
Abstract
Overweight and obesity are common and important causes of chronic disease. This should mean that primary care physicians feel tackling obesity is important, but it is uncommon for them to do so. Physicians perceive that this is not their job; they fear offending their patients and are unclear what may be effective. In this review we found two systematic reviews showing that motivational interviewing can lead to effective weight loss but it may not be practicable in this setting. Two trials show referral to specially trained nurses in primary care appears ineffective. Several randomized trials show referral to commercial weight management companies is effective. Observational data but no trials suggest that screening for and opportunistic brief interventions may motivate attempts to lose weight and lead to some weight loss. We conclude there is insufficient evidence to promote treatment opportunistically but sufficient evidence to refer patients wanting to lose weight to commercial weight management services.
Similar content being viewed by others


Introduction
Overweight and obesity are important causes of disease in most countries of the world, with excess body weight contributing toward 44 % of the global burden of diabetes, 23 % of ischemic heart disease burden, and 7–41 % of certain cancer burdens, as well as other medical conditions [1]. Research shows that weight loss is associated with significant improvements in health outcomes, such as reduced mortality, improved lung function, reduced blood pressure and improved lipid profiles [2]. Even modest weight loss (i.e., 5–10 % of initial weight) through lifestyle changes has been linked with a 58 % reduction of type 2 diabetes over four years amongst overweight adults with impaired glucose tolerance [3], with benefits still identifiable after ten years, despite weight regain [4]. Similar findings were also reported in the Finnish Diabetes Prevention Study [5, 6]. Whilst these weight loss programs have been successfully implemented at moderate scale in a research context [5], they tend to involve in-depth counseling or support to change diet and physical activity behaviors and a high level of contact with a specialist over an extended period of time. There is some evidence that the effectiveness of such interventions do not necessarily translate to a routine primary care setting [7].
Not only is obesity a major risk factor for disease, it is also common worldwide; rates in the UK are amongst the highest, only exceeded by the USA. It is estimated that by 2050 the majority of the UK’s population will be obese [8]. This means it is common for primary care physicians to see patients in whom obesity has not yet caused disease as well as those patients where obesity has been a contributing factor to their disease. For example, over 80 % of the UK’s population visits their general practice annually [9], and, on average, patients have five-and-a-half consultations within the year [10]. In England, a physician with a patient list of 2000 adults will typically have 520 (26 %) patients who are obese (BMI ≥30 kg/m2), and 840 men and 640 women (42 % and 32 %, respectively) who are overweight (BMI 25.0–29.9 kg/m2) [11] and who may benefit from weight loss interventions. Many more of the patients seen in primary care will be gaining weight and at high risk of subsequent obesity and so there are also opportunities for the primary prevention of weight gain in this setting.
Preventative medicine is a normal part of the physician’s workload [12]. Most vaccines are delivered by primary care teams. Hypertension screening, diagnosis, and management are delivered mainly by primary care teams. It is common for physicians to identify smokers and make brief interventions to motivate cessation and provide or refer to services offering medication and behavioral counseling to support cessation. Thus it appears that there is a prima facie case for primary care teams to help manage obesity and to prevent the diseases that might occur or treat the complications of obesity through weight loss. What may seem surprising though, is that physician involvement in weight loss is uncommon.
In the UK, Michie investigated 40 physicians’ and 47 nurses’ communication about weight with their overweight and obese patients [13]. When there was no identified medical problem, only 38 % of physicians and 14 % of nurses reported raising the issue on less than 50 % of occasions. When they did raise the issue of overweight, only 9 % offered some form of support to help lose weight. Furthermore, Noordman and colleagues explored the frequency of physicians discussing lifestyles choices with their patients [14]. Analysis of video recordings from a random sample of 6203 medical consultations between 1975 and 2008 in Dutch primary care practices revealed that overall, physicians only discussed obesity related issues, such as nutrition and physical activity in 10.3 % and 13.2 % of consultations, respectively. These data demonstrate the limited frequency of physicians discussing weight management with patients in primary care.
Why do physicians intervene so seldom in relation to the opportunity to do so? Physicians perceive there to be several practical obstacles to effective weight management including: a lack of time during consultations [15]; a lack of knowledge, including uncertainty about the best ways to assist and limited confidence in their ability to address weight management [16, 17]; negative attitudes about obesity linked to a belief that patients, and not physicians, have the onus to act first [18]; and fear of offending patients by raising or discussing the issue of excess weight [13]. Physicians commonly believe that obesity is best addressed through societal interventions to prevent weight gain or when patients take greater personal responsibility for weight control, implying that these may be more important than action in primary care [19].
In addition, whatever physicians might do has to be fitted into routine consultations, typically only 10 minutes long in primary care practice. There are two key questions: first, what can be done for patients who ask their physicians for support to lose weight, and, second, is there sufficient evidence to justify screening for and proactively identifying and managing obesity? Much more evidence is required for the second, but it would mean placing obesity on the physicians’ agenda in the same way that hypertension is, where physicians offer and are often managed to screen for and intervene to detect hypertension. We therefore examine the literature to identify evidence of the suitability, practicability, and effectiveness of different approaches to weight management for overweight and/or obese adults presenting in primary care.
Approaches to Weight Management in Primary Care
In other aspects of health promotion, time constraints are overcome by delivering brief interventions. Brief interventions are usually opportunistic and delivered during a consultation about something else and where the practitioner takes the opportunity to raise a topic that is either unrelated to or not directly the topic of the current consultation [20]. They take only a few minutes. In practice, the term is used interchangeably with brief behavioral counseling, sometimes with multiple sessions, which are obviously scheduled and where behavior change is directly the topic of the consultation. Brief interventions originated from addiction-based research and reviews demonstrate their effectiveness in reducing problem drinking and motivating smoking cessation [21, 22]. These reviews demonstrate that genuinely brief (1 minute), opportunistic interventions can motivate some patients consulting for reasons unrelated to the behavior to either reduce their alcohol consumption or stop smoking.
Accordingly we consider whether brief interventions can be effective for weight management in primary care by reviewing evidence [20, 23] considering data on current practice and the views of physicians [13, 16, 17, 24, 25] and identify five brief interventions.
Brief Advice
Brief advice, delivered in a single session, is often aimed at increasing awareness of health risks and is the physician’s preferred intervention, rather than delivering a high-intensive intervention specifically targeting physical activity or dietary habits, goal setting or prescribing weight loss medication [13, 17, 26]. Survey data suggests that advice to lose weight by a physician is strongly associated with future weight loss ‘attempts’ for overweight and obese patients [25, 27]. In 1996, the US Behavioral Risk Factor Surveillance System found that 42 % of obese patients reported that their physician had ‘ever’ advised them to lose weight [24, 25] and people who received advice were more likely to have tried to do so (odds ratio [OR] 2.79 [2.53–3.08]). Rose and colleagues recently conducted a systematic review and meta-analysis of survey data examining physician-provided advice and its association with changes in patient weight loss behavior [28•]. The type of advice given included; general advice to lose weight, specific advice related to weight loss, information or communication regarding overweight and the use of motivational interviewing to promote weight loss. The odds ratio for the association between physician intervention and an attempt to lose weight was 3.85 (95 % CI 2.71, 5.49; p < 0.01). Two studies suggested that people who received some kind of advice lost about 1–2 kg more than people who did not. Five other studies suggested that weight loss was more common in those who did receive an intervention. These survey data suggest that a brief advice-orientated intervention, which could easily be delivered by physicians, may motivate weight loss. However, the data are all observational. It is possible that the association arises because patients who are thinking of losing weight discuss this with their physicians. There is evidence that conversations about exercise and nutrition are more frequently initiated by patients than by physicians [14], so these data are weak evidence for causality. We sought more robust evidence of effectiveness from randomized trials, however no such evidence was found.
Accordingly, while there is evidence that physician-provided advice can have positive influences on weight loss-related behaviors, there was variation between studies in the type of advice given (e.g., general advice to lose weight vs. specific advice about weight loss). This makes it difficult to develop guidance for effective advice.
Motivational Interviewing
Motivational interviewing is a collaborative, person-centered form of guiding to elicit and strengthen motivation for change, and it incorporates three key elements: ‘collaboration’ between the patient and physician; ‘evoking or drawing out’ the patient’s thoughts about behavior change; and encouraging the patient’s ‘autonomy’ [29]. To engage and deliver motivational interviewing competently, physicians require specialist skills and expertise, usually involving training that follows a sequence of eight stages and takes at least two days, plus on-going supervision and follow-up training. Additional time may be required if the physician is not familiar with the health topic in hand [20].
Rubak and colleagues conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) using motivational interviewing as the intervention compared to a control condition for a wide-range of health conditions [30]. The meta-analysis included six trials of motivational interviewing versus control for weight management. The mean change in BMI was −0.72 (0.33 to 1.11) kg/m2, which we calculated is approximately 2 kg difference. The median follow-up for all studies in the review was 12 months. Across all behavioral areas, they reported that studies that compared 15 minutes of motivational interviewing to control were less likely to show statistically significant differences than studies that compared 60 minutes of counseling to a control. A more recent systematic review of RCTs investigated the effectiveness of motivational interviewing versus control in overweight or obese adults (n = 1448) [31•]. Follow-up ranged from 3–18 months. In the nine interventions tested in eight trials with weight change as the outcome, the mean reduction in weight was −1.47 kg [95 % CI −2.05, −0.88) kg. The data in Rubak et al. [30] and Armstrong et al. [31•] do not report whether or how participants who were lost to follow up were included in the analysis. A recent RCT compared the effectiveness of delivering standard exercise and nutritional information plus up to five face-to-face motivational interviewing sessions over a six-month period (intervention), with the provision of standard information only in a single session (control) in adults with more than one cardiovascular risk factor, including excess weight [32••]. At six months the difference in mean change in weight was −0.75 kg and at 18 months was −0.81 kg, neither difference was significant.
This evidence indicates that while motivational interviewing can be effective for weight loss, in the short term (≤6 months), the application of this approach by a generalist physician on a large scale seems doubtful given the amount of time required for training and delivery (≥15 minutes, with multiple sessions). This may explain why motivational interviewing techniques are not widely implemented as opportunistic interventions in a primary care setting.
Primary Care-led (In-house) Weight Management Services
In many instances, physicians may advise overweight and/or obese patients to see non-specialist healthcare professionals, such as nurses or healthcare assistants, on a one-to-one basis at the practice to review their weight and deliver behavioral weight management. This takes a small amount of physician’s time, yet provides patients with help to lose weight, rather than just advice to do so.
In many cases, nurses in the UK offer an ad hoc program with little training. However, there are national organizations that offer a program and training to deliver it. The Counterweight program offers a structured behavioral program to help patients achieve a 5–10 % weight loss (5–10 kg) by providing them with skills to change unhealthy eating and activity behaviors. Patients meet with practice nurses, either on a one-to-one basis (10–30 minutes per session), or in groups (60 minutes per session), for nine sessions over a year. A recent evaluation of 1906 patients (mean BMI 37 kg/m2), using baseline observation carried forward (BOCF), reported that mean weight loss at one year was 1.3 kg, with 30.7 % of patients achieving ≥5 % weight loss [33]. There are no randomized trials of the Counterweight program to show whether this is more than might have been achieved if patients tried to lose weight without such support.
Two recent RCTs suggest that training healthcare assistants and/or nurses to deliver support programs has limited effectiveness. The CAMWEL study randomized 381 overweight adults (BMI ≥25 kg/m2) to either a structured one-to-one lifestyle program for weight loss delivered over 14 session (30 minutes each) in a year by healthcare assistants in general practice, or usual care [34••]. At one year, using BOCF, weight losses were small in the intervention group (1.4 kg) and not significantly different to the control treatment (0.8 kg), though more patients lost ≥5 % baseline weight (32.7 % in the structured program vs. 20.4 % in the usual care group). Similarly, in the Lighten Up trial, 740 obese adults (≥30 kg/m2, 18+ years) were randomized to minimal control or one of six interventions (12 week programs), two of which were either physician- or pharmacist-led care [35, 36••]. Dietitians trained physicians and pharmacists in weight management. Using intention to treat (ITT) analysis, physician and pharmacy care achieved similar and small weight loss to the minimal control (1.0 kg at one year). Only 14.3 %, 15.7 % and 17 % of patients in the pharmacy, physician and minimal control arms respectively, achieved ≥5 % weight loss at one year. Data on this type of service are limited and there is probably considerable heterogeneity in the services offered by in-house primary care teams. However the failure of these two well-planned programs to give better weight loss than control means that such interventions cannot be recommended in general.
Referral to Commercial Weight Management Services
There is evidence from trials and routine practice of the effectiveness of commercial providers in delivering weight management services [37]. Most of this is based on self-referrals, but there is growing interest in establishing partnerships between physicians and commercial weight management services analogous to those offered in other areas of health promotion.
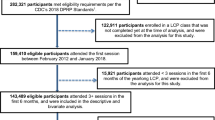
Group-based behavioral programs for weight loss are often provided close to people’s homes and run throughout the day and evening. Weight Watchers is available in many countries of the world and has been investigated in trials, as have two UK services that operate in broadly similar ways, namely Slimming World and Rosemary Conley. The groups are led by lay people almost all of whom have lost weight using the service. They receive some training and deliver a programed course developed by specialists. Data from two trials of partnerships between the commercial sector and primary care suggest this is a promising approach. In the Lighten Up trial, 740 obese adults (≥30 kg/m2, 18+ years) were randomized to 12 week programs of a minimal control or one of six interventions, three of which were UK-based commercial weight management services- Weight Watchers, Slimming World, Rosemary Conley [35, 36••]. Using BOCF ITT analysis, mean weight loss at one year for those receiving Weight Watchers, Slimming World and Rosemary Conley was 2.5 (±6.2) kg compared to 0.8 (±0.8) kg for primary care-led programs. Likewise, Jebb and colleagues randomized 772 participants (≥30 kg/m2, 18+ years) to 12 months of Weight Watchers or physician care [38••]; at one year those randomized to receive Weight Watchers achieved a weight loss of 4.0 kg and those to physician care lost 1.6 kg. Other trials in the UK [39] and the USA [40] also show similar amounts of weight loss through attending these group-based commercial weight management services. A systematic review and meta-analysis of commercial weight management programs that do not provide meal replacements showed that participants using these programs lost 2.27 kg (95 % CI −2.81, −1.73) more than controls at one year using BOCF ITT analysis (Fig. 1) [41•]. These kinds of services are finding their place in health service provision. In England, for example, over two thirds of primary care trusts (PCTs) currently contract with the commercial weight management services described above, costing PCTs about £50 per patient to provide a free (to the patient) 12-week treatment course ‘on prescription’. Observational data from these referral schemes supports the effectiveness of partnerships between primary care and commercial weight management services [42, 43]. In an independent audit of the NHS Weight Watchers referral scheme median weight change for all referrals (n = 29,326 overweight and obese adults) was −2.8 kg [IQR −5.9– −0.7 kg] and 33 % of all courses resulted in loss of ≥5 % initial weight. Of those who completed all 12 sessions of a first recorded referral course (n = 11,851) median weight change was −5.4 kg [IQR −7.8– −3.1 kg] and 57 % lost ≥ 5 % initial weight [42]. Similarly, in an evaluation of 34,271 patients referred to a Slimming World group for 12 weeks, mean weight change for all referrals was −4.0 kg (SD 3.7 kg) and 35.8 % lost ≥5 % initial weight [43]. Of the 19,907 patients who attended ten or more of the 12 sessions, mean weight change was −5.5 kg (SD 3.8 kg) and 54.7 % lost 5 % initial weight [43].

Weight changes at 12 months: commercial weight management services versus control
Referral to commercial weight management services may overcome some of the perceived obstacles for physicians to offer weight management interventions. Firstly, evidence from trials show that commercial weight management services are an effective way for patients to lose weight, and that they can be easily implemented via primary care [35, 36••, 38••]. Thus, with minimal training physicians could be educated about effective strategies and confidently offer effective treatments to their patients. Secondly, referring patients to commercial weight management services would only take physicians less than a minute, and does not require specialist in-depth knowledge and skills to deliver. Furthermore, in contrast to motivational interviewing interventions or most other services delivered within primary care, referral to commercial weight management services such as those presented here, would provide patients with regular (weekly) group-based sessions lasting ≥60 minutes, delivered by dedicated weight management consultants; elements that have been identified as important requirements for long-term behavior change [30, 44]. Finally, these services are already operating at a meaningful scale and with relatively low costs compared to services delivered by health professionals.
There is some evidence that referral to commercial weight management services is acceptable to patients. Ahern and colleagues interviewed 16 female participants in a research trial comparing standard care within a practice with referral to a commercial weight management service to explore their accounts of weight loss interventions to identify possible reasons why those who attended a commercial weight management service achieved greater weight loss [45]. They reported that people who did not require specialist clinical care, wanted support and motivation to lose weight rather than education and as such, found referral to the commercial weight management services very fitting. This study also suggested that many, though not all patients favored referral to external services. Those people perceived that primary care did not offer appointments at convenient times (e.g., evenings and weekends) and offered only infrequent support.
These data indicate that referring people who ask for help to commercial weight management services is an effective and practicable approach for primary care physicians.
Weight Loss Medication
When purely behavioral approaches to weight management in primary care have not resulted in weight loss despite commitment from the patient, it is reasonable for physicians to consider pharmacotherapy, which forms part of the national guidelines (e.g., [46–48]). A meta-analysis of primary care relevant trials looked at the evidence that orlistat (currently the only drug licensed specifically for weight loss in the UK) can increase weight loss in the context of a group behavioral treatment [49•]. In 12 trials that could be combined for meta-analysis (n = 5910), participants randomly assigned to orlistat (plus behavioral treatment) lost 3.0 kg more (95 % CI −3.9, −2.0 kg) at one year than those who received a placebo. The authors also found that metformin led to a 1.5 kg greater weight-loss than placebo, though metformin is not licensed for use in this way. The combination of pharmacotherapy and behavioral support is important. Wadden and colleagues showed that combining both medication and lifestyle modification resulted in more weight loss (mean [SD] 12.1 [+/−9.8] kg) than pharmacotherapy (sibutramine) (5.0 [+/−7.4] kg) or lifestyle modification alone (6.7 [+/−7.9] kg) [50]. Obesity treatment guidelines therefore encourage physicians to only prescribe weight-loss medications alongside behavioral interventions (e.g., [46–48]).
Conclusion
There is reasonable evidence that motivational interviewing addressing why patients might change their behavior can result in modest weight loss. Likewise, referral to a commercial weight management service is also effective. There is no strong evidence that training primary care teams to deliver weight management is effective. There is no strong evidence that it is effective for physicians to screen for and offer intervention to people who are not seeking support to lose weight.
Motivational interviewing typically aims to help people resolve ambivalence about whether to act and is not confrontational. This style of counseling means that it is suitable, in that it is unlikely to offend patients. However, it may fail on practicability grounds because the length of time taken to deliver an opportunistic intervention makes it unfeasible in many settings. In addition, the skill requirements for practitioners mean that specialist training is required.
The evidence from observational data suggests that even brief advice to lose weight may trigger weight loss attempts and useful weight loss. This may suggest that screening and opportunistic intervention could be effective, but there is currently no evidence to justify this from robust randomized trials.
One intervention that appears to be suitable, practicable, and effective is referral to commercial weight management services, such as Weight Watchers, Slimming World and Rosemary Conley. For people who ask for help to lose weight this may represent the current best approach. In many cases, the trials have tested interventions that consisted of lengthy or indefinite entitlement to free weight loss support from these programs. In practice, many such programs are limited, typically in the UK to three months. Nonetheless, both trial and observational data suggest such short courses may be effective, though further data would be welcome. However, the widespread availability of such programs in many countries and their acceptance by the population suggests they have an important role to play in supporting primary care to tackle obesity.
Most of the evidence to date relates to patients who are seeking weight management interventions or motivated to take up such an offer. There is insufficiently robust evidence to justify screening and opportunistic interventions for obesity. Given the high prevalence of obesity, a pragmatic approach is to first enhance the provision of support services to patients seeking treatment or with specific obesity-related comorbidities to build experience and confidence in treating obesity in primary care. Meanwhile, more research is needed to expand the range of suitable, practicable, and effective interventions available in primary care and to examine whether screening and opportunistic intervention could have a population level-impact on weight.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
WHO. Global health risks: mortality and burden of disease attributable to selected major risks. Geneva: World Health Organization; 2009.
McTigue KM, Harris R, Hemphill B, et al. Screening and interventions for obesity in adults: summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2003;139:933–49.
Knowler WC, Barrett-Conner E, Fowler, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393–403.
Diabetes Prevention Program Research Group, Knowler WC, Fowler SE, et al. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet. 2009;374:1677–86.
Tuomilehto J, Lindström J, Eriksson J, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001;344:1343–50.
Lindström J, Louheranta A, Mannelin M, et al. The Finnish Diabetes Prevention Study (DPS): lifestyle intervention and 3-year results on diet and physical activity. Diabetes Care. 2003;26:3230–6.
Vermunt PW, Milder IE, Wielaard F, et al. Lifestyle counseling for type 2 diabetes risk reduction in Dutch primary care: results of the APHRODITE study after 0.5 and 1.5 years. Diabetes Care. 2011;34:1919–25.
Foresight. Tackling obesities: future choices – Project report, 2007. www.bis.gov.uk/foresight [accessed 01 April 2013].
Walker A, Maher J, Coulthard M, et al. Living in Britain. Results from the 2000/01 General Household Survey. Office for National Statistics, 2001.
Hippisley-Cox J, Vinogradova Y. Trends in consultation rates in general practice 1995/1996 to 2007/2008: analysis of the QRESEARCH database . NHS Information Centre, 2008. https://catalogue.ic.nhs.uk/publications/primary-care/general-practice/qres-rep-tren-consrate-gene-prac-1995-08/qres-rep-cons-gene-prac-1995-08-1995-08-rep.pdf.
Statistics on Obesity, Physical Activity and Diet: England, 2013; Health and Social Care Information Centre, Lifestyles Statistics, 2013.
Aveyard P, Raw M. Improving smoking cessation approaches at the individual level. Tob Control. 2012;21:252–e257.
Michie S. Talking to primary care patients about weight: a study of GPs and practice nurses in the UK. Psychol Health Med. 2007;12:521–5.
Noordman J, Verhaak P, van Dulmen Noordman S, et al. Discussing patient’s lifestyle choices in the consulting room: analysis of GP-patient consultations between 1975 and 2008. BMC Fam Pract. 2010;11:87.
Simkin-Silverman LR, Conroy MB, King WC. Treatment of overweight an obesity in primary care: current evidence and future directions. Am J Lifestyle Med. 2008;2:296–304.
Huang J, Yu H, Marin E, et al. Physicians' weight loss counseling in two public hospital primary care clinics. Acad Med. 2004;79:156–161.
Leverence RR, Williams RL, Sussman A, et al. Obesity counseling and guidelines in primary care. a qualitative study. Am J Prev Med. 2007;32:334–9.
Gunther S, Gui F, Sinfield P, et al. Barriers and enablers to managing obesity in general practice: a practical approach for use in implementation activities. Qual Prim Care. 2012;20:93–103.
Lawlor DA, Keen S, Neal RD. Can general practitioners influence the nation’s health through a population approach to provision of lifestyle advice? Br J Gen Prac. 2000;50:455–9.
Cavill N, Hillsdon M, Anstiss T. Brief interventions for weight management. Oxford: National Obesity Observatory; 2011.
Stead LF, Bergson G, Lancaster T. Physician advice for smoking cessation. Cochrane Database of Systematic Reviews: Reviews 2008 Issue 2 John Wiley & Sons, Ltd Chichester, UK doi:10.1002/14651858 CD000165 pub3 2008.
Kaner EF, Dickinson HO, Beyer FR, et al. Effectiveness of brief alcohol interventions in primary care settings: a systematic review. Drug Alchol Rev. 2009;28:301–23.
Tsai A, Wadden T. Treatment of obesity in primary care practice in the United States: a systematic review. J Gen Intern Med. 2009;24:1073–9.
Galuska DA, Will JC, Serdula MK, et al. Are health care professionals advising obese patients to lose weight? JAMA. 1999;282:1576–8.
Sciamanna CN, Tate DF, Lang W, et al. Who reports receiving advice to lose weight?: results from a multistate survey. Arch Intern Med. 2000;160:2334–9.
Shiffman S, Sweeney CT, Pillitteri JL, et al. Weight management advice: what do doctors recommend to their patients? Prev Med. 2009;49:482–6.
Mehrotra C, Naimi TS, Serdula M, et al. Arthritis, body mass index, and professional advice to lose weight: implications for clinical medicine and public health. Am J Prev Med. 2004;27:16–21.
• Rose SA, Poynter PS, Anderson JW, et al. Physician weight loss advice and patient weight loss behaviour change: a literature review and meta-analysis of survey data. Int J Obes. 2013;37:118–28. This is a systematic review and meta-analysis of survey data examining physician-provided advice and its association with changes in patient weight loss behaviour.
Miller WR, Rollnick S. Ten things that motivational interviewing is not. Bahv Cogn Psychother. 2009;37:129–40.
Rubak S, Sandbaek A, Lauritzen T, et al. Motivational interviewing: a systematic review and meta-analysis. Brit J Gen Prac. 2005;55:305–12.
• Armstrong MJ, Mottershead TA, Ronksley PE, et al. Motivational interviewing to improve weight loss in overweight and/or obese patients: a systematic review and meta-analysis of randomized controlled trials. IASO. 2011;12:709–23. This is a systematic review of RCTs that investigated the effectiveness of motivational interviewing versus control in overweight or obese adults.
•• Hardcastle SJ, Taylor AH, Bailey MP, et al. Effectiveness of a motivational interviewing intervention on weight loss, physical activity and cardiovascular disease risk factors: a randomised controlled trial with a 12-month post-intervention follow-up. Int J Behav Nutr Phys Act. 2013;10:40. This RCT evaluated the effectiveness of a six-month low-intensity motivational interviewing intervention, and usual care, in a UK primary care setting in maintaining reductions in CVD risk factors at 12 months post-intervention.
Counterweight Project Team. Evaluation of the counterweight programme for obesity management in primary care. Br J Gen Pract. 2008;58:548–54.
•• Nanchahal K, Power T, Holdsworth E, et al. A pragmatic randomised controlled trial in primary care of the Camden Weight Loss (CAMWEL) programme. BMJ Open. 2012;2:e000793. doi:10.1136/bmjopen-2011-000793. This RCT compared the effectiveness of a structured primary care-led weight loss program on weight loss with usual care.
Jolly K, Daley A, Adab P, et al. A randomised controlled trial to compare a range of commercial or primary care led weight reduction programmes with a minimal intervention control for weight loss in obesity: the lighten up trial. BMC Public Health. 2010;10:439.
•• Jolly K, Lewis A, Beach J, et al. Comparison of range of commercial or primary care led weight reduction programmes with minimal intervention control for weight loss in obesity: lighten up randomised controlled trial. BMJ. 2011;343:d6500. doi:10.1136/bmj.d6500. This RCT compared the effectiveness of a range of commercial or primary care led weight reduction program with minimal intervention control for weight loss in obesity.
Tsai AG, Wadden TA. Systematic review: an evaluation of major commercial weight loss programs in the United States. Ann Intern Med. 2005;142:56–66.
•• Jebb SA, Ahern AL, Olson AD, et al. Primary care referral to a commercial provider for weight loss treatment versus standard care: a randomised controlled trial. Lancet. 2011;378:1485–92. This RCT compared the effectiveness of a 12-month referral to Weight Watchers, with standard care, for weight loss.
Truby H, Baic S, de Looy A, et al. Randomised controlled trial of four commercial weight loss programmes in the UK: initial findings from the BBC “diet trials”. BMJ. 2006;332:1309–14.
Heshka S, Anderson JW, Atkinson RL, et al. Weight loss with self-help compared with a structured commercial program: a randomized trial. JAMA. 2003;289:1792–8.
• Hartmann-Boyce J, Johns D, Aveyard P, et al. Managing overweight and obese adults: update review. The clinical effectiveness of long-term weight management schemes for adults (Review 1a). Report to NICE, London, in press. This is a systematic review and meta-analysis of commercial weight management services.
Ahern AL, Olson A, Aston L, et al. Weight watchers on prescription: an observational study of weight change among adults referred to weight watchers by the NHS. BMC Public Health. 2011;11:434.
Stubbs RJ, Pallister C, Whybrow S, et al. Weight outcomes audit for 34,271 adults referred to a primary care/commercial weight management partnership scheme. Obes Facts. 2011;4:113–20.
Carvajal R, Wadden TA, Tsai AG, et al. Managing obesity in primary care practice: a narrative review. Ann N Y Acad Sci. 2013;1281:191–206.
Ahern AL, Boyland EJ, Jebb SA, et al. Participants’ explanatory model of being overweight and their experience of standard care compared with a commercial partnership weight loss intervention. 2013. doi:10.1370/afm.1446.
NICE. NICE Clinical Guidance 43. Obesity: guidance on the prevention, identification, assessment and management of overweight and obesity in adults and children, 2006.
NIH. The practical guide: identification, evaluation, and treatment of overweight and obesity in Adults, 2000. http://www.nhlbi.nih.gov/guidelines/obesity/prctgd_c.pdf, [accessed 1st April 2013].
NHMRC. Clinical practice guidelines for the management of overweight and obesity in adults, 2003. http://www.health.gov.au/internet/main/publishing.nsf/Content/7AF116AFD4E2EE3DCA256F190003B91D/$File/adults.pdf [accessed 1st April 2013].
• LeBlanc ES, O’Connor E, Whitlock, et al. Effectiveness of primary care-relevant treatments for obesity in adults: a systematic evidence review for the U.S. preventive services task force. Ann Intern Med. 2011;155:434–47. This systematic review evaluated the effectiveness and harms of different primary care-relevant treatments for overweight and obese adults.
Wadden TA, Berkowitz RI, Womble LG, et al. Randomized trial of lifestyle modification and pharmacotherapy for obesity. N Engl J Med. 2005;353:2111–20.
Acknowledgments
Amanda L. Lewis has received grant support for 2012–2015: A randomised controlled trial of the effectiveness of brief weight management for obese adults in primary care. 2012–2015. MRC NPRI Phase 4; 2011–2013: Development of a community midwife-led intervention to prevent excessive weight gain in healthy and overweight pregnant women. 2011–2013. National Schools of Primary Care; Weight management in primary care. 2011–2014. National Schools of Primary Care PhD studentship; Development and initial evaluation of attentive eating intervention for weight management in primary care. National Schools of Primary Care; plus National Schools of Primary Care Seedcorn funding.
Susan A. Jebb has received grant support for 2012–2015: ‘An RCT to test the clinical and cost-effectiveness of primary care referral to a commercial weight loss provider’ NPRI; 2012 2013: 'Managing overweight and obese adults: update review ' NICE Review:; 2012–2016: ‘A randomised controlled trial of the effectiveness and cost-effectiveness of a brief weight management intervention for obese adults in primary care’ NPRI; 2012–2015: ‘A randomised controlled trial to test the impact of a fruit and vegetable supplement on endothelial function and cardiovascular risk’ NSA; 2011–2015: ‘Behaviour Health and Research Unit’ Department of Health Policy Research Programme; 2011–2013: ‘Telling ‘good’ population health science from ‘bad’ science’ MRC Population Health Sciences Research Network; 2011–2013: ‘A randomised controlled trial to examine the efficacy of regular weighing and feedback in preventing excess weight gain in pregnant women’ NSPCR; 2009–2014: ‘Centre for Diet and Activity Research’ UKCRC.
Paul Aveyard is funded by the UK Centre for Tobacco Control Studies, a UKCRC Public Health Research: Centre of Excellence. Funding from British Heart Foundation, Cancer Research UK, Economic and Social Research Council, Medical Research Council, and the Department of Health, under the auspices of the UK Clinical Research Collaboration, is gratefully acknowledged. Paul Aveyard has received grant support for 2012–2015: A randomised controlled trial of the effectiveness of brief weight management for obese adults in primary care. 2012–2015. MRC NPRI Phase 4; 2011–2013: Development of a community midwife-led intervention to prevent excessive weight gain in healthy and overweight pregnant women. 2011–2013. National Schools of Primary Care; Weight management in primary care. 2011–2014. National Schools of Primary Care; plus National Schools of Primary Care Seedcorn funding. for 2012-2015: ‘An RCT to test the clinical and cost-effectiveness of primary care referral to a commercial weight loss provider’ NPRI; 2012 2013: ‘Managing overweight and obese adults: update review’ NICE Review.
Compliance with Ethics Guidelines
ᅟ
Conflict of Interest
Amanda L. Lewis is a Postdoctoral Research Fellow for NIHR SPCR; she has also received hospitality from Weight Watchers twice and Slimming World once; and is involved with a publicly funded trial where the treatment courses are donated by Rosemary Conley and Slimming World.
Paul Aveyard has received lunch and dinner courtesy of Weight Watchers twice and Slimming World once.
Susan A. Jebb serves on the advisory board for Tanita Medical; is Head of Diet and Obesity Research for the Medical Research Council; has received payment for lectures including service on speakers bureaus from Rosemary Conley 'Diet and Fitness' Club; has received a fee for nutrition-related articles for Rosemary Conley 'Diet and Fitness' magazine; has received honoraria as Chair of NICE Public Health Advisory Committee.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lewis, A.L., Aveyard, P. & Jebb, S.A. Brief Interventions for Weight Loss in Primary Care. Curr Obes Rep 2, 341–347 (2013). https://doi.org/10.1007/s13679-013-0073-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13679-013-0073-8