
Abstract
Introduction
There is currently a lack of research regarding disease course and burden as well as treatment patterns and goals in patients with non-segmental vitiligo (NSV). The aim of this analysis was to evaluate disease course, treatment patterns and goals in patients with NSV.
Methods
This analysis used secondary data from the Adelphi Real World Vitiligo Disease Specific Programme™ 2021, specifically, a survey of physicians and their adult and adolescent patients with NSV. Physicians categorized patients by the extent of NSV at time of survey completion as mild, moderate or severe/very severe. Physician-reported patient information included demographics, current/previously prescribed NSV therapies, treatment satisfaction and the Vitiligo Noticeability Scale (VNS). Patients completed a survey on treatment satisfaction and the VNS. Treatment pattern data were stratified by disease extent and Fitzpatrick skin type.
Results
At survey completion, physicians reported that 38, 50 and 12% of patients (N = 1865) had improving, stable and deteriorating/progressing disease, respectively. Most patients (96%) with mild disease at treatment initiation still had mild disease at the time of survey completion. More than half of patients with moderate disease (62%) or severe/very severe disease (57%) at treatment initiation still had moderate or severe/very severe disease at survey completion. Topical calcineurin inhibitors (TCIs) were the most common treatment in 40% of patients followed by phototherapy in 30%. Patients hoped for re-pigmentation (mild 56%, moderate 62%, severe/very severe 66%), reduction (mild 50%, moderate 56%, severe/very severe 49%) or cessation of affected areas with vitiligo (mild 48%, moderate 54%, severe/very severe 43%).
Conclusion
The study findings indicate that a significant proportion of patients with NSV are not improving on current treatments, most commonly TCIs and phototherapy. The results highlight the unmet need for novel and effective therapies to substantially improve re-pigmentation, an important treatment goal for patients with NSV.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
There is currently a lack of research regarding disease course and burden as well as treatment patterns and goals in patients with non-segmental vitiligo (NSV) |
The aim of this real-world analysis was to evaluate current disease course, treatment patterns and goals in patients with NSV in Europe and the USA |
What was learned from the study? |
The findings of this study demonstrate that a significant proportion of patients with NSV are not improving on current treatments, most commonly topical calcineurin inhibitors and phototherapy, and most patients’ disease extent did not change following treatment |
The results highlight the unmet need for novel and effective therapies for patients with NSV to substantially improve re-pigmentation |
Introduction
Vitiligo is an autoimmune disorder characterized by selective loss of melanocytes, which appears as depigmented patches of skin [1, 2]. This skin disorder affects 1.3% of the worldwide population [3]. Of the two types of vitiligo, segmental and non-segmental vitiligo (NSV), the latter is more common and is characterized by symmetrical and bilateral white patches, whereas segmental vitiligo has unilateral distribution [2].
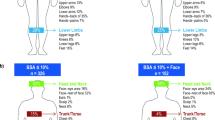
Vitiligo is associated with psychological comorbidities, such as depression and anxiety, and autoimmune comorbidities, such as thyroid disease and psoriasis [4,5,6]. As a result, vitiligo can have a significant negative impact on quality of life with patients experiencing psychosocial burden [4, 7]. In particular, patients with vitiligo have reported that the disorder impacts daily activities, self-esteem, relationships and their career [4]. Patients with > 5% body surface area (BSA), darker skin types and facial or hand lesions reported being more affected by the psychosocial burden of vitiligo [4]. In recent studies, facial involvement in vitiligo has been shown to drive psychosocial burden and patients’ perceived disease extent [8, 9]. Moreover, disease-perceived extent is higher in patients with > 5% compared with < 5% BSA [5]. Additionally, management of vitiligo is associated with increased healthcare costs and resource utilization, further burdening patients managing the disorder [10].
Until recently, there was no approved treatment for vitiligo. In 2022, the United States (US) Food and Drug Administration approved ruxolitinib, a topical cream, as the first and only treatment for NSV [11]. Ruxolitinib was more recently approved in 2023 in Europe [12]. Therefore, patients have been frequently prescribed topical corticosteroids, oral corticosteroids and calcineurin inhibitors as a first line of therapy [13]; however, these treatments have limitations, including side effects and poor efficacy [14]. Additionally, a large proportion of patients are not receiving any therapy [5, 13].
Both patients and healthcare professionals consider a reduction in the spread of vitiligo and re-pigmentation of skin affected by vitiligo to be important treatment goals [15]. Furthermore, in a recent survey, patients with NSV reported that novel, improved treatments are needed for NSV, with approximately half of patients indicating that they are not satisfied with current therapies and that available treatments are not effective [7]. Thus, there is an unmet need in vitiligo for effective treatments that satisfy both patient and healthcare provider treatment goals.
There is currently a lack of research regarding disease course and burden in patients with NSV as well as treatment patterns and goals. Thus, the aim of this real-world analysis was to evaluate disease course, current treatment patterns and goals in patients with NSV in Europe and the US.
Methods
Study Design and Patients
This analysis used secondary data from the Adelphi Real World Vitiligo Disease Specific Programme™ (DSP). The DSP is a linked cross-sectional survey of physicians and their adult and adolescent NSV patients with elements of retrospective data collection, conducted in the US, France, Germany, Italy, Spain and the UK in 2021. Full methodology of the DSP has been published elsewhere [16, 17].
Dermatologists were recruited through publicly available lists according to predefined eligibility criteria to ensure a geographically diverse sample. Physicians whose specialty was dermatology, those actively involved in the treatment and management of patients with NSV and those who had a minimum monthly workload of ≥ 6 adult and 2 adolescent patients with NSV were eligible for inclusion. Following selection, physicians completed an online survey on their disease management approach, prescribing of medications, knowledge of future drugs and their patient caseload.
Physicians subjectively assessed and classified patients by the extent of their NSV at the time of survey completion as mild, moderate or severe/very severe. Physicians categorized disease extent using their own holistic judgement, which was deemed the best way to represent real-world clinical practice. Physicians provided information on patient demographics, current/previously prescribed NSV therapies, satisfaction with treatment, reasons for dissatisfaction and how noticeable the vitiligo was (using the Vitiligo Noticeability Scale [VNS]) compared with before the initiation of their current treatment.
Recruited patients were ≥ 18 years for adults and 12–17 years for adolescents, had a physician-confirmed diagnosis of NSV, were not currently participating in an NSV clinical trial and were in the DSP database. Patients were invited to complete a survey that provided information on treatment satisfaction, reasons for dissatisfaction and the VNS.
Outcomes
Demographics were presented by disease extent (mild, moderate, severe/very severe) for a total patient population and included age, sex, ethnic origin, Fitzpatrick skin type (type I + II, III + IV, V + VI) and days since vitiligo diagnosis. For patients who were receiving treatment, disease extent at initiation of current treatment and days since treatment initiation were reported. A description of the current disease course (improving, stable or deteriorating/progressing) and treatment patterns was presented. Treatment patterns included type of treatment, line of therapy, change in disease extent since treatment initiation and vitiligo diagnosis and most common treatments stratified by most recently used line of therapy and by monotherapy or combination therapy. Treatment patterns were also stratified by disease extent and Fitzpatrick skin type. Treatment goals and improvement in disease extent were reported.
Statistical Analysis
All analyses were descriptive; data were presented as total number, mean (standard deviation [SD]) and percentages. Treatment patterns were aggregated and masked any country-specific differences.
Ethics
This analysis was conducted on existing de-identified data; therefore, the study team did not have access to any personal information on the patients or physicians and this study did not require ethics committee approval. As part of the DSP, patients were asked to complete a declaration page where they agreed to partake in the completion of the patient self-completion form in accordance with Health Insurance Portability and Accountability Act (HIPAA) and equivalent European Union guidelines. The DSP was submitted to the Pearl institutional review board. National data collection regulations were adhered to (European Society for Opinion and Market Research; US Department of Health and Human Services National Institutes of Health HIPAA; The Market Research Society; British Standards Institute).
Results
Patient Characteristics
This analysis included a total of 1865 patients with NSV, of which 1754 patients were receiving treatment. The mean age of patients was 31.8 years, 50% were female, and the most common Fitzpatrick skin type was III + IV in 45.7% (n = 852) of patients (Table 1). Of the 1754 patients who were receiving treatment, the majority had moderate disease (50.1%; n = 878), followed by mild (40.8%; n = 715) and severe/very severe (9.2%; n = 161). The mean (SD) time since diagnosis of NSV and since start of current treatment was 1196 (1834) and 345 (473) days, respectively.
Disease Course
Among all patients (N = 1865), 38%, 50% and 12% had improving, stable and deteriorating/progressing disease, respectively, as reported by physicians (Fig. 1). In patients with mild disease, 44% or 49% were considered currently improving or stable, respectively, whereas the percentages were 33% and 52%, respectively, in patients with moderate disease and 13% and 53%, respectively, in patients with severe/very severe disease.

Physician-reported disease course at time of survey completion based on disease extent for all patients
In patients who were receiving treatment (n = 1754), there was little change in disease extent with treatment; 96% of patients who had mild disease at treatment initiation still had mild disease at the time of survey completion. Similarly, 62% and 57% of patients with moderate and severe/very severe disease, respectively, at treatment initiation still had moderate and severe/very severe disease at the time of survey completion (Fig. 2). Likewise, since vitiligo diagnosis (n = 1407), most patients had the same disease extent at the time of survey completion (Fig. 3). In patients with moderate and severe/very severe disease, only 41% and 53% had improved, respectively.

Change in disease extent from treatment initiation to time of survey completion

Change in disease extent from vitiligo diagnosis to time of survey completion
In patients with darker skin types (type V + VI), 56% had moderate disease, whereas in patients with lighter skin types 51% (type III + IV) and 46% (type I + II) had moderate disease. Mild disease was less common in darker skin types than in lighter skin types (34% for type V + VI; 40% for type III + IV; 44% for type I + II). The percentages of patients with severe/very severe disease were similar across all skin types (10% for type V + VI; 9% for type III + IV; 10% for type I + II).
Treatment Patterns
At the time of survey completion, topical calcineurin inhibitors (TCIs) were the most commonly prescribed treatment in 40% of patients (monotherapy 17%; combination therapy 23%), followed by phototherapy in 30% of patients (monotherapy 9%; combination therapy 21%) (Fig. 4). Of 568 patients treated with phototherapy, 67%, 19% and 13% received narrow band ultra-violet B (NBUVB), ultra-violet A (UVA) combined and psoralen plus UVA (PUVA) combined, respectively. Among all patients (N = 1865), TCI and phototherapy were the most common treatments regardless of disease extent (Fig. 5). Of patients with mild, moderate and severe/very severe disease, 36.7%, 50.9% and 38.7% of patients were on two or more treatments. Moreover, 13.4% of patients with severe/very severe disease were not receiving any treatment. TCI was the most common treatment for all skin types in 40%, 43% and 35% of patients with skin type V + VI (n = 290), III + IV (n = 852) and I + II (n = 723), respectively (Fig. 6).

Most common physician-reported treatments at time of survey completion. *No Tx has been greyed out as this cannot be classed as either monotherapy or combination therapy. IS systemic immunosuppressant; JAKi Janus kinase inhibitor; MiP-TCS mild potency topical corticosteroid; MP-TCS moderate potency topical corticosteroid; NB-UVB narrow band ultra-violet B; Photo phototherapy; P-TCS potent topical corticosteroid; SC systemic corticosteroid; TCI topical calcineurin inhibitor; Tx treatment; Vit D vitamin D analogue

Most common prescribed treatments across mild, moderate and severe/very severe disease at time of survey completion. IS systemic immunosuppressant; JAKi Janus kinase inhibitor; MiP-TCS mild potency topical corticosteroid; MP-TCS moderate potency topical corticosteroid; NB-UVB narrow band ultra-violet B; Photo phototherapy; P-TCS potent topical corticosteroid; SC systemic corticosteroid; TCI topical calcineurin inhibitor; Tx treatment; Vit D vitamin D analogue

Most common physician-reported treatments by Fitzpatrick skin type at time of survey completion. IS systemic immunosuppressant; JAKi Janus kinase inhibitor; MiP-TCS mild potency topical corticosteroid; MP-TCS moderate potency topical corticosteroid; NB-UVB narrow band ultra-violet B; Photo phototherapy; P-TCS potent topical corticosteroid; SC systemic corticosteroid; TCI topical calcineurin inhibitor; Tx treatment; Vit D vitamin D analogue
The most frequent first-line therapy was phototherapy for patients with severe/very severe disease (35%), TCI for patients with mild disease (35%) and moderate potency topical corticosteroids for patients with moderate disease (32%) (Fig. 7a). At second line, phototherapy was the most common therapy for patients with severe/very severe (40%) and moderate disease (47%) and TCI for patients with mild disease (46%) (Fig. 7b).

Most common physician-reported treatments by disease extent at a first line and b second line of therapy. 8-MOP methoxsalen; MiP-TCS mild potency topical corticosteroid; MP-TCS moderate potency topical corticosteroid; NB-UVB narrow band ultra-violet B; NST non-steroidal topical (crisaborole); Photo phototherapy; P-TCS potent topical corticosteroid; PUVA psoralen + UVA; SC systemic corticosteroid; TCI topical calcineurin inhibitor; UVA ultra-violet A; Vit D vitamin D analogue; VP-TCS very potent topical corticosteroid
Treatment Goals
Of 574 patients who completed the patient self-completion form, 570 reported on treatment goals. More than half of all patients with mild (n = 332), moderate (n = 203) and severe/very severe (n = 35) disease extent hoped for treatments that would re-pigment affected areas (mild 56%, moderate 62%, severe/very severe 66%). Additionally, patients hoped for treatments that would shrink affected areas (mild 50%, moderate 56%, severe/very severe 49%) and stop the spread of vitiligo (mild 48%, moderate 54%, severe/very severe 43%).
Of 476 patients who answered questions on the patient self-completion form regarding meaningful changes in vitiligo on their body, 31% stated that a 50% improvement would be meaningful and 24% indicated a 75% improvement in body coverage would be considered a meaningful change (Table 2).
A total of 399 patients reported on a meaningful change in vitiligo on their face; 30% reported that only 100% improvement in vitiligo on their face would be meaningful. When examined by disease extent, 29% of patients with mild disease and 31% with moderate disease reported that 100% improvement would be a meaningful change in vitiligo on their face; 33% of patients with severe/very severe vitiligo reported that a 75% improvement would be meaningful.
Discussion
The results of this study show that while current treatments may work for some patients with NSV, a considerable number of patients with NSV do not improve. Disease extent was subjectively assessed by the physician at the time of consultation with the patient. It was more common for patients with darker skin types (III–VI) to have moderate disease than lighter skin types (I + II). Most patients had the same disease extent at survey completion as at vitiligo diagnosis or initiation of treatment, with the majority of patients on two or more treatments at the time of survey completion. TCIs and phototherapy were the most frequently used treatments for mild, moderate and severe/very severe disease across first and second lines of therapy. Regarding treatment goals, patients hoped for re-pigmentation of the affected area and reduction or cessation of the spread of vitiligo.
Our findings in patients across Europe and the US show that TCIs (40%) and phototherapy (30%) were the most common treatments prescribed. Rosmarin et al. reported that TCIs and phototherapy were prescribed in 14% and 4%, respectively, of their patient population with vitiligo in the US (N = 19,335), although not as frequently as oral corticosteroids (21%) and high-potency topical corticosteroids (20%) [13]. In the VIOLIN study of the CONSTANCES cohort of patients in France (N = 681), the most commonly reported treatments were oral corticosteroids (17%) and topical corticosteroids (14%) with tacrolimus (a type of TCI) the third most common treatment in only 3% of patients and < 1% received phototherapy [5]. Prior to the approval of ruxolitinib in 2023 [12], there were no approved re-pigmentation treatments in Europe, which is a possible explanation for the low percentage of patients receiving tacrolimus in the VIOLIN study [5]. The differences in the most common treatments and proportions of patients across studies could also be due to geographic location, varying data sources or differences in health insurance coverage. This comparison of treatment frequency across studies indicates that a range of therapies are being prescribed to patients with vitiligo.
In the current study, the data for treatment patterns through first and second lines of therapy show that large proportions of patients are cycling through TCIs and phototherapy. When patients were assessed at treatment initiation and then at time of survey completion, 62% still had moderate disease and 57% still had severe/very severe disease, indicating that treatment failed for a large proportion of patients with moderate and severe/very severe disease. This highlights an unmet need for effective treatments for managing vitiligo.
It is important to understand the patients’ perspective of vitiligo and treatment. The ComPaRe e-cohort study reported that adult patients’ perception of change in their vitiligo was correlated with their perceived disease extent, and the effect was increased with facial involvement compared to the rest of the body [9]. Another study showed that patients with lesions in visible areas of their body versus not, those with ≥ 10% facial involvement versus < 10% involvement, and > 5% versus < 5% BSA had higher disease-perceived extent [5]. No differences were reported among patients with darker versus fairer skin types. Additionally, Narayan et al. found that 67% of patients with NSV experienced their facial lesions as an extreme emotional disease burden and believed that novel treatments for vitiligo are needed [7].
In the VALIANT study, patients with vitiligo (N = 3541) reported that a reduction or cessation of spread (25%) and re-pigmentation of affected skin (23%) were important treatment goals [15], which agrees with the findings of the current study where 43–56% and 56–66% of patients, respectively, stated that these same treatment goals were very important. Regarding the patient’s perception of other meaningful improvements in vitiligo, three quarters of the patients in this study reported that a 50–100% improvement in vitiligo on their face or body would be a meaningful change. Similarly, Kitchen et al. showed that 66% (n = 59) and 17% (n = 50) of patients in their study reported that a 50% improvement in vitiligo on their face and body, respectively, would be considered an improvement [18]. Additionally, Kitchen et al. presented patient data showing that vitiligo on the face was the most bothersome area to have lesions (87%; n = 60) and the most important area to have improvement (74%; n = 54) [18]. Thus, across several studies, most patients reported that it was more important to have improvements in vitiligo on their face than their body and that a ≥ 50% improvement would be meaningful.
Narayan et al. reported that approximately half of patients with vitiligo are not satisfied with current treatment options and found them ineffective [7]. Moreover, the findings presented by Hamzavi et al. showed that a quarter of healthcare providers believe effective treatments do not exist and 45% of patients had given up on finding an effective treatment [15]. Consequently, the disease burden of vitiligo is high for patients with several factors exacerbating that burden, which further emphasizes the need for effective treatments.
There is limited research on treatment patterns, treatment satisfaction and disease course in NSV; this study helps to address this gap in the literature while highlighting unmet needs in vitiligo treatment. Ruxolitinib was recently approved, so it remains to be determined how it will impact treatment patterns or sequencing. Another strength of this study includes the sample size across multiple countries, increasing the generalizability of the findings. The DSP provides a large, representative sample of real-world patients, with methodology that is published and validated [16, 17]. The limitations of this study are that the data are descriptive, and no statistical analyses were conducted. Physicians subjectively assessed and categorized disease extent using their own holistic judgement, which was deemed the best way to represent real-world clinical practice. While the DSP has strengths as a methodology, it collates data exclusively on patients who visit their physician. Therefore, findings may not be generalizable to all patients with NSV, particularly those not frequently consulting their physician or who do not consult at all.
Conclusion
The findings of this study demonstrate that a significant proportion of patients with NSV are not improving on current treatments, most commonly TCIs and phototherapy. Most patients’ disease extent did not change following treatment. Yet, patients with NSV hoped for treatments that would re-pigment or shrink affected areas and stop the spread of vitiligo. These results highlight the unmet need for novel and effective therapies for patients with NSV to substantially improve disease course and treatment satisfaction.
Data Availability
All data, i.e., methodology, materials, data and data analysis that support the findings of this survey are the intellectual property of Adelphi Real World. All requests for access should be addressed directly to Peter Anderson, an employee of Adelphi Real World, at peter.anderson@adelphigroup.com.
References
Bergqvist C, Ezzedine K. Vitiligo: a review. Dermatology. 2020;236:571–92.
Ezzedine KEV, Whitton M, van Geel N. Vitiligo. Lancet. 2015;386:74–84.
Bibeau K, Pandya A, Ezzedine K, et al. Vitiligo prevalence and quality of life among adults in Europe, Japan and the USA. J Eur Acad Dermatol Venereol. 2022;36:1831–44.
Bibeau K, Ezzedine K, Harris JE, et al. Mental health and psychosocial quality-of-life burden among patients with vitiligo: findings from the global VALIANT study. JAMA Dermatol. 2023;159:1124–8.
Ezzedine K, Seneschal J, Da Silva A, et al. Vitiligo patient population and disease burden in France: VIOLIN study results from the CONSTANCES cohort. J Eur Acad Dermatol Venereol. 2023;37:2249–58.
Ezzedine K, Soliman AM, Li C, Camp HS, Pandya AG. Comorbidity burden among patients with vitiligo in the United States: a large-scale retrospective claims database analysis. Dermatol Ther (Heidelb). 2023;13:2265–77.
Narayan V, Uitentuis S, Luiten R, Bekkenk M, Wolkerstorfer A. Patients’ perspective on current treatments and demand for novel treatments in vitiligo. J Eur Acad Dermatol Venereol. 2021;35:744–8.
Ezzedine K, Eleftheriadou V, Jones H, et al. Psychosocial effects of vitiligo: a systematic literature review. Am J Clin Dermatol. 2021;22:757–74.
Merhi S, Salameh P, Abboud M, et al. Facial involvement is reflective of patients’ global perception of vitiligo extent. Br J Dermatol. 2023;189:188–94.
Ezzedine K, Soliman AM, Li C, Camp HS, Pandya AG. Economic burden among patients with vitiligo in the United States: a retrospective database claims study. J Invest Dermatol. 2023;144:540–6.
Incyte. Incyte announces FDA approval of Opzelura (Ruxolitinib) cream for the treatment of vitiligo. Available from: https://investor.incyte.com/news-releases/news-release-details/incyte-announces-us-fda-approval-opzeluratm-ruxolitinib-cream-0 (2022). Accessed 1 Feb 2024.
Incyte. European commission approval of opzelura (ruxolitinib) cream for the treatment of non-segmental vitiligo with facial involvement in adults and adolescents. Available from: https://investor.incyte.com/news-releases/news-release-details/incyte-announces-european-commission-approval-opzelurar (2023). Accessed 1 Feb 2024.
Rosmarin D, Soliman A, Li C. Real-world treatment patterns in patients with vitiligo in the United States. Dermatol Ther (Heidelb). 2023;13:2079–91.
Kubelis-López DE, Zapata-Salazar NA, Said-Fernández SL, et al. Updates and new medical treatments for vitiligo (review). Exp Ther Med. 2021;22:797.
Hamzavi IH, Bibeau K, Grimes P, et al. Exploring the natural and treatment history of vitiligo: perceptions of patients and healthcare professionals from the global VALIANT study. Br J Dermatol. 2023;189:569–77.
Anderson P, Benford M, Harris N, Karavali M, Piercy J. Real-world physician and patient behaviour across countries: disease-specific programmes–a means to understand. Curr Med Res Opin. 2008;24:3063–72.
Anderson P, Higgins V, Courcy J, et al. Real-world evidence generation from patients, their caregivers and physicians supporting clinical, regulatory and guideline decisions: an update on disease specific programmes. Curr Med Res Opin. 2023;39:1707–15.
Kitchen H, Wyrwich KW, Carmichael C, et al. Meaningful changes in what matters to individuals with vitiligo: content validity and meaningful change thresholds of the vitiligo area scoring index (VASI). Dermatol Ther (Heidelb). 2022;12:1623–37.
Acknowledgements
This secondary database analysis draws on data collected by Adelphi Real World, the DSP. AbbVie did not influence the original survey through either contribution to the design or questionnaires or data collection. AbbVie is one of multiple subscribers to the DSP; the analysis for this study was included in that subscription. Publication of survey results was not contingent on the subscriber’s approval or censorship of the abstract. We thank the participants included in this analysis.
Medical Writing Assistance
Medical writing services provided by Natalie Mitchell, of Fishawack Facilitate Ltd, part of Avalere Health, and funded by AbbVie.
Funding
This work was supported by AbbVie. AbbVie funded the Rapid Service and Open Access Fees.
Author information
Authors and Affiliations
Contributions
AbbVie participated in interpretation of data, review, and approval of the manuscript. All authors contributed to the development of the manuscript and maintained control over final content. No honoraria or payments were made for authorship.
Corresponding author
Ethics declarations
Conflict of Interest
David Rosmarin has consulted, spoken for, or conducted trials for AbbVie, Abcuro, AltruBio, Amgen, Arena, Boehringer Ingelheim, Bristol Meyers Squibb, Celgene, Concert, CSL Behring, Dermavant, Dermira, Galderma, Incyte, Janssen, Kyowa Kirin, Lilly, Merck, Nektar, Novartis, Pfizer, RAPT, Regeneron, Recludix, Revolo Biotherapeutics, Sanofi, Sun Pharmaceuticals, UCB, VielaBio, Zura Bio. Ahmed M. Soliman and Heidi S. Camp are full-time employees of AbbVie and may hold AbbVie stock and/or stock options or patents. Khaled Ezzedine declares acting as a consultant for Incyte, La Roche Posay, Pfizer, Pierre Fabre, Almirall, MSD, BMS, and AbbVie. Simran Marwaha, James Piercy, and Peter Anderson are employees of Adelphi Real World.
Ethical Approval
This analysis was conducted on existing de-identified data; therefore, the study team did not have access to any personal information on the patients or physicians and as such this study did not require ethics committee approval. As part of the DSP, patients were asked to complete a declaration page where they agreed to partake in the completion of the patient self-completion form in accordance with HIPAA and equivalent European Union guidelines. The DSP was submitted to the Pearl institutional review board. National data collection regulations were adhered to (European Society for Opinion and Market Research; US Department of Health and Human Services National Institutes of Health HIPAA; The Market Research Society; British Standards Institute).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Rosmarin, D., Soliman, A.M., Marwaha, S. et al. Disease Course, Treatment Patterns and Goals Among Patients with Non-segmental Vitiligo Across Europe and the United States. Dermatol Ther (Heidelb) 14, 1945–1957 (2024). https://doi.org/10.1007/s13555-024-01212-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-024-01212-1