
Abstract
Introduction
Vitiligo was historically regarded as a cosmetic disorder; however, it is an autoimmune disease. As a visible condition, it affects patient well-being. We assessed the impact of disease severity, lesion location, and body surface area (BSA) affected on patient health-related quality of life (HRQoL).
Methods
Retrospective data were from the Adelphi Real World Vitiligo Disease Specific Programme: a cross-sectional survey of physicians and their patients with vitiligo (10/2021–07/2022). Patient-reported outcomes were assessed by the Vitiligo-Specific Quality of Life Instrument (VitiQoL), Hospital Anxiety and Depression Scale (HADS), and EQ-5D-5L. The Work Productivity and Impairment Questionnaire (WPAI) questionnaire was used to assess disease-related impairment of daily activities. Data were stratified by physician-reported disease severity, presence/absence of vitiligo on the face, and BSA percentage affected.
Results
In total, 1388 patients were included. Mean (SD) VitiQoL, HADS depression, and anxiety scores were higher for those with severe disease [40.5 (26.1), 5.2 (4.4), and 6.8 (4.7)] than those with mild [24.8 (18.8), 3.6 (3.8), 4.2 (3.8)] or moderate [27.1 (22.6), 3.8 (4.5), 4.3 (4.4)] disease. Patients with face affected reported higher VitiQoL [30.0 (22.3) versus 23.2 (19.3)], and HADS scores [depression, 4.3 (4.3) versus 3.2 (3.9); anxiety, 5.0 (4.3) versus 3.8 (3.9)] than those without. Patients with ≥ 5% BSA affected had higher VitiQoL, depression and anxiety scores [27.9 (21.8), 4.0 (4.4), and 4.5 (4.2)] than those with 0–5% [24.6 (19.7), 3.4 (3.7), and 4.3 (4.1)]. Patients with severe vitiligo, facial lesions, or ≥ 5% BSA reported higher activity impairment. Mean EQ-5D-5L-utility score was approximately 0.9 regardless of disease severity or total BSA affected.
Conclusions
These data demonstrate the impact disease severity can have on HRQoL and daily activities for patients with vitiligo. Lesions that are more severe, on the face, or covering a greater BSA are more often associated with poorer outcomes and activity impairment. These data also highlight the potential insensitivity of commonly used HRQoL measures and a need for more sensitive disease-specific measures.
Plain Language Summary
Vitiligo is a disorder that causes patches of skin to lose pigment. In this study, we examined medical records of patients who have non-segmental vitiligo (the most common type of vitiligo) to better understand how the following factors affect the quality of life of patients with non-segmental vitiligo: (a) disease severity, (b) whether the face was affected, and (c) how much of the body was affected. Using a variety of measures, we found that patients with non-segmental vitiligo had lower quality of life, more symptoms of anxiety and depression, and higher activity impairment than those who did not. Our research highlights the differences in the measures used to assess the quality of life of patients, as well as the need for new therapies for non-segmental vitiligo.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Non-segmental vitiligo (NSV) is the most common type of vitiligo, which, along with the overt cosmetic effects on patients, is associated with stigmatization and psychological stress that may have a negative impact on their health-related quality of life (HRQoL). |
This study assessed the impact of disease severity, facial lesions, and body surface area (BSA) affected on HRQoL and work productivity for patients with NSV. |
What was learned from the study? |
This study found that patients with more severe or extensive NSV had lower HRQoL as measured by the Vitiligo-Specific Quality of Life Instrument (VitiQoL), more symptoms of anxiety and depression as measured by Hospital Anxiety and Depression (HADS) depression and anxiety scales, and higher activity impairment as measured by the Work Productivity and Impairment Questionnaire (WPAI). |
The EQ-5D-5L questionnaire demonstrated a statistically significant correlation between lowered HRQoL and the face being affected, but not severity and BSA affected. |
This study demonstrates the potential differences in sensitivity between HRQoL measures and reaffirms the need for new therapies. |
Introduction
Vitiligo is an autoimmune-related depigmentation disorder, with an estimated worldwide presence of 1.3% and a lifetime prevalence of 0.36% in the general population with the greatest lifetime prevalence observed in South Asia and Central Europe [1,2,3]. Vitiligo is characterized by clearly delineated, chalky-white macules and patches caused by the selective loss of functional melanocytes [2], and is classified into different subtypes, which may include segmental vitiligo (SV), non-segmental vitiligo (NSV), and universal vitiligo [4,5,6]. NSV, which presents in bilaterally and often symmetrical macules, accounts for 80–90% of vitiligo cases [7]. A multifactorial disorder, vitiligo is influenced by both hereditary and environmental factors [8], and while the exact cause is unknown, explanations include an autoimmune response that triggers the expression of cytokines, reactive oxygen species, and other proinflammation factors that attack melanocytes [9,10,11]. As a result, common treatments include corticosteroids and other immunosuppressants, along with phototherapy and surgical methods [12]. Calcineurin inhibitors, such as tacrolimus and pimecrolimus, are used as off-label treatments [13]; however, currently, there is only one medication, ruxolitinib, approved for NSV repigmentation in the US [14] and European Union (EU) [15].
Vitiligo has long been dismissed by some as a strictly cosmetic disorder, but along with having comorbidities with other autoimmune disorders [16], patients may experience physical symptoms including itch and increased risk of sunburn [17]. Most importantly, patients with vitiligo often experience stigmatization and psychological stress [18], affecting their daily lives, professional development, and emotional well-being [19]. Thus, patients with vitiligo are more likely to have depression and anxiety than patients without vitiligo [19]. These outcomes may be exacerbated by the severity of the condition [19, 20] or the location of lesions and may be associated with negative impacts on health-related quality of life (HRQoL) and work productivity [1, 18]. The objective of this study was to assess how disease severity, specific body area, and amount of body surface area (BSA) affected by vitiligo impact patient health-related quality of life and work productivity.
Methods
Overview of Study Design and Treatments
This study is a secondary data analysis that utilized data collected as part of the Adelphi Real World Vitiligo Disease Specific Programme (DSP) [21, 22] between October 2021 and July 2022. The DSP is a cross-sectional, multi-subscriber survey of physicians and their patients in the USA and the EU5 (France, Germany, Spain, Italy, and UK) designed to include retrospective data collection and provide impartial observations on real-world clinical practice from a physician-and-matched-patient viewpoint. While not designed to test any specific hypothesis nor to demonstrate cause and effect, the Vitiligo DSP is designed to provide a holistic understanding of NSV, including both physician attitudes towards treatment and management as well as patient clinical data.
Dermatologists who were actively managing patients with vitiligo were recruited from publicly available lists to ensure a geographically diverse sample. Physicians first completed a physician survey and subsequently a patient record form (PRF) for each of the next six consecutive adult patients with NSV. These patients were then invited to complete a patient self-completion form (PSC), which took approximately 15–20 min to complete. Completed forms were returned to the physician in a sealed envelope to ensure separation between patient and physician responses. To compare responses, physician and patient data collection forms were linked using a unique identifier code.
Ethics
Before participating in the DSP, patients and physicians completed a consent form where they agreed to partake in the completion of the PSC in accordance with the Health Insurance Portability and Accountability Act (HIPAA) [23] and equivalent EU guidelines [24,25,26]. The DSP fieldwork teams adhered to national data collection regulations and submitted the DSP methodology and fieldwork (including consent forms) to Pearl Institutional Review Board.
Eligibility Criteria
Eligible physicians were dermatologists who were actively involved in the management of NSV patients and maintained minimum weekly workload of at least five adults with NSV.
Eligible patients were ≥ 18 years of age, had a physician-confirmed diagnosis of NSV, and were not participating in an NSV clinical trial at the time of consultation.
Outcomes
Several patient-reported outcomes (PROs) were used to assess the full psychological disease burden and impact on patients with NSV. Outcomes were stratified by disease severity or body area affected to assess their impact on patient HRQoL and daily life. The Vitiligo-Specific Quality of Life Instrument (VitiQoL) [27] is a 16-item vitiligo-specific questionnaire scored on a 0–6 scale to assess the impact of vitiligo on HRQoL over the past month. The tool has a maximum score of 90, with higher scores representing worse outcomes. The Hospital Anxiety and Depression Scale (HADS) [28] is a two-subscale questionnaire used to assess symptoms of anxiety and depression over the previous week. Each subscale has a scoring range of 0–21, with higher scores representing worse anxiety and/or depression symptoms. The EuroQol 5-dimensional questionnaire (EQ-5D) [29], UK crosswalk value set [30], consists of a questionnaire that assesses the health status of patients using a descriptive system (EQ-5D-5L) with a scoring range of − 0.59 to 1 [31], where higher scores represent better quality of health. The Work Productivity and Impairment Questionnaire (WPAI) [32] questionnaire assesses impairment in ability to work and perform daily activities. Work time missed, impairment while working, overall work impairment, and overall activity impairment due to vitiligo over the previous week are reported as impairment percentages, with higher percentages corresponding to greater impairment. Patients completed the VitiQol, HADS, EQ-5D-5L, and WPAI questionnaires in the physician’s office without input from their physician. The completed questionnaires were returned to the physician in a sealed envelope to ensure that patient’s response remained anonymous.
Data Analysis
Descriptive statistics on patient demographics and clinical characteristics such as age, sex, ethnic origin, and skin phototype according to the Fitzpatrick scale [33] were collected and are reported overall and by disease severity groupings. Disease severity was assessed subjectively by the physician in response to the question “Currently, how would you describe the severity/extent of this patient’s vitiligo?” This approach was taken as it best represents how physicians would assess a patient’s vitiligo disease severity in real-world practice and gives a holistic view of the patient’s condition. Impact of vitiligo on HRQoL was evaluated by important disease features such as severity of disease (mild, moderate, severe), extent of disease (BSA 0–5%, > 5%), and location of lesions (facial, non-facial). Physician and patient collected data were linked at data processing using a unique identifier code so that comparisons could be conducted with physician- and patient-reported data. All PROs were stratified by subjective physician-reported disease severity (mild, moderate, and severe) and were compared by Bonferroni test. All PROs were also stratified by the presence of vitiligo on the face (affected or not affected) and percent of BSA affected (0–5% or ≥ 5%). These groups were compared by t test. Sample sizes were determined by feasibility, time to recruit, and availability of resources. Analyses were replicated across countries and combined into a pooled sample.
Results
Patient Population
Of the 1388 patients for whom a PRF was completed, 1028 (74.1%) were from the EU5 and 360 (25.9%) were from the USA. The mean [standard deviation (SD)] age of patients was 37.6 (14.3) years, and 695 (50.1%) were female. Mean (SD) duration since diagnosis was 4.0 (5.6) years.
At the time of survey administration, 756, 512, and 120 patients had mild, moderate, and severe vitiligo, respectively, as stated by their physician. Of the total 1388 patients, 492 were classified as having 0–5% BSA affected, whereas 896 patients had ≥ 5% affected. Slightly more than half of the total patient population (n = 751) were affected on the face. Various demographics including gender, ethnic origin, and Fitzpatrick skin phototype were comparable across disease severities, with age increasing slightly with increased severity (Table 1).
Outcomes
Disease Severity
As severity of vitiligo increased, PRO scores on most measures were higher, corresponding to worse HRQoL (Fig. 1). VitiQoL scores were higher for the severe subgroup compared with mild and moderate. VitiQoL (SD) mean scores for mild, moderate, and severe subgroups were as follows: 24.8 (18.8), 27.1 (22.6), and 40.5 (26.1), p = 0.0004, indicating worsening HRQoL with increasing severity of disease.

Patient-reported outcomes by severity subgroup. Labels represent mean (SD). EQ-5D-5L 5-level EuroQol 5-dimensional questionnaire, HADS Hospital Anxiety and Depression Scale, SD standard deviation, VitiQoL Vitiligo-Specific Quality of Life Instrument
The HADS anxiety score (SD) was significantly higher for the severe subgroup versus mild and moderate subgroups [6.8 (4.7) versus 4.2 (3.8) and 4.3 (4.4), respectively, p = 0.0036]. HADS depression scores (SD) were statistically similar at 3.6 (3.8), 3.8 (4.5), and 5.2 (4.4) for mild, moderate, and severe subgroups, respectively (p = 0.1524).
EQ-5D-5L UK crosswalk utility index scores (SD), in which a higher score corresponds to a better HRQoL, were 0.898 (0.177), 0.875 (0.196), and 0.864 (0.170), p = 0.3537, respectively, for mild, moderate, and severe subgroups.
Although there was not a statistically significant correlation between patient groups with regard to overall work impairment, work time missed, or impairment while working when stratified by disease severity, there was a correlation between severity and activity impairment [14.4 (18.6), 19.1 (21.5), and 19.7 (25.1) for mild, moderate, and severe subgroups, respectively, p = 0.042] (Fig. 2).

WPAI domains by severity subgroup. Labels represent mean (SD). SD standard deviation, WPAI Work Productivity and Activity Impairment Questionnaire
Facial Area Affected
Likewise, patients who experienced facial vitiligo reported worse outcomes on most HRQoL measures (Fig. 3). VitiQoL (SD) mean scores for those unaffected and affected on the face, respectively, were 23.2 (19.3) and 30.0 (22.3), p = 0.0009, respectively.

Patient-reported outcomes by face involvement. Labels represent mean (SD). EQ-5D-5L 5-level EuroQol 5-dimensional questionnaire, HADS Hospital Anxiety and Depression Scale, SD standard deviation, VitiQoL Vitiligo-Specific Quality of Life Instrument
HADS anxiety scores (SD) were 3.8 (3.9) and 5.0 (4.3) for those not affected on the face and affected on the face, respectively (p = 0.0036). HADS depression scores (SD) for those not affected on the face relative to those affected on the face were 3.2 (3.9) and 4.3 (4.3), p = 0.012. EQ-5D-5L UK crosswalk utility index value (SD) set levels demonstrated better scores for those not affected on the face compared to those who were affected, at 0.905 (0.160) and 0.871 (0.200), p = 0.0461, respectively.
Patients with vitiligo lesions on their face experienced greater activity impairment, 19.1 (21.20) versus 13.5 (18.8), p = 0.029, and no significant difference in the ability to work or work time missed (Fig. 4).

WPAI domains by face involvement. Labels represent mean (SD). SD standard deviation, WPAI Work Productivity and Activity Impairment Questionnaire
BSA Affected
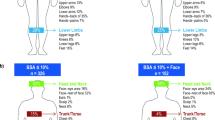
Regarding overall BSA affected, patients with > 5% of their body affected by vitiligo had higher VitiQoL (SD) mean scores than those with 0–5% of their body affected [27.9 (21.8) versus 24.6 (19.7), p = 0.1383, Fig. 5]. HADS anxiety scores (SD) were 4.5 (4.2) versus 4.3 (4.1), p = 0.678; HADS depression scores (SD) were 4.0 (4.4) and 3.4 (3.7), p = 0.2109; and EQ-5L-UK scores were 0.880 (0.192) versus 0.900 (0.165), p = 0.2739, for patients with > 5% versus 0–5% of their body affected by vitiligo.

Patient-reported outcomes by BSA affected. Labels represent mean (SD). BSA body surface area, EQ-5D-5L 5-level EuroQol 5-dimensional questionnaire, HADS Hospital Anxiety and Depression Scale, SD standard deviation, VitiQoL Vitiligo-Specific Quality of Life Instrument
Those who had > 5% BSA affected reported higher activity impairment than those with 0–5% [17.7 (21.1) versus 14.2 (18.5); p = 0.0818]; however, those with 0–5% BSA affected reported higher rates of overall work impairment, work time missed, and impairment while working than those with > 5% BSA affected, although not statistically significant (Fig. 6).

WPAI domains by BSA affected. Labels represent mean (SD). BSA body surface area, SD standard deviation, WPAI Work Productivity and Activity Impairment Questionnaire
Discussion
This study adds to the growing body of evidence that vitiligo has additional detrimental effects on HRQoL and daily activities for those affected outside of the overt cosmetic ramifications [1, 18,19,20]. Understanding the impact of vitiligo on HRQoL and daily activities in relation to disease severity and body areas affected by lesions may better inform healthcare professionals on treatment and management strategies.
Our data demonstrated that patients with more severe disease reported worse HRQoL, as evidenced by the higher mean VitiQoL scores, as well as greater anxiety and depressive symptoms, as reported among patients with severe relative to mild and moderate vitiligo. Our data also indicate that those with vitiligo on the face have worse HRQoL and more anxiety and depression symptoms based on PRO scores relative to those without vitiligo on the face, which is in line with previous studies [20, 34]. In addition, this study showed that patients with ≥ 5% BSA affected had numerically higher mean VitiQoL scores, aligning with previous studies reporting that those with > 5% of BSA affected have worse HRQoL than those with a smaller BSA affected [19, 35, 36]. Lastly, more severe vitiligo, vitiligo on the face, or greater than 5% BSA affected were associated with greater impairment in the ability to perform daily activities. Indeed, prior studies have also demonstrated that those with more visible vitiligo have encountered more stigma and are at greater risk for perceived embarrassment, affecting their social interactions and self-perceptions, both professionally [37] and personally [38]. Additionally, our data show that increasing levels of disease severity can cause incremental patient burden. Overall, these data indicate that patients affected with lesions that are more difficult to cover, whether due to extent or placement, are negatively impacted by their disease.
Along with disrupting patients’ lives, the reduced HRQoL results in a higher economic burden. One study reported more than a $10 million annual excess in costs from hospitalization of patients with vitiligo for mental health disturbances [39]. A second study assessing healthcare resource use and associated costs found that patients with vitiligo incur nearly $3500 in vitiligo-related costs per year (including costs for vitiligo-related treatments, medical claims, pharmacy costs, and total costs for related healthcare) and have nearly twice as much all-cause costs ($15,551 versus $7735) compared with those without vitiligo [40]. Autoimmune and psychiatric comorbidities associated with vitiligo have been shown to contribute to these higher costs [41], as patients with vitiligo who have these conditions tend to have more medical visits, including emergency room outpatient, and inpatient visits [40].
Interestingly, although the EQ-5D-5L utility scores do not demonstrate a statistically significant correlation between QoL and severity and BSA subgroups, the EQ-5D-5L utility score did demonstrate a modest correlation between lower QoL and the face being affected. However, the magnitude of the difference in EQ-5D-5L utility scores between patients with facial involvement compared to those without facial involvement was very small. On the other hand, the VitiQoL measure consistently and significantly reports worsening scores with increased disease severity among patients with vitiligo on their face and those with a greater BSA affected. The discrepancy between EQ-5D-5L compared with other PROs may indicate that EQ-5D-5L is less sensitive to assessing QoL in patients with vitiligo, and that other measurements that are disease-specific may prove more insightful. As EQ-5D-5L focuses on “mobility, self-care, usual activities, pain/discomfort, and anxiety/depression” [29], it is reasonable to conclude that it might not fully capture the extent to which issues like stigma and self-image affect patients’ HRQoL. This apparent discrepancy between QoL instruments was also observed in the VIOLIN study, conducted in France, in which vitiligo-specific assessments demonstrated larger QoL differences depending on lesion location and BSA affected than skin-specific assessments, such as Dermatology Life Quality Index (DLQI), with the least differences seen using general assessments such as the EQ-5D-5L [35]. Indeed, standardized assessment for examining QoL such as DLQI have previously been found to require modifications to adequately assess the disease burden of vitiligo [42], supporting the idea that these more generalized QoL instruments may not be sensitive enough to capture the impact of vitiligo. The use of more generalized patient assessments might partially explain the perception of vitiligo as a cosmetic disease and highlights the need for more consistent use of sensitive vitiligo-specific instruments such as the VitiQoL and the Vitiligo Patient Priority Outcome (ViPPO) measures [43] to fully capture the burden of disease on patients and clinical responses to treatments.
Strengths of the study include the use of the DSP, which is a published and validated methodology that provides physician–patient matched perspectives and uses local fieldwork agencies to account for potential variations in customs and practices. The large sample size and demographic diversity inside and outside of the USA represented in this study allow these conclusions to be broadened to outside a particular region or country. Also, the battery of PROs examined through various methodologies allows assessment of different aspects of the patient experience with vitiligo.
Although the DSP is a cross-sectional survey, this is not a limitation because the aim of this study was to describe the patient disease burden. However, there may be patient selection bias in that the participants in the DSP sample are the next eligible patients who consult the physician, making it more likely that patients who consult frequently have been included in the study; thus, this study may be more representative of the consulting, and not the overall population with vitiligo. Furthermore, the majority of patients sampled in this study were classified on the Fitzpatrick scale from I to III and therefore likely not representative of patients who have a darker skin phenotype and may consequently feel a greater disease burden [20]. Likewise, the geographical restriction to the USA and EU5 might limit the data, excluding cultures that may have long-standing historical stigmas surrounding vitiligo [18, 44].
Conclusions
For patients with vitiligo, increasing disease severity has increasing disease burden regarding HRQoL and daily activities. Lesions on the face are most often associated with activity and work impairment, along with poorer HRQoL. Patients with > 5% BSA affected had higher VitiQoL scores and higher activity impairment than those with 0–5% BSA affected. These data highlight the potential insensitivity of generic HRQoL measures and suggest that more sensitive disease-specific measures are needed while also emphasizing the need to access new emerging therapies.
Data Availability
All data generated or analyzed during this study were derived from the privately held Adelphi Real World Vitiligo Disease Specific Programme and are not publicly available.
References
Bibeau K, Pandya A, Ezzedine K, et al. Vitiligo prevalence and quality of life among adults in Europe, Japan and the USA. J Eur Acad Dermatol Venereol. 2022;36:1831–44.
Bergqvist C, Ezzedine K. Vitiligo: a review. Dermatology. 2020;236:571–92.
Akl J, Lee S, Ju HJ, et al. Estimating the burden of vitiligo: a systematic review and modelling study. Lancet Public health. 2024;Mar 26:S2468–2667(24)00026–4.
Ezzedine K, Lim HW, Suzuki T, et al. Revised classification/nomenclature of vitiligo and related issues: the Vitiligo Global Issues Consensus Conference. Pigment Cell Melanoma Res. 2012;25:E1–13.
van Geel N, Speeckaert R, Taïeb A, et al. Worldwide expert recommendations for the diagnosis and management of vitiligo: position statement from the International Vitiligo Task Force Part 1: towards a new management algorithm. J Eur Acad Dermatol Venereol. 2023;37:2173–84.
Eleftheriadou V, Atkar R, Batchelor J, et al. British Association of Dermatologists guidelines for the management of people with vitiligo 2021. Br J Dermatol. 2022;186:18–29.
AL-smadi K, Imran M, Leite-Silva VR, Mohammed Y. Vitiligo: a review of aetiology, pathogenesis, treatment, and psychosocial impact. Cosmetics. 2023;10:84.
Picardo M, Huggins R, Jones H, Marino R, Ogunsola M, Seneschal J. The humanistic burden of vitiligo: a systematic literature review of quality-of-life outcomes. J Eur Acad Dermatol Venereol. 2022;36:1507–23.
Baldini E, Odorisio T, Sorrenti S, et al. Vitiligo and autoimmune thyroid disorders. Front Endocrinol (Lausanne). 2017;8:290.
Eletto D, Chevet E, Argon Y, Appenzeller-Herzog C. Redox controls UPR to control redox. J Cell Sci. 2014;127:3649–58.
Boissy RE, Liu Y-Y, Medrano EE, Nordlund JJ. Structural aberration of the rough endoplasmic reticulum and melanosome compartmentalization in long-term cultures of melanocytes from vitiligo patients. J Invest Dermatol. 1991;97:395–404.
Bishnoi A, Parsad D. Clinical and molecular aspects of vitiligo treatments. Int J Mol Sci. 2018;19:1509.
Kubelis-López DE, Zapata-Salazar NA, Said-Fernández SL, et al. Updates and new medical treatments for vitiligo (review). Exp Ther Med. 2021;22:797.
Incyte. OPZELURA (ruxolitinib) Highlights of Prescribing Information. 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/215309s001lbl.pdf. Accessed Feb 14, 2024.
Incyte. Opzelura (ruxolitinib) 2023. https://www.ema.europa.eu/en/documents/overview/opzelura-epar-medicine-overview_en.pdf. Accessed Feb 14, 2024.
Hu Z, Wang T. Beyond skin white spots: vitiligo and associated comorbidities. Front Med. 2023;10:1072837.
Homan MWL, Spuls PI, de Korte J, Bos JD, Sprangers MA, van der Veen JW. The burden of vitiligo: patient characteristics associated with quality of life. J Am Acad Dermatol. 2009;61:411–20.
Parsad D, Dogra S, Kanwar AJ. Quality of life in patients with vitiligo. Health Qual Life Outcomes. 2003;1:58.
Bibeau K, Ezzedine K, Harris JE, et al. Mental health and psychosocial quality-of-life burden among patients with vitiligo: findings from the global VALIANT study. JAMA Dermatol. 2023;159:1124–8.
Grimes P, Miller M. Vitiligo: patient stories, self-esteem, and the psychological burden of disease. Int J Womens Dermatol. 2018;4:32–7.
Anderson P, Benford M, Harris N, Karavali M, Piercy J. Real-world physician and patient behaviour across countries: Disease-Specific Programmes–a means to understand. Curr Med Res Opin. 2008;24:3063–72.
Anderson P, Higgins V, de Courcy J, et al. Real-world evidence generation from patients, their caregivers and physicians supporting clinical, regulatory and guideline decisions: an update on Disease Specific Programmes. Curr Med Res Opin. 2023;39:1707–15.
US Department of Health. Summary of the HIPAA privacy rule. 2003. https://www.hhs.gov/hipaa/for-professionals/privacy/laws-regulations/index.html. Accessed Feb 14, 2024.
European Society for Opinion and Marketing Research. ICC/ESOMAR International Code on Market, Opinion and Social Research and Data Analytics. 2016. https://www.ipsos.com/sites/default/files/2017-11/ICCESOMAR_Code_English.pdf. Accessed Feb 14, 2024.
British Standards Institute. Standards. 2016. https://www.bsigroup.com/en-ID/Standards/. Accessed Feb 14, 2024.
Market Research Society. Code of conduct. 2019 https://www.mrs.org.uk/pdf/MRS-Code-of-Conduct-2019.pdf. Accessed Feb 14, 2024.
Lilly E, Lu PD, Borovicka JH, et al. Development and validation of a vitiligo-specific quality-of-life instrument (VitiQoL). J Am Acad Dermatol. 2013;69:e11–8.
Snaith RP. The Hospital Anxiety and Depression Scale. Health Qual Life Outcomes. 2003;1:29.
EuroQol Research Foundation. EQ-5D-5L user guide. 2019 https://euroqol.org/information-and-support/documentation/user-guides/. Accessed Feb 14, 2024.
van Hout B, Janssen MF, Feng YS, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15:708–15.
Garratt AM, Engen K, Kjeldberg IR, et al. Use of EQ-5D-5L for assessing patient-reported outcomes in a national register for specialized rehabilitation. Arch Phys Med Rehabil. 2024;105:40–8.
Reilly MC. Development of the work productivity and activity impairment (WPAI) questionnaire. New York: Reilly Associates; 2008.
Elmets CA, Lim HW, Stoff B, et al. Joint American Academy of Dermatology-National Psoriasis Foundation guidelines of care for the management and treatment of psoriasis with phototherapy. J Am Acad Dermatol. 2019;81:775–804.
Chen D, Tuan H, Zhou EY, Liu D, Zhao Y. Quality of life of adult vitiligo patients using camouflage: a survey in a Chinese vitiligo community. PLoS ONE. 2019;14:e0210581.
Ezzedine K, Seneschal J, Da Silva A, et al. Vitiligo patient population and disease burden in France: VIOLIN study results from the CONSTANCES cohort. J Eur Acad Dermatol Venereol. 2023;37(11):2249–58.
Tabassum S, Rahman A, Ghafoor R, et al. Quality of life index in patients with vitiligo. J Coll Physicians Surg Pak. 2023;33:521–7.
Krüger C, Schallreuter KU. Stigmatisation, avoidance behaviour and difficulties in coping are common among adult patients with vitiligo. Acta Derm Venereol. 2015;95:553–8.
Porter JR, Beuf AH, Lerner AB, Nordlund JJ. The effect of vitiligo on sexual relationships. J Am Acad Dermatol. 1990;22:221–2.
Patel KR, Singam V, Rastogi S, Lee HH, Silverberg NB, Silverberg JI. Association of vitiligo with hospitalization for mental health disorders in US adults. J Eur Acad Dermatol Venereol. 2019;33:191–7.
Ezzedine K, Soliman AM, Li C, Camp HS, Pandya AG. Economic burden among patients with vitiligo in the United States: a retrospective database claims study. J Invest Dermatol. 2024;144:540-46.e1.
Ezzedine K, Soliman AM, Li C, Camp HS, Pandya AG. Comorbidity burden among patients with vitiligo in the United States: a large-scale retrospective claims database analysis. Dermatol Ther (Heidelb). 2023:13(10):2265–77.
Yang TT, Lee CH, Lan CE. Impact of Vitiligo on life quality of patients: assessment of currently available tools. Int J Environ Res Publ Health. 2022;19:14943. https://doi.org/10.3390/ijerph192214943.
Kitchen H, Gandhi K, Carmichael C, et al. A qualitative study to develop and evaluate the content validity of the vitiligo patient priority outcome (ViPPO) measures. Dermatol Ther (Heidelb). 2022;12:1907–24.
Tsadik AG, Teklemedhin MZ, Mehari Atey T, Gidey MT, Desta DM. Public knowledge and attitudes towards vitiligo: a survey in Mekelle City. Northern Ethiopia Dermatol Res Pract. 2020;2020:3495165. https://doi.org/10.1155/2020/65.
Medical Writing and Editorial Assistance.
Medical writing services were provided by Nakeirah Christie, PhD, of Fishawack Facilitate Ltd, part of Avalere Health, and funded by AbbVie.
Funding
Data collection was undertaken by Adelphi Real World as part of an independent survey, entitled the Adelphi Real World Vitiligo DSP. AbbVie did not influence the original survey through either contribution to the design of questionnaires or data collection. The analysis described here used data from the Adelphi Real World Vitiligo DSP. The DSP is a wholly owned Adelphi Real World product. AbbVie is one of multiple subscribers to the DSP. AbbVie provided funding for the journal’s Rapid Service Fee for this publication.
Author information
Authors and Affiliations
Contributions
Substantial contributions to study conception and design: Ahmed Soliman, James Piercy, Peter Anderson, and Simran Marwaha. Data analysis: Ahmed M. Soliman, James Piercy, Simran Marwaha, and Peter Anderson. Data interpretation: David Rosmarin, Ahmed Soliman, James Piercy, Simran Marwaha, Peter Anderson, and Heidi Camp. Involved in drafting and critically reviewing the article for important intellectual content: David Rosmarin, Ahmed Soliman, James Piercy, Simran Marwaha, Peter Anderson, and Heidi Camp. All authors approved the final version of the article and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of Interest
David Rosmarin has consulted, spoken for, or conducted trials for the following companies: AbbVie, Abcuro, AltruBio, Amgen, Arena, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Concert, CSL Behring, Dermavant, Dermira, Galderma, Incyte, Janssen, Kyowa Kirin, Lilly, Merck, Nektar, Novartis, Pfizer, RAPT, Regeneron, Recludix, Revolo Biotherapeutics, Sanofi, Sun Pharmaceuticals, UCB, Viela Bio, Zura Bio. James Piercy, Simran Marwaha, and Peter Anderson are employees of Adelphi Real World and were contracted by AbbVie for this study. Ahmed M. Soliman and Heidi S. Camp are full-time employees of AbbVie and may hold AbbVie stock and/or stock options and patents.
Ethical Approval
Patients completed a declaration page where they agreed to partake in the completion of the PSC in accordance with HIPAA and equivalent EU guidelines. The DSP fieldwork teams adhered to national data collection regulations and submitted the DSP methodology and fieldwork (including consent forms) to Pearl Institutional Review Board.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Rosmarin, D., Soliman, A.M., Piercy, J. et al. Health-Related Quality of Life Burden Among Adults with Vitiligo: Relationship to Disease Severity and Disease Location. Dermatol Ther (Heidelb) 14, 1633–1647 (2024). https://doi.org/10.1007/s13555-024-01187-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-024-01187-z