
Abstract
Patients diagnosed with Ewing sarcoma family of tumors (ESFT) commonly require multimodality therapy including radiation therapy, in addition to surgery and chemotherapy, to achieve optimal outcomes. In most cases, a specific genetic defect with a translocation t(11:22)(q24;q12) corresponding to fusion between the EWS gene and an ETS proto-oncogene is present. The Intergroup Ewing Sarcoma Studies (IESS) Studies, the CESS studies, and the Euro-Ewing studies, among others, have helped to define the efficacy of chemotherapy agents, as well as the radiation therapy backbone for ESFT used today. The relative effectiveness of surgery, radiation therapy, and combinations of these local control modalities continue to be defined in specific clinical situations and body sites. Important late effects of radiation therapy may include pneumonitis, radiation cystitis, and second malignancy. Promising for the future may be new chemotherapeutic agents, improved radiation techniques including proton radiation therapy, and possibly myeloablative strategies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ewing’s Sarcoma and Primitive Neuroectodermal Tumor of Bone are closely related and may be collectively referred to as Ewing sarcoma family of tumors (ESFT) [1–4]. These cancers differ from other sarcomas in their greater sensitivity to chemotherapy and radiation therapy (RT). Radiotherapy treatment was applied for Ewing’s sarcoma almost from its first description. In the words of James Ewing, “When the diagnosis of endothelial myeloma (ESFT) is suspected the writer believes that the first indication is for treatment by radiation in full doses and over considerable periods. This recommendation is based on the reported cure of certain cases in the Registry by radiation alone, and on the clinical disappearance of the disease for variable periods in many more cases. The response to radiation also confirms the diagnosis” [5]. Of course, after many decades of clinical research, radiation remains a primary treatment for this disorder.
ESFT generally requires multimodality therapy to achieve optimal outcomes. The translocation t(11;22) and its variants are the hallmark of ESFT. Its incidence is estimated at 0.6–3 per 1 million individuals [1, 4]. By using aggressive local control strategies combined with systemic therapy, even some patients with locally advanced and metastatic disease may achieve long-term tumor control. Mainly as a result of multicenter randomized clinical trials, significant advances have been made in the surgical, chemotherapeutic, and radiotherapeutic management of Ewing’s sarcoma. This article will mainly concern itself with the optimal integration of RT in the multimodality therapy of ESFT.
James Ewing was a pathologist interested in radiation and pioneered its use. Ewing reported on “Endothelial Myeloma” in a presentation entitled “Observations on a Malignant Bone Neoplasm” to the New York Pathological Society in 1920 [6]. He noted, “broad sheets of small polyhedral cells with pale cytoplasm, small hyperchromatic nuclei, well defined cell borders and complete absence of inter-cellular material.” Dr. Ewing endeavored to understand the natural history of cancer and opposed extensive surgery when the patient was incurable [5–10]. As a pathologist at the Memorial General Hospital beginning in 1912 (now Memorial Sloan–Kettering Cancer Center), he eventually directed the departments of cancer surgery and RT. He is credited for observing that radiation may be a curative treatment in Ewing sarcoma. He applied radiation physics including the principle of increasing source to skin distance and increasing the energy of the beam [6–10].
Natural history of ESFT
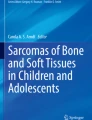
ESFT make up 6–10 % of primary malignant bone tumors with a male/female ratio of 1.5:1 [1–4]. Remarkably, the incidence in African Americans is only 1/14 that for Caucasians. About one-fourth of patients have metastasis at diagnosis. Clinical presentation most commonly involves the diaphysis of long bones (femur, tibia) and the pelvis, but may occur in any location (scapula, rib, vertebral body). Hematogenous metastases including lung (38 %), bone (31 %) and bone marrow (BM) (11 %) are characteristic. Extra-osseous Ewing’s Sarcoma and metastases to liver, peritoneum, and GI tract are not uncommon. In Fig. 1, magnetic resonance imaging (MRI) images of two cases with relatively unusual presentations are shown; these include Ewing’s sarcoma presenting in the skull (Fig. 1a) and in the cervical spine (Fig. 1b).

a Ewing sarcoma involving the skull. A 14-year-old male presented with a mass on the head and a neurosurgical resection revealed Ewing’s sarcoma. Although gross total resection was recorded, the margin was felt to be close and post-operative radiation therapy of 5,040 cGy was delivered. Axial, sagittal, and coronal T1 gadolinium enhanced images are shown. b Cervical Spinal Ewing’s. A 3-year-old girl presented with severe pain and failure to thrive. Workup showed massive cervical spinal tumor with bilateral lung metastases. Sagittal T1 gadolinium enhanced image is shown
ESFT cells are recognized to synthesize acetylcholine transferase and believed to be derived from postganglionic parasympathetic primordial cells. In tissue culture, neural processes, neurosecretory granules, and neurofilament may be observed. In most tumors, translocations t (11; 22) (q24; q12) corresponding to fusions between the EWS gene with an ETS proto-oncogene (FLI1 85 % or ERG 10 %) are present [11–14]. There are also other rare fusion partners. Essentially, the C-terminal portion of the EWS is replaced by the DNA-binding domain of a transcription factor resulting in deregulation of many other genes. Various FLI1 exons may be fused (type 1 = exon 6; type 2 = exon 5). Fusion transcripts can be detected by RT-PCR and FISH. Previous data had suggested a prognostic benefit for non-type 1 fusion [13, 14]. Recent studies from the Children’s Oncology Group (COG) and the Euro-Ewing 99 study demonstrate that ESFT shows similar outcomes regardless of fusion subtype [11, 12, 15].
Clinical treatment trials for ESFT
It was with the addition of chemotherapy to surgery and RT that higher control rates for localized disease were first realized [1–4]. Randomized trials performed in the United States and Europe were instrumental both in proving the effectiveness of multi-modality therapy and in integrating local control measures (i.e., surgery and/or RT) with combination chemotherapy. These trials are reviewed below; the relative role and effectiveness of surgery and/or RT for local control are examined.
The Intergroup Ewing Sarcoma Studies (IESS), while important in defining chemotherapy agents and efficacy, have also established the RT backbone for ESFT as used today [16–19]. The IESS-I study accrued patients between 1975 and 1977 [16]. Two groups of institutions were defined. One group randomized patients between vincristine, dactinomycin, cyclophosphamide, and doxorubicin (VACA) and vincristine, dactinomycin, cyclophosphamide (VAC) while the other between VAC and VAC plus whole lung RT. RT was given 2–4 weeks after wound healing or biopsy. RT dose to the primary site (whole bone plus 5 cm margin on soft tissue mass) was 4,500–5,400 cGy depending on age. Lung radiation was 1,500–1,800 cGy. Similar doses (but with smaller margins and partial bone treatment) are currently used in North America [20]. The results of IESS-1 showed statistically significant improvement in 5-year relapse-free survival (RFS) and overall survival of 60 % and 65 % for VACA compared to 24 % and 28 % for VAC, respectively [16]. Interestingly whole lung RT combined with VAC yielded a 5-year EFS and overall survival of 44 % and 53 %, respectively (p < 0.06 compared to VACA). Results of IESS-1 are summarized in Table 1. RT was the primary modality used for local control with only 14 % complete resection (68 % biopsy only, 18 % incomplete resection, 15 % local failure). The study defined the significant prognostic factor of pelvic versus non-pelvic primary (p < 0.001) and showed improved prognosis with younger age (younger than 10 years; p < 0.001). Based on IESS-I, VACA became standard and IESS-II (1980–1983) studied high-dose intermittent VACA versus moderate dose continuous VACA [16]. In this study, 29 % of cases had surgery only, 17 % had incomplete resection plus postoperative RT, and 54 % had primary RT after biopsy only. RT was similar to IESS-1, except that whole lung RT was not used. There was no significant difference in relapse or overall survival according to the type of local control modality [17, 18]. High dose intermittent VACA was superior with 5-year RFS and overall survival of 73 % and 77 % compared with 56 % (p < 0.03) and 63 % (p < 0.05), respectively, for moderate dose continuous VACA [17]. After IESS-II therefore high-dose intermittent VACA became standard.
RT guidelines in following studies introduced a local control period which would take place after two cycles of chemotherapy (in IESS I, radiation began immediately with chemotherapy) [21, 22]. During the local control period, doxorubicin was used only for the first concurrent chemotherapy (week 9) and was given at least 1 day prior to radiation. The next concurrent cycles (weeks 12 and 15) included just vincristine and cytoxan, Patients with residual gross disease after surgery or biopsy only received cone down boost to total of 5,580 cGy. For metastatic patients [20], RT was prescribed to all sites (brain 4,500 cGy, positive cerebrospinal fluid 3,000 cGy to craniospinal axis, bone metastases 4,500 cGy, lung metastasis 1,200–1,500 cGy depending on age <6 years).
One other radiotherapy study performed at this time is worthy of note. In POG 8346, a randomization was performed between whole bone and a tailored bone RT field [23]. The target accrual was not met (40 patients were accrued), but there did not appear to be any advantage to treating the entire bone and current trials no longer include whole bone RT.
Also during the 1980s, clinical trials were conducted in Europe by the German/Dutch/Austrian/Swiss cooperative group (CESS-81, CESS-86) [24–30]. This group initially used VACA followed by local therapy followed by VACA (CESS-81). This study showed surprisingly poor outcome for patients receiving radiation compared with surgery for local control [24]. Local failure was 6 % for surgery only (5-year RFS 54 %) versus 17 % for surgery plus postoperative RT (68 % 5-year RFS) and 50 % for RT alone (43 % 5-year RFS). The high local failure rate has been attributed to poor quality assurance. CESS-86 used VACA or VAIA (with ifosfamide replacing cyclophosphamide) together with local control therapy [25]. In CESS-86, local failure for surgery alone was 4 %, for surgery plus postoperative RT 3 %, and for RT alone 13 % (24, 25). Five-year RFS rates were not different [25, 26] using ifosfamide (62 % versus 67 %; p = 0.74). Irradiated patients were randomized between conventional (1.8 Gy daily) or hyperfractionated split-course RT (1.6 Gy BID with break of 12 days after 22.4 and 44.8 Gy) but no differences were detected. Relapses were 30 % after radiotherapy (44 cases), 26 % after radical surgery (22 % of cases) and 34 % after combined treatment (93 cases) [24]. These rates of relapse with surgery and/or RT seem most consistent with our current understanding of the relative treatment efficacies of surgery and RT but also reflect the fact that patients with larger tumors and pelvic primaries are more likely to receive RT as the primary local control modality [24].
Next, the CESS combined efforts with the United Kingdom Children’s Cancer Study Group (UKCCSG) to undertake the EICESS-92 study [24, 29]. These groups defined standard risk (localized tumor volume <100 ml) and high risk among 647 cases. The standard risk patients were randomly assigned to VAIA induction followed by ten courses of VACA or VAIA (with ifosfamide replacing cytoxan). With respect to radiotherapy, EICESS-92 delivered 54.4 Gy for those not having surgery, incomplete surgery, or poor histologic response. Cases of marginal excision with good histologic response received 44.8 Gy to the primary site. Patients with lung and/or pleural metastases received 15 to 18 Gy whole lung radiation. High risk patients were randomized to 14 courses of VAIA or VAIA plus etoposide. The study concluded that cyclophosphamide had similar EFS and overall survival as ifosfamide but with greater toxicity. Etoposide appeared to be beneficial for high risk patients [24, 29].
A subset of CESS 81/86 cases in which primary radiotherapy was used for vertebral body tumors was reported [30]. A total of 116 cases were identified with 64.6 % treated with RT, 27.5 % with surgery and RT, and 3.4 % with surgery alone. Local recurrence was seen in 22.6 % (17 out of 75) with definitive RT. The authors concluded that surgery with wide resection margins is rarely possible and that efficacy of definitive RT was comparable to other sites of disease [30]. In another study of patients treated on CESS 81, CESS 86, and EICESS 92, the type of local therapy in 1,058 localized Ewing tumors was analyzed [24]. The rate of local failure was 8.5 % after surgery with or without postoperative RT and was 5.3 % after preoperative RT. After definitive RT the rate was 26.3 % (p = 0.001). The study emphasized that irradiated patients were a negatively selected population with unfavorable tumor sites.
Together with the IESS and CESS studies listed above, the most recent two large randomized studies completed by the NCI (Children’s Cancer Group [CCG], Pediatric Oncology Group [POG], and COG) between 1988 and 1998 have defined the current standard therapy with local control (surgery and/or RT) and chemotherapy for ESFT. The first of these studies primarily examined the addition of ifosfamide and etoposide to standard chemotherapy (vincristine, dactinomycin, cyclophosphamideand doxorubicin), and the second investigated a dose-intensive regimen using similar agents. Both ifosfamide and etoposide had been found to show response in relapsed Ewing sarcoma, and a strategy was designed to alternate treatment between these and standard doxorubicin, vincristine, cyclophosphamide and dactinomycin. Grier and coworkers [21] undertook a randomized study of chemotherapeutic agents in Ewing’s sarcoma (INT-0091), performed jointly between the CCG (CCG-7881) and the POG (POG-8850), completing accrual in 1992. Of 518 patients, 398 were non-metastatic and showed statistically improved 5-year overall survival (72 % vs. 61 %; p = 0.01) and EFS (69 % vs. 54 %; p = 0.005) with the addition of ifosfamide and etoposide [21]. There was no significant benefit for adding ifosfamide and etoposide for metastatic patients (EFS 22 % vs. 22 %).
In this Intergroup study, local control was prescribed at week 12 of chemotherapy and could include radiation, surgery, or both [21]. For resectable tumors achieving negative margins, no radiation was given. For patients having radiation alone, the pre-chemotherapy tumor volume tumor was treated with a 3-cm margin to 4,500 cGy, followed by boost to post-chemotherapy volume to 5,580 cGy. Sparing of the epiphysis was allowed. For residual disease after surgery, post-operative radiation was 4,500 cGy with 1-cm margin. For non-metastatic patients, 39 % received radiation only, 38 % surgery only, and 23 % had both surgery and radiation [21].
Interestingly for radiation oncologists, the beneficial effect of the addition of new systemic agents appeared to be manifested mainly in increased local control [21]. There were 28 (rate = 0.15) non-metastatic cases with local progression on standard therapy and nine of 398 (rate = 0.05) using experimental therapy (p < 0.001). Rates of systemic progression were 0.21 versus 0.22 (p = 0.92) in the two arms. Both local and systemic progression was seen in ten and four cases using standard and experimental therapy, respectively (p = 0.10). In five cases (20) the site of progression was not reported. As in other studies, patients treated with radiation alone or surgery plus radiation, generally had larger and/or unresectable tumors such that the relative effectiveness of these modalities was not determined.
In an attempt to further improve on the results of INT-0091, a dose-intensified regimen of VDC/IE was tested by Granowetter et al. [22] in INT-0154 (CCG-7942, POG-9354) in non-metastatic patients. A total of 478 eligible patients were randomized between standard doses of VDC/IE over 48 weeks, or a dose-intensified VDC/IE regimen given over 30 weeks. Chemotherapy doses in the standard arm were: vincristine (1.5 mg/m2), doxorubicin (75 mg/m2), cyclophosphamide (1,200 mg/m2) alternating every 3 weeks with ifosfamide 1,800 mg/m2 × 5 and etoposide 100 mg/m2 × 5. In the intensified arm, the treatment was still alternated every 3 weeks but the vincristine was given weekly × 3, the cyclophosphamide dose was 2,100 mg/m2 × 2 and the ifosfamide dose was 2,400 mg/m2 × 5. Local control at week 12 was resection or RT. Post-operative radiation was given for close or positive margins. The majority of patients had surgery alone for local therapy. In the standard arm the patients having surgery alone were 66 % versus 20 % with radiation alone and 15 % with combined treatment. For the dose-intensified arm, surgery, radiation, and combined treatments were 65 %, 23 %, and 12 %, respectively. For unresected tumor or gross residual disease the dose was 45 Gy to initial volume plus 2 cm margin, followed by boost to 55.8 Gy. For post-operative microscopic residual or close margin (less than 1 cm for bone, 5 mm for fat and muscle, and less than 2 mm for fascial planes) the dose was 45 Gy with 2 cm margin and boost to 50.4 Gy [22].
Results of this study showed no significant difference in the 5-year EFS of 72.1 % versus 70.1 % for dose intensification [22]. A total of 119 out of 478 eligible patients showed progression of disease. Local control with RT only was associated with increased local plus distant failure (p = 0.038); however local recurrence was not statistically different (p = 0.16). Local recurrence with surgery only was 5.1 %, with RT only 9.2 %, and with surgery plus RT 2.0 % [21]. The study concluded that dose intensification did not improve outcome in ESFT. A comparison of the CESS-86, INT-0091, and INT-0154 results is given in Table 2.
Decision making in ESFT may commonly require specialized knowledge regarding the surgical and radiation techniques for different sites (extremity, truncal, pelvic, vertebral, etc.) especially on clinical trials. It should be emphasized that close collaboration between pediatric orthopedic oncologist and the pediatric radiation oncologist will lead to optimal outcomes. Recently, a series of articles from the University of Florida [31–33] described their major experience in treating Ewing’s tumor in various body areas between 1970 and 2006. (1) In tumors of the pelvis and sacral bones [31], 35 cases were identified. Of these 26 were treated with radiation alone and nine had combination surgery and radiation. The 15-year cause-specific survival, freedom from relapse, and local control rates were 26 % versus 76 % (p = 0.016), 28 % versus 78 % (p = 0.015) and 64 % versus 100 % (p = 0.087) for patients treated with definitive RT and for combined surgery/RT, respectively. (2) Nine patients treated to the head and neck were identified and received radiation [33]. Three of these also had local excision. The 10-year cause specific survival was 77 percent and late complications included poor dentition, mild xerophthalmia, cataract, and mandibular hypoplasia [33]. (3) A total of 53 cases of lower extremity Ewing’s were reported, of these 30 were treated with radiation alone and 23 had combination surgery and radiation [32]. The University of Florida researchers noted increased risk of recurrence in lower extremity cases treated without surgery although overall survival and cause specific survival were not statistically different. Interestingly, from 1985 the rate of lower extremity cases treated primarily with surgery at the University of Florida increased from 24 % to 61 %. The rates of overall survival and cause specific survival were 68 % versus 47 % (p = 0.21) and 73 % versus 47 % (p = 0.13) [32]. Once again, interpretation of the relative benefits of primary surgical and radiation approach such is made difficult because radiation patients commonly have more advanced disease. In general, surgery is favored in resectable cases.
Radiation therapy for metastatic disease
In addition to multi-agent chemotherapy, RT regimens have been increasingly employed for ESFT metastatic at diagnosis. Most of the larger cooperative group trials outlined above included both clinically localized and metastatic patients. Thus radiation for metastatic sites in ESFT has historical basis and may include whole lung radiation (usually 12–15 Gy depending on age; some have used 18 Gy bid) and/or radiation to numerous sites with up to 55.8 Gy [34–37]. Radiation for widespread metastatic disease is limited by BM suppression and clinical trials have limited radiation to less than 30 % to 50 % of the estimated active marrow [38]. Such aggressive radiation for metastases may be unfamiliar in the management of adult patients with solid tumors. Surgery or radiation or both has been used for the primary site in metastatic cases.
Paulino and coworkers [37] reported on the University of Iowa experience in a retrospective review of ESFT cases treated from 1976 to 2001. A total of 30 cases with metastatic disease at diagnosis were identified. Most common sites of distant metastases were lung and bone (63 % each). Six patients (20 %) had isolated pulmonary metastases. The overall survival at 5 years was 22.1 %. The use of local control to the primary site (p < 0.001) was a statistically significant prognostic factor for overall survival. For eight patients who did not have local control (surgery and/or radiation) to the primary site, the median survival was only 9 months. Sixteen cases were treated to distant metastatic sites and nine of 19 patients with lung metastases received whole lung irradiation (12.5–18 Gy). Six patients having had lung and/or other distant sites radiated were long-term survivors.
Pneumonitis
Reported rates of pneumonitis among pediatric patients treated with whole lung radiation have varied in Wilms’ tumor, ESFT, and rhabdomyosarcoma. In a 1975 report, 13 of 62 (21 %) patients of total lung irradiation developed radiation pneumonitis [39]. Pneumonitis was slightly greater (23 %) in those receiving 1,500 cGy or more. 3D dosimetry employed in modern clinics has dramatically improved since the 1970s and whole lung radiation cases should be treated using heterogeneity corrections.
Both pneumonitis and hemorrhagic cystitis were increased in the COG AEWS02P1 trial [40]. This was a pilot study of low dose antiangiogenic chemotherapy with standard alternating five drug chemotherapy for metastatic disease. Patients received radiation to all sites of metastatic disease. Whole lung radiation (12–15 Gy) was given for lung metastases. The experimental regimen of vinblastine (1 mg/m2/dose i.v. push three times per week) and celecoxib (250 mg/m2/b.i.d.) was given beginning day of cycle 1 and continuing through day 21 of cycle 14. Thirty-five eligible patients were enrolled. Results showed two deaths from pneumonitis attributed possibly to the combination with celecoxib. Seven of 21 patients who received pulmonary irradiation had grade 2 or greater toxicity [40]. This compares with reports of minimal lung toxicity reported in CESS 86 and EICESS 92 in which only one patient having fatal pneumonitis after whole lung radiation was reported [29].
Hemorrhagic cystitis
Hemorrhagic cystitis is a well-known complication of chemotherapy in ESFT but radiation is contributing factor [41]. Besides hemorrhagic cystitis, bladder fibrosis, and bladder carcinoma may occur. In a Mayo Clinic study of 116 Ewing’s sarcoma cases (1964 to 1985) in which cyclophosphamide was used as part of the chemotherapy, 17 patients developed hemorrhagic cystitis defined as either gross hematuria or cystoscopic finding of bladder mucosal hemorrhage [42]. Nine of the 17 (53 %) had also had pelvic RT. An additional 12 patients had minor urinary complaints such as irritative voiding symptoms, frequency, urgency, dysuria, mild incontinence or enuresis. The use of MESNA [43] which inhibits the urotoxicity of acrolein, was then introduced to reduce cystitis.
In the AEWS02P1 study including vinblastine and celecoxib, 14 out of 15 cases with pelvic disease had local RT [40]. Of these, six of 15 developed hemorrhagic cystitis, a much higher level than seen on larger trials. This finding has been attributed to the combination of radiation with anti-angiogenic chemotherapy.
Second malignancy
A wide range of values for risk for second malignancy after radiation treatment for Ewing sarcoma have been published [21, 22, 44–46]. Some data suggest that uncharacterized predisposing genetic influences result in increased second cancer risk in ESFT and osteosarcomas even without added carcinogens, chemotherapy and radiation. This is manifested in the fact that the most frequent second malignancy after a primary sarcoma of childhood is another sarcoma of different histology [44].
With respect to second cancers, both epidemiologic and group investigations are informative. From St. Jude’s Children’s Research Hospital, there were 16 second malignancies including ten sarcomas, among the 266 survivors of Ewing’s sarcoma [45]. The median follow-up was 9.5 years, and the median latency was 7.6 years. The 20-year cumulative incidence rates for any second malignancy and for secondary sarcoma were 9.6 % and 7.5 %, respectively. Most recent data from cooperative group experience confirms a finite rate of second solid cancers occurring at least four fold as often as in the general population [21, 22]. Goldsby and coworkers [46] looked at the incidence of solid organ second malignancy in survivors of pediatric malignant bone tumors for COG and POG protocols from 1976 to 2005. There were 2,482 patients, and 1,156 of these had Ewing’s sarcoma. With a median follow-up of 6.1 years, nine out of 1,156 patients developed solid organ SMNs amongst Ewing’s sarcoma cases. Six of the nine were secondary sarcomas. The standardized incidence ratio for development of SMN with the use of radiation was 4.08 (95 % CI 2.43–7.13) considering all osteosarcoma and Ewing’s sarcoma cases together. The authors concluded that radiation related solid SMNs would likely increase with longer follow-up but that recurrence of the tumor remains a greater problem. A German/Austrian/Dutch study of 690 cases treated between 1992 and 1999 showed that with 56 months observation time, six out of 690 developed second cancers (three were solid tumors) [47].
In the study of Grier et al. [21], there were seven cases of second malignancy observed among 518 cases. Two were AML, one myelodysplastic syndrome, one ALL, one MFH, one osteosarcoma, and one ovarian tumor. The MFH and the osteosarcoma were within the radiation fields. In the study of Granowetter et al. [22] (INT-0091), 18 second malignancies were observed out of 478 cases. Second malignancy was detected in 2.8 % of surgery alone cases versus 3.5 % of radiation and 2.9 % of surgery plus radiation patients (p = 0.30). The incidence of secondary solid tumor was relatively small and equal number of patients with secondary solid tumors had been treated with or without radiation.
Currently open clinical trials
With respect to the details of radiotherapy for currently open cooperative group trials, both European and American approaches must be considered. The COG study AEWS1031 randomizes non-metastatic patients to standard chemotherapy with or without vincristine, topotecan and cyclophophamide. As in previous trials, for definitive radiation or gross residual disease after surgery the dose remains 45 Gy plus 10.8 Gy boost. Exceptions are vertebral body tumors (45 Gy plus 5.4 Gy boost) and extraosseous tumors with complete response to chemotherapy (50.4 Gy). The study allows for pre-operative RT (36 Gy) in selected cases. If a patient has pre-operative therapy and there is greater than 90 % necrosis an additional 14.4 Gy is given. Patients with positive pleural fluid receive lung radiation.
The Euro-EWING 99 trial is divided into a localized disease protocol and a pulmonary/pleural disease protocol. A number of cooperative groups are participating in this trial including the United Kingdom Children's Cancer Study Group, Gesellschaft für Pädiatrische Onkologie und Hämatologie, Société Française des Cancers d'Enfants, European Organisation for Research and Treatment of Cancer — Soft Tissue and Bone Sarcoma Group, Schweizerisches Institut für Angewandte Krebsforschung, Scandinavian Sarcoma Group, Children's Oncology Group, European Organisation of Blood and Marrow Transplantation). Briefly, for localized disease, the trial uses six cycles of VIDE induction therapy with collection of peripheral blood stem cells, then randomization to various consolidation chemotherapy regimens (either VAI vs. VAC vs. high-dose busulfan, melphalan with stem cell rescue). For patients with pleural and pulmonary metastases, VAI plus whole lung radiation is compared to consolidation with high dose busulfan melphalan and stem cell rescue. There is a local control period after four courses of VIDE; patients who remain inoperable may be offered definitive RT. Postoperative RT is given in cases of intralesional or marginal surgery and is advised for poor histologic response regardless of margins. The radiation prescription for primary site in Euro-EWING study may be summarized as follows: There is accelerated hyperfractionated radiation of 44.8 Gy (1.6 Gy bid) given to the “compartment” and boost to 54.4 Gy at 1.6 Gy bid. There is a planned break of about 7–12 days after half of the total dose. For postoperative treatment (i.e., marginal surgery or wide resection with poor histologic response), the dose is 44.8 Gy. Although the hyperfractionated accelerated course is strongly advised, a number of exceptions have to be made, e.g., with large radiation portals, small bowel in the radiation field, and radiation of the central nervous system. Since some patients will have high dose therapy with busulfan and melphalan, radiotherapy must often be delayed until 8–10 weeks after high dose treatment. Whole lung radiation is 15 Gy (either 1.5 Gy once daily or 1.25 Gy twice daily) and is not allowed for patients on busulfan containing regimens.
Proton radiation therapy
Radiation with hadron particles including protons may have theoretical advantages in treating pediatric cancers. Proton therapy may have similar biologic dose effectiveness as standard photon treatment but because of the Bragg peak effect, the exit dose is limited [48]. This has the possibility of limiting the dose to normal tissue. The availability of proton therapy is rapidly increasing and many new centers are under construction. Current cooperative group trials allow proton therapy and have proton therapy quality assurance.
A report from the Francis Burr proton center at Massachusetts General Hospital described a total of 30 patients treated with proton therapy as part of the treatment for ESFT. Median dose was 54 Gy. This unit provides a rotational gantry system and maximum proton beam energy of 231 MeV. Chemotherapy was based on the POG 9354 protocol. The median age was relatively low at 10 years and the distribution of tumor sites was unusual possibly attributed to referral bias to spare critical normal structures. The 3-year event-free survival and overall survival were 60 % and 89 %, respectively [48]. Proton therapy was well tolerated generally, with five of 30 cases showing confluent moist desquamation of the skin. Scolioses/kyphoses were noted in five patients (1 severe) having vertebral body tumor and laminectomy. Four patients had secondary malignancies (three AML and one MDS). The authors concluded that proton therapy provides a means to improve dose localization and minimize dose to normal tissue [48].
Myeloablative studies
High dose chemotherapy with stem cell rescue is also a strategy for advanced ESFT and in many ways may be a competing modality to RT. Toxicities may be additive (especially with lung radiation) when these treatments are combined. Dose-intensive chemotherapy with autologous BM or peripheral blood stem cell (PBSC) rescue has been studied in both single institution and cooperative group settings. Burke et al. [49] described tandem high-dose chemotherapy with peripheral stem cell rescue as consolidation therapy for high-risk ESFT [48]. Four out of eight consecutive patients treated between 1992 and 2003 remained in complete remission. Three of the remission patients did not have local therapy at primary or metastatic sites.
Burdach and coworkers [50] performed both allogeneic and autologous stem-cell transplantation in advanced Ewing tumor. Thirty-six patients had the hyperME protocol treatment (hyperfractionated total body irradiation, melphalan, etoposide ± carboplatin), and all had remission to induction chemotherapy and local treatment before myeloablative therapy. A total of 26 patients had autologous and ten had allogeneic stem cells. The event-free survival was 24 % with 18 of 36 cases relapsed or died of disease and nine of 36 died of treatment related toxicity. Nine of 36 cases remained alive in CR at the time of the report [50]. Later these workers tested tandem melphalan/etoposide (Tandem ME). Event-free survival with HyperME and Tandem ME were 22 ± 8 % versus 29 ± 9 %, respectively [50]. Hawkins and coworkers [51] described myeloablative therapy in 16 patients followed by stem cell rescue. Patients had busulfan, melphalan, and thiotepa; nine also had total marrow irradiation [51]. Six patients survived without relapse from 27 to 66 months. They concluded that dual myeloablative therapy with these agents and total marrow radiation was feasible and promising although their inability to collect sufficient peripheral blood stem cells and extensive previous RT was a limitation [51].
Kushner and Meyers reviewed the use of BM and peripheral blood stem cell therapies at the Memorial Sloan Kettering Cancer Center [52]. Twenty-one patients with bone or BM metastases were treated upfront with the P6 chemotherapy regimen and those who achieved complete remission or very good partial remission were then treated with myeloablative therapy. This dose-intensive treatment included either total body irradiation (15 Gy) with melphalan (180 mg/m2) or used thiotepa (900 mg/m2) and carboplatin (1,500 mg/m2). The P6 regimen included cyclophosphamide (4.2 g/m2), doxorubicin (75 mg/m2), vincristine (2 mg/m2) cycles 1, 2, 3, and 6 and ifosfamide (9 g/m2) and etoposide (500 mg/m2) cycles 4,5, and 7, and tumor resection was after cycle 3 [52]. Radiation was given after completion of all chemotherapy (1.5 Gy bid to a total of 45 or 54 Gy).
Results of the MSKCC experience showed only one patient to be a long term event-free survivor [52]. Four of eight patients with TBI/melphalan relapsed within 2–7 months and three patients treated with thiotepa/carboplatin relapsed within 3–4 months. Three of eight TBI/melphalan patients died of toxicity. The authors reviewed the literature and concluded that dose-intensive treatment was reaching limits of efficacy and toxicity and that introduction of new therapies was needed to make any major impact on prognosis [52].
Relatively limited efficacy and high toxicity of BM/PBSC therapy for Ewing’s sarcoma with similar strategies is also reflected from the report of the European Bone Marrow Transplantation Registry (EBMTR) [53]. Six different myeloablative regimens were tried in 21 patients with metastatic bone/BM disease with six long-term survivors and two deaths from toxicity [53]. Recent data from the EBMTR suggested relatively improved overall survival with the use of busulfan based regimens [54]. The ongoing Euro-Ewing trial may help to answer this question.
Conclusions
It may be said that advances in radiotherapy have paralleled advances in treatment for Ewing’s sarcoma. The words of Dr. Ewing remind us of the many decades of radiotherapy advances: “Roentgenologists who engaged in therapy were looked upon with suspicion. It was difficult to enlist the interest of any established roengenologist in this questionable field. The advance into the use of higher voltages, frequent calibration and increasing standardization of methods rescued Roentgen therapy from imminent disrepute. It would have been impossible to imagine the dramatic expansion of radiation oncology in the coming century.”
The clinical trials reviewed here primarily considered chemotherapy questions but still attest to the incremental advances in RT achieved over many decades. We have made progress in optimally integrating radiation pre-operatively and post-operatively with surgery for disease sites. Still, determining relative efficacy of surgery and radiation modalities has been limited by the fact that radiation cases generally had more advanced disease. The dose-limiting toxicities of radiation combined with aggressive chemotherapy require further definition. Factors predicting for pneumonitis and rates of second malignancy are problems requiring further study. Myeloablative study has not so far achieved overly promising results. Proton therapy is an example of the further advances in RT for Ewing’s sarcoma on the horizon. These treatments will no doubt require careful integration into future clinical trials with both targeted chemotherapy agents and improvements in surgical techniques.
References
Hense HW, Ahrens S, Paulussen M et al (1999) Descriptive epidemiology of Ewing’s tumor: analysis of German patients from (EI)CESS 1980–1997. Klin Paediatr 21:271–275
Dunst J, Schuck A (2004) Role of Radiotherapy in Ewing Tumors. Pediatr Blood Cancer 42:465–470
Paulino AC, Nguyen TX, Mai WY (2007) An analysis of primary site control and late effects according to local control modality in non-metastatic Ewing sarcoma. Pediatr Blood Cancer 49:423–429
Karosas A (2010) Ewing’s Sarcoma. Am J Health Syst Pharm 67:1599–1605
Ewing J (1922) The mode of action of radiation upon carcinoma. Am J Roentgenol 9:331–336
Ewing J (1921) Diffuse endothelioma of bone. Proc NY Pathol Soc 21:17–24
Ewing J (1917) Radium therapy in cancer. J Am Med Assoc 68:1238–1247
Ewing J (1926) Tissue reactions to radiation. Am J Roentgenol 15:93–115
Ewing J (1930) Factors determining radioresistance in tumors. Radiology 14:186–190
Ewing J (1934) American Radium Society Janeway lecture excerpts. Am J Roentgenol 31:153–163
LeDeley MC, Delattre O, Schaefer KL et al (2010) Impact of EWS-ETS fusion type on disease progression in Ewing’s sarcoma/peripheral primitive neuroectodermal tumor: prospective results from the cooperative Euro-EWING 99 Trial. J Clin Oncol 28:1982–1988
Van Doorminck JA, Ji L, Schoab B et al (2010) Current treatment protocols have eliminated the prognostic advantage of type 1 fusions in Ewing sarcoma: a report from the Children’s Oncology Group. J Clin Oncol 28:1989–1994
Zoubek A, Dockhorn-Dwomiczak B, Dlattre O et al (1996) Does expression of different EWS chimeric transcripts define clinically distinct risk groups of Ewing tumor patients? J Clin Oncol 14:1245–1251
De Alava E, Kawai A, Heley JH et al (1998) EWS-FLI1 fusion transcript structure is an independent determinant of prognosis in Ewing’s sarcoma. J Clin Oncol 16:1248–1255
Barr FG, Meyer WH (2010) Role of fusion subtype in Ewing sarcoma. J Clin Oncol 28:1973–1981
Nesbit ME et al (1990) Multimodal therapy for the management of primary, nonmetastatic Ewing’s sarcoma of bone: a long-term follow-up of the first intergroup study. J Clin Oncol 7:1664–1674
Burgert EO Jr et al (1990) Multimodal therapy for the management of nonpelvic localized Ewing’s sarcoma of bone: Intergroup Study IESS-II. J Clin Oncol 8:1514–1524
Evans RG et al (1991) Multimodal therapy for the management of localized Ewing’s sarcoma of pelvic and sacral bones: a report from the second intergroup study. J Clin Oncol 9:1173–1180
Cangir A et al (1990) Ewing’s sarcoma metastatic at diagnosis: results and comparison of two Intergroup Ewing’s sarcoma studies. Cancer 66:887–893
Merchant TE, Kushner BH, Sheldon JM, LaQuaglia M, Healey JH (1999) Effect of low-dose radiation therapy when combined with surgical resection for Ewing sarcoma. Med Pediatr Oncol 33:65–70
Grier HE, Krailo MD, Tarbell NJ et al (2003) Addition of ifosfamide and etoposide to standard chemotherapy for Ewing’s sarcoma and primitive neuroectodermal tumor of bone. NEJM 348:694–701
Granowetter L, Womer R, Devidas M, Krail M et al (2009) Dose-intensified compared with standard chemotherapy for non-metastatic Ewing sarcoma family of tumors: a Children’s Oncology Group study. J Clin Oncol 27:2536–2541
Donaldson SS et al (1989) The Pediatric Oncology Group (POG) experience in Ewing’s sarcoma of bone. Med Pediatr Oncol 17:283
Schuck A, Ahrens S, Paulussen M et al (2003) Local therapy in localized Ewing tumors: results of 1058 patients treated in the CESS 81, CESS 86, and EICESS 92 trials. Int J Radiat Oncol Biol Phys 55:168–177
Dunst J, Jurgens H, Sauer R et al (1995) Radiation therapy in Ewing’s sarcoma: an update of the CESS 86 trial. Int J Radiat Oncol Biol Phys 32:919–930
Dunst J, Sauer R, Burgers JM et al (1991) Radiation therapy as local treatment in Ewing’s sarcoma: results of the cooperative Ewing’s sarcoma studies CESS 81 and CESS 86. Cancer 67:2818–2825
Jurgens H, Exner U, Gardner H et al (1988) Multidisciplinary treatment of primary Ewing’s sarcoma of bone: a 6-year experience of a European cooperative trial. Cancer 61:23–32
Schuck A, Ahrens S, Konarzewska A et al (2002) Hemithorax irradiation for Ewing tumors of the chest wall. Int J Radiat Oncol Biol Phys 54:830–838
Paulussen M, Craft AW, Lewis I et al (2008) Results of the EICESS-92 study: two randomized trials of Ewing’s sarcoma treatment—cyclophosphamide compared with ifosfamide in standard-risk patients and assessment of benefit of etoposide added to standard treatment in high-risk patients. J Clin Oncol 26:4385–4393
Schuck A, Ahrens S, Von Schorlemer I et al (2005) Radiotherapy in Ewing tumor of the vertebrae: treatment results and local relapse analysis of the CESS 81/86 and EICESS 92 trials. Int JRadiat Oncol Biol Phys 63:1562–1567
Indelicato DJ, Keole SR, Shahlahee AH et al (2008) Impact of local management on long-term outcomes in Ewing tumors of the pelvis and sacral bones: the University of Florida experience. Int J Radiat Oncol Biol Phys 72:42–48
Indelicato DJ, Keole SR, Shahlahee AH et al (2008) Long-term clinical and functional outcomes after treatment for localized Ewing’s tumor of the lower extremity. Int J Radiat Oncol Biol Phys 70:501–509
Whaley JT, Indelicato DJ, Morris CG et al (2010) Ewing tumors of the head and neck. Am J Clin Oncol 33:321–325
Paulussen M, Ahrens S, Burdach S et al (1998) Primary metastatic (stage IV) Ewing tumor: survival analysis of 171 patients from the EICESS studies. Ann Oncol 9:275–281
Paulussen M, Ahrens S, Craft AW et al (1998) Ewing’s tumors with primary lung metastases: survival analysis of 114 (European Intergroup) cooperative Ewing’s sarcoma Studies patients. J Clin Oncol 15:3044–3052
Spunt SL, McCarville MB, Kun LE et al (2001) Selective use of whole-lung irradiation for patients with Ewing sarcoma family tumors and pulmonary metastases at the time of diagnosis. J Pediatr Hematol Oncol 23:93–98
Paulino AC, Mai WY, Teh BS (2012) Radiotherapy in metastatic Ewing’s sarcoma. Am J Clin Oncol (Epub ahead of print)
Ellis R (1961) The distribution of active bone marrow in the adult. Phys Med Biol 5:255–258
Baeza MR, Barkley HT Jr, Fernandez CH (1975) Total-lung irradiation in the treatment of pulmonary metastases. Radiology 116:151–154
Felgenhauer JL, Nieder ML, Krailo MD et al. (2012)A pilot study of low-dose antiangiogenic chemotherapy in combination with standard multiagent chemotherapy for patients with newly diagnosed metastatic Ewing sarcoma family of tumors: a Children’s Oncology Group (COG) phase II study (Epub ahead of print)
Crew JP, Jephcott CR, Reynard JM (2001) Radiation-induced haemorrhagic cystitis. Eur Urol 40:111–123
Stillwell TJ, Benson RC Jr, Burgert EO Jr (1988) Cyclophosphamide-induced hemorrhagic cystitis in Ewing’s sarcoma. J Clin Oncol 6:76–82
Bryant BM, Jarman M, Ford HT et al (1980) Prevention of isophosphamide induced urothelial toxicity with 2-mercaptoethane sulphonate sodium (mesnum) in patients with advanced carcinoma. Lancet 2:657–59
Chuba PJ, Hamre MR, Thomas R et al. (2005) Radiation induced second sarcomas occurring after primary sarcoma of childhood. (abstract) Proceedings of Pediatric Radiation. Oncology Society (PROS), Lyon.
Kuttesch JF, Wexler LH, Marcus RB et al (1996) Second malignancies after Ewing’s sarcoma. Radiation dose-dependency of secondary sarcomas. J Clin Oncol 14:2818–2825
Goldsby R, Burke C, Nagarajan R et al (2008) Second solid malignancies among children, adolescents, and young adults diagnosed with malignant bone tumors after 1976: follow-up of a Children’s Oncology Group Cohort. Cancer 113:2597–2604
Paulussen M, Ahrens S, Lehnert M et al (2001) Second malignancies after Ewing tumor treatment in 690 patients from a cooperative German/Austrian/Dutch study. Ann Oncol 12:1619–1630
Rombi B, Delaney T, Macdonald S et al (2012) Proton radiotherapy for pediatric Ewing’s sarcoma: initial clinical outcomes. Int JRadiat Oncol Biol Phys 82:1142–1148
Burke MJ, Walterhouse DO, Jacobsohn DA et al (2007) Tandem high-dose chemotherapy with autologous peripheral hematopoietic progenitor cell rescue as consolidation therapy for patients with high-risk Ewing family tumors. Pediatr Blood Cancer 49:196–198
Burdach S, van Kaick B, Laws HJ et al (2000) Allogeneic and autologous stem-cell transplantation in advanced Ewing tumors. An update after long-term follow-up from two centers of the European Intergroup study EICESS. Stem-cell transplant programs at Dusseldorf University Medical Center, Germany and St. Anna Kinderspital, Vienna Austria. Ann Oncol 11:1451–1462
Hawkins D, Barnett T, Bensinger W et al (2000) Busulfan, melphalan, and thiotepa with or without total marrow irradiation with hematopoietic stem cell rescue for poor-risk Ewing-Sarcoma-Family tumors. Med Pediatr Oncol 34:328–337
Kushner BH, Meyers PA (2001) How effective is dose-intensive/myeloablative therapy against Ewing’s sarcoma/primitive neuroectodermal tumor metastatic to bone or bone marrow? The Memorial Sloan–Kettering experience and a literature review. J Clin Oncol 19:870–880
Ladenstein R, Lasset C, Pinkerton R et al (1995) Impact of megatherapy in children with high-risk Ewing’s tumors in complete remission: a report from the BMT solid tumor registry. Bone Marrow Transplant 15:697–705
Laurence V, Peirga JY, Barthier S et al (2005) Long-term follow up of high-dose chemotherapy with autologous stem cell rescue in adults with Ewing tumor. Am J Clin Oncol 28:301–309
Conflict of interest
The author of this review has no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chuba, P.J. Radiation therapy strategies and clinical trials in pediatric Ewing’s sarcoma. J Radiat Oncol 2, 149–158 (2013). https://doi.org/10.1007/s13566-012-0082-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13566-012-0082-3