
Abstract
The aim of this research is to study the influence of atmospheric pollutants and meteorological variables on the incidence rate of COVID-19 and the rate of hospital admissions due to COVID-19 during the first and second waves in nine Spanish provinces. Numerous studies analyze the effect of environmental and pollution variables separately, but few that include them in the same analysis together, and even fewer that compare their effects between the first and second waves of the virus. This study was conducted in nine of 52 Spanish provinces, using generalized linear models with Poisson link between levels of PM10, NO2 and O3 (independent variables) and maximum temperature and absolute humidity and the rates of incidence and hospital admissions of COVID-19 (dependent variables), establishing a series of significant lags. Using the estimators obtained from the significant multivariate models, the relative risks associated with these variables were calculated for increases of 10 µg/m3 for pollutants, 1 °C for temperature and 1 g/m3 for humidity. The results suggest that NO2 has a greater association than the other air pollution variables and the meteorological variables. There was a greater association with O3 in the first wave and with NO2 in the second. Pollutants showed a homogeneous distribution across the country. We conclude that, compared to other air pollutants and meteorological variables, NO2 is a protagonist that may modulate the incidence and severity of COVID-19, though preventive public health measures such as masking and hand washing are still very important.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In December 2019 in Wuhan (China), cases of pneumonia were detected, brought about by an unknown coronavirus. The newly discovered virus was called SARS-CoV-2 and its associated illness, Coronavirus Disease 19 (COVID-19). In light of the global increase in cases, the World Health Organization (WHO) declared COVID-19 a “pandemic” on March 11, 2020 (Cucinotta and Vanelli 2020; WHO 2020).
The first case of COVID-19 was detected in Spain in late January of 2020. During the month of February, cases began to be diagnosed around the country. Due to an exponential increase in cases, a state of alarm was declared in all of Spain, and the general population was confined to their homes (BOE 2020a). The state of alarm ended on June 21, 2020 (BOE 2020b). After the summer months, a new state of alarm was declared in all of the national territory (BOE 2020c), which resulted in a nighttime curfew and which ended on May 9, 2021 (BOE 2020d).
Air pollution is a current environmental problem. Among all of the pollutants, particulate matter under 10 µm in diameter (PM10), nitrogen dioxide (NO2) and ozone (O3) are among the most recognized pollutants in the scientific literature (Adamkiewicz et al. 2020; Chen et al. 2007a, b; Kampa and Castanas 2008).
PM10 are a group of diverse pollutants that are capable of causing different respiratory and cardiovascular diseases, among others (de Kok et al. 2006; Querol et al. 2004). Although they can be of natural origin, it is anthropogenic origin that is considered the most problematic for health, given that it is strongly linked to road traffic (de Kok et al. 2006), which is one of its primary determinants. Studies link hospital admissions in adults with PM10 in a positive way. Thus, when there is a greater concentration of PM10 in the environment, there is an increase in admissions due to illnesses related to the respiratory and circulatory systems (Ab Manan et al. 2018). Some studies have linked air pollution caused by particulate matter (PM) to other respiratory diseases caused by coronaviruses such as SARS (Cui et al. 2003). Some studies also seem to conclude that the presence of pollution by these compounds above the established limits has a positive influence [when there is more pollution, there seem to be more cases reported (Coccia 2020a)].
The effect of NO2 on human health is well documented in the scientific literature. A short-term exposure to NO2 is capable of increasing the risk of contracting cardiorespiratory disease (Kampa and Castanas 2008). Travaglio et al. (2021) found that in the UK the presence of excess NO2 was a good estimator of the number of cases and deaths due to COVID-19. This has been confirmed in other studies carried out in Northern Italy (Zoran et al. 2020), which have also defined a geographic component to the distribution of the transmission of the virus. The areas most polluted by NO2 seem to have a higher incidence of COVID-19, as indicated by studies carried out in northern Italy (specifically in the city of Milan) and in the province of Tarragona, in the region of Catalonia (Marquès et al. 2021; Zoran et al. 2020). However, in Spain studies such as that of Linares et al. have not found sufficient evidence of this distribution of the disease (Linares et al. 2021).
O3 is an air pollutant that is only considered as such when it appears in the lowest layer of the atmosphere, known as the troposphere. However, when studied together with NO2, O3 becomes secondary as it acts as a precursor to NO2 in the photochemical reaction in which it is formed (Logan 1985). The marked seasonality presented by concentrations of O3, normally during the summer months (Logan 1985), has a certain influence on how this air pollutant behaves in conjunction with epidemiological variables related to COVID-19 (Zoran et al. 2020). Therefore, O3 is related to an increase in morbidity and mortality due to cardiovascular and respiratory problems.
Noise pollution is an agent that is capable of affecting health (Stansfeld and Matheson 2003). It has been shown that high levels of noise positively affect the incidence and severity of COVID-19, which increase when noise pollution increases, independently of other factors such as PM10, NO2 and other air pollutants (Díaz et al. 2021).
Furthermore, it has also been shown that, in addition to air pollution and noise pollution, other agents are also capable of significantly influencing the incidence and severity of COVID-19. These variables are classified as “meteorological variables” and include maximum temperature and absolute humidity, among others. When the pandemic began, because of the lack of quality scientific information available, it was thought that because SARS-CoV-2 was a respiratory virus it would be affected by low and humid temperatures (Tang 2009), as was the case with other types of coronavirus such as SARS or MERS. However, after advances in knowledge related to the virus, other authors consider that the best transmission occurs in environments without high humidity, though this can be distorted by the implementation of public health measures (Mecenas et al. 2020).
The existence of a nonlinear relationship between temperature and the number of cases reported suggests that the transmission of the virus cannot be stopped without additional preventive public health measures, such as the use of masks, hand washing and social distancing (Vokó and Pitter 2020; Yin et al. 2021). Some studies seem to point to the existence of an association between lower temperatures and greater transmission of the virus, given that in low temperatures people gather together indoors in places that tend to have less ventilation (Ujiie et al. 2020).
In addition to the meteorological variables mentioned above, there are other variables that influence the epidemiological variables of COVID-19. Some of these are solar radiation, which seems to present a positive correlation with COVID-19 incidence (Isaia et al. 2021), wind direction and speed, which presents a negative relationship between wind speed and COVID-19 incidence (Coccia 2020b), among others. However, in this study they have not been taken into account due to the impossibility of obtaining data in all the Spanish provinces to be analyzed.
The objective of this study was to confirm the existence of an association between air pollutants and meteorological variables and the incidence and severity of COVID-19. This study was carried out in nine of the fifty-two provinces of Spain during the first and second waves of the COVID-19 pandemic.
Materials and methods
Area, period and study type
This study was an ecological, longitudinal, retrospective time-series study. The study population was the Spanish population, which used a sample of nine provinces based on the geographic regions defined by the Ministry of Ecological Transition and Demographic Challenge (MITECO).
The selected provinces represented the nine geographic areas mentioned: A Coruña (Northwest), Vizcaya (North), Zaragoza (Northeast), Madrid (Center), Valencia (East), Palma de Mallorca (Balearic Islands), Sevilla (Southwest) Malaga (Southeast) and Las Palmas of Gran Canaria (Canary Islands). These provinces were representative of their corresponding geographic regions. The measurements were taken in the province capitals. Provinces included had complete information on the presence of PM10, NO2 and O3 and meteorological variables. Those provinces, which could not provide this information, were excluded.
The time period of this study was from February 1, 2020, through May 31, 2020 (first wave), and from June 1, 2020, through November 30, 2020 (second wave).
Dependent and independent variables
Dependent variables used included the incidence rate of COVID-19 (TIC) and the rate of hospital admissions due to COVID-19 (TIHC). Rates were calculated in the following way:
Incidence rate per 1,000,000 inhabitants: (Number of positive COVID-19 cases/population) × 1,000,000 inhabitants.
Rate of admissions per 1,000,000 inhabitants: (Number of hospital admissions due to COVID-19/population) × 1,000,000 inhabitants.
The data on positive cases and admissions were provided by the National Center for Epidemiology (CNE) of the Carlos III Health Institute, and the population data were provided by the National Statistics Institute (INE).
The independent variables in this study were the concentrations of the air pollutants PM10, NO2 and O3 and the average values of the meteorological variables maximum temperature (Tmax) and absolute humidity (HA). The data on air pollutants were provided by MITECO, and the meteorological variables were provided by the State Meteorological Agency (AEMET).
HA was calculated using the Clausus Clapeyron equation based on the average daily relative humidity (HR) and the average daily temperature (Iribarne and Cho 1980):
Statistical analysis
Generalized linear models (GLM) with Poisson link were carried out in the selected provinces between the dependent variables and the average values of the independent variables, by which a series of lags were established. In carrying out the GLM, we controlled for the series trend by introducing the variable “n1”, which took a value of 1 on February 1, 2020, and June 1, 2020, and increased to 121 (May 31) and 183 (November 30). We also controlled for the seasonality of the time series at 120, 90, 60 and 30 days for the first wave and 180, 120, 90, 60 and 30 days for the second wave, and for over-dispersion by using an autoregressive component of order 1.
The lag period considered was 28 days, divided into four periods of 7 days each, which was the time thought to be related to contagion [with an incubation period, set at 4.5 and 5.6 days (Bolaño-Ortiz et al. 2020; Quesada and Gutiérrez 2021)] and a worsening of symptoms resulting in a hospital admission. The lags were introduced between days 0 and 7, 8 and 14, 15 and 21, and finally 22 and 28.
The dependent and independent variables were included in a single significant multivariate model. Based on the estimators of the model (β), the relative risks (RRs) were calculated, using the expression \({\text{RR}} = e^{\beta }\) based on the absolute value of the estimator. The RR was calculated for increases of 10 µg/m3 for the air pollutants, 1 °C for Tmax and 1 g/m3 for HA. In cases where the estimator obtained in the multivariate model was a negative number, a negative relationship between the dependent and independent variables was said to exist (if there is an increase in the dependent variable, the independent variable decreases, and vice versa). As an example, the population attributable risk was calculated (RAP) using the expression \({\text{RAP}} = \left( {{\text{RR}} - 1/{\text{RR}}} \right) \times 100\), which allows for calculation of the incidence of the variable at the population level.
The modeling process was carried out using a back-stepwise methodology with a p value of < 0.05.
Software used
The programs STATA 16.1 and SPSS 25 were used for the GLM and the time-series analysis. The maps were produced using Qqis 3.16.3, and tables were constructed using Microsoft Excel.
Results and discussion
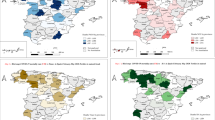
The relative risks (RRs) related to the air pollutants (PM10, NO2 and O3) calculated based on the GLM carried out in the analyzed provinces for TIC and TIHC are shown in Fig. 1 (corresponding to TIC). The relative risks (RRs) related to the meteorological variables (Tmax and HA) calculated using the GLM in the selected provinces are shown in Figs. 2, 3 shows the RRs corresponding to TIHC and air pollutants (see Supplementary Table 1). Figure 4 shows the RRs calculated for the meteorological variables and TIHC. The maps show the information related to RR classified into terciles using natural breaks.

Maps of air pollutants (μg/m3) associated with the rate of incidence of COVID-19 (TIC) in provinces in Spain (*) from Feb., 1 through May 31, 2020 and Jun., 1 through November 30, 2020. Tertiles in natural breack

Maps of atmospheric variables associated with the rate of incidence of COVID-19 (TIC) in provinces in Spain (*) from Feb., 1 through May 31, 2020 and Jun., 1 through November 30, 2020. Tertiles in natural breack
About 56 percent of the provinces presented a significant association between PM10 and TIC in the first wave and 44 percent in the second wave (Supplementary Table 1). Thirty-three percent of provinces were identified that presented an association between PM10 and TIHC both for the first and second waves (see Table 1).
Tables 2 and 3 shows the provinces with lag days associated with TIC and TIHC for the air pollutants considered (PM10, NO2 y O3) and the meteorological variables (Tmax y HA). The specified lag days are indicated in parentheses.
It can be seen in Fig. 1a, d that there was a decrease in the number of provinces that presented an association between PM10 and TIC between the first and second waves (see Table 1). Between the two waves, the most frequent tercile was tercile 2. As shown in Supplementary Table 1a, the greatest value of RR of an association between PM10 and TIC was 1.036 (IC 95% 1.00–1.07) for the first wave 1.021 (IC 95% 1.00–1.04) for the second wave. Figure 3a, d show that for TIHC there was neither an increase nor a decrease in the number of provinces that presented an association between TIHC and PM10 (see Table 1). In the first wave, the three associated provinces were found in different terciles, and the same occurred in the second wave. The greatest value of RR of association between PM10 and TIHC was 1.030 (IC 95% 1.00–1.05) in the first wave and 1.022 (IC 95% 1.00–1.04) (see Supplementary Table 1b). By way of example, we calculated the attributable risk (RA) for TIC and TIHC of PM10, which was 7.07 percent for the first wave and 4.16 for the second in relation to TIC, and 5.91 percent for the first wave and 4.35 percent for the second in relation to TIHC.

Maps of air pollutants (μg/m3) associated with the rate of hospital admissions of COVID-19 (TIHC) in provinces in Spain (*) from Feb., 1 through May 31, 2020 and Jun., 1 through November 30, 2020. Tertiles in natural breack
About 89 percent of the provinces presented an association between NO2 and TIC during the first wave, while for the second wave this increased to 100 percent. For NO2 and TIHC, associations were identified in 44 percent of the provinces for the first wave, while the second wave produced an increase of 89 percent (see Table 1).
Figure 1b, e showed an increase in the percentage of provinces that presented an association between NO2 and TIC in the first and second waves. The lag days that were significantly associated were found primarily between days 0 and 14 (see Table 2). In the first wave, the most frequent tercile was tercile 1, while for the second wave it was tercile 2. Therefore, in addition to an increase in the number of provinces with an association, those that maintained an association between the two waves primarily increased in tercile from the first to the second wave. The RR of association between NO2 and TIC that was highest in the first wave had a value of 1.339 (IC 95% 1,01–1,79); the value for the second wave was 1.174 (IC 95% 1,01–1,34). Figure 3b, e show the association between TIHC and NO2. As shown, there was an important increase in the association between the first and second waves. In the first wave, the most frequent tercile was tercile 2, while for the second wave it was tercile 1. This could signal that the provinces that previously had an association experienced a decrease in the RR of association between NO2 and TIHC; however, in reality, four provinces did not present an association in the first wave but did so in the second. In the first wave, the RR of association between NO2 and TIHC with the highest value was 1.051 (IC 95% 1.02–1.08), while for the second it was 1.158 (IC 95% 1.00–1.31) (see Supplementary Table 1b).
Statistically significant associations were found between O3 and TIC for 56 percent of the provinces in the first wave and 44 percent in the second. Fifty-six percent of provinces showed an association for O3 and TIHC in both waves (see Table 1).
Figure 1c, f show a decrease in the provinces showing an association between TIC and O3 (see Table 1). In the first wave, the most frequent tercile was tercile 2, while in the second it decreased to tercile 1. The highest value for the RR of association between O3 and TIC was 1.146 (IC 95% 1.00–1.28), while for the second, it was 1.050 (IC 95% 1.00–1.10). Figure 3c, f show the provinces with significant associations between O3 and TIHC. As can be seen, there was a decrease in the number of associated provinces in the second wave, similarly to what occurred with TIC. During the first wave, the terciles that were most frequently associated were terciles 2 and 1. During the second wave, tercile 1 was most frequently associated. The highest RR of association between TIHC and O3 for the first wave was 1.065 (IC 95% 1,01–1,12) and 1.031 (IC 95% 1,00–1,06) for the second wave.
We found significant associations between Tmax and TIC in 67 percent of the provinces in the first wave and 33 percent in the second. A single province showed an association between Tmax and TIHC (11%) in the first wave, and two provinces did so in the second (22%) (see Table 1). Figure 2a, c show the provinces that showed an association between Tmax and TIC. The provinces with an association were reduced by half (from 6 to 3) from the first wave to the second. The RR of association between TIC and Tmax with the highest value was 1.161 (IC 95% 1.00–1.32) for the first wave and 1.127 (IC 95% 1,01–1,24) for the second wave. Figure 4a, c show the association between Tmax and TIHC. The number of provinces that showed an association decreased between the first and second waves (Table 1). In the first wave, the maximum value of the RR of association between TIHC and Tmax was 1.096 (IC 95% 1.04–1.15) for the first wave and (IC 95% 1.00–1.06) for the second wave.

Maps of atmospheric variables associated with the rate of hospital admissions of COVID-19 (TIC) in provinces in Spain (*) from Feb., 1 through May 31, 2020 and Jun., 1 through November 30, 2020. Tertiles in natural breack
In terms of TIC and HA, associations were found in 67 percent of the provinces for the first wave and 33 percent for the second. For TIHC and HA, associations were found in 11 percent of the provinces for the first wave and 22 percent for the second (see Table 1).
Figure 2b, d show the provinces that presented an association between HA and TIC. During the second wave, there was a decrease in the number of associations, compared to the first wave. For the first wave, the greatest value for the RR of association between TIC and HA was 2.946 (IC 95% 1.01–4.89) and 1.082 (IC 95% 1.00–1.16) wave. Figure 4b, d show the provinces that had an association between TIHC and HA. There was an increase in the number of provinces with an association between the first and second waves (see Table 1). The maximum RR of association between TIHC and HA was 1.050 (IC 95% 1.01–1.09) for the first wave and 1.045 (IC 95% 1.02–1.07) for the second wave. (The RR values and their confidence intervals are shown in Supplementary Tables 1a, b.)
Discussion
Nitrogen dioxide (NO2)
The principal finding of this study was a high increase in the number of provinces with an association between NO2 and TIC between the first and second waves of COVID-19. This increase was the consequence of the end of confinement in homes and an increase in the number of cars in circulation, which increased the concentration of NO2 in the environment (Baldasano 2020). The origin of NO2 in the atmosphere is, primarily, an anthropogenic phenomenon based on emissions from individual and industrial vehicles (Grange et al. 2019). The short-term exposure to high concentrations of NO2 has been frequently studied, and such studies have found different negative effects on health and increases in the risk of respiratory tract infections, decreases in lung capacity in individuals, asthma, bronchitis, emphysema, etc., especially in children (Copat et al. 2020).
Prior studies (Linares et al. 2021; Travaglio et al. 2021; Zhu et al. 2020) conclude that among all of the air pollutants, NO2 is the compound that has the greatest association with TIC. There is a similar relationship with TIHC, although it is somewhat lesser than TIC, given that a subject requiring hospitalization is also affected by other factors such as the presence of comorbidities, among others (Ab Manan et al. 2018).
In studies such as those carried out by Copat et al. (2020) and Zhu et al., (2020) it has been found that an increase in the concentration of NO2 (by 10 µg/m3) with lags of between 0 and 14 days) is associated with a 6.94 percent increase in the number of cases. This tendency was confirmed by this study, given that in the majority of the provinces that presented an association with NO2 the lag days were found between day 0 and 14, which is also confirmed by studies carried out on the physiopathology of the SARS-CoV-2 virus (Quesada and Gutiérrez 2021). The angiotensin angiotensin-converting enzyme II (AEC2) has been proposed as a mechanism by which SARS-CoV-2 acts, since it acts as a receptor for the virus in the sense that the entrance of the virus into the organism is capable of blocking it (Lamas-Barreiro et al. 2020). It has been suggested that NO2 could influence the interference process in AEC2, due to the presence of high levels in the pulmonary cells (Alifano et al. 2020), as occurs with SARS-CoV-2. This generates imbalances in the inflammatory response of the organism, which ends up severely worsening the disease.
Studies carried out in other parts of Europe, such as in the North of Italy, suggest that concentrations of NO2 are found in urban areas such as Milan (Zoran et al. 2020). However, prior studies carried out in Spain (Linares et al. 2021) do not show a special distribution in the accumulation of NO2, nor did we find this in the present study.
Particulate matter under 10 µm in diameter (PM10)
Emissions of PM10 in the atmosphere are primarily a consequence of road traffic or the mineral dust emitted during construction work (Querol et al. 2004). Thus, different studies such as that carried out by Kim et al. have found associations between exposure to an overly high concentration of this pollutant and respiratory diseases such as asthma, lung cancer and chronic obstructive pulmonary disease (COPD) and circulatory diseases, with the appearance of non-lethal arrhythmias and myocardial strokes, and a clear elevation in the risk of hospitalization and emergency room visits (Copat et al. 2020; Kim et al. 2018). These findings support the associations found in the present study.
In general, these types of particulate matter (whether PM2.5 or PM10) have a great influence on hospital admissions due to both cardiovascular and respiratory illnesses, because they are capable of overcoming the lung’s defense mechanisms and can penetrate the blood flow and thus affect the circulatory system (Ab Manan et al. 2018; Cheng et al. 2015).
In terms of COVID-19, there is a positive relationship between TIC and TIHC and PM10 concentrations in the environment, even though this relationship is less strong than the relationship between NO2 and TIC and TIHC,
especially in places in which maximum recommended levels have been surpassed 14 days prior to the onset of symptoms (Copat et al. 2020; Setti et al. 2020). In the present study, the majority of significant lags were found between day 0 and 14, which makes sense given the incubation period of the disease (Quesada and Gutiérrez 2021).
Ozone (O3)
The presence of ozone in the atmosphere is considered natural and even beneficial, when it is present in the upper layers of the stratosphere, for example the so-called ozone cap. When it is found in the lowest layer, the troposphere, it is considered a pollutant and is damaging to human health (Logan 1985). The effects on health of this pollutant include respiratory irritation (which causes cough among other symptoms), a reduction in pulmonary function and worsening of chronic lung diseases such as emphysema and bronchitis (Chen et al. 2007a; Radakovic and Krope 2007).
The concentration of this compound presents a collinear relationship with NO2. This is due to the origin of tropospheric ozone as a secondary pollutant and product of the photochemical reaction \({\text{NO}}\left( {\text{g}} \right) + {\text{O}}_{3} \left( {\text{g}} \right) \to {\text{NO}}_{2} \left( {\text{g}} \right)\), which establishes an inverse relationship between both concentrations (Logan 1985; Zoran et al. 2020) and ends up forming part of what is known as “photochemical smog.” It is generally more abundant in peripheral zones, in which there is a lower concentration of nitrogen oxide, than in urban zones, in which it intervenes in the above-mentioned chemical reaction (though this tendency has become inverted in recent years) (Paoletti et al. 2014).
During the confinement in homes that took place during the first wave, the concentration of O3 increased compared to the prior year (Briz-Redón et al. 2021). This phenomenon can be explained due to the absence of NO2 due to the confinement. The level of O3 increased in a notable way during the first wave, primarily due to the absence of NO2 due to the confinement. The lack of photochemical reaction and formation of NO2 meant a greater concentration of O3 compared to NO2. This influenced TIC and TIHC, as more provinces had an association for O3 than for NO2 in the first wave. The situation inverted during the second wave, in which there were no mobility restrictions. Motor traffic resumed as did activities that cause NO2 emissions, and in consequence, levels of NO2 recovered, with a decrease in the level of O3. Thus, associations between TIC and TIHC decreased during the second wave.
Maximum temperature (Tmax)
The temperature is one of the most influential factors in the transmission of viral pathogens that spread through the air, because they are sensitive to changes in this variable (Tang 2009). A study carried out by Cheng et al. suggested that hospital admissions due to respiratory illness related to PM10 may be positively associated with lower temperatures, while there is no association with higher temperatures, even when adding other pollutants (Cheng et al. 2015).
The influence of temperature on the expansion and severity of COVID-19 has been debated. While some authors have found that a higher temperature implies a decrease in the number of cases (Bolaño-Ortiz et al. 2020; To et al. 2021), others have found no association (Xie and Zhu 2020). The present study did not find any association between an increase in TIC and TIHC and a decrease in temperature, although fewer provinces were found with an association with Tmax than provinces associated with air pollutants.
Absolute humidity (HA)
Prior studies using the absolute humidity variable have not had conclusive results. While some have found a negative association between the incidence of COVID-19 and humidity (Liu et al. 2020; Şahin 2020), others have found that environments with high humidity favor the transmission of the virus (Islam et al. 2021a, b), which coincides with what is known about other types of respiratory viruses. However, other studies have not found an association between epidemiological variables related to COVID-19 and humidity. Recent studies suggest the possibility that the SARS-CoV-2 virus, which causes COVID-19, presents better transmission in dry environments than in humid ones (Correa-Araneda et al. 2021; Sajadi et al. 2020), although a more humid environment does not prevent the transmission or severity of the disease. Therefore, public health measures are needed that focus on prevention, such as the use of masks and social distancing (Vokó and Pitter 2020; Yin et al. 2021).
It should be noted that both the Tmax and HA variables that were used in this study presented negative relationships with TIC and TIHC. That is to say that an increase in one of the meteorological variables is accompanied by a decrease in the epidemiological variables, and vice versa.
This study found that, in addition to temperature, humidity was associated in a lower number of provinces than were the air pollutants, both for TIC and for TIHC, although the relationship found in terms of TIHC was very weak.
Strengths and limitations of the study
The primary strength of this study was its ability to use both air pollutants and meteorological variables in a single significant GLM, which better corresponds to the true relationship between variables. Another strength was the availability of data for both of the waves of COVID-19, which allowed for a comparative analysis of the two waves.
One of the limitations relates to the home confinement measures implemented during the first state of alarm at the national level, which modified the levels of air pollutants such as NO2 and O3. Another limitation relates to the limited diagnostic tests that were carried out during the first wave. PCR tests (antigen tests were not available during this period) were only carried out with patients that presented severe symptoms of the disease, which could have influenced the number of cases reported during the period and affected incidence and admissions. Another of the limitations that we have found in this study is the subsequent modification of the data on the incidence of hospital admissions in some of the provinces analyzed, which may have modified the data with respect to previous studies.
In addition to temperature and absolute humidity, there are other meteorological variables that are capable of influencing COVID-19 expansion, such as wind speed and direction (Coccia 2021, 2020b; Islam et al. 2021a, b), and solar radiation. However, these factors have not been taken into account in this study due to the absence of data on them in all the provinces analyzed.
Conclusion
The primary conclusion of this research relates to the protagonist role played by NO2 in the first and second waves of COVID-19. The rest of the air pollutants and meteorological variables presented a less important role than did NO2. There was no specific geographic behavior in the country in terms of the air pollutants and the meteorological variables.
Among the factors analyzed in this study, NO2 is the one that shows the most association, although there are others that have not been analyzed such as radiation, wind speed and noise pollution.
Data availability
No human subjects were used as this was an ecological analysis. The COVID-19 data used in this study are subject to statistical secrecy and, therefore, are not freely available.
References
Adamkiewicz G, Liddie J, Gaffin JM (2020) The respiratory risks of ambient/outdoor air pollution. Clin Chest Med 41(4):809–824. https://doi.org/10.1016/j.ccm.2020.08.013
Alifano M, Alifano P, Forgez P, Iannelli A (2020) Renin-angiotensin system at the heart of COVID-19 pandemic. Biochimie 174:30–33. https://doi.org/10.1016/j.biochi.2020.04.008
Baldasano JM (2020) COVID-19 lockdown effects on air quality by NO2 in the cities of Barcelona and Madrid (Spain). Sci Total Environ. https://doi.org/10.1016/j.scitotenv.2020.140353
BOE (2020a) Real Decreto 463/2020, de 14 de marzo, por el que se declara el estado de alarma para la gestión de la situación de crisis sanitaria ocasionada por el COVID-19. Boletín of Del Estado 67:25390–25400
BOE (2020b) Real Decreto 555/2020, de 5 de junio, por el que se prorroga el estado de alarma declarado por el Real Decreto 463/2020, de 14 de marzo, por el que se declara el estado de alarma para la gestión de la situación de crisis sanitaria ocasionada por el COVID-. Boletín of Del Estado 67:61561–61567
BOE (2020c) Real Decreto 926/2020, de 25 de octubre, por el que se declara el estado de alarma para contener la propagación de infecciones causadas por el SARS-CoV-2. del Estado, Boletín Of
BOE (2020d) Real Decreto 956/2020, de 3 de noviembre, por el que se prorroga el estado de alarma declarado por el Real Decreto 926/2020, de 25 de octubre, por el que se declara el estado de alarma para contener la propagación de infecciones causadas por el SARS-CoV-2. del Estado, Boletín Of, pp 61561–61567
Bolaño-Ortiz TR, Camargo-Caicedo Y, Puliafito SE, Ruggeri MF, Mayor-Bracero OL, Torres-Delgado E, Cereceda-Balic F (2020) Spread of SARS-CoV-2 through Latin America and the Caribbean region: a look from its economics conditions, climate and air indicators. Environ Res. https://doi.org/10.1016/j.envres.2020.109938
Briz-Redón Á, Belenguer-Sapiña C, Serrano-Aroca Á (2021) Changes in air pollution during COVID-19 lockdown in Spain: a multi-city study. J Environ Sci 101:16–26. https://doi.org/10.1016/j.jes.2020.07.029
Chen TM, Gokhale J, Shofer S, Kuschner WG (2007a) Outdoor air pollution: ozone health effects. Am J Med Sci 333:244–248. https://doi.org/10.1097/MAJ.0b013e31803b8e8c
Chen TM, Gokhale J, Shofer S, Kuschner WG (2007b) Outdoor air pollution: particulate matter health effects. Am J Med Sci 333:235–243. https://doi.org/10.1097/MAJ.0b013e31803b8dcc
Cheng MH, Chiu HF, Yang CY (2015) Coarse particulate air pollution associated with increased risk of hospital admissions for respiratory diseases in a Tropical city, Kaohsiung. Taiwan Int J Environ Res Public Health 12:13053–13068. https://doi.org/10.3390/ijerph121013053
Coccia M (2020a) An index to quantify environmental risk of exposure to future epidemics of the COVID-19 and similar viral agents: theory and practice. Environ Res 191:110155. https://doi.org/10.1016/j.envres.2020.110155
Coccia M (2020b) How (Un)sustainable environments are related to the diffusion of covid-19: the relation between coronavirus disease 2019, air pollution, wind resource and energy. Sustain 12:1–12. https://doi.org/10.3390/su12229709
Coccia M (2021) The effects of atmospheric stability with low wind speed and of air pollution on the accelerated transmission dynamics of COVID-19. Int J Environ Stud 78:1–27. https://doi.org/10.1080/00207233.2020.1802937
Copat C, Cristaldi A, Fiore M, Grasso A, Zuccarello P, Signorelli SS, Conti GO, Ferrante M (2020) The role of air pollution (PM and NO2) in COVID-19 spread and lethality: a systematic review. Environ Res 191:110129. https://doi.org/10.1016/j.envres.2020.110129
Correa-Araneda F, Ulloa-Yáñez A, Núñez D, Boyero L, Tonin AM, Cornejo A, Urbina MA, Díaz ME, Figueroa-Muñoz G, Esse C (2021) Environmental determinants of COVID-19 transmission across a wide climatic gradient in Chile. Sci Rep 11:1–8. https://doi.org/10.1038/s41598-021-89213-4
Cucinotta D, Vanelli M (2020) WHO declares COVID-19 a pandemic. Acta Biomed 91:157–160
Cui Y, Zhang ZF, Froines J, Zhao J, Wang H, Yu SZ, Detels R (2003) Air pollution and case fatality of SARS in the People’s Republic of China: an ecologic study. Environ Heal A Glob Access Sci Source 2:1–5. https://doi.org/10.1186/1476-069X-2-1
de Kok TMCM, Driece HAL, Hogervorst JGF, Briedé JJ (2006) Toxicological assessment of ambient and traffic-related particulate matter: a review of recent studies. Mutat Res Rev Mutat Res 613:103–122. https://doi.org/10.1016/j.mrrev.2006.07.001
Díaz J, Antonio-López-Bueno J, Culqui D, Asensio C, Sánchez-Martínez G, Linares C (2021) Does exposure to noise pollution influence the incidence and severity of COVID-19? Environ Res. https://doi.org/10.1016/j.envres.2021.110766
Grange SK, Farren NJ, Vaughan AR, Rose RA, Carslaw DC (2019) Strong temperature dependence for light-duty diesel vehicle NOx emissions. Environ Sci Technol 53:6587–6596. https://doi.org/10.1021/acs.est.9b01024
Iribarne JV, Cho H-R (1980) Atmospheric thermodynamics and vertical stability. In: Iribarne JV, Cho H-R (eds) Atmospheric physics. Springer Netherlands, pp 79–96. https://doi.org/10.1007/978-94-009-8952-8_4
Isaia G, Diémoz H, Maluta F, Fountoulakis I, Ceccon D, di Sarra A, Facta S, Fedele F, Lorenzetto G, Siani AM, Isaia G (2021) Does solar ultraviolet radiation play a role in COVID-19 infection and deaths? An environmental ecological study in Italy. Sci Total Environ. https://doi.org/10.1016/j.scitotenv.2020.143757
Islam ARMT, Hasanuzzaman M, Azad MAK, Salam R, Toshi FZ, Khan MSI, Alam GMM, Ibrahim SM (2021a) Effect of meteorological factors on COVID-19 cases in Bangladesh. Environ Dev Sustain 23:9139–9162. https://doi.org/10.1007/s10668-020-01016-1
Islam N, Bukhari Q, Jameel Y, Shabnam S, Erzurumluoglu AM, Siddique MA, Massaro JM, D’Agostino RB (2021b) COVID-19 and climatic factors: a global analysis. Environ Res 193:110355. https://doi.org/10.1016/j.envres.2020.110355
Kampa M, Castanas E (2008) Human health effects of air pollution. Environ Pollut 151:362–367. https://doi.org/10.1016/j.envpol.2007.06.012
Kim D, Chen Z, Zhou L-F, Huang S-X (2018) Air pollutants and early origins of respiratory diseases. Chronic Dis Transl Med 4:75–94. https://doi.org/10.1016/j.cdtm.2018.03.003
Lamas-Barreiro JM, Alonso-Suárez M, Fernández-Martín JJ, Saavedra-Alonso JA (2020) Supresión de angiotensina II en la infección por el virus SARS-CoV-2: una propuesta terapéutica. Nefrologia 40:213–216. https://doi.org/10.1016/j.nefro.2020.04.006
Linares C, Culqui D, Belda F, López-Bueno JA, Luna Y, Sánchez-Martínez G, Hervella B, Díaz J (2021) Impact of environmental factors and Sahara dust intrusions on incidence and severity of COVID-19 disease in Spain. Effect in the first and second pandemic waves. Environ Sci Pollut Res 28(37):51948–51960. https://doi.org/10.1007/s11356-021-14228-3
Liu J, Zhou J, Yao J, Zhang X, Li L, Xu X, He X, Wang B, Fu S, Niu T, Yan J, Shi Y, Ren X, Niu J, Zhu W, Li S, Luo B, Zhang K (2020) Impact of meteorological factors on the COVID-19 transmission: a multi-city study in China. Sci Total Environ 726:138513. https://doi.org/10.1016/j.scitotenv.2020.138513
Logan JA (1985) Tropospheric ozone: seasonal behavior, trends, and anthropogenic influence. J Geophys Res 90:463–482
Manan NA, Aizuddin AN, Hod R (2018) Effect of air pollution and hospital admission: a systematic review. Ann Glob Heal 84(4):670. https://doi.org/10.29024/aogh.2376
Marquès M, Rovira J, Nadal M, Domingo JL (2021) Effects of air pollution on the potential transmission and mortality of COVID-19: a preliminary case-study in Tarragona Province (Catalonia, Spain). Environ Res 192:110315. https://doi.org/10.1016/j.envres.2020.110315
Mecenas P, da Rosa Moreira Bastos RT, Rosário Vallinoto AC, Normando D (2020) Effects of temperature and humidity on the spread of COVID-19: a systematic review. PLoS ONE 15:1–21. https://doi.org/10.1371/journal.pone.0238339
Paoletti E, De Marco A, Beddows DCS, Harrison RM, Manning WJ (2014) Ozone levels in European and USA cities are increasing more than at rural sites, while peak values are decreasing. Environ Pollut 192:295–299. https://doi.org/10.1016/j.envpol.2014.04.040
Querol X, Alastuey A, Viana MM, Rodriguez S, Artiñano B, Salvador P, Garcia Do Santos S, Fernandez Patier R, Ruiz CR, De La Rosa J, De La Campa AS, Menendez M, Gil JI (2004) Speciation and origin of PM10 and PM2.5 in Spain. J Aerosol Sci 35:1151–1172. https://doi.org/10.1016/j.jaerosci.2004.04.002
Quesada JA, Gutiérrez F (2021) Período de incubación de la COVID-19: revisión sistemática y metaanálisis. Rev Clínica Española 221:109–117. https://doi.org/10.1016/j.rce.2020.08.005
Radakovic B, Krope T (2007) The effect of ambient air pollution on human health. Proc. 2nd Iasme/Wseas Int. Conf. Energy Environ. 254+
Şahin M (2020) Impact of weather on COVID-19 pandemic in Turkey. Sci Total Environ. https://doi.org/10.1016/j.scitotenv.2020.138810
Sajadi MM, Sajadi MM, Habibzadeh P, Vintzileos A, Shokouhi S, Miralles-Wilhelm F, Miralles-Wilhelm F, Amoroso A, Amoroso A (2020) Temperature, humidity, and latitude analysis to estimate potential spread and seasonality of coronavirus disease 2019 (COVID-19). JAMA Netw Open 3:1–11. https://doi.org/10.1001/jamanetworkopen.2020.11834
Setti L, Passarini F, De Gennaro G, Barbieri P, Licen S, Perrone MG, Piazzalunga A, Borelli M, Palmisani J, Gilio DI, A., Rizzo, E., Colao, A., Piscitelli, P., Miani, A., (2020) Potential role of particulate matter in the spreading of COVID-19 in Northern Italy: first observational study based on initial epidemic diffusion. BMJ Open 10:1–9. https://doi.org/10.1136/bmjopen-2020-039338
Stansfeld SA, Matheson MP (2003) Noise pollution: non-auditory effects on health. Br Med Bull 68:243–257. https://doi.org/10.1093/bmb/ldg033
Tang JW (2009) The effect of environmental parameters on the survival of airborne infectious agents. J R Soc Interface. https://doi.org/10.1098/rsif.2009.0227.focus
To T, Zhang K, Maguire B, Terebessy E, Fong I, Parikh S, Zhu J (2021) Correlation of ambient temperature and COVID-19 incidence in Canada. Sci Total Environ. https://doi.org/10.1016/j.scitotenv.2020.141484
Travaglio M, Yu Y, Popovic R, Selley L, Leal NS, Martins LM (2021) Links between air pollution and COVID-19 in England. Environ Pollut 268:115859. https://doi.org/10.1016/j.envpol.2020.115859
Ujiie M, Tsuzuki S, Ohmagari N (2020) Effect of temperature on the infectivity of COVID-19. Int J Infect Dis 95:301–303. https://doi.org/10.1016/j.ijid.2020.04.068
Vokó Z, Pitter JG (2020) The effect of social distance measures on COVID-19 epidemics in Europe: an interrupted time series analysis. GeroScience 42:1075–1082. https://doi.org/10.1007/s11357-020-00205-0
WHO (2020) Virtual press conference on COVID-19 11 March 2020. World Health Organization
Xie J, Zhu Y (2020) Association between ambient temperature and COVID-19 infection in 122 cities from China. Sci Total Environ. https://doi.org/10.1016/j.scitotenv.2020.138201
Yin H, Sun T, Yao L, Jiao Y, Ma L, Lin L, Graff JC, Aleya L, Postlethwaite A, Gu W, Chen H (2021) Association between population density and infection rate suggests the importance of social distancing and travel restriction in reducing the COVID-19 pandemic. Environ Sci Pollut Res. https://doi.org/10.1007/s11356-021-12364-4
Zhu Y, Xie J, Huang F, Cao L (2020) Association between short-term exposure to air pollution and COVID-19 infection: evidence from China. Sci Total Environ 727:138704. https://doi.org/10.1016/j.scitotenv.2020.138704
Zoran MA, Savastru RS, Savastru DM, Tautan MN (2020) Assessing the relationship between ground levels of ozone (O3) and nitrogen dioxide (NO2) with coronavirus (COVID-19) in Milan. Italy Sci Total Environ 740:140005. https://doi.org/10.1016/j.scitotenv.2020.140005
Funding
This study has been carried out with funding from the Instituto de Salud Carlos III (ISCIII) through the ENPY 221/20 project Granted to Julio Díaz and Cristina Linares.
Author information
Authors and Affiliations
Contributions
Conceptualization: JD, CL; Methodology: JD, CL; Software: JB, AB; Supervision: JD, CL, DRC. Data curation: DRC, AB, JB; Writing-Original draft preparation: JB, DRC; Writing-Reviewing and Editing: JB, DRC. Visualization: JAL; MAN; GS-M; Y L; BH; FB; Investigation: JAL; MAN; GS-M; YL; BH; FB; Software: JAL; MAN; Validation: JAL; MAN.
Corresponding author
Ethics declarations
Conflict of interest
The researchers declare that they have no competing interest within the last 3 years of beginning the work (conducting the research and preparing the work for submission). Furthermore, the authors have no competing interests to declare that are relevant to the content of this article.
Consent to participate
This study used anonymous aggregated data; therefore, there are no individual data, and the consent to participate is not applicable.
Consent to publication
This study used anonymous aggregated data; therefore, there are no individual data, and the consent to publish is not applicable.
Ethical approval
This manuscript should not be submitted to more than one journal at the same time for consideration. This submitted work should be original and should not have been published elsewhere in any form or language (partially or in full) unless the new work concerns an expansion of previous work. This study does not contain any studies with human participants or animals performed by any of the authors. This study used anonymous aggregated data, and therefore, it was not necessary to obtain ethics committee approval. The provisions of the Helsinki Declaration were followed.
Additional information
Editorial responsibility: Samareh Mirkia.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Bañuelos Gimeno, J., Blanco, A., Díaz, J. et al. Air pollution and meteorological variables’ effects on COVID-19 first and second waves in Spain. Int. J. Environ. Sci. Technol. 20, 2869–2882 (2023). https://doi.org/10.1007/s13762-022-04190-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13762-022-04190-z