
Abstract
Introduction
Coronary sclerosis is a risk factor for the progression to obstructive coronary artery disease (CAD). However, understanding its impact on the outcomes of patients with myocardial infarction and non-obstructive coronary arteries is limited. This study aimed to explore the prognostic influence of coronary sclerosis on in- and out-of-hospital events in troponin-positive patients with non-obstructive coronary arteries.
Methods
This study was a retrospective cohort analysis based on prospectively collected data. A total of 24,775 patients who underwent coronary angiography from 2010 to 2021 in a German university hospital were screened, resulting in a final study cohort of 373 troponin-positive patients with non-obstructive coronary arteries and a follow-up period of 6.2 ± 3.1 years. Coronary sclerosis was defined as coronary plaques without angiographically detectable stenotic lesions of 50% or more in the large epicardial coronary arteries. The primary study endpoint was the occurrence of in-hospital events. Secondary endpoints included events during follow-up.
Results
Patients with coronary sclerosis were significantly older (70 ± 12 vs. 58 ± 16 years, p < 0.001), had ST-segment elevation less frequently on electrocardiogram (9.4% vs. 18.7%, p = 0.013), and suffered more often from diabetes mellitus (23.3% vs. 13.1%, p = 0.009), arterial hypertension (79.6% vs. 59.8%, p < 0.001), chronic obstructive pulmonary disease (17.1% vs. 9.4%, p = 0.028), chronic kidney disease (22.2% vs. 8.4%, p < 0.001), atrial fibrillation (19.8% vs. 12.2%, p = 0.045), and valvular diseases than patients without CAD. Patients with coronary sclerosis were more likely to receive medication for primary/secondary prevention on admission and at discharge. The incidence of in- and out-of-hospital events was significantly higher in patients with coronary sclerosis (in-hospital: 42.8% vs. 29.9%, p = 0.010; out-of-hospital: 46.0% vs. 26.1%, p < 0.001). Mortality rates tended to be higher in the coronary sclerosis group (29.4% vs. 20.0%, p = 0.066).
Conclusion
Patients diagnosed with coronary sclerosis presented a higher incidence of comorbidities and increased medication use, and experienced higher rates of both in-hospital and out-of-hospital events, primarily due to the clustering of cardiovascular risk factors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
It is unclear whether and how the presence of coronary sclerosis as a precursor of obstructive coronary heart disease influences the prognosis of patients with myocardial infarction with non-obstructive coronary arteries (MINOCA). |
The aim of this study was to assess the prognostic impact of coronary sclerosis in troponin-positive patients with non-obstructive coronary arteries, focusing on both in-hospital and out-of-hospital events and long-term outcomes, including mortality. |
What was learned from this study? |
Patients with coronary sclerosis had a higher burden of comorbidities and higher medication use and experienced a higher rate of both in- and out-of-hospital events than patients without coronary artery disease. |
Large randomized, controlled, and prospective studies are urgently needed to better characterize the cohorts with MINOCA and investigate the impact of pre-existing coronary sclerosis in order to identify therapeutic strategies for these patients to reduce the risk of events. |
Introduction
Myocardial infarction with non-obstructive coronary arteries (MINOCA) refers to a clinical condition in which a patient exhibits symptoms of acute coronary syndrome, elevated troponin levels, and non-obstructive coronary arteries, as defined by less than 50% stenosis in any major epicardial vessel during coronary angiography [1, 2]. The prevalence of MINOCA varies widely across studies, ranging from about 1% to 14% of acute coronary syndrome cases undergoing coronary angiography [1, 3]. MINOCA is a broad term covering various underlying conditions, leading to a highly diverse patient population [3]. These conditions involve both coronary and non-coronary issues, encompassing cardiac and extracardiac disorders [1, 3]. After coronary angiography revealing no evidence of coronary artery stenosis, MINOCA is considered a working diagnosis rather than a definitive one [1, 3].
Research suggests that patients with MINOCA, compared to those with myocardial infarction and obstructive coronary artery disease (CAD), are generally younger, more often nonobese and nonsmokers, and lack traditional cardiovascular risk factors like arterial hypertension or chronic kidney disease 4,5,6,7,8,9,10]. Despite a more favorable prognosis for patients with MINOCA, with a 1-year mortality rate of 3.5% versus 6.7% for myocardial infarction patients with CAD, the survival rate of patients with MINOCA remains lower than that of healthy individuals [7, 11]. In previous studies, patients with MINOCA were often compared with patients with myocardial infarction and obstructive CAD. However, it is unclear whether and how the presence of coronary artery sclerosis, i.e. coronary plaques without angiographically detectable stenotic lesions of 50% or more in the large epicardial coronary arteries, as a precursor of obstructive CAD, influences the prognosis of patients with MINOCA.
Therefore, the objective of this study was to assess the prognostic implications of coronary sclerosis in troponin-positive patients with non-obstructive coronary arteries, focusing on both in-hospital and out-of-hospital events, as well as long-term outcomes, including mortality.
Methods
This study analyzed all patients who underwent coronary angiography at University Hospital Bergmannsheil Bochum from January 2010 to April 2021. All participants provided informed consent, and during their hospitalization, extensive data, including medical history, medications, laboratory results, electrocardiograms (ECG), and echocardiography, were systematically documented. This study was performed as a retrospective analysis based on clinical data from a single center. The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Committee of Ruhr University Bochum (protocol code [22-7684] and date of approval [03/01/2023]). All subjects provided informed consent to participate in the study.
Inclusion and Exclusion Criteria, Follow-Up, and Study Endpoints
This study included troponin-positive patients meeting the criteria for non-obstructive coronary arteries after coronary angiography. The working diagnosis in these patients was MINOCA, requiring an increase or decrease in cardiac troponin levels, with at least one value surpassing the 99th percentile. In addition, at least one clinical manifestation of myocardial infarction was required, by symptoms of myocardial ischemia, new ischemic changes on ECG, pathologic Q waves, evidence of new loss of viable myocardium or new regional wall motion abnormalities suggestive of an ischemic cause, and/or evidence of coronary thrombus by angiography or autopsy. Patients undergoing coronary angiography needed to exhibit no coronary artery obstruction (coronary artery stenosis < 50%).
The diagnosis of troponin-positivity with non-obstructive coronary arteries was independently established by two experienced interventional cardiologists and a graduate student through the evaluation of coronary angiograms, echocardiograms, ECG, and laboratory results. The final study cohort was categorized into patients with coronary artery sclerosis and those without CAD for subsequent analysis. Coronary artery sclerosis was diagnosed in the presence of coronary plaques without angiographically detectable stenotic lesions of 50% or more in the large epicardial coronary arteries.
Exclusion criteria encompassed patients with conceivable alternative diagnoses causing troponin elevation, pre-existing obstructive CAD, those younger than 18, and individuals with incomplete data sets.
The primary study endpoint was the occurrence of in-hospital events, a combined endpoint including stroke, cardiopulmonary resuscitation, cardiogenic shock, pulmonary edema, ventilation, left ventricular thrombus, thromboembolic events, life-threatening arrhythmias, and all-cause mortality. The secondary endpoint involved out-of-hospital events during follow-up, a combined endpoint including thromboembolic events, recurrence of troponin-positive non-obstructive coronary arteries, percutaneous coronary intervention, cardiac arrest, and all-cause mortality. Follow-up data were collected between May and September 2023 through hospital presentations, telephone contact with patients, and, in the case of deceased patients, communication with their primary care physicians.
Statistics
The statistical analysis was conducted using SPSS Statistics 23.0 software. Continuous variables with a normal distribution were expressed as mean ± standard deviation, while those with a non-normal distribution were presented as median (interquartile range). Categorical variables were reported as numbers and relative frequencies (%). The normality of continuous variables was assessed using the Kolmogorov–Smirnov test. Comparison between continuous variables with normal and non-normal distributions was performed using either Student's t-test for independent samples or the Mann–Whitney U test. Categorical variables were compared using either the chi-square test or Fisher's exact test. The prognostic impact of coronary artery sclerosis on the outcome was assessed through Kaplan–Meier analyses. Cox regression analysis was conducted to identify independent predictors of in- and out-of-hospital events. A significance level of p < 0.05 was considered statistically significant, and all reported probability values are two-sided.
Results
Baseline Characteristics of the Cohort
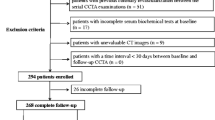
A total of 24,775 patients who underwent coronary angiography from 2010 to 2021 were screened for this study (Fig. 1). The final study population consisted of 373 troponin-positive patients with non-obstructive coronary arteries with a follow-up period of 6.2 ± 3.1 years, including 159 patients with coronary artery sclerosis and 214 without CAD. The cohort comprised 185 men and 188 women. Patients with coronary sclerosis were significantly older than those without CAD (70 ± 12 vs. 58 ± 16 years, p < 0.001). Clinical symptoms and vital parameters were similar between the groups. On ECG, ST-segment elevation was less frequent in patients with coronary sclerosis (9.4% vs. 18.7%, p = 0.013). Compared with patients without CAD, patients with coronary sclerosis had more morbidities. They were significantly more likely to have diabetes mellitus (23.3% vs. 13.1%, p = 0.009), arterial hypertension (79.6% vs. 59.8%, p < 0.001), chronic obstructive pulmonary disease (17.1% vs. 9.4%, p = 0.028), chronic kidney disease (22.2% vs. 8.4%, p < 0.001), and atrial fibrillation (19.8% vs. 12.2%, p = 0.045).

Flow chart presenting the screened data and included patients. CAD coronary artery disease; SD standard deviation
Except for thyroid-stimulating hormone (1.8 ± 1.6 mU/L in coronary sclerosis vs. 2.1 ± 1.7 mU/L in no CAD, p = 0.043), there were no relevant differences in laboratory chemistry between the groups, particularly not in cardiac enzymes.
The left ventricular ejection fraction was 36.2 ± 25.3% in the group with coronary sclerosis and 37.4 ± 26.0% in the group without CAD (p = 0.437). Patients with coronary sclerosis were more likely to exhibit mild aortic (13.6% vs. 4.7%, p = 0.003), mitral (26.3% vs. 16.9%, p = 0.028), and tricuspid valve regurgitation (21.9% vs. 13.6%, p = 0.036) on echocardiography (Table 1).
Medication on Admission and at Discharge
Patients with coronary sclerosis were more likely to receive beta-blockers, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, calcium channel blockers, diuretics, alpha-2 agonists, anticoagulants, and acetylsalicylic acid on admission than those without CAD (Table 1). At the time of discharge, an increased prescription was noted for all medications in both groups. Regarding the use of beta-blockers and angiotensin-converting enzyme inhibitors, the groups equalized and there was no longer a difference. However, patients with coronary artery sclerosis were still significantly more likely to receive angiotensin receptor blockers, diuretics, calcium channel blockers, anticoagulants, acetylsalicylic acid, and clopidogrel (Table 2).
In-Hospital Events
In this study, the primary study endpoint was the occurrence of in-hospital events in patients with coronary artery sclerosis and without CAD. The overall incidence of in-hospital events was significantly higher in patients with coronary sclerosis (42.8% vs. 29.9%, p = 0.010). Notably, patients with coronary sclerosis experienced atrial fibrillation more often than those without CAD (26.4% vs. 16.4%, p = 0.018), especially new-onset atrial fibrillation (15.7% vs. 8.4%, p = 0.029).
Regarding in-hospital death, the overall incidence was 3.1% in patients with coronary sclerosis and 2.3% in those without CAD (p = 0.633) (Table 3).
Multivariable Cox analysis identified arterial hypertension (HR 2.22, 95% CI 1.067–4.600, p = 0.033), heart failure with mild-reduced ejection fraction (HR 3.23, 95% CI 1.345–7.763, p = 0.009), and heart failure with reduced ejection fraction (HR 3.51, 95% CI 1.705–7.236, p < 0.001) as independent predictors of in-hospital events (Table 4).
Out-of-Hospital Events During Follow-Up
This study included 373 troponin-positive patients with non-obstructive coronary arteries, 10 of whom died during hospitalization. Follow-up data were available for 288 patients.
The overall incidence of out-of-hospital events during follow-up was significantly higher in patients with coronary artery sclerosis than in patients without CAD (46.0% vs. 26.1%, p < 0.001) (Fig. 2). While stroke, thromboembolic events, recurrence of troponin positivity with non-obstructive coronary arteries, and cardiac arrest demonstrated no significant differences between the groups, the rate of percutaneous coronary interventions was significantly higher in patients with coronary sclerosis (12.4% vs. 3.6%, p = 0.010). Five patients without coronary artery disease at the time of the MINOCA event underwent percutaneous coronary interventions during follow-up after an average of 1372 days (two patients for non-ST-segment elevation myocardial infarction, three patients for angina pectoris symptoms and development of coronary artery disease). In the coronary sclerosis group, 12 patients underwent percutaneous coronary interventions on average after 1176 days (three patients due to myocardial infarction with non-ST-segment elevation, nine patients due to progression of coronary sclerosis).

Kaplan–Meier curves representing survival free from out-of-hospital events during follow-up. CAD coronary artery disease
Furthermore, overall death rates tended to be higher in the coronary sclerosis group (29.4% vs. 20.0%, p = 0.066) (Table 5) (Fig. 3).

Kaplan–Meier curves representing mortality during follow-up. CAD coronary artery disease
Multivariable analysis for out-of-hospital events identified age (HR 1.07, 95% CI 1.013–1.127, p = 0.015) and diabetes mellitus (HR 7.91, 95% CI 1.841–33.992, p = 0.005) as independent predictors of out-of-hospital events (Table 6).
Discussion
The present study examined the prognostic significance of coronary artery sclerosis with regard to in- and out-of-hospital complications, as well as long-term outcomes, including mortality, in a cohort of 373 troponin-positive patients with non-obstructive coronary arteries. Patients with coronary artery sclerosis demonstrated a higher burden of comorbidities and increased medication use, and experienced higher rates of both in-hospital and out-of-hospital events than those without CAD. Remarkably, our study covered a follow-up period exceeding 6 years, underscoring the reliability of our findings over a substantial timeframe, and allowing for a comprehensive analysis of long-term outcomes.
The observed higher mortality in patients with coronary sclerosis may be attributed to the elevated prevalence of cardiovascular risk factors, each contributing individually to increased mortality. Cardiovascular risk factors play a pivotal role in the development and progression of atherosclerosis, with diabetes mellitus and arterial hypertension standing out as significant contributors [12, 13]. These factors are closely associated with the occurrence of CAD [12, 13] and are associated with a sixfold increase in mortality [14]. Therefore, it was not surprising to find that diabetes mellitus and arterial hypertension were significantly more prevalent among patients with coronary sclerosis than those without CAD in our study. In addition, arterial hypertension was an independent predictor for in-hospital events and diabetes mellitus was an independent predictor for out-of-hospital events. Another cardiovascular risk factor linked to coronary sclerosis in our study was chronic kidney disease. Chronic kidney disease can result from other cardiovascular risk factors, including diabetes mellitus and arterial hypertension, making patients with chronic kidney disease more susceptible to developing CAD [13, 15, 16]. Additionally, chronic kidney disease contributes not only to the development of CAD but also to its progression [15].
Furthermore, in our study, patients with coronary sclerosis also exhibited a significantly higher prevalence of chronic obstructive pulmonary disease, primarily caused by long-term cigarette smoking. Smoking itself is a major risk factor for the development of CAD, making an association with coronary sclerosis in our study highly plausible [13, 17].
Moreover, age is considered a nonmodifiable risk factor for atherosclerosis [18]. Advancing age is associated with physiological changes such as arterial stiffening, endothelial dysfunction, and the gradual accumulation of atherosclerotic plaque within the coronary arteries [13]. Additionally, older age often coincides with the presence of other cardiovascular risk factors, such as hypertension, diabetes mellitus, and dyslipidemia, which further contribute to the susceptibility to CAD [18]. The higher rate of events in the coronary sclerosis group may therefore be attributed to the cumulative effect of these cardiovascular risk factors, combined with age-related changes in the coronary arteries.
A meta-analysis comprising 54 studies with a total of 35,039 patients experiencing angina without obstructive CAD assessed the composite primary outcome of all-cause death and nonfatal myocardial infarction [19]. After a median follow-up of 5 years, the pooled incidence of the primary outcome was 0.98/100 person-years, with significant heterogeneity among studies [19]. The primary outcome was associated with prevalent dyslipidemia, diabetes, and hypertension [19]. Notably, studies enrolling patients with less-than-obstructive CAD exhibited a higher incidence of the primary outcome than those including only patients with “entirely normal” coronary arteries [19]. The presence of coronary atherosclerosis has therefore been identified as a main determinant of major adverse events [19]. Additionally, patients in this category experienced a high incidence of recurrent hospitalization, angina recurrence, and repeated coronary angiography [19].
Besides the higher prevalence of cardiovascular risk factors in patients with MINOCA with coronary sclerosis relative to patients with MINOCA without CAD in our study, those with coronary sclerosis were also significantly more likely to have cardiac comorbidities such as atrial fibrillation and valvular disease. Atrial fibrillation and CAD often coexist in individuals, with each condition potentially influencing the development and progression of the other [20,21,22,23]. In addition, shared risk factors contribute to the strong association between atrial fibrillation and CAD [22]. Conditions such as hypertension, diabetes mellitus, and aging, all of which were associated with coronary sclerosis in our study, increase the likelihood of developing both disorders [22].
The association in our study between valvular regurgitation and coronary artery sclerosis further emphasizes the higher frequency of more complex cardiac diseases in this patient cohort [24].
The results of this study suggest that troponin-positive patients with non-obstructive coronary arteries but with coronary sclerosis present with significantly more cardiovascular risk factors and cardiac comorbidities than those without CAD. Considering the risk factors for the development and progression of coronary sclerosis or CAD, these are almost identical to the findings of our study and thus not surprising. However, studies which differentiate between patients with MINOCA with and without coronary sclerosis and analyze the clinical baseline characteristics of these patients are very limited, and hence the present study was nevertheless able to provide novel findings.
The baseline characteristics of the cohort already indicated that patients with coronary sclerosis had a higher prevalence of comorbidities, particularly cardiovascular conditions, than those without. The findings from the medication analysis further supported this observation. Notably, patients with coronary sclerosis exhibited a greater number of pre-existing cardiovascular disorders, influencing their medication intake at both admission and discharge. In contrast, individuals without CAD received additional medications for the secondary prevention of CAD, contributing to more comparable prescription rates overall at discharge.
According to the current guidelines of the European Society of Cardiology (ESC), the diagnosis of the underlying cause of the working diagnosis of MINOCA enables the initiation of appropriate treatment based on the final diagnosis. Secondary prevention therapies should be considered for those who have been diagnosed with atherosclerotic coronary artery disease and to control risk factors [1].
Previous studies have demonstrated that patients with MINOCA received secondary prophylactic medication less frequently than patients with myocardial infarction and obstructive CAD. However, data on patients with MINOCA with coronary sclerosis compared to patients with MINOCA without CAD are lacking. An observational study included 9466 consecutive patients with MINOCA from the SWEDEHEART registry [25]. After matching treated and untreated groups using a propensity score analysis, the study found that treatment with statins and angiotensin-converting enzyme inhibitors/angiotensin receptor blockers was associated with a lower risk of major adverse cardiac events, while beta-blocker treatment showed a trend toward a positive effect [25]. However, dual antiplatelet therapy exhibited a neutral effect [25]. The results suggest long-term benefits of certain secondary prophylactic medications in patients with MINOCA [25]. However, the study did not differentiate between patients with and without coronary sclerosis. Dal Fabbro et al. conducted a retrospective study with 244 patients with MINOCA focusing on the impact of coronary sclerosis [25]. Significant differences in secondary prevention therapy were observed, with coronary sclerosis patients being more frequently prescribed acetylsalicylic acid, statins, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers than patients without CAD [26]. Similarly, our results revealed that there was a difference at discharge in the prescription of antiplatelet agents and angiotensin receptor blockers, but prescription rates of angiotensin-converting enzyme inhibitors converged from admission to discharge, with no significant difference between the two groups.
The extent to which the differences in secondary prophylactic medication affected the rate of events during follow-up cannot be assessed in this study. Patients with coronary sclerosis received secondary prophylactic medication more frequently and still suffered events more often, but they also had a significantly higher cardiovascular risk profile, which may have been the decisive factor. This observation would be supported by the predictor analysis, as cardiovascular risk factors and comorbidities were identified as independent predictors of a worse outcome, both in-hospital and out-of-hospital.
Limitations
The retrospective design of the current study represents a major limitation. Moreover, the study cohort exhibits heterogeneity. The inclusion of patients with a working diagnosis of MINOCA is a potential confounding factor, given that variations in final diagnoses and treatments within this subgroup could impact the observed outcomes. It is plausible that some patients may have received a definitive diagnosis during or after hospitalization, such as myocarditis or Takotsubo syndrome, factors not considered in this analysis. Both the inclusion of Takotsubo cardiomyopathy patients and the partial lack of echocardiographic parameters due to the retrospective study design could explain why the mean ejection fraction of the study cohort was relatively low.
This study was conducted in a single center, which may have implications for the medications prescribed at discharge. The focus on a single center raises questions about the generalizability of our results to larger populations with MINOCA. In addition, the cohort is relatively small, complicating the detection of statistically significant differences and potentially limiting the power of some comparisons. Another notable limitation is the absence of a control group with obstructive CAD. The diagnosis of “coronary sclerosis” was made by experienced interventional cardiologists, but only visually, i.e., no quantitative coronary angiography, intravascular ultrasound, or optical coherence tomography was used as standard in each patient. Furthermore, exercise stress testing was not performed as standard in all patients, which could have provided a possible additional indication of coronary microvascular dysfunction as the cause of myocardial ischemia [27, 28].
Conclusion
The current study, with an extensive follow-up period exceeding 6 years, examined the prognostic implications of coronary artery sclerosis for complications both within and outside the hospital, as well as for long-term outcomes, including mortality, in a cohort of 373 troponin-positive patients with non-obstructive coronary arteries. Patients with coronary artery sclerosis, compared to those without CAD, presented a higher prevalence of cardiovascular risk factors and comorbidities and increased medication prescription rates, both at admission and as part of secondary prevention following the MINOCA event. Moreover, they experienced a higher frequency of events both within and outside the hospital, primarily due to the clustering of cardiovascular risk factors. Large randomized controlled and prospective trials are urgently needed to better characterize cohorts with MINOCA and investigate the impact of pre-existing coronary artery sclerosis, in order to identify therapeutic strategies for these patients to reduce the risk of adverse events.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Byrne RA, et al. ESC guidelines for the management of acute coronary syndromes. Eur Heart J. 2023. https://doi.org/10.1093/eurheartj/ehad191.
Thygesen K, et al. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138:e618–51. https://doi.org/10.1161/cir.0000000000000617.
Collet J-P, et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2020;42:1289–367. https://doi.org/10.1093/eurheartj/ehaa575.
Ishii M, et al. Characteristics and in-hospital mortality of patients with myocardial infarction in the absence of obstructive coronary artery disease in super-aging society. Int J Cardiol. 2020;301:108–13. https://doi.org/10.1016/j.ijcard.2019.09.037.
Kallmeyer A, et al. Absence of high lipoprotein(a) Levels is an independent predictor of acute myocardial infarction without coronary lesions. J Clin Med. 2023;12:960. https://doi.org/10.3390/jcm12030960.
Lopez-Pais J, et al. Clinical characteristics and prognosis of myocardial infarction with non-obstructive coronary arteries: a prospective single-center study. Cardiol J. 2022;29:798–806. https://doi.org/10.5603/CJ.a2020.0146.
Barr PR, et al. Myocardial infarction without obstructive coronary artery disease is not a benign condition (ANZACS-QI 10). Heart, Lung & Circ. 2018;27:165–74. https://doi.org/10.1016/j.hlc.2017.02.023.
Pizzi C, et al. Nonobstructive versus obstructive coronary artery disease in acute coronary syndrome: a meta-analysis. J Am Heart Assoc. 2016. https://doi.org/10.1161/JAHA.116.004185.
Rakowski T, et al. Characteristics of patients presenting with myocardial infarction with non-obstructive coronary arteries (MINOCA) in Poland: data from the ORPKI national registry. J Thromb Thrombolysis. 2019;47:462–6. https://doi.org/10.1007/s11239-018-1794-z.
Safdar B, et al. Presentation, clinical profile, and prognosis of young patients with myocardial infarction with nonobstructive coronary arteries (MINOCA): results from the VIRGO study. J Am Heart Assoc Cerebrovasc Dis. 2018. https://doi.org/10.1161/JAHA.118.009174.
Kong M, Liu F, Zhu Z. Analysis between high risk of myocardial infarction with non-obstructive coronary artery disease in single center and occurrence of major adverse cardiovascular events. Ann Noninvasive Electrocardiol. 2022;27:e13007.
Arnold SV, et al. Clinical management of stable coronary artery disease in patients with type 2 diabetes mellitus: a scientific statement from the American Heart Association. Circulation. 2020;141:e779–806. https://doi.org/10.1161/CIR.0000000000000766.
Raitakari O, Pahkala K, Magnussen CG. Prevention of atherosclerosis from childhood. Nat Rev Cardiol. 2022;19:543–54. https://doi.org/10.1038/s41569-021-00647-9.
Charoensri S, Kritmetapak K, Tangpattanasiri T, Pongchaiyakul C. The impact of new-onset diabetes mellitus and hypertension on all-cause mortality in an apparently healthy population a ten-year follow-up study. J Diabet Res. 2021;2021:3964013. https://doi.org/10.1155/2021/3964013.
Batra G, et al. Interleukin 6 and cardiovascular outcomes in patients with chronic kidney disease and chronic coronary syndrome. JAMA Cardiol. 2021;6:1440–5. https://doi.org/10.1001/jamacardio.2021.3079.
Ruilope LM, et al. Blood pressure and cardiorenal outcomes with finerenone in chronic kidney disease in type 2 diabetes. Hypertension. 2022;79:2685–95. https://doi.org/10.1161/HYPERTENSIONAHA.122.19744.
Li Y, et al. The impact of chronic obstructive pulmonary disease on the prognosis outcomes of patients with percutaneous coronary intervention or coronary artery bypass grafting: a meta-analysis. Heart lung: J Crit Care. 2023;60:8–14. https://doi.org/10.1016/j.hrtlng.2023.02.017.
Lowenstern A, et al. Age-related differences in the noninvasive evaluation for possible coronary artery disease: insights from the prospective multicenter imaging study for evaluation of chest pain (PROMISE) trial. JAMA Cardiol. 2020;5:193–201. https://doi.org/10.1001/jamacardio.2019.4973.
Radico F, et al. Determinants of long-term clinical outcomes in patients with angina but without obstructive coronary artery disease: a systematic review and meta-analysis. Eur Heart J. 2018;39:2135–46. https://doi.org/10.1093/eurheartj/ehy185.
Kristensen KE, et al. Subclinical atherosclerosis is associated with incident atrial fibrillation: a systematic review and meta-analysis. Eur : Eur Pacing, Arrhythm, Cardiac Electrophysiol. 2020;22:991–1000. https://doi.org/10.1093/europace/euaa030.
Taha A, et al. New-onset atrial fibrillation after coronary artery bypass grafting and long-term outcome: a population-based nationwide study from the SWEDEHEART registry. J Am Heart Assoc. 2021;10:e017966.
Joglar JA, et al. ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024;149:e1–156. https://doi.org/10.1161/CIR.0000000000001193.
Frederiksen TC, et al. The bidirectional association between atrial fibrillation and myocardial infarction. Nat rev Cardiol. 2023;20:631–44. https://doi.org/10.1038/s41569-023-00857-3.
Emren ZY, et al. Evaluation of the prevalence of coronary artery disease in patients with valvular heart disease. J Cardiothorac Surg. 2014;9:153. https://doi.org/10.1186/s13019-014-0153-1.
Lindahl B, et al. Medical therapy for secondary prevention and long-term outcome in patients with myocardial infarction with nonobstructive coronary artery disease. Circulation. 2017;135:1481–9. https://doi.org/10.1161/circulationaha.116.026336.
Dal Fabbro J, et al. Clinical and electrocardiographic features of patients with myocardial infarction with non-obstructive coronary artery disease (MINOCA). J Cardiovasc Med. 2021;22:104–9. https://doi.org/10.2459/JCM.0000000000001027.
Sinha A, et al. Rethinking false positive exercise electrocardiographic stress tests by assessing coronary microvascular function. J Am Coll Cardiol. 2024;83:291–9. https://doi.org/10.1016/j.jacc.2023.10.034.
Bogossian H, Alhanafi D, Kloppe A, Höltgen R, Mijic D. Stress testing: a relevant examination in rhythmology. Herzschr Elektrophysiol. 2023;34:333–8. https://doi.org/10.1007/s00399-023-00967-y.
Acknowledgements
We thank the participants of the study.
Funding
No funding or sponsorship was received for this study. The Rapid Service Fee was funded by the authors.
Author information
Authors and Affiliations
Contributions
Fabienne Kreimer: Formal analysis, Writing original draft. Clara Schlettert: Conceptualization, Data curation, Formal analysis, Investigation. Mohammad Abumayyaleh: Validation, Writing: review & editing. Ibrahim Akin: Validation, Writing: review & editing. Daniel Materzok: Data curation, Investigation. Michael Gotzmann: Validation, Writing: review & editing. Fabian Schiedat: Validation, Writing: review & editing. Harilaos Bogossian: Validation, Writing: review & editing. Mido Max Hijazi: Validation, Writing: review & editing. Nazha Hamdani: Supervision, Writing: review & editing. Andreas Mügge: Formal analysis, Investiagation, Supervision, Writing: review & editing. Ibrahim El-Battrawy: Conceptualization, Data curation, Formal analysis, Writing original draft. Rayyan Hemetsberger: Formal analysis, Supervision, Writing: review & editing. Assem Aweimer: Conceptualization, Data curation, Formal analysis, Writing original draft.
Corresponding author
Ethics declarations
Conflict of Interest
Fabienne Kreimer, Clara Schlettert, Mohammad Abumayyaleh, Ibrahim Akin, Daniel Materzok, Michael Gotzmann, Fabian Schiedat, Harilaos Bogossian, Mido Max Hijazi, Nazha Hamdani, Andreas Mügge, Ibrahim El-Battrawy, Rayyan Hemetsberger and Assem Aweimer have nothing to disclose.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Committee of Ruhr University Bochum (protocol code [22-7684] and date of approval [03/01/2023]). All subjects provided informed consent to participate in the study.
Additional information
Prior publications: The following study is an analysis of a MINOCA database. This has already resulted in two publications:
1. Kreimer F, Schlettert C, Abumayyaleh M, Akin I, Hijazi MM, Hamdani N, Gotzmann M, Mügge A, El-Battrawy I, Aweimer A. The impact of diabetes mellitus on the outcome of troponin-positive patients with non-obstructive coronary arteries. Int J Cardiol Heart Vasc. 2024 Feb 2; 50:101350. doi: 10.1016/j.ijcha.2024.101350. PMID: 38328690; PMCID: PMC10847989.
2. Kacmaz, M.; Schlettert, C.; Kreimer, F.; Abumayyaleh, M.; Akin, I.; Mügge, A.; Aweimer, A.; Hamdani, N.; El-Battrawy, I. Ejection Fraction-Related Differences of Baseline Characteristics and Outcomes in Troponin-Positive Patients without Obstructive Coronary Artery Disease. J. Clin. Med. 2024, 13, 2826. https://doi.org/10.3390/jcm13102826.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Kreimer, F., Schlettert, C., Abumayyaleh, M. et al. Prognostic Implications of Coronary Artery Sclerosis in Troponin-Positive Patients with Non-Obstructive Coronary Arteries. Cardiol Ther (2024). https://doi.org/10.1007/s40119-024-00375-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40119-024-00375-4