
Abstract
Introduction
Though less common in the current era, surgical closure of secundum atrial septal defects (ASD2) is still performed in certain clinical situations. Guidelines currently recommend lifelong follow-up with transthoracic echocardiograms (TTE) for patients who have undergone a surgical ASD2 closure. The goal of this study was to determine the utility of follow-up TTE in patients who underwent an uncomplicated ASD2 closure.
Methods
Chart review was performed on patients who had a surgical ASD2 closure between April 1, 1996, and August 30, 2021. Patients were excluded if they had other congenital heart disease, had a diagnosis of a residual ASD2, atrial/ventricular arrhythmias, pulmonary hypertension, heart failure, or did not have a follow-up TTE > 6 months after the procedure. The most recent TTEs and clinic notes were evaluated.
Results
A total of 30 patients met the criteria. The median age at ASD2 surgery was 4.0 years (IQ; 1.9–10.5). ASD2 was closed via patch repair in 16 patients and primarily closed in 14 patients. The most recent TTE was performed a median of 9.5 years (IQ; 4.0, 14.7) after ASD2 closure. Two patients had mild right atrial and ventricular dilation, one patient had mild right atrial dilation, and one patient had mild right ventricular dilation. All other patients had qualitatively normal right-sided chamber sizes. All patients had normal biventricular function (left ventricular fractional shortening (median 36% (IQ; 33, 42)), no evidence of residual atrial shunts, and no evidence of pulmonary hypertension. No patient was on any cardiac medications at last clinic visit. Four patients were discharged from cardiology clinic and 10 patients were lost to follow-up. There were no deaths. Twenty-four patients had 46 repeat echocardiograms > 1 year after ASD2 with no change in clinical management.
Conclusion
In patients who underwent an uncomplicated ASD2 closure, there were no significant abnormalities noted on follow-up TTEs. The need for repeat lifetime TTEs and their frequency, in this uncomplicated population, should be reassessed if larger studies with longer follow-up confirm these initial findings.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
Why carry out the study? |
North American guidelines recommend lifelong intermittent echocardiograms in patients who have undergone surgical closure of a secundum atrial septal defect (ASD2). |
In this study, no significant complications with follow-up echocardiograms were noted in patients who had an uncomplicated ASD2 surgical closure. |
What was learned from the study? |
Larger studies with longer follow-up are needed, but if results are corroborated, the need for routine lifelong echocardiograms in this population may need to be re-evaluated to determine the cost-effectiveness of this recommendation. |
Introduction
Atrial septal defects are the second most common form of congenital heart defects, with a prevalence of 1.6 in 1000 live births worldwide [1], or about 1 in every 625 live births. Secundum atrial septal defects (ASD2) are the most common type of atrial defect. Though catheter closure of ASD2 has become prevalent [2, 3], there is still a subset of patients that undergo surgical closure because of patient or family choice or if catheter closure is contraindicated or unsuccessful. Although some complications have been described, the morbidity and mortality of surgical ASD2 closure is low with most complications occurring early after surgical repair [4, 5].
Current North American guidelines rate as appropriate, scoring 9/9, lifelong intermittent (every 2–5 years) transthoracic echocardiograms (TTE) in patients who have undergone surgical ASD2 repair, even those with mild or no sequelae [6, 7]. TTEs and outpatient clinic follow-up come at a significant cost to both families and the healthcare system. However, there are minimal data to suggest that lifelong follow-up changes outcomes in these patients [8, 9].
The objective of this study was to perform a preliminary analysis to determine the utility of follow-up TTEs in patients who underwent an uncomplicated surgical closure of an ASD2.
Methods
This single-site retrospective chart review study was approved by the Institutional Review Board of Nationwide Children’s Hospital. Patients were identified using the Heart Center database. Chart review was performed on all patients who had a surgical ASD2 closure between April 1, 1996 and August 30, 2021. This study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments.
All patients who had a surgical ASD2 closure were included in the initial review. Patients were excluded if they had other congenital heart disease or residual defects on their first TTE 6 months after surgery. Patients were also excluded if they had a diagnosis of a residual ASD2, atrial/ventricular arrhythmias, pulmonary hypertension, or heart failure 6 months post-repair. In addition, patients were excluded if they did not have TTE data available 6 months post-repair or if they were lost to follow-up < 1 year after surgery.
Demographic data as well as data on type of repair and most recent clinic notes were documented. Data on each patient’s preoperative TTE and TTE at discharge, at 6-month follow-up, and at the most recent visit were also collected. Description of chamber dilation was qualitative in nature whereas left ventricular function was quantitative in nature.
Values are presented as medians and interquartile ranges unless otherwise specified. Paired t-tests were used to compare pre- and postoperative data. P < 0.05 was considered significant.
Results
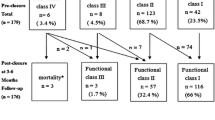
Fifty-one patients were reviewed. Twenty-one patients were excluded (lost to follow-up ≤ 1 year after surgery, n = 14; residual issues at 6 month follow-up, n = 4 (residual ASD2, n = 3; chronic pericardial effusion, n = 1); other cardiac diagnosis, n = 3 (sinus venosus defect, n = 1; moderate mitral regurgitation, n = 1; arrhythmogenic right ventricular dysplasia, n = 1)). This study therefore consisted of 30 patients who underwent a surgical ASD2 repair who had no clinical or significant TTE abnormalities > 6 months post-surgery.
Seven patients had an associated genetic diagnosis (Down syndrome, n = 2; Emanuel syndrome, n = 1; partial deletion of chromosome 15, n = 1; Holt-Oram syndrome, n = 1; prothrombin gene mutation, n = 1; 16p11 deletion, n = 1). Age at time of ASD2 repair was 4.0 years (IQ; 1.9, 10.5). ASD2 was closed via patch repair in 16 patients and primarily closed in 14 patients. Complications after ASD2 surgery included pneumomediastinum, n = 2; pericardial effusion, n = 2, right pleural effusion, n = 1, and 3rd degree atrioventricular block, n = 1. All complications resolved prior to hospital discharge.
Discharge TTE was performed 2.0 days (IQ; 2, 3) after ASD2 repair. One patient had echocardiographic evidence of elevated right ventricular pressures, two patients had a residual ASD2 shunt, 13 patients had mild right atrial dilation, five patients had moderate right atrial dilation, 10 patients had mild right ventricular dilation, and six patients had moderate right ventricular dilation. First follow-up TTE > 6 months post-ASD2 repair was performed at 1.3 years (IQ; 1.1, 5.1) after surgery. On the first follow-up TTE > 6 months, no patient had indirect echocardiographic evidence of elevated right ventricular pressures or residual ASD2 shunts. One patient had mild right atrial dilation. No other echocardiographic abnormalities were noted on this follow-up TTE. The most recent TTE was performed at 9.5 years (IQ; 4.0, 14.7) post-ASD2 repair. The longest follow-up period was 19.2 years. Two patients had mild right atrial and ventricular dilation, one patient had mild right atrial dilation, and one patient had mild right ventricular dilation. All other parameters on the most recent TTE documented no residual ASD2 shunts or indirect echocardiographic evidence of elevated right ventricular pressures, qualitatively normal right-sided chamber sizes, and normal biventricular systolic function (left ventricular fractional shortening, 36.0% (IQ; 33, 42)). No other echocardiographic abnormalities were documented on the most recent TTE. Preoperative data and most recent postoperative data are presented in Table 1.
No patient underwent a surgical or catheter intervention due to any complications after ASD2 repair. All patients were noted to be clinically doing well at their last clinic visit with no cardiac medications being administered. There was no evidence of any atrial or ventricular arrhythmias, pulmonary hypertension, or heart failure issues per the last clinic notes. Per the last clinic note available, no patient had a precordial heave, hepatosplenomegaly, peripheral edema, or jugular vein distention. Five patients were noted to have a non-specific systolic ejection murmur graded either as a I or II in intensity. There were no mortalities. Four patients were discharged from cardiology clinic, 10 patients were lost to follow-up, and 16 patients are still being followed in cardiology clinic out of the 30 patients evaluated.
Twenty-four patients had a total of 46 TTEs > 6 months after ASD2 repair. No clinical changes were made based on the follow-up TTE based on clinical notes.
Discussion
Though ASD2 closure via device placement has become the first choice of most ASD2 repairs, surgical ASD2 repair is still performed in some circumstances [3]. Despite low morbidity and low mortality in surgical closure of ASD2 [3, 4], current North American guidelines recommend lifelong intermittent (every 2 to 5 years) TTE even in patients with mild or no sequelae [6, 7]. In this preliminary analysis evaluating the utility of follow-up TTE in an uncomplicated cohort of patients who had undergone ASD2 surgical repair, no significant abnormalities were noted on follow-up TTE. No clinical changes were made based on follow-up TTE > 6 months after surgical repair.
Surgical ASD2 closure is relatively safe, with estimated mortality < 0.3% [10]. Major complications after surgical ASD2 repair are also relatively low, though minor complications have been reported to range from 20% to 80% [11, 12]. Many of the cardiac complications noted after ASD2 such as residual shunts, pericardial effusions, and arrhythmias are noted in hospital or during the early follow-up period [11, 12]. Because of these issues and in the absence of high-quality evidence, routine surveillance within a year following surgical ASD2 closure in an asymptomatic patient with no or mild sequelae is recommended, scoring 9/9 in consensus national guidelines in North America [6, 7].
The long-term outcomes after surgical ASD2 repair are usually good, with a low incidence of complications [4, 5, 8, 9, 13, 14]. The main long-term cardiac concerns related to surgical ASD2 repair may include issues such as arrhythmias, heart failure, and pulmonary hypertension. However, those patients who develop late complications after surgical ASD2 closure can usually be identified as being high risk either preoperatively or in the first 6–12 months postoperatively. Older age at repair, male sex, presence of peri-operative arrhythmias, peri-operative heart failure, and higher peri-operative mean pulmonary artery pressures have been documented to be risk factors for late complications in this cohort of patients [5, 8, 14,15,16].
The results of this study are essentially consistent with the previous publications. In a cohort of patients with ASD2 and minimal to no risk factors, surgical repair had excellent short-, medium-, and long-term outcomes. No patient had any evidence of documented arrhythmias, pulmonary hypertension, or heart failure. A small percentage of patients did have qualitatively mild right-sided dilation, but in the absence of objective measurements, no conclusion can be drawn. One study showed that despite right-sided dilation, the exercise capacity and incidence of arrhythmias was not different from those of patients who did not have right-sided dilation after surgical ASD2 repair [4]. Furthermore, since the ASD2 was repaired, one may assume that further right-sided dilation would no longer occur or would even potentially regress.
These data, in conjunction with previous publications, call into question the utility of lifelong TTE in patients post-ASD2 repair with no complications. The data are also consistent with the European guidelines for follow-up of patients undergoing surgical ASD2 repair [17]. The European guidelines state “Patients repaired at age < 25 years without relevant sequelae or residua (no residual shunt, normal pulmonary artery pressures, normal right ventricle, no arrhythmias) do not require regular follow-up, though families should be made aware of the occurrence of late arrhythmias”. Along with the previously cited publications, these data support the European guidelines for follow-up indications in patients with ASD2 versus the lifelong TTE recommendations from the North American guidelines. It may be reasonable to follow these patients for a set period of time with TTE, but after this period, then clinical follow-up may be all that is needed unless other concerns arise. This study used a 6-month TTE as a starting point marker for inclusion in the study to increase the study population evaluated, but the time interval proposed could be 1 or even 5 years after repair before stopping routine TTE follow-up. Assuming that an ASD2 is repaired at 5 years of life and assuming an average life span of 80 years, obtaining a TTE every 2–5 years could mean up to approximately 15–35 extra TTE over the patient’s life. Regardless of the time period chosen, it is unlikely that lifelong is the most cost-efficient time period to choose for follow-up TTE. In addition to the lack of cost efficiency, there may be other unintended consequences of lifelong TTE evaluations such as scheduling and transportation burden for the patient, persistent patient apprehension, and the risk of identifying incidental but clinically irrelevant findings, prompting further unneeded investigations. In this study, the follow-up TTE > 6 months after repair did not change medical management.
This study has multiple limitations. It is a single-center retrospective study with all the inherent limitations of such a design. The sample size was small despite the study collecting data over a 25-year period. The patient population was relatively homogeneous, with a strong pediatric age predilection. This may limit the generalizability of these results to patients who had their ASD2 repaired as adults. Cardiac chamber dilation and right ventricular function was graded qualitatively versus quantitatively. The longest follow-up time evaluated in this uncomplicated cohort was 19 years, so no specific comment can be made beyond that time frame. A third of patients were lost to follow-up; however, if there were any subsequent complications noted, the patients who were lost to follow-up would likely have been referred back to our surgical center.
Conclusion
In conclusion, in patients who underwent an uncomplicated ASD2 closure, there were no significant abnormalities noted on follow-up TTEs. The need for repeat lifetime TTEs and their frequency in this uncomplicated population should be reassessed if larger studies with longer follow-up confirm these initial findings.
References
van der Linde D, Konings EE, Slager MA, et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol. 2011;58:2241–7.
Matitiau A, Birk E, Kachko L, Blieden LC, Bruckheimer E. Transcatheter closure of secundum atrial septal defects with the amplatzer septal occluder: early experience. Isr Med Assoc J. 2001;3:32–5.
DiBardino DJ, McElhinney DB, Kaza AK, Mayer JE Jr. Analysis of the US Food and Drug Administration manufacturer and user facility device experience database for adverse events involving Amplatzer septal occluder devices and comparison with the Society of Thoracic Surgery congenital cardiac surgery database. J Thorac Cardiovasc Surg. 2009;137:1334–41.
Meijboom F, Hess J, Szatmari A, et al. Long-term follow-up (9 to 20 years) after surgical closure of atrial septal defect at a young age. Am J Cardiol. 1993;72:1431–4.
Cuypers JA, Opic P, Menting ME, et al. The unnatural history of an atrial septal defect: longitudinal 35 year follow up after surgical closure at young age. Heart. 2013;99:1346–52.
Writing G, Sachdeva R, Valente AM, et al. ACC/AHA/ASE/HRS/ISACHD/SCAI/SCCT/SCMR/SOPE 2020 appropriate use criteria for multimodality imaging during the follow-up care of patients with congenital heart disease: a report of the American College of Cardiology solution set oversight committee and appropriate use criteria task force, American Heart Association, American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Pediatric Echocardiography. J Am Soc Echocardiogr Off Publ Am Soc Echocardiogr. 2020;33:e1–48.
Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;73:e81–192.
Kutty S, Hazeem AA, Brown K, et al. Long-term (5- to 20-year) outcomes after transcatheter or surgical treatment of hemodynamically significant isolated secundum atrial septal defect. Am J Cardiol. 2012;109:1348–52.
Bolz D, Lacina T, Buser P, Buser M, Guenthard J. Long-term outcome after surgical closure of atrial septal defect in childhood with extensive assessment including MRI measurement of the ventricles. Pediatr Cardiol. 2005;26:614–21.
O’Brien SM, Clarke DR, Jacobs JP, et al. An empirically based tool for analyzing mortality associated with congenital heart surgery. J Thorac Cardiovasc Surg. 2009;138:1139–53.
Galal MO, Wobst A, Halees Z, et al. Peri-operative complications following surgical closure of atrial septal defect type II in 232 patients–a baseline study. Eur Heart J. 1994;15:1381–4.
de Beco G, Mambour N, Vo C, et al. Recent experience and follow-up after surgical closure of secundum atrial septal defect in 120 children. Pediatr Cardiol. 2018;39:1440–4.
Houck CA, Evertz R, Teuwen CP, et al. Time course and interrelationship of dysrhythmias in patients with surgically repaired atrial septal defect. Heart Rhythm Off J Heart Rhythm Soc. 2018;15:341–7.
Gatzoulis MA, Freeman MA, Siu SC, Webb GD, Harris L. Atrial arrhythmia after surgical closure of atrial septal defects in adults. N Engl J Med. 1999;340:839–46.
Van De Bruaene A, Moons P, Belmans A, et al. Predictive model for late atrial arrhythmia after closure of an atrial septal defect. Int J Cardiol. 2013;164:318–22.
D’Alto M, Romeo E, Argiento P, et al. Hemodynamics of patients developing pulmonary arterial hypertension after shunt closure. Int J Cardiol. 2013;168:3797–801.
Baumgartner H, De Backer J, Babu-Narayan SV, et al. 2020 ESC guidelines for the management of adult congenital heart disease. Eur Heart J. 2021;42:563–645.
Acknowledgements
We thank the participants of the study
Funding
No funding or sponsorship was received for this study or publication of this article.
Author contributions
Concept/design—Ritika Gupta, Clifford Cua. Data analysis/collection—Ritika Gupta, Mayling Mah, Clifford Cua. Drafting—Ritika Gupta, Clifford Cua. Review/approval—Ritika Gupta, Mayling Mah, Jessica Bowman, Clifford Cua.
Prior Presentation
American Academy of Pediatrics Meeting October 2022.
Disclosures
Ritika Gupta, Mayling Mah, Jessica Bowman, and Clifford Cua all have nothing to disclose.
Compliance with Ethics Guidelines
This study was approved by the Investigational Review Board at Nationwide Children’s Hospital (study 00000149). This study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments.
Data Availability
All data generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Gupta, R., Mah, M.L., Bowman, J. et al. Utility of Follow-Up Echocardiograms in Uncomplicated Surgical Secundum Atrial Septal Defect Closures: Preliminary Analysis. Cardiol Ther 12, 525–531 (2023). https://doi.org/10.1007/s40119-023-00327-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40119-023-00327-4