
Abstract
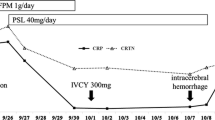
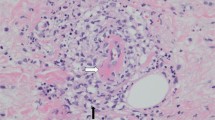
Microscopic polyangiitis (MPA) is a type of necrotizing vasculitis associated with high levels of myeloperoxidase-specific antineutrophil cytoplasmic antibody (MPO-ANCA). While generally associated with renal dysfunction, MPA can also cause intraabdominal hemorrhage in rare cases. A 66-year-old man was admitted to our hospital for renal dysfunction, numbness, and weight loss for 3 months. He had no significant medical history. Renal biopsy revealed crescentic glomerulonephritis with necrotizing vasculitis, which was associated with a high serum titer of MPO-ANCA, leading to a diagnosis of MPA. Remission-induction treatment with glucocorticoids and rituximab was initiated, which improved the patient’s general condition and renal failure. His blood pressure was elevated and was controlled by amlodipine treatment. Two months after discharge, he visited the emergency department because of chest pain. A diagnosis of acute cardiovascular syndrome was suggested; however, his cardiac artery was not stenotic. The patient’s blood pressure was high despite antihypertensive therapy, and he developed posterior reversible encephalopathy syndrome (PRES). Despite intensive treatment, the patient died 3 days later. An autopsy revealed that the cause of death was hypovolemic shock due to massive intra-abdominal hemorrhage from the ruptured mesenteric artery involved in vasculitis. In cases of MPA with sudden-onset chest or abdominal pain, a ruptured intra-abdominal artery should be considered. Secondary hypertension associated with vasculitis should be carefully managed to prevent hemorrhagic complications and PRES.







Similar content being viewed by others

Availability of data and materials
The dataset supporting the findings and conclusions of this case report is included in this article.
References
Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, Flores-Suarez LF, Gross WL, Guillevin L, Hagen EC, Hoffman GS, Jayne DR, Kallenberg CG, Lamprecht P, Langford CA, Luqmani RA, Mahr AD, Matteson EL, Merkel PA, Ozen S, Pusey CD, Rasmussen N, Rees AJ, Scott DG, Specks U, Stone JH, Takahashi K, Watts RA. 2012 revised International Chapel Hill consensus conference nomenclature of vasculitides. Arthritis Rheum. 2013;65:1–11.
Kurata A, Nishimura Y, Yamato T, Arimura Y, Yamada A, Sakamoto A, Fujioka Y. Systemic granulomatous necrotizing vasculitis in a MPO-ANCA-positive patient. Pathol Int. 2004;54:636–40.
Ravanan R, Weale AR, Lear PA, Thornton MJ, Kamel D, Tomson CR. Hemoperitoneum in a patient with ANCA-associated polyangiitis syndrome. Am J Kidney Dis. 2004;44:908–11.
Hayashi Y, Sugawara H, Otsuka M, Yamada S, Tabei K, Ueki A. Fatal hemoperitoneum preceded by cranial hypertrophic pachymeningitis in a patient with ANCA-positive microscopic polyangiitis. Intern Med. 2008;47:1061–3.
Yahata K, Okamoto C, Imamaki H, Seta K, Terashima T, Minamiguchi S, Sugawara A. Fatal hemoperitoneum due to rupture of the left gastric artery in a patient with microscopic polyangiitis. Clin Exp Nephrol. 2009;13:512–7.
Cheung CK, Tan J, Lowe RA, Gouldesbrough D, Stoves J. ANCA-associated vasculitis complicated by haemoperitoneum. NDT Plus. 2010;3:142–4.
Ito Y, Tanaka A, Sugiura Y, Sezaki R. An autopsy case of intraabdominal hemorrhage in microscopic polyangiitis. Intern Med. 2011;50:1501–2.
Fanaroff AC, Rymer JA, Goldstein SA, Simel DL, Newby LK. Does this patient with chest pain have acute coronary syndrome? the rational clinical examination systematic review. JAMA. 2015;314:1955–65.
Yamasaki T, Fass R. Noncardiac chest pain: diagnosis and management. Curr Opin Gastroenterol. 2017;33:293–300.
Zhu Q, Liu S, Heizhati M, Yao X, Wang M, Luo Q, Wang L, Zhang D, Chang G, Li N. Systemic vasculitis: an important and underestimated cause of malignant hypertension. CVIA. 2019;4:99–108.
Sada KE, Ohashi K, Asano Y, Hayashi K, Morishita M, Watanabe H, Matsumoto Y, Fujimoto S, Takasaki Y, Yamagata K, Banno S, Dobashi H, Amano K, Harigai M, Arimura Y, Makino H, Japan Research Committee of the Ministry of Health, Labour, and Welfare for Intractable Vasculitis (JPVAS) and the Research Committee of Intractable Renal Disease of the Ministry of Health, Labour, and Welfare of Japan. Treatment-related damage in elderly-onset ANCA-associated vasculitis: safety outcome analysis of two nationwide prospective cohort studies. Arthritis Res Ther. 2020;22:236.
Hinchey J, Chaves C, Appignani B, Breen J, Pao L, Wang A, Pessin MS, Lamy C, Mas JL, Caplan LR. A reversible posterior leukoencephalopathy syndrome. N Engl J Med. 1996;334:494–500.
Fuentes AG, Komarla A, Gomez JI. Posterior reversible encephalopathy syndrome in a patient with ANCA-associated vasculitis. Rheumatol Int. 2012;32:2529–30.
Patel UV, Patel NJ. Posterior reversible leukoencephalopathy syndrome as a presenting manifestation of p-ANCA-associated vasculitis. BMJ Case Rep. 2014. https://doi.org/10.1136/bcr-2013-202022.
Tajima Y, Matsumoto A. Reversible posterior leukoencephalopathy syndrome in p-ANCA-associated vasculitis. Intern Med. 2006;45:1169–71.
Acknowledgements
We would like to thank all members of our department of Kenwakai Otemachi Hospital for their helpful comments and general support. We are also grateful to Editage for editing the draft of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
Ethical approval
All of the treatment and the examination followed the guideline laid down in the Declaration of Helsinki.
Informed consent
Informed consent was obtained from the patient’s family in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Nawata, A., Nakamura, A., Taba, M. et al. Fatal hemoperitoneum due to rupture of mesenteric artery in remission state of microscopic polyangiitis, concomitant with severe hypertension and posterior reversible encephalopathy syndrome: an autopsy case report. CEN Case Rep 10, 549–558 (2021). https://doi.org/10.1007/s13730-021-00606-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13730-021-00606-w