the CEIs. Most of the participants were White (78.6%) and female (78.6%). The mean duration since diagnosis was 6.6 years (range 2–10 years). The two cohorts were well balanced between sites for age, sex, ethnicity, and time since diagnosis (Table 1).
Most Common Symptoms and Impacts
Initially, participants were asked to describe the specific MS-related symptoms they experienced. Symptoms reported by at least 10 participants were cognitive dysfunction (n = 13), heat intolerance (n = 13), loss of balance/instability (n = 13), numbness/tingling in hands or feet (n = 13), fatigue/tiredness (n = 12), visual problems (n = 11), muscle spasm/tightness/spasticity (n = 11), and weakness/heaviness in limbs (n = 10). All the reported symptoms are shown in Fig. 2a.

Distribution of MS symptoms (a) and impacts (b) reported by CEI participants (n = 14). CEI concept elicitation interview, GI gastrointestinal, MS multiple sclerosis
Participants were subsequently asked to describe the impact of MS on their lives. The impacts reported by at least 10 participants were balance problems/instability (n = 13), work life/productivity (n = 12), difficulty walking (n = 11), daily activities/household chores (n = 11), leisure activities (hobbies, vacations; n = 10). Impact concepts broadly fell into the following themes: physical activities, work life/productivity, emotional, and social/relationships (Fig. 2b). To provide further context to the types of impacts experienced by PwMS, quotations from the interview transcripts related to each theme are included in Table 2.
Across the most frequently reported symptom and impact concepts, there was a high frequency of concepts associated with physical function (difficulty walking balance problems/instability; limitations in performing daily activities, household chores, and leisure pursuits) and fatigue (weakness or heaviness in the limbs; mental fatigue or cognitive dysfunction) in addition to concepts related to sensory-motor function (heat intolerance; numbness or tingling in the hands or feet; visual problems; muscle spasm, tightness, or spasticity). Quotations from the interview participants are included to provide rich detail and context for the effects of MS related to physical function and fatigue (Tables 3 and 4). Extended versions of these tables, which include a more comprehensive selection of quotations, are included in Supplementary Tables 3 and 4.
Some patterns in the presentation of symptoms and impacts were observed across subgroups of PwMS. For example, gastrointestinal problems, swallowing, vertigo/dizziness, and disturbed sleep were not reported by any participant with mild MS. Vision problems and bladder problems were mostly mentioned by participants with moderate or severe MS. With regards to the impacts of MS, none of the participants with mild MS had issues with climbing stairs, while those with moderate or severe MS commonly mentioned impacts on social life or family life. Surprisingly, problems with standing unsupported were more frequently reported by participants with mild MS.
Most Bothersome Effects of MS
PwMS were asked to report the first, second, and third most bothersome effects of MS, including symptoms or impacts. The reported concepts were then weighted by bothersomeness ranking (weights ranging from 1 [third most bothersome] to 3 [most bothersome]) and are presented in order of the summed weighted scores across the 14 PwMS (Table 5). Weighted scores ranged from 1 to 21; higher weighted scores indicate greater overall bothersomeness. Fatigue was reported as being the most bothersome concept, both when weighted and in frequency of reporting (weighted score = 21, n = 9). The other most bothersome concepts were mobility/walking difficulty (weighted score = 8, n = 3), cognitive dysfunction (weighted score = 8, n = 5), and vision problems (weighted score = 7, n = 3). Examples of the context in which these concepts were described as bothersome are included in Table 2.
Discussion
It is important for the development of well-defined and reliable PRO instruments that there is a detailed understanding of patients’ experiences, and specific disease concepts, prior to the development of PRO instruments [29]. This study aimed to identify the symptoms and impacts that PwMS experience which affect their daily lives; the in-depth patient experience narratives supported the development of novel PRO measures of fatigue and physical function that are currently in use in MS trials [27, 33]. The most important and bothersome impacts of RRMS identified by study participants were impairments in the following functional abilities: walking and being mobile, working and being productive, and performing daily activities and chores. These disease concepts are consistent with examples in the literature summarized in Supplementary Table 1 [7, 21, 36, 37]. However, as previously noted, the outcomes of such qualitative studies are sensitive to the methodologies used for elicitation. Moreover, the objective of this study was to gain insight into the concepts that are the most important and relevant for PwMS, not just those with the highest frequency. Given the objective of this study, it was not possible to provide detailed insights on certain aspects of MS, such as the broad spectrum of cognitive impairments or mental health impacts. The additional context provided in Tables 3 and 4 enables greater understanding of the physical function- and fatigue-related concepts that can be gained by studying frequency of symptoms and impacts alone.
With respect to the frequency of the most important symptom/impact concepts for participants in this study, the findings were generally consistent with those reported in similar studies. For example, fatigue, vision problems, pain, muscle spasms, and impacts on participation in physical activities and working are commonly reported [4, 7, 21, 37,38,39,40]. One of the main differences with surveys of larger populations is the frequency with which bladder problems were reported. Larger cohort studies often identify bladder/bowel problems as one of the most frequently experienced symptoms among PwMS [7, 21]. In this study, bladder issues were reported by 8/14 participants. This relatively lower frequency is explained by the qualitative nature of this study, study objectives, and outcome measures, and the MS subtypes and severity levels of the participants. For example, although several emotional impacts were identified (mood/emotions, psychological distress, lack of control/frustration with limitations), studies that specifically assessed mental health and psychological impacts described symptoms of depression and anxiety in more detail [28, 41]. We postulate that the unexpected observation that participants with mild MS reported problems with standing unsupported more frequently than those with moderate/severe MS is likely to be, at least in part, because those with moderate or severe MS may already require some support to stand up, which they are used to, and as such they do not reflect on their ability to stand without support; in other words, their expectations have shifted. Socioeconomic issues and healthcare system experiences were not described. It should also be noted that the frequency of reported concepts, in particular impacts, may vary by country; this study was conducted in the USA only.
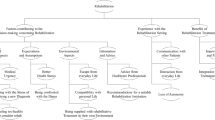
The summary outputs of the CEIs, together with the additional context provided from quotations (Tables 2, 3, and 4) and relevant literature in the field, were used to generate a conceptual model of MS (Fig. 3). This model captures the disease symptoms, functional impairments and psychosocial impacts identified in the interviews of people with RRMS, as well as known disease processes and symptoms of RRMS, SPMS, and PPMS identified in the literature, and patient- and disease-related variables, including age and duration of MS disease. This model can help to inform future MS trials, particularly in providing a patient viewpoint supporting selection of outcomes. In addition, on the basis of the conceptual model, self-reported symptoms such as fatigue and pain, as well as impacts such as walking ability and physical functioning, have potential as targets for PRO measures owing to their proximity to the disease. Breaking down the disease into these separate aspects provides insight supporting the development of PRO measures and other clinical outcome assessments, as it summarizes feedback from PwMS that can inform endpoints in clinical trials or decisions regarding clinical care. However, it should be noted that MS-related symptoms often have complex and overlapping effects; for example, difficulty walking and fatigue may both contribute to an impaired ability to climb stairs.

Conceptual model of MS developed on the basis of the findings from interviews of people with RRMS and further informed by a literature search including studies evaluating the experiences of people with RRMS, SPMS, and PPMS. It should be noted that MS-related symptoms often have complex and overlapping effects; for example, difficulty walking and fatigue may both contribute to an impaired ability to climb stairs. CNS central nervous system, MS multiple sclerosis, PPMS primary progressive multiple sclerosis, RRMS relapsing–remitting MS, SPMS secondary progressive multiple sclerosis
Implications for Outcomes Measurement
Regulatory bodies such as the EMA and FDA recognize the importance of the appropriate assessment of how PwMS feel and function, to provide a holistic evaluation of disability and support evidence of treatment benefit in MS. Generic PROs including the Short Form Health Survey 36 (SF-36) have been used as an indicator of perceived general health in PwMS, allowing comparisons with people with other chronic conditions and the general population [42]. However, generic PROs may contain irrelevant questions that can make PwMS feel alienated, and they may not assess concepts important to PwMS [43]. The development of MS-specific PRO measures, including measures that focus on specific types of disability and disability impact, is therefore critical.
The concepts identified in the CEIs and incorporated in the conceptual model are key to the development of targeted PRO instruments for MS. Assessment of fatigue by PROs is considered important by the EMA in providing a complete picture of disability [44]. Four MS-specific clinical outcome assessments have been submitted to the FDA Clinical Outcome Assessment qualification program, which will conclude whether the assessments are well defined and reliable for use in MS [45]: PROMIS Fatigue (MS) 8a [27], PROMIS Physical Function (MS) 15a [33], Symbol Digit Modality Test (processing speed) [46], and Actibelt® in MS (real-world walking speed) [47]. Concepts identified relating to fatigue, pain, walking ability, and performance of different activities, therefore, have potential as targets for endpoint design and development, and could be informative if included in labeling language for MS therapies [29]. The specific physical function-related concepts elicited in this interview study directly contributed to the development of the PROMIS Physical Function (MS) 15a instrument [33], and also supported the content validity of the PROMIS Fatigue (MS) 8a instrument [27]. Importantly, both instruments demonstrated strong evidence of validity in MS and were found to have robust psychometric properties [27, 33].
Self-reporting of symptoms early in the disease course may benefit treatment strategies [17, 48]. PROs have scope to play an important role in describing symptom development and progression in MS disease processes, particularly in the context of disability progression independent of relapse activity [49]. PROs may also provide an approximate means to assess disease progression before it would typically be captured through routine clinical assessments, which may occur annually or less frequently. Regular self-reporting of changes in physical function, cognition, or fatigue via PRO measures may be a beneficial strategy to track disease course, complementing suggested clinical composite measures and screening using neuroimaging [10, 13, 15, 50]. Appropriately developed PRO measures may be more patient friendly than clinical assessments and allow for greater patient-centricity in MS treatment pathways. In addition, for concepts such as fatigue and cognitive dysfunction, PROs may be more sensitive to a broader range of symptoms than established clinical assessments, potentially helping to identify additional signs and symptoms of progression that are not related to relapse activity in MS.
Limitations
One potential limitation of the CEIs in this study is the sample size. Formal sample size calculations based on hypothesis testing were not performed because of the qualitative nature of the study, although a sample size of 14 was anticipated to achieve saturation of concepts. Following completion of the 14 interviews, concept saturation was evaluated, and no further interviews were deemed necessary, although the study protocol allowed for them if required. Furthermore, the sample size used in this study is consistent with similar CEI studies performed in MS [26, 37] and the findings were generally consistent with those of the 27 studies identified in the targeted literature review (total > 56,000 PwMS).
This study sample, including only people with RRMS, may also be a limitation. Symptoms such as depression, pain, and walking difficulty have been found to impact quality of life across all three of the MS subtypes; however, recent large cohort studies have found some differences among the frequency and relative significance of concepts reported by people with RRMS, PPMS, and SPMS [6, 21, 51], and reported differences may be confounded by severity and disability levels. There are additional limitations in relation to the degree of inference that can be drawn from qualitative interviews. Qualitative research, by definition, does not support statistical inference to larger populations. Rather, the objective of qualitative research is to capture an in-depth view of individual experiences, including the subjective and nuanced aspects of experiential knowledge, as well as the language that individuals use to describe their condition and its effects. These objectives are particularly important in CEIs conducted as the basis of developing fit-for-purpose PRO measures. In subsequent development and evaluation studies of the PROMIS Fatigue (MS) 8a and PROMIS Physical Function (MS) 15a instruments, sample sizes were expanded in line with best practice standards of psychometric testing [27, 33]. It should be noted that the research team felt it was important to present the classification of symptoms and impacts that organically emerged from the interviews. For example, “balance problems/instability” was listed as an impact as it was reported by PwMS in response to questions/prompts specifically related to disease impacts. As balance problems are a disease symptom, they were considered as such in the conceptual model. A further consideration is that the interviews were conducted in the USA only, reflecting the focus of the overall PRO measure development research program on the USA healthcare system. Further investigations in other locations and cultural contexts may reveal additional important concepts for PwMS.
Conclusions
This study identified symptoms and impacts related to the experiences of people with RRMS and formulated a conceptual model of MS; this is important to ensure that symptoms and impacts that matter most to PwMS are considered for the development of fit-for-purpose PRO instruments. Fatigue and cognitive dysfunction were among the most bothersome symptoms identified and impacts on walking ability and physical functioning were commonly reported. Standardized assessment of experiences of PwMS, based on self-reported outcomes, requires further development to become part of formal disability assessment. The development of appropriate PRO instruments, sensitive to key MS symptoms and impacts, will benefit the design of clinical trials and the development of MS therapies. More fundamentally, well-designed PRO instruments, developed in collaboration with PwMS [52], provide tools for increased patient-centricity in MS treatment, increasing the potential for earlier recognition of disease progression, and may support the understanding of disease processes such as silent progression [10, 13] and progression independent of relapse activity [15]. The concepts identified in this study underpin the appropriateness and content validity of the PROMIS Fatigue (MS) 8a and the PROMIS Physical Function (MS) 15a [27, 33] and the conceptual model further supports their use in clinical trials and clinical care in MS.
Data Availability
Any requests for data by qualified scientific and medical researchers for legitimate research purposes will be subject to Merck Healthcare KGaA, Darmstadt, Germany’s Data Sharing Policy. All requests should be submitted in writing to Merck Healthcare KGaA, Darmstadt, Germany’s data sharing portal. When Merck Healthcare KGaA, Darmstadt, Germany, has a co-research, co-development, or co-marketing or co-promotion agreement, or when the product has been out licensed, the responsibility for disclosure might be dependent on the agreement between parties. Under these circumstances, Merck Healthcare KGaA, Darmstadt, Germany, will endeavor to gain agreement to share data in response to requests.
References
Filippi M, Bar-Or A, Piehl F, et al. Multiple sclerosis. Nat Rev Dis Primers. 2018;4(1):43.
Compston A, Coles A. Multiple sclerosis. Lancet. 2008;372(9648):1502–17.
Hauser SL, Cree BAC. Treatment of multiple sclerosis: a review. Am J Med. 2020;133(12):1380-90.e2.
Newland PK, Thomas FP, Riley M, Flick LH, Fearing A. The use of focus groups to characterize symptoms in persons with multiple sclerosis. J Neurosci Nurs. 2012;44(6):351–7.
Kister I, Bacon TE, Chamot E, Salter AR, Cutter GR, Kalina JT, Herbert J. Natural history of multiple sclerosis symptoms. Int J MS Care. 2013;15(3):146–58.
Barin L, Salmen A, Disanto G, et al. The disease burden of multiple sclerosis from the individual and population perspective: which symptoms matter most? Mult Scler Relat Disord. 2018;25:112–21.
Rommer PS, Eichstädt K, Ellenberger D, et al. Symptomatology and symptomatic treatment in multiple sclerosis: results from a nationwide MS registry. Mult Scler J. 2019;25(12):1641–52.
Feys P, Giovannoni G, Dijsselbloem N, Centonze D, Eelen P, Lykke AS. The importance of a multi-disciplinary perspective and patient activation programmes in MS management. Mult Scler J. 2016;22(2_suppl):34–46.
Kuhlmann T, Moccia M, Coetzee T, et al. Multiple sclerosis progression: time for a new mechanism-driven framework. Lancet Neurol. 2023;22(1):78–88.
Giovannoni G, Popescu V, Wuerfel J, et al. Smouldering multiple sclerosis: the 'real MS'. Ther Adv Neurol Disord. 2022;15. https://doi.org/10.1177/17562864211066751.
Cagol A, Schaedelin S, Barakovic M, et al. Association of brain atrophy with disease progression independent of relapse activity in patients with relapsing multiple sclerosis. JAMA Neurol. 2022;79(7):682–92.
Elliott C, Wolinsky JS, Hauser SL, et al. Slowly expanding/evolving lesions as a magnetic resonance imaging marker of chronic active multiple sclerosis lesions. Mult Scler. 2019;25(14):1915–25.
Cree BAC, Hollenbach JA, Bove R, et al. Silent progression in disease activity-free relapsing multiple sclerosis. Ann Neurol. 2019;85(5):653–66.
Sucksdorff M, Matilainen M, Tuisku J, et al. Brain TSPO-PET predicts later disease progression independent of relapses in multiple sclerosis. Brain. 2020;143(11):3318–30.
Kappos L, Wolinsky JS, Giovannoni G, et al. Contribution of relapse-independent progression vs relapse-associated worsening to overall confirmed disability accumulation in typical relapsing multiple sclerosis in a pooled analysis of 2 randomized clinical trials. JAMA Neurol. 2020;77(9):1132–40.
Inojosa H, Proschmann U, Akgün K, Ziemssen T. Should we use clinical tools to identify disease progression? Front Neurol. 2020;11:628542.
Thrue C, Riemenschneider M, Hvid L, Stenager E, Dalgas U. Time matters: early-phase multiple sclerosis is accompanied by considerable impairments across multiple domains. Mult Scler J. 2021;27(10):1477–85.
Mountford S, Kahn M, Balakrishnan P, et al. Correlation and differences of patient-reported outcomes vs. Likert-rating of MS symptoms in a real-world cohort using a digital patient app. Digit Health. 2023;9:20552076231173520.
Khan F, Pallant JF. Use of International Classification of Functioning, Disability and Health (ICF) to describe patient-reported disability in multiple sclerosis and identification of relevant environmental factors. J Rehabil Med. 2007;39(1):63–70.
Newland PK, Lorenz R, Budhathoki C, Jensen MP. The presence of symptoms with comorbid conditions in individuals with multiple sclerosis (MS). Clin Nurs Res. 2016;25(5):532–48.
Zhang Y, Taylor BV, Simpson S, et al. Feelings of depression, pain and walking difficulties have the largest impact on the quality of life of people with multiple sclerosis, irrespective of clinical phenotype. Mult Scler J. 2021;27(8):1262–75.
Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurol. 1983;33(11):1444–52.
Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17(2):162–73.
Inojosa H, Schriefer D, Ziemssen T. Clinical outcome measures in multiple sclerosis: a review. Autoimmun Rev. 2020;19(5):102512.
van’t Hullenaar CAA, Coerver E, Kalkers NF, et al. The use of multi-domain patient reported outcome measures for detecting clinical disease progression in multiple sclerosis. Mult Scler Relat Disord. 2021;55:103165.
Hudgens S, Schuler R, Stokes J, Eremenco S, Hunsche E, Leist TP. Development and validation of the FSIQ-RMS: a new patient-reported questionnaire to assess symptoms and impacts of fatigue in relapsing multiple sclerosis. Value Health. 2019;22(4):453–66.
Kamudoni P, Johns J, Cook KF, et al. Standardizing fatigue measurement in multiple sclerosis: the validity, responsiveness and score interpretation of the PROMIS SF v1.0 Fatigue (MS) 8a. Mult Scler Relat Disord. 2021;54:103117.
Prakash RS, Schirda B, Valentine TR, Crotty M, Nicholas JA. Emotion dysregulation in multiple sclerosis: Impact on symptoms of depression and anxiety. Mult Scler Relat Disord. 2019;36:101399.
Food and Drug Administration. Patient-reported outcome measures: use in medical product development to support labeling claims. 2009. https://www.fda.gov/downloads/drugs/guidances/ucm193282.pdf. Accessed 14 Apr 2023.
European Medical Agency. Guideline on clinical investigation of medicinal products for the treatment of multiple sclerosis. 2015. http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2015/03/WC500185161.pdf. Accessed 14 Apr 2023.
Zaratin P, Vermersch P, Amato MP, Brichetto G, Coetzee T, Cutter G, et al. The agenda of the global patient reported outcomes for multiple sclerosis (PROMS) initiative: Progresses and open questions. Mult Scler Relat Disord. 2022;61: 103757.
Scholz M, Haase R, Trentzsch K, Stölzer-Hutsch H, Ziemssen T. Improving Digital Patient Care: Lessons Learned from Patient-Reported and Expert-Reported Experience Measures for the Clinical Practice of Multidimensional Walking Assessment. Brain Sci. 2021;11(6):786.
Kamudoni P, Amtmann D, Johns J, et al. The validity, responsiveness, and score interpretation of the PROMISnq Physical Function Multiple Sclerosis 15a short form in multiple sclerosis. Mult Scler Relat Disord. 2022;62:103753.
Cohen MZ, Phillips JM, Palos G. Qualitative research with diverse populations. Semin Oncol Nurs. 2001;17(3):190–6.
Mateen FJ. Is It Time for Quotas to Achieve Racial and Ethnic Representation in Multiple Sclerosis Trials? Front Neurol. 2021;12:680912.
Westergaard K, Skovgaard L, Magyari M, Kristiansen M. Patient perspectives on patient-reported outcomes in multiple sclerosis treatment trajectories: A qualitative study of why, what, and how? Mult Scler Relat Disord. 2022;58:103475.
Matza LS, Stewart KD, Phillips G, Delio P, Naismith RT. Development of a brief clinician-reported outcome measure of multiple sclerosis signs and symptoms: the Clinician Rating of Multiple Sclerosis (CRoMS). Mult Scler Relat Disord. 2019;35:253–61.
Larocca NG. Impact of walking impairment in multiple sclerosis: perspectives of patients and care partners. Patient. 2011;4(3):189–201.
Campos-Lucas FJ, Fernández-Fernández Ó, Monge-Martín D, Moral-Torres E, Carrascal-Rueda P, Caballero-Martínez F. The evolution of multiple sclerosis in Spain over the last decade from the patient’s perspective. Mult Scler Relat Disord. 2022;57: 103355.
Harrison AM, Bogosian A, Silber E, McCracken LM, Moss-Morris R. “It feels like someone is hammering my feet”: understanding pain and its management from the perspective of people with multiple sclerosis. Mult Scler. 2015;21(4):466–76.
Maurino J, Martínez-Ginés ML, García-Domínguez JM, et al. Workplace difficulties, health-related quality of life, and perception of stigma from the perspective of patients with multiple sclerosis. Mult Scler Relat Disord. 2020;41:102046.
Krokavcova M, Van Dijk JP, Nagyova I, et al. Perceived health status as measured by the SF-36 in patients with multiple sclerosis: a review. Scand J Caring Sci. 2009;23(3):529–38.
D’Amico E, Haase R, Ziemssen T. Review: Patient-reported outcomes in multiple sclerosis care. Mult Scler Relat Disord. 2019;33:61–6.
European Medical Agency. Qualification opinion on multiple sclerosis clinical outcome assessment (MSCOA). 2020. https://www.ema.europa.eu/en/documents/other/qualification-opinion-multiple-sclerosis-clinical-outcome-assessment-mscoa_en.pdf. Accessed 14 Apr 2023.
Food and Drug Administration. Clinical Outcome Assessments (COA) qualification program submissions. 2021. https://www.fda.gov/drugs/clinical-outcome-assessment-coa-qualification-program/clinical-outcome-assessments-coa-qualification-program-submissions. Accessed 14 Apr 2023.
Benedict RH, DeLuca J, Phillips G, LaRocca N, Hudson LD, Rudick R. Validity of the Symbol Digit Modalities Test as a cognition performance outcome measure for multiple sclerosis. Mult Scler J. 2017;23(5):721–33.
Motl RW, Weikert M, Suh Y, et al. Accuracy of the actibelt® accelerometer for measuring walking speed in a controlled environment among persons with multiple sclerosis. Gait Posture. 2012;35(2):192–6.
Ziemssen T. Symptom management in patients with multiple sclerosis. J Neurol Sci. 2011;311(Suppl 1):S48–52.
Voigt I, Inojosa H, Wenk J, Akgün K, Ziemssen T. Building a monitoring matrix for the management of multiple sclerosis. Autoimmun Rev. 2023;22(8):103358.
Cadavid D, Cohen JA, Freedman MS, et al. The EDSS-Plus, an improved endpoint for disability progression in secondary progressive multiple sclerosis. Mult Scler J. 2017;23(1):94–105.
Ziemssen T, Tolley C, Bennett B, et al. A mixed methods approach towards understanding key disease characteristics associated with the progression from RRMS to SPMS: physicians’ and patients’ views. Mult Scler Relat Disord. 2020;38:101861.
Bharadia T, Vandercappellen J, Chitnis T, et al. Patient-reported outcome measures in MS: do development processes and patient involvement support valid quantification of clinically important variables? Mult Scler J Exp Transl Clin. 2022;8(2):20552173221105640.
Acknowledgements
We would like to thank those who took part in the study.
Medical Writing and Editorial Assistance
Medical writing and editorial support were provided by Samantha Lommano of Bioscript Group Ltd, Macclesfield, UK, funded by Merck Healthcare KGaA, Darmstadt, Germany.
Funding
This study was sponsored by Merck Healthcare KGaA, Darmstadt, Germany (CrossRef Funder ID: 10.13039/100009945), who contracted RTI Health Solutions to conduct the interviews. Merck Healthcare KGaA, Darmstadt, Germany funded medical writing and editorial support by Bioscript Group Ltd, Macclesfield, UK, and paid the journal’s Rapid Service Fee.
Author information
Authors and Affiliations
Contributions
Amy Barrett, Oyebimpe Olayinka-Amao, Christian Henke and Paul Kamudoni contributed to the study conception and design. Material preparation, data collection and data analysis were performed by Amy Barrett and Oyebimpe Olayinka-Amoa. All authors contributed to interpretation of the results, reviewed and commented on previous versions of the manuscript, and read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of Interest
Amy Barrett and Oyebimpe Olayinka-Amao are employees of RTI Health Solutions. Tjalf Ziemssen reports consulting or serving on speaker bureaus for Biogen, Celgene, Roche, Novartis, Celgene, Merck Healthcare KGaA, Darmstadt, Germany, and Sanofi, as well as research support from Biogen, Novartis, Merck Healthcare KGaA, Darmstadt, Germany, and Sanofi. Trishna Bharadia has received honoraria and/or consulting fees from AbbVie, Becaris, King’s College London, Lumanity, Blue Latitude Health, Curatio, University College London, MS International Federation, Future Science Group, Savvy Cooperative, WEGO Health, Prime Global, Eyeforpharma, Professional Record Standards Body, DODS D&I, Queen Mary University London, Merck Healthcare KGaA, Darmstadt, Germany, The Method, Clara Health, The Conference Forum, Greenphire, Hollister, Medable, Oxford Health Policy Forum, College of Contemporary Health, Pfizer, Bristol Myers Squibb, UCB, Medidata, Talking Medicines, Pivot Digital, NHS England, Boeringher Ingelheim, MSD, Novartis, Parexel, Roche, Roche Information Solutions, Teva, and Sandoz. Christian Henke and Paul Kamudoni are employees of Merck Healthcare KGaA, Darmstadt, Germany.
Ethical Approval
Ethical approvals were obtained from RTI’s Institutional Review Board (ID number 14206). The research was performed in accordance with the protocol, the provisions of the International Conference on Harmonisation, the Declaration of Helsinki, and applicable local regulatory requirements and laws.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Barrett, A., Olayinka-Amao, O., Ziemssen, T. et al. Understanding the Symptoms and Impacts Experienced by People with Relapsing–Remitting MS: A Qualitative Investigation Using Semi-Structured Interviews. Neurol Ther 13, 449–464 (2024). https://doi.org/10.1007/s40120-024-00584-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40120-024-00584-y