
Abstract
Introduction
Critical gaps exist in the understanding of the continuum of multiple sclerosis (MS) progression, particularly with regard to the patient experience prior to and during the transition from relapsing–remitting MS (RRMS) to secondary-progressive MS (SPMS) stages. To date, there are no clear diagnostic criteria in the determination of the clinical transition. We report here the use of patient experience data to support the development of a qualitative conceptual model of MS that describes the patient journey of transition from active-relapsing disease to progressive MS.
Methods
The study used a single-encounter, multicenter, qualitative observational study design that included a targeted literature review and individual, in-depth interviews with adult patients with a clinically confirmed diagnosis of SPMS and their adult care partners. Descriptions of symptoms and impacts of RRMS and SPMS were extracted from the literature review and used to support development of the interview guide and conceptual model.
Results
Participants described a slow progression in terms of change in symptoms over time, including both the development of new symptoms and the worsening of existing symptoms.
Conclusions
The conceptual model of the transitionary period from RRMS to SPMS expands the current understanding of the progression of MS from the patient and care partner perspectives.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Critical gaps exist in understanding the continuum of multiple sclerosis (MS) progression, particularly specific to the patient experience prior to and during the transition from relapsing–remitting MS (RRMS) to secondary-progressive MS (SPMS). |
This study explored patient and care partner perspectives of MS progression, emphasizing the understanding of transition from RRMS to SPMS. |
What was learned from the study? |
The developed conceptual model depicts the patient journey, including both progression and the impact of progression, and may be useful in helping to determine factors that lead to the transition point of SPMS. |
Consideration of the patient experience through the transition process by elucidating patient views, concerns, and preferences may be useful to health care providers and other stakeholders as they seek to provide timely and relevant care to patients with SPMS. |
Feedback from patients and care partners in this qualitative study underscores the need for availability of a tool to identify early signs of MS progression and further augment patient-clinician communication related to disease state and management. |
Introduction
Multiple sclerosis (MS) is a progressive central nervous system (CNS) disease affecting a wide range of functions. Throughout the disease continuum, some symptoms tend to appear, disappear, and reappear [1], while others remain for long periods. Although the progression of MS is unpredictable, its phenotypes can be categorized as relapsing or progressive. These categories, however, do not provide information about the ongoing disease process. Clinical evidence of disease progression is often independent of relapses over a period of time in patients who have a progressive disease course. Progressive disease, either primary-progressive MS or secondary-progressive MS (SPMS), may remain relatively stable over periods of time, during which progression must be determined by patient history or objective measure of change (i.e., evidence of lesions). Both relapsing and progressive disease may be characterized by severity of signs and symptoms, relapses, worsening disability, and impairment [2], but these characteristics do not provide sufficient evidence of active disease course. In fact, incomplete recovery from acute relapse can be indicative of disease worsening over time. SPMS is diagnosed retrospectively via history of gradual worsening after an initial relapsing disease course, with or without acute exacerbations during the progressive course [2]. Despite this characterization of the clinical course of MS, critical gaps exist in understanding the continuum of MS progression, particularly specific to the patient experience prior to and during the transition from relapsing-remitting MS (RRMS) to SPMS. To date, no clear diagnostic criteria exist that define the clinical transition.
In this study, we explored patient and care partner perspectives of MS progression, emphasizing the understanding of transition from RRMS to SPMS. Patient experience data were used to develop a qualitative conceptual model of MS describing the patient journey of transition from active-relapsing disease to progressive MS, integrated clinical and psychological aspects of health outcomes, and proposed specific relationships between the different health outcomes. By exploring the transition process from the perspective of both the patient and the care partner, the model may improve patient outcomes through identifying factors that lead to the transition from RRMS to SPMS.
Methods
Study design
The study used a single-encounter, multicenter, qualitative observational study design including a targeted literature review and individual, in-depth interviews with dyads of adult patients with a clinically confirmed diagnosis of SPMS and their adult care partners. Care partner was defined as a nonmedical provider who is in daily or near daily contact with the patient. The term care partner was used instead of care giver to emphasize the inclusive role of these individuals and the autonomous participation of the patient receiving care. The interview component of this study was approved by the RTI Institutional Review Board (Federal-Wide Assurance #3331). The study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments. Participants provided written informed consent to participate and for publication of study results. A convenience sample was employed in this study, as supported by 2020 Food and Drug Administration (FDA) guidance [3] for the collection of patient experience data, and concept saturation, the point at which interviews yield no new information, was monitored and documented using a saturation grid. Participants were identified via medical record review by physician investigators. Inclusion criteria required patients be aged 35–65 years, have a care partner 18 years or older, and have a clinician-verified diagnosis of MS for at least 8 years with progression. Additionally, patients had to have confirmed accumulation of disability either through an Expanded Disability Status Scale (EDSS) score ≥ 3 or an equivalent clinical presentation based on physician assessment. Participants were excluded if they self-reported a concurrent diagnosis of any other neurologic or neuromuscular disease. Participants meeting eligibility criteria were scheduled for telephone interviews. The semistructured interviews were conducted to capture feedback describing the patient journey of transition from RRMS to SPMS. Interview transcripts were prepared that underwent a structured quality review.
Literature Review and Interview Structure
A literature search of the MEDLINE database (Electronic Supplementary Material Table S-1), targeting publications since 2007, identified 145 abstracts, from which 29 articles were selected for full-text review. The review focused on identification of concepts deemed most meaningful from the patient and care partner perspective. Concepts were extracted from 11 articles, informing development of a semistructured interview guide [4,5,6,7,8,9,10,11,12,13,14].
The use of semistructured guides allows flexibility to follow the conversation and gather rich data. The overarching concepts included within the guides were explored in depth; however, the interviewers followed the natural flow of conversation to allow participants to fully express their ideas and experiences. Interviews explored high-level concepts, including the awareness of change in disease status, reaction to the new diagnosis, the reality of living with progressive disease, health care experiences surrounding transition, and thoughts related to the future. All interviews were conducted by independent researchers with extensive experience in leading qualitative research who have conducted interviews across a wide variety of therapeutic areas and who were unaffiliated with the participants’ health care.
Data Analysis and Conceptual Model Building
Interviewer field notes and transcripts were used to analyze interview data. Standard qualitative analysis methods were used to identify, characterize, and summarize patterns found in the interview data. Constant comparative analysis [3] methodology was utilized. Dominant trends were identified in each interview and compared across the results of other interviews to generate themes or patterns in the way participants described their experiences. Concepts gleaned from interviews, in conjunction with the targeted literature review, were used to develop a conceptual model of disease progression in MS. The model included key concepts, definitions, and information on how concepts are related to one another and to key outcomes of interest.
Results
Targeted Literature Review
Descriptions of symptoms and impacts of RRMS and SPMS were extracted from the literature. The synthesized results of the review that were used to support development of the interview guide and conceptual model are described here. Symptoms of MS are variable and unpredictable but may include fatigue, pain, loss of function or feeling in the legs, loss of balance and coordination, slurring of speech, loss of bowel or bladder control, sexual dysfunction, loss of cognitive functioning, and emotional changes [4, 13]. These symptoms of MS, coupled with the progressive and irreversible functional disability that some patients experience, can have a profound impact on all aspects of patients’ lives. SPMS develops in approximately 85% of those with RRMS within 20 years of onset [5], although recent improvement in treatment options may reduce this frequency. The median time to SPMS transition is consistently reported at around 20 years [8]. Neither imaging criteria nor biomarkers are available to objectively distinguish RRMS from SPMS; therefore, SPMS is diagnosed retrospectively [4]. The transition from RRMS to SPMS is a period of diagnostic uncertainty that may last for several years (3 years on average) [6, 9].
SPMS is characterized by the progressive accumulation of disability over at least 6 months after an initial RR course, with or without acute exacerbations during progression. Patients with SPMS are likely to have higher scores of depression and anxiety, tend to lose emotional control more easily, and demonstrate worse scores on all dimensions of quality of life [10]. Three articles identified in the literature review discussed the patient experience with the transition from RRMS to SPMS [5, 6, 12]. Each of these three UK-based studies were based on qualitative interviews with patients. Consistent themes around patient experiences with transition emerged from all three papers (Table 1).
Interviews
A total of 19 in-depth, individual interviews were conducted (patients, n = 10; care partners, n = 9) (Table 2). The mean patient age was 52.2 years, the majority of respondents were female (70%) and Caucasian (60%), and educational status represented a range of levels. Scores on the EDSS ranged from 4 to 7. Most symptoms and impacts were identified following completion of the fourth dyad. With the exception of the impact concept of “rarely leaves the house,” no new concepts were raised following the conclusion of the interview with the seventh dyad. All symptom and impact item concepts identified during the literature review were endorsed by patients with MS and their care partners. These combined results provide further evidence of concept saturation, supporting finalization of the conceptual disease model.
RRMS Diagnosis and Symptoms
While a variety of symptoms and impacts were noted prior to transition, fatigue was the symptom most predominantly reported by interview participants (73.7%). Additional symptoms that were highly endorsed (reported by at least 50% of respondents) included bladder incontinence, problems walking, numbness/tingling in hands and feet, and spasms (Table 3). The most commonly reported impacts were professional (i.e., the need to stop working) and emotional; both of these impacts were endorsed by 52.6% of interview participants (Table 4). Participants noted that the need to stop working resulted from overwhelming fatigue as well as cognitive impacts. Participants also expressed functional, social, and emotional impacts due to RRMS. The most commonly reported functional impacts included those related to physical activity and mobility (47.4%). Other functional impacts reported by at least 20% of respondents included those related to hobbies or recreational activities and the ability to engage in or complete household chores. Impacts specific to social relationships were reported by 47.4% of participants, with impacts specific to family life also reported (31.6%).
Disease Progression Diagnosis
Sample participant reactions to the news of progression can be found in Table 5. Participants reported receiving minimal or no information about the possibility of progression of MS. While some did not recall any conversation with their physician, other participants noted engaging in minimal discussion with their health care provider (HCP) or doing some research on their own. Participants reported that diagnoses of progression came between 1 and 14 years after initial diagnosis with MS (median, 7–10 years) but noted that little to no information was provided specific to how the diagnosis was made. Participants indicated that, in some instances, the HCP suggested that the disease had likely progressed, but did not offer a clear diagnosis; in other cases, participants shared that HCPs were reluctant to apply an SPMS diagnosis because of potential limitations accessing medication. Participants indicated that most discussions with their HCP occurred over time, as the elapsed time to progression of MS was slow.
Initial reactions to the news of progression ranged from fear and depression to understanding and acceptance. While participants described modifications in treatment throughout the course of their disease, none reported specific treatment modifications made at the time of diagnosis to SPMS. One participant described a conversation about progression in which her physician conveyed being “sorry,” but noted that “there [wasn’t] anything [treatment] available at that time.” Two participants expressed a desire for their physician to approach the discussion more optimistically (with “hope”). Three participants indicated that the initial diagnosis of transition was overwhelming and frightening, and the tone of the conversation was very bleak.
Participants described a slow progression in terms of change in symptoms over time, including both the development of new symptoms and the worsening of existing symptoms. Specifically, participants highlighted worsening fatigue, a decline in mobility/ambulation, and deteriorating cognitive effects. Issues with bladder incontinence (reported by 84% of participants) and cognitive dysfunction were also reported by a majority of the sample (80%). Symptoms of SPMS described by participants were generally more severe than those experienced before the transition and occurred without periods of remission (Table 6). Overall, impacts specific to mobility limitations (89%), household chores (79%), daily activities (58%), and socialization (63%) were highly endorsed (Table 7).
Care partners described MS as having both a physical and emotional toll on their own lives as they tried to assist and respond to patient needs, while reminding themselves to be patient and understanding. Care partners commented on challenges they encountered in physical aspects of care relating to assisting in dressing and frustration or disappointment in the difficulty of finding places to take the patient outside of the home. Paid care partners wanted to ensure they had accomplished enough for the patient during the limited time they were in the home, noting that sometimes it was hard to get to everything if the patient was having a difficult day. Finally, familial care partners described the fear of the unknown, fear of what was going to happen next, and uncertainty as to whether they would be equipped to continue to care for the patient.
Conceptual model
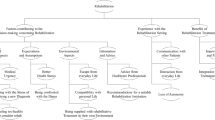
Data from the targeted literature review and participant interviews were used to build the conceptual model (Fig. 1). Participant feedback confirmed the continuum of interrelated concepts as hypothesized from the literature and expert review. Participant responses informed minor changes to the preliminary model. Specifically, the absence of periods of remission was added to mediating factors. Descriptions of emotional impacts were refined to add descriptive terms related to broader concepts of independence and sense of self. Impacts specific to social functioning were expanded, and additional descriptions of concepts raised by participants were included. Productivity was called out and further defined by aspects related to work and employment impacts.

Conceptual model of transition to SPMS. RRMS Relapsing-remitting multiple sclerosis, SPMS secondary-progressive multiple sclerosis
Discussion
The key milestone of this research included the development and refinement of a qualitative conceptual disease model. Conceptual model development serves as the foundational basis to identify and refine concepts of interest from an inclusive stakeholder perspective and demonstrates interdependent relationships that depict both disease symptoms and impacts and the additional factors that may influence overall well-being. The model integrated clinical and psychological aspects of health outcomes and proposed specific relationships between the different components. The model depicted the patient journey, including both progression and the impact of progression, and may be useful in helping to determine factors that lead to the transition point of SPMS. In evaluating the effect of therapy, the model provided the rationale for identifying outcomes of interest that are both clinically relevant and meaningful to patients and can provide further support during regulatory decision making for product approval and labeling [15]. This model serves to fill a gap in the literature, where qualitative work regarding the transition from RRMS to SPMS has been limited to small studies conducted in the UK [5, 6, 12]. A recently published article [16] described a mixed-methods approach, including qualitative interviews with 32 patients and 16 neurologists in the USA and Germany as well as quantitative analysis of real-world observational data from 3294 individuals with MS. The study explored and characterized key symptoms and impacts associated with the transition from RRMS to SPMS to support development of a clinical tool to support early evaluation of signs of progressive disease in a standardized manner. This study reinforced our own findings that the transition period is associated with impacts to ambulation or motor functions, daily activities, and employment. The conceptual model presented here serves as a basis for furthering understanding and fostering improved communication between HCPs and their patients by providing insight into patient views, concerns, and preferences within the context of managing the transition to SPMS.
The interviews confirmed the continuum of interrelated concepts. Prior to transition, fatigue was the symptom most predominantly reported by participants, and this symptom significantly impacted patients’ ability to maintain employment. Upon transition, symptoms of fatigue, symptoms related to mobility, issues with incontinence, and cognitive dysfunction continued to be important to patients. Participants especially noted impacts to mobility limitations, daily activities, and socialization. Care partner reports were noted to be particularly valuable with regard to providing information on cognitive impairment and mood changes, two concepts related to MS about which patients may have had less objective insight and for which care partner reports offered an essential complement to the patient’s self-report. The slow decline over time was described as a difficult experience for patients, with participants noting fears related to future impacts as well as lack of available treatment options. Participants also reported a lack of communication about the possibility of progression of MS, which could be improved through educational outreach to patients on the signs of transition that could potentially lead to earlier diagnosis of progression. Digital tools to improve clinical evaluation and monitoring in patients, such as MSProDiscuss and Floodlight, could also be used to identify early signs of MS progression [17, 18]. Once diagnosed with progression, patient discussions with HCPs regarding their diagnosis were reported to be inconsistent, in terms of both the depth and the quality of information provided, which could have contributed to the fears of life impacts and lack of available treatment options.
Results from the literature review, expert opinion, and interviews supported hypothesized relationships, beginning with the cardinal signs and symptoms of MS that impair function, leading to limitations in work/employment and social life. Similarly, symptoms of MS can impact patients’ independence and cause emotional disturbances. All of these factors may directly impact one’s perceptions of health and health-related quality of life. Key modifiers of progression included the overarching severity of new or worsening symptoms experienced combined with speed of progression and associated age when advanced disease occurs.
Additionally, the availability of support resources, the psychological implications of disease progression, and the availability of care partner support as functional ability declines are all factors that directly influence patients’ perceptions of overall quality of life. Other factors that were described as impacting the patient journey included interactions with HCPs; assistance with navigating therapeutic options and resources for psychological support; and various financial aspects, including navigation of insurance coverage and support for obtaining mobility aids or care partner support and respite care. Patients and families who adjust to and accept the transition to an advanced disease state are bolstered by ongoing interaction and support. These factors can provide them with hope about their ability to manage the symptoms and impacts of MS as well as offer foundational support as these individuals adjust to life and lifestyle impacts that occur as part of disease progression. Variability in patient experiences may be influenced by the patient’s specific clinical site or by the motivation of the patient to actively participate in patient advocacy organizations.
A limitation of this study is that the sampling procedure may limit the generalizability of the results. However, the use of a non-probability sampling approach is in alignment with FDA guidance as an appropriate approach for obtaining patient experience data [3]. Additionally, the variability in patient experience may be influenced by the specific clinical site due to the potential for homogeneity in practice at a given site.
Conclusion
The conceptual model of the transitionary period from RRMS to SPMS expands the current understanding of the progression of MS from the patient and care partner perspective. A better understanding of the patient experience through the transition process by elucidating patient views, concerns, and preferences may be useful to HCPs and other stakeholders as they seek to provide timely and relevant care to patients with SPMS, especially given the advanced treatments becoming available for SPMS. The current model provides further support in describing the relationships of symptoms and impacts through progression of disease. Feedback from patients and care partners in this qualitative study underscores the need for availability of a tool to further augment patient-clinician communication related to disease state and management.
References
Kasser SL, Goldstein A, Wood PK, Sibold J. Symptom variability, affect and physical activity in ambulatory persons with multiple sclerosis: understanding patterns and time-bound relationships. Disabil Health J. 2017;10(2):207–13.
Lublin FD, Reingold SC, Cohen JA, Cutter GR, Sorensen PS, Thompson AJ, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2014;83(3):278–86.
US Food and Drug Administration. Patient-focused drug development: collecting comprehensive and representative input. Guidance for industry, food and drug administration staff, and other stakeholders. 2020. https://www.fda.gov/media/139088/download. Accessed 12 May 2021.
Bamer AM, Cetin K, Amtmann D, Bowen JD, Johnson KL. Comparing a self report questionnaire with physician assessment for determining multiple sclerosis clinical disease course: a validation study. Mult Scler. 2007;13(8):1033–7.
Bogosian A, Morgan M, Bishop FL, Day F, Moss-Morris R. Adjustment modes in the trajectory of progressive multiple sclerosis: a qualitative study and conceptual model. Psychol Health. 2017;32(3):343–60.
Davies F, Edwards A, Brain K, et al. “You are just left to get on with it”: qualitative study of patient and carer experiences of the transition to secondary progressive multiple sclerosis. BMJ Open. 2015;5(7):e007674.
Davies F, Wood F, Brain KE, et al. The transition to secondary progressive multiple sclerosis: an exploratory qualitative study of health professionals’ experiences. Int J MS Care. 2016;18(5):257–64.
Doward LC, McKenna SP, Meads DM, Twiss J, Eckert BJ. The development of patient-reported outcome indices for multiple sclerosis (PRIMUS). Mult Scler. 2009;15(9):1092–102.
Giovannetti AM, Giordano A, Pietrolongo E, et al. Managing the transition (ManTra): a resource for persons with secondary progressive multiple sclerosis and their health professionals: protocol for a mixed-methods study in Italy. BMJ Open. 2017;7(8):e017254.
Montel SR, Bungener C. Coping and quality of life in one hundred and thirty five subjects with multiple sclerosis. Mult Scler. 2007;13(3):393–401.
Newland PK, Thomas FP, Riley M, Flick LH, Fearing A. The use of focus groups to characterize symptoms in persons with multiple sclerosis. J Neurosci Nurs. 2012;44(6):351–7.
O’Loughlin E, Hourihan S, Chataway J, Playford ED, Riazi A. The experience of transitioning from relapsing remitting to secondary progressive multiple sclerosis: views of patients and health professionals. Disabil Rehabil. 2017;39(18):1821–8.
Reade JW, White MB, White CP, Russell CS. What would you say? Expressing the difficulties of living with multiple sclerosis. J Neurosci Nurs. 2012;44(1):54–63.
van der Hiele K, van Gorp DA, Heerings MA, et al. The MS@Work study: a 3-year prospective observational study on factors involved with work participation in patients with relapsing-remitting multiple sclerosis. BMC Neurol. 2015;12(15):134.
Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. JAMA. 1995;273(1):59–65.
Ziemssen T, Tolley C, Bennett B,et al. A mixed methods approach towards understanding key disease characteristics associated with the progression from RRMS to SPMS: physicians’ and patients’ views. Mult Scler Relat Disord. 2020;38:101861.
Baker M, van Beek J, Gossens C. Digital health: Smartphone-based monitoring of multiple sclerosis using Floodlight. https://www.nature.com/articles/d42473-019-00412-0. Accessed 24 June 2021.
Ziemssen T, Piani-Meier D, Bennett B, et al. A physician-completed digital tool for evaluating disease progression (multiple sclerosis progression discussion tool): validation study. J Med Internet Res. 2020;22(2):e16932.
Acknowledgements
We thank the participants of the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: RTI Health Solutions received funding under a research contract with Novartis Pharmaceuticals to conduct this study and provide publication support in the form of manuscript writing, styling, and submission. Novartis Pharmaceuticals funded the journal’s Rapid Service Fee.
Medical Writing Assistance
The authors thank Brian Samsell of RTI Health Solutions for medical writing assistance. Novartis Pharmaceuticals provided funding for publication support in the form of manuscript writing, styling, and submission.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
All authors declare that they have made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; have drafted or written, or substantially revised or critically reviewed the article; have agreed on the journal to which the article will be submitted; have reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage; and agree to take responsibility and be accountable for the contents of the article.
Disclosures
Wendy Su is a Novartis Pharmaceuticals employee. Roshani Shah and Patricia A. Russo were employees of Novartis at the time the work was completed. Lauren Bartolome was a post-doc fellow at Thomas Jefferson University providing services to Novartis at the time of this research. Sibyl E. Wray is a paid consultant for Novartis Pharmaceuticals but did not receive compensation for participation in this study. Sandy Lewis and Carla Romano are employees of RTI Health Solutions, an independent nonprofit research organization that does work for government agencies and pharmaceutical companies. Emily Evans was an employee of RTI Health Solutions at the time the work was completed.
Compliance with Ethics Guidelines
The interview component of this study was approved by the RTI Institutional Review Board (Federal-Wide Assurance #3331). This study was performed in accordance with the Helsinki Declaration of 1964, and its later amendments. Individuals meeting eligibility criteria provided written informed consent for participation. Participants provided written informed consent for publication of study results.
Data Availability
Data are available upon reasonable request to the corresponding author.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Lewis, S., Wray, S.E., Evans, E. et al. Patients’ Experiences in Transitioning to Secondary Progressive Multiple Sclerosis: Qualitative Interviews. Neurol Ther 10, 887–904 (2021). https://doi.org/10.1007/s40120-021-00265-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40120-021-00265-0