
Abstract
Purpose
Visceral leishmaniasis (VL) has become a rising concern to transplantation teams, being associated with graft dysfunction and reduced survival of renal transplant recipients. Here, we describe a case of VL occurring in a kidney transplant (KT) recipient in Italy, a country in which Leishmania infantum is endemic and we reviewed the literature on the clinical course and diagnosis of VL in KT recipients residing or travelling to southern Europe.
Results
The VL case was diagnosed 18 months after transplant and 28 days after the onset of symptoms by quantitative PCR (qPCR) on peripheral blood. A graft biopsy showed renal involvement, and PCR performed on graft tissue displayed the presence of Leishmania DNA. The retrospective confirmation of Leishmania-positive serology in a serum sample collected before transplantation, as well as the absence of anti-Leishmania IgG in the graft donor strongly suggest that reactivation of a latent parasitic infection caused VL in the current case.
Conclusion
VL is often underdiagnosed in transplant recipients, despite the presence of latent Leishmania infection being reported in endemic countries. This case report, as well as the literature review on leishmaniasis in KT recipients, underline the importance of rapid VL diagnosis to promptly undergo treatment. Serology is scarcely sensitive in immunocompromised patients, thus molecular tests in peripheral blood should be implemented and standardized for both VL identification and follow-up.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Visceral leishmaniasis (VL) is an infectious disease caused by protozoa of the Leishmania donovani complex, and associated with considerable morbidity and mortality [1]. VL is also a known complication of solid organ transplantation (SOT) [2]; the prevalence of VL among SOT recipients in endemic areas is up to 0.9% [3, 4]. In these patients, VL can occur either ex novo or through reactivation of a pre-existing infection induced by the immunosuppressive drugs. In kidney transplant (KT) recipients, leishmaniasis often includes acute interstitial nephritis with moderate inflammation and infiltration of lymphocytes, plasma cells and macrophages, and can lead to graft dysfunction [5]. VL occurring in SOT is a severe event, being associated with frequent relapses and a mortality rate that exceeds 20% [6].
Here, we report a VL case in a KT recipient residing in central Italy, where L. infantum circulates. We diagnosed and monitored VL by quantitative PCR (qPCR) and retrospectively screened pre-transplant samples of the index patient and the graft donor by serology. We also briefly reviewed the literature on the clinical course and diagnosis of VL in KT recipients residing or travelling to southern Europe.
Case presentation
A 36-year-old Caucasian male underwent pre-emptive kidney transplantation at the Nephrology, Dialysis and Renal Transplant Unit, University Hospital of Bologna, Italy, for end-stage renal disease (ESRD) secondary to autosomal dominant polycystic kidney disease (ADPKD). The graft was available from a living donor (a first-degree relative). Induction therapy with high dose steroids and anti-IL2r monoclonal antibodies (basiliximab) was first administered after transplant, followed by maintenance therapy with prednisone, tacrolimus and mycophenolic acid. No major complications were reported, and graft function was stabilized with serum creatinine (sCreat) levels at 2 mg/dl (eGFR CKD-EPI 42 ml/min).
Approximately 18 months after transplant, the patient was admitted following a routine follow-up appointment during which he complained of night sweat and persistent mild fever in the previous 3 weeks. Symptoms had been empirically treated with oral antibiotics by the patient’s general practitioner, with no benefit. Laboratory examination showed pancytopenia (WBC 2370/mmc, Hb 10.5 g/dl, PLT 76.000/mmc), renal impairment (sCreat 3.7 mg/dl, eGFR CKD-EPI 19 ml/min), elevated C-reactive protein (CRP 12 mg/dl), and elevated ferritin (902 ng/ml). 18F-FDG PET/C was performed, showing splenomegaly and splenic hypercaptation. Since a discrepancy between the donor’s and the recipient’s serostatuses for human cytomegalovirus (CMV) was known (D + /R −), a primary CMV infection was initially suspected, and mycophenolic acid was suspended at admission. As CMV DNAemia tested negative, the suspicion of CMV disease was dismissed.
Two real-time (rt)PCR assays targeting the small-subunit ribosomal (r)RNA gene and the leishmanial kinetoplast (k)DNA, respectively, were simultaneously performed on peripheral whole blood as described by Varani et al. [7]. Quantification of parasitic kinetoplast (k)DNA was also performed. At diagnosis, the parasite load was 9360 parasite equivalents/ml (Fig. 1a–c). VL serology was carried out by rK39-based immunochromatographic test (ICT; Rapydtest, Diagnostic International Distribution S.p.A, Milan, Italy), by enzyme-linked immunosorbent assay (ELISA, Vircell, Granada, Spain) and by immunofluorescence assay (IFA, BioMérieux, Marcy-l’Étoile, France). The sample tested positive on ELISA and negative on the ICT, while the IFA returned a title of 1:80, corresponding to an indeterminate result.

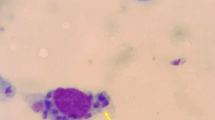
Molecular diagnosis and monitoring and histological evaluation of visceral leishmaniasis in a kidney transplant recipient. a–c Time course of parasitological and laboratory parameters in the index patient. Parasitaemia was measured by quantitative real-time PCR (qPCR) before and after anti-leishmanial treatment (L-Amb). Detection of kDNA by qPCR was set up as described in Mary et al. [8]. The standard curve was created from Leishmania DNA extracted from 5 × 106 promastigotes of the L. infantum reference strain MHOM/TN/80/IPT1, performing serial dilution to 0.0005 parasites. Detection of kDNA reached the sensitivity of 0.05 parasite equivalents/ml. d. Histology examination of the kidney biopsy shows interstitial fibrosis and tubular atrophy (Trichrome stain, 10×). sCreat; serum creatinine levels. WBC; white blood cells. PLT platelets. Eq.par. equivalent parasites
As the renal function worsened, a graft biopsy was performed. Histological examination of the biopsy showed diffuse interstitial fibrosis/tubular atrophy with moderate chronic interstitial inflammation and glomerulosclerosis in almost 50% of glomeruli associated to chronic vascular damage (Fig. 1d). CD1a staining was negative and parasite amastigotes were not detected at histology nor at electron microscopy, while parasitic kDNA was identified by rtPCR in renal tissue (data not shown). Bone marrow biopsy was also carried out, showing myelodysplasia, which was consistent with VL. Unfortunately, this sample was not sent to the Microbiology Unit and kDNA rtPCR was not performed.
Anti-leishmanial therapy with liposomal amphotericin B (L-Amb) was carried out (eight infusions; 5 mg/kg/dose) with good response. During treatment, both thrombocytopenia and leukopenia rapidly improved, and a decrease of sCreat levels was also observed after a brief initial increase, likely due to L-AmB-related nephrotoxicity. rtPCR for Leishmania tested negative on peripheral blood within 3 months after the first L-AmB infusion (Fig. 1a–c). Graft function partially recovered, with sCreat stabilizing at 2.1–2.5 mg/dl at 15 months after VL diagnosis and further decreasing to 1.8–2.0 mg/dl at 42 months; at this time the patient was also free from VL relapses, with no Leishmania DNA detected in peripheral blood samples. Administration of mycophenolic acid was not reinstated after treatment.
The serostatus for Leishmania in the index patient and the graft donor was also retrospectively analysed by testing sera that were collected immediately before the transplant with the Leishmania Western Blot IgG (LDBio Diagnostics®, Lyon, France), a sensitive method to detect specific IgG in individuals with VL or asymptomatic Leishmania infection [9, 10]. The test revealed the presence of anti-leishmanial IgG in the patients’ serum immediately before the transplant, while the donor’s serum tested negative.
Methods
We conducted a review of case reports and case series published in the MEDLINE (PubMed) database between 1990 and 2021 using the following search terms: “Leishmania”, “transplant” and their derivatives, and excluding results relative to non-European countries, cutaneous leishmaniasis and haematological transplants. Furthermore, the bibliographies of extant case series were searched for relevant articles. The results included articles in English, French and Spanish.
Data were entered into a pre-designed Excel file. Information extracted from each paper was (1) country where the infection likely took place; (2) characteristics of patients (sex, age); (3) immunosuppressive treatment; (4) time to VL after transplant; (4) clinical and laboratory markers (5) histology of renal biopsy; (6) methods of VL diagnosis; (7) VL treatment; (8) outcome after treatment (including recovery, relapse, death).
Discussion
Epidemiology and transmission
VL is an underrecognized and misdiagnosed disease among transplant recipients [6]. According to our review of the extant literature (Table 1), 61 VL cases (including the current case) have been reported in KT recipients in southern Europe, or in patients who travelled there, since 1990. Most cases (n = 23) were reported in Spain, which is among the foremost countries in performing organ transplantation and in which L. infantum is endemic [11], followed by France (n = 15), Italy (n = 12, including the case of this study) and Greece (n = 5); Turkey reported two cases, and Portugal and Malta reported one VL case each. Finally, two cases were described in patients residing in non-endemic countries, but reporting travelling to Spain. Thus, VL is a threat for SOT recipients in areas where leishmaniasis is endemic.
In the examined case, reactivation of a latent infection was strongly suggested by the retrospective serological analysis of the patient’s and the donor’s sera, which were collected before transplantation; this may be of importance since we recently observed the presence of a latent Leishmania infection in 16% of ESRD patients in haemodialysis treatment [44]. These findings call for further evaluation of the clinical utility of pre-transplant screening strategies, which are currently not recommended for this parasitic infection [4].
VL onset and diagnosis
Development of VL is considered a late event post-transplantation, with an average VL onset at 18 months after transplants [6]. Accordingly, in southern Europe, 45 (75%) KT recipients who developed VL did so at least 6 months after the transplant (Table 1): this includes the examined case, who progressed into VL at around 18 months after receiving the graft.
Timely diagnosis of VL is critical in SOT recipients, but leishmaniasis is often overlooked in differential diagnosis, leading to treatment delay. Antinori et al. [6] reported a mean time to diagnosis of 30 days from the onset of symptoms, with peaks of up to 5 months. Time to diagnosis is seldom reported in studies of VL in KT, with only 13 (21%) case reports from southern Europe stating it (data not shown). In line with previous studies [6, 45], the current VL case was diagnosed 8 days after hospital admission, corresponding to 28 days after the symptoms’ onset.
In immunocompromised patients, diagnostic tools for VL exhibit variable performances, with serological tests showing lower sensitivity than in immunocompetent individuals and non-invasive direct diagnosis, such as molecular testing on peripheral blood, being of great value [46,47,48,49]. Nevertheless, microscopy on bone marrow samples has been the most used diagnostic method (53 cases, 87%), with PCR in peripheral or bone marrow blood carried out in 12 (20%) VL cases in KT recipients described in southern Europe, including the current case (Table 1).
Renal involvement in VL
Renal involvement is frequent in human leishmaniasis and it is associated with increased mortality. Clinical features are diverse, mainly represented by urinary abnormalities (proteinuria, haematuria, and pyuria) and acute kidney injury (AKI), which is reported in 4–46% of VL cases. Tubular and glomerular dysfunction have also been reported, although less frequently [5, 50,51,52,53].
Renal injury can be the consequence of direct kidney involvement, but can also be caused or exacerbated by concomitant events.
Direct Leishmania-induced renal damage mainly results from immunological phenomena, such as the deposition of immune complexes, activation of T cells, up-regulation of adhesion molecules, inflammatory processes, but can also be caused by parasite proliferation in the kidney tissue [54, 55] Beside VL, the other causes that can contribute to the development of renal damage in VL patients are drug toxicity, presence of associated infections and haemodynamic abnormalities [51, 53, 56]. Histological examination of graft biopsies in KT recipients with VL is seldom described (Table 1); findings range from the absence of parasites [39] to diffuse interstitial inflammation and abundant parasites [35] to complete occlusion of renal vasculature [34]. The examined case shows interstitial fibrosis, tubular atrophy and glomerulosclerosis (seven out of 13 glomeruli) at histology; these chronic lesions may be related to the prolonged damage caused by the parasitic infection, considering the long-time interval between VL onset and histological evaluation. The presence of leishmanial DNA in the kidney tissue sustains this hypothesis, even though no amastigotes were detected in the lesions.
VL treatment and monitoring
Treatment of VL in SOT recipients is mostly based on case reports or small case series. A high dose L-Amb (total dose of 40 mg/kg) is considered the therapy of choice in immunocompromised patients with VL; doses of immunosuppressive drugs should be decreased during VL treatment whenever possible [1]. In the examined case, immunosuppressants were decreased and the response to specific anti-leishmanial therapy was rapid.
qPCR on peripheral blood is considered the most useful technique for monitoring the efficacy of VL treatment and for identifying relapses in immunocompromised patients [1, 46]. In the current case, the employment of qPCR for the patient’s follow-up allowed the observation of an effective response to anti-parasitic therapy with a rapid drop of parasitaemia, with no Leishmania DNA detected in peripheral blood samples for the entire monitoring period (48 months) (Fig. 1a–c and data not shown). Importantly, leishmanial DNA can be detected in immunocompromised patients after treatment without clinical significance, thus caution should be taken to identify VL relapse merely on a positive PCR test [46]. qPCR should be used, with raised levels of parasitic DNA predicting relapses. It is also important to underline that qPCR results should be combined with clinical and laboratory signs to evaluate whether the patient undergo a clinically evident relapse and requires VL treatment.
Conclusions
VL must be suspected among the opportunistic infections that can develop in SOT patients who reside in (or travelled to) Leishmania-endemic countries, including southern Europe. As VL exhibits high mortality in KT patients, prompt VL diagnosis and early anti-parasitic treatment are essential. PCR in peripheral blood appears to be effective for VL identification and follow-up; nevertheless, standardization and validation of a consensus protocol for molecular diagnosis and parasite load estimation is still lacking as well a consensus for screening strategies for SOT candidates in endemic regions.
References
Gradoni L, López-Vélez R, Mokni M. Manual on case management and surveillance of the leishmaniases in the WHO European Region. Geneva: World Health Organization; 2017.
Clemente WT, Mourão PHO, Lopez-Medrano F, Schwartz BS, García-Donoso C, Torre-Cisneros J. Visceral and cutaneous leishmaniasis recommendations for solid organ transplant recipients and donors. Transplantation. 2018;102:S8–15.
Gajurel K, Dhakal R, Deresinski S. Leishmaniasis in solid organ and hematopoietic stem cell transplant recipients. Clin Transpl. 2017;31:e12867.
La Hoz RM, Morris MI, Transplantation IDCOPOTASO. Tissue and blood protozoa including toxoplasmosis, Chagas disease, leishmaniasis, Babesia, Acanthamoeba, Balamuthia, and Naegleria in solid organ transplant recipients. Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transpl. 2019;33:13546.
Clementi A, Battaglia G, Floris M, Castellino P, Ronco C, Cruz DN. Renal involvement in leishmaniasis: a review of the literature. NDT Plus. 2011;4:147–52.
Antinori S, Cascio A, Parravicini C, Bianchi R, Corbellino M. Leishmaniasis among organ transplant recipients. Lancet Infect Dis. 2008;8:191–9.
Varani S, Ortalli M, Attard L, et al. Serological and molecular tools to diagnose visceral leishmaniasis: 2-years’ experience of a single center in Northern Italy. PLoS ONE. 2017;12: e0183699.
Mary C, Faraut F, Lascombe L, Dumon H. Quantification of Leishmania infantum DNA by a real-time PCR assay with high sensitivity. J Clin Microbiol. 2004;42:5249–55.
Ortalli M, De Pascali AM, Longo S, et al. Asymptomatic Leishmania infantum infection in blood donors living in an endemic area, northeastern Italy. J Infect. 2020;80:116–20.
Lévêque MF, Battery E, Delaunay P, et al. Evaluation of six commercial kits for the serological diagnosis of Mediterranean visceral leishmaniasis. PLoS Negl Trop Dis. 2020;14: e0008139.
Akuffo H, Costa C, van Griensven J, Burza S, Moreno J, Herrero M. New insights into leishmaniasis in the immunosuppressed. PLoS Negl Trop Dis. 2018;12: e0006375.
Donovan KL, White AD, Cooke DA, Fisher DJ. Pancreatitis and palindromic arthropathy with effusions associated with sodium stibogluconate treatment in a renal transplant recipient. J Infect. 1990;21:107–10.
Le Cacheux P, Hurault de Ligny B, Reman O, Ryckelynck JP. Visceral leishmaniasis of favourable course in a patient with renal transplantation. Rev Med Interne. 1990;11:250–1.
Rousaud F, Solá R, Oliver A, Ayats R, del Rio G. Primary visceral leishmaniasis in a renal transplant patient. Nefrologia. 1991;11:72–4.
Orofino L, Marcen R, Gamez C, et al. Visceral leishmaniasis in renal transplant patients. Nephrol Dial Transpl. 1992;7:651.
Moulin B, Ollier J, Bouchouareb D, Purgus R, Olmer M. Leishmaniasis: a rare cause of unexplained fever in a renal graft recipient. Nephron. 1992;60:360–2.
Jokipii L, Salmela K, Saha H, et al. Leishmaniasis diagnosed from bronchoalveolar lavage. Scand J Infect Dis. 1992;24:677–81.
Dunan S, Mary C, Gambarelli F, et al. Four cases of visceral leishmaniasis in renal graft recipients. Epidemiological and therapeutical reflexions. Med Mal Infect. 1993;23:297–301.
Torregrosa JV, Ricart MJ, Montesinos M, et al. Visceral leishmaniasis-like cause of unexplained fever in a reno-pancreatic graft recipient. Nephron. 1993;65:318–9.
Moroni G, Bossi L. Don’t forget visceral leishmaniasis in transplant patients. Nephrol Dial Transpl. 1995;10:563–4.
Esteban RJ, Bravo JA, Osuna A, Asensio C. Early antimoniate poisoning in a non-fatal visceral leishmaniasis kidney transplant recipient with renal failure. Nephrol Dial Transpl. 1996;11:1898.
Torrús D, Boix V, Massa B, Portilla J, Pérez-Mateo M. Fluconazole plus allopurinol in treatment of visceral leishmaniasis. J Antimicrob Chemother. 1996;37:1042–3.
Apaydin S, Ataman R, Serdengeçt K, et al. Visceral leishmaniasis without fever in a kidney transplant recipient. Nephron. 1997;75:241–2.
Berenguer J, Gómez-Campderá F, Padilla B, et al. Visceral leishmaniasis (Kala-Azar) in transplant recipients: case report and review. Transplantation. 1998;65:1401–4.
Gómez Campderá F, Berenguer J, Anaya F, Rodriguez M, Valderrábano F. Visceral leishmaniasis in a renal transplant recipient. Short review and therapy alternative. Am J Nephrol. 1998;18:171.
Boletis JN, Pefanis A, Stathakis C, Helioti H, Kostakis A, Giamarellou H. Visceral leishmaniasis in renal transplant recipients: successful treatment with liposomal amphotericin B (AmBisome). Clin Infect Dis. 1999;28:1308–9.
Hernández-Pérez J, Yebra-Bango M, Jiménez-Martínez E, et al. Visceral leishmaniasis (kala-azar) in solid organ transplantation: report of five cases and review. Clin Infect Dis. 1999;29:918–21.
Hueso M, Bover J, Serón D, et al. The renal transplant patient with visceral leishmaniasis who could not tolerate meglumine antimoniate—cure with ketoconazole and allopurinol. Nephrol Dial Transpl. 1999;14:2941–3.
Llorente S, Gimeno L, Navarro MJ, Moreno S, Rodriguez-Gironés M. Therapy of visceral leishmaniasis in renal transplant recipients intolerant to pentavalent antimonials. Transplantation. 2000;70:800–1.
Rodríguez-Wilhelmi P, Panizo C, Ruza E, Rocha E. Treatment of visceral leishmaniasis with liposomal amphotericin B in three immunocompromised patients. Med Clin (Barc). 2001;116:37–8.
Sabbatini M, Pisani A, Ragosta A, Gallo R, Borrelli F, Cianciaruso B. Visceral Leishmaniasis in renal transplant recipients: is it still a challenge to the nephrologist? Transplantation. 2002;73:299–301.
Sipsas NV, Boletis J. Fever, hepatosplenomegaly, and pancytopenia in a renal transplant recipient. Transpl Infect Dis. 2003;5:47–52.
Basset D, Faraut F, Marty P, et al. Visceral leishmaniasis in organ transplant recipients: 11 new cases and a review of the literature. Microbes Infect. 2005;7:1370–5.
Veroux M, Corona D, Giuffrida G, et al. Visceral leishmaniasis in the early post-transplant period after kidney transplantation: clinical features and therapeutic management. Transpl Infect Dis. 2010;12:387–91.
Dettwiler S, McKee T, Hadaya K, Chappuis F, van Delden C, Moll S. Visceral leishmaniasis in a kidney transplant recipient: parasitic interstitial nephritis, a cause of renal dysfunction. Am J Transpl. 2010;10:1486–9.
Simon I, Wissing KM, Del Marmol V, et al. Recurrent leishmaniasis in kidney transplant recipients: report of 2 cases and systematic review of the literature. Transpl Infect Dis. 2011;13:397–406.
Postorino MC, Bellantoni M, Catalano C, et al. Visceral leishmaniasis reactivation in transplant patients: a minireview with report of a new case. J Nephrol. 2011;24:530–4.
Yücel S, Ozcan D, Seçkin D, Allahverdiyev AM, Kayaselçuk F, Haberal M. Visceral leishmaniasis with cutaneous dissemination in a renal transplant recipient. Eur J Dermatol. 2013;23:892–3.
Duvignaud A, Receveur MC, Ezzedine K, Pistone T, Malvy D. Visceral leishmaniasis due to Leishmania infantum in a kidney transplant recipient living in France. Travel Med Infect Dis. 2015;13:115–6.
Pedroso JA, Paola Salerno M, Spagnoletti G, et al. Elderly kidney transplant recipient with intermittent fever: a case report of leishmaniasis with acute kidney injury during liposomal amphotericin B therapy. Transpl Proc. 2014;46:2365–7.
Pérez-Jacoiste Asín MA, Carrasco-Antón N, Fernández-Ruiz M, et al. Experience with miltefosine for persistent or relapsing visceral leishmaniasis in solid organ transplant recipients: a case series from Spain. Transpl Infect Dis. 2017;19:13546.
Clavijo Sánchez F, Vázquez Sánchez T, Cabello Díaz M, Sola Moyano VE, Jironada Gallego C, Hernández MD. Visceral leishmaniasis in renal transplant recipients: report of 2 cases. Transpl Proc. 2018;50:581–2.
Marques N, Bustorff M, Cordeiro Da Silva A, et al. Visceral dissemination of mucocutaneous leishmaniasis in a kidney transplant recipient. Pathogens. 2020. https://doi.org/10.3390/pathogens10010018.
Comai G, Mistral De Pascali A, Busutti M, et al. Screening strategies for the diagnosis of asymptomatic Leishmania infection in dialysis patients as a model for kidney transplant candidates. J Nephrol. 2021;34:191–5.
Clemente W, Vidal E, Girão E, et al. Risk factors, clinical features and outcomes of visceral leishmaniasis in solid-organ transplant recipients: a retrospective multicenter case-control study. Clin Microbiol Infect. 2015;21:89–95.
van Griensven J, Diro E. Visceral leishmaniasis: recent advances in diagnostics and treatment regimens. Infect Dis Clin N Am. 2019;33:79–99.
de Ruiter CM, van der Veer C, Leeflang MM, Deborggraeve S, Lucas C, Adams ER. Molecular tools for diagnosis of visceral leishmaniasis: systematic review and meta-analysis of diagnostic test accuracy. J Clin Microbiol. 2014;52:3147–55.
van Griensven J, Carrillo E, López-Vélez R, Lynen L, Moreno J. Leishmaniasis in immunosuppressed individuals. Clin Microbiol Infect. 2014;20:286–99.
Aronson N, Herwaldt BL, Libman M, Pearson R, Lopez-Velez R, Weina P, Carvalho EM, Ephros M, Jeronimo S, Magill A. Diagnosis and treatment of leishmaniasis: clinical practice guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH). Clin Infect Dis. 2016;63:e202–64. https://doi.org/10.1093/cid/ciw670.
Silva Junior GB, Barros EJ, Daher EEF. Kidney involvement in leishmaniasis–a review. Braz J Infect Dis. 2014;18:434–40.
Oliveira MJ, Silva Júnior GB, Abreu KL, et al. Risk factors for acute kidney injury in visceral leishmaniasis (Kala-Azar). Am J Trop Med Hyg. 2010;82:449–53.
Dutra M, Martinelli R, de Carvalho EM, Rodrigues LE, Brito E, Rocha H. Renal involvement in visceral leishmaniasis. Am J Kidney Dis. 1985;6:22–7.
Hailu W, Mohamed R, Fikre H, et al. Acute kidney injury in patients with Visceral Leishmaniasis in Northwest Ethiopia. PLoS ONE. 2021;16: e0252419.
Daher EF, da Silva Junior GB, Trivedi M, et al. Kidney complications of parasitic diseases. Nat Rev Nephrol. 2022. https://doi.org/10.1038/s41581-022-00558-z.
Sethi S, Fervenza FC, Siddiqui A, Quint PS, Pritt BS. Leishmaniasis-associated membranoproliferative glomerulonephritis with massive complement deposition. Kidney Int Rep. 2016;1:125–30.
Deray G. Amphotericin B nephrotoxicity. J Antimicrob Chemother. 2002;49:37–41.
Funding
This manuscript was supported by research fundings from the Italian Health Ministry “Ministero della Salute” (Ricerca Corrente).
Author information
Authors and Affiliations
Contributions
MB: conceptualisation, writing—original draft, data curation, visualisation, formal analysis. AD: conceptualisation, writing—original draft, data curation, visualisation, formal analysis. AMP: investigation, resources. MO: investigation, resources. LA: supervision, writing—review and editing. BG: visualisation, investigation, writing—review and editing. BF: investigation, resources. GLM: supervision, writing—review and editing. GC: conceptualisation, writing—review and editing, methodology, visualisation. SV: conceptualisation, writing—original draft, visualisation, methodology, project administration.
Corresponding author
Ethics declarations
Conflict of interest
All other authors declare that they have no relevant financial interests.
Ethical approval
Ethical approval was not needed by local ethical committee, as this is a case report. Patient provided written informed consent to publish details of this case. A copy of the consent form is available for review by the Editor of this journal.
Consent to participate
Not applicable.
Consent to publish
All authors confirm that they had full access to all the data in the study and accept responsibility to submit for publication. Patient gave consent to publication.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Busutti, M., Deni, A., De Pascali, A.M. et al. Updated diagnosis and graft involvement for visceral leishmaniasis in kidney transplant recipients: a case report and literature review. Infection 51, 507–518 (2023). https://doi.org/10.1007/s15010-022-01943-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-022-01943-3