
Abstract
Psoriasis is now considered a systemic disease, and several comorbidities have been described such as cardiovascular diseases, neurologic and psychiatric disorders, chronic inflammatory bowel disease, psoriatic arthritis, etc. Regarding cardiovascular comorbidities, major adverse cardiovascular events have been reported in psoriasis patients by multiple epidemiologic studies. Moreover, smoking, obesity, metabolic syndrome, hypertension, dyslipidemia, diabetes and reduced physical activity are associated with psoriasis, increasing cardiovascular risk. Consequently, several aspects should be considered when making the treatment decision. The aim of this review manuscript was to investigate the effectiveness and safety of biologic drugs acting on molecular mechanisms involved in the pathogenesis of psoriasis in preventing cardiovascular complications.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why carry out this study? |
Several cardiovascular risk factors such as smoking, obesity, metabolic syndrome, hypertension, dyslipidemia, diabetes and reduced physical activity are associated with psoriasis. |
Consequently, the cardiovascular risk should be considered during treatment decision-making. |
What was learned from the study? |
The pathogenetic mechanism regarding cardiovascular risk in psoriasis patients seems to have a complex nature. |
Our review highlighted the role of adipokines in psoriatic disease as well as the possible impact of systemic biologic drugs. |
Biologics seem to be safe and well tolerated, also with a cardioprotective role in some cases. |
Introduction
Psoriasis is a chronic inflammatory disease affecting up to 3% of the worldwide population [1]. Plaque psoriasis is the most common clinical form of the disease characterized by well-defined erythematous desquamative plaques covered by whitish or silvery scales, predominantly found on elbows, knees, the scalp and lumbar areas [2, 3]. Psoriasis is now considered a systemic disease, and several comorbidities have been described, such as cardiovascular diseases, neurologic and psychiatric disorders, chronic inflammatory bowel disease, psoriatic arthritis (PsA), etc. [2, 3]. Regarding cardiovascular comorbidities, major adverse cardiovascular events (MACEs) have been reported in psoriasis patients by multiple epidemiologic studies. For example, McDonald showed a 2.2 times higher risk associated with vascular diseases in patients with psoriasis than in controls with other dermatologic conditions [4]. Similarly, a higher prevalence of cardiovascular heart disease has been reported in North American psoriasis patients compared with general population (14.3% vs 11.3%) [5]. In particular, the association between coronary artery disease and psoriasis has been shown to be significant regardless of age and the presence or absence of diabetes, smoking or hypertension (OR 1.48, 95% CI 1.04–2.11, p = 0.03) [6]. Moreover, also the incidence of per 1000 person-years of myocardial infarction in patients with mild and severe psoriasis was higher compared with controls [4.04 (95% CI 3.88–4.21) vs 5.13 (95% CI 4.22–6.17) vs 3.58 (95% CI 3.52–3.65)] [7] as was the risk of stroke [8]. Finally, severe psoriasis seems to be associated with an increased risk of cardiovascular mortality independent of traditional cardiovascular risk factors [9].
Notably, traditional risk factors and metabolic abnormalities play a key role in the high cardiovascular burden in psoriasis patients, acting in a synergistic manner [10]. Finally, smoking, obesity, metabolic syndrome, hypertension, dyslipidemia, diabetes and reduced physical activity are associated with psoriasis [10]. However, all of these factors are associated with increased cardiovascular risk [10]. Therefore, several aspects should be considered during treatment decision-making.
The aim of this review article was to investigate the effectiveness and safety of biologic drugs acting on molecular mechanisms involved in psoriasis pathogenesis in preventing cardiovascular complications. This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Current Therapeutic Scenario of Psoriasis
Psoriasis treatment depends on its severity. Thus, adequate disease assessment plays a key role. Currently, several tools are used in clinical practice, also for special areas (e.g., nail psoriasis).
Globally, Psoriasis Area Severity Index (PASI) and body surface area (BSA) are the most used tools in clinical practice and clinical trials. Specifically, the PASI score evaluates both lesion severity and affected area, amalgamating them into a singular score from 0 (absence of disease) to 72 (most severe), with the body divided into four regions (head: 10%, arms: 20%, trunk: 30%, legs: 40%) and each area scored individually. These individual scores are then aggregated to yield the final PASI. Skin involvement for each region is assessed, graded from 0 (no involvement) to 6 (90–100% involvement), alongside severity measured via three clinical indicators ranging from 0 (none) to 4 (maximum): erythema (redness), induration (thickness) and desquamation (scaling). The cumulative severity parameter for each skin section is calculated, factoring in the respective area score and section weight (0.1 for head, 0.2 for arms, 0.3 for body and 0.4 for legs) [11].
Regarding BSA, it represents the average of affected skin surface [12]. Moderate-to-severe forms of psoriasis are defined when PASI and/or BSA is ≥ 10 or if PASI and/or BSA is < 10 but the disease involves the so-called “difficult-to-treat areas” (scalp, palmoplantar area, face, genitals, nails), strongly impacting patients’ quality of life [13]. In this context, Dermatology Life Quality of Life (DLQI) questionnaire, a simple, self-administered validated questionnaire, is essential to measure the health-related quality of life of adult patients suffering from a skin disease [14].
Globally, psoriasis management may be challenging, especially for moderate-to-severe forms of disease. Indeed, while mild psoriasis often responds well to topical therapies, systemic treatments become necessary for moderate-to-severe cases. Conventional systemic medications like cyclosporine, acitretin, methotrexate and fumarates are commonly used, but their usage is frequently restricted because of contraindications (such as cardiovascular disease, hepatic or renal failure, etc.) and the potential for adverse events (AEs) [15, 16]. For instance, cyclosporine is contraindicated in patients with hypertension and renal failure and can interact with other drugs. Acitretin is teratogenic and may affect lipid levels, while methotrexate can cause alterations in blood counts or liver enzymes, making them less suitable for patients with hepatic or hematologic comorbidities or those who are on multiple medications [17, 18].
Phototherapy is another option, but its use is hindered by logistical challenges as patients need to attend the phototherapy center three times a week. In recent years, biologic disease-modifying antirheumatic drugs (bDMARDs) and oral small molecules have transformed psoriasis management. They offer superior efficacy compared to conventional systemic treatments and generally have a better safety profile. Various classes of bDMARDs, including anti-tumor necrosis factor (TNF)-α (adalimumab, etanercept, infliximab, certolizumab), anti-interleukin (IL)-12/23 (ustekinumab), anti-IL-17s (brodalumab, ixekizumab, secukinumab, bimekizumab) and anti-IL-23s (guselkumab, risankizumab, tildrakizumab), have been approved for psoriasis management, delivering rapid and sustained clinical responses with relatively few AEs [17, 18]. Despite their overall safety, also during the COVID-19 pandemic [19,20,21], some factors need to be considered regarding bDMARDs before initiating treatment, such as the risk of reactivating latent tuberculosis infection (especially with anti-TNF and anti-IL-12/23 drugs) or triggering or worsening inflammatory bowel diseases (anti-IL-17 drugs) [15, 16]. Moreover, anti-TNF-α is contraindicated in patients with multiple sclerosis and advanced heart failure [15, 16].
Consequently, psoriasis comorbidities should be considered during treatment choice for both traditional and biologic systemic drugs [22].
Role of Adipokines in Psoriatic Disease
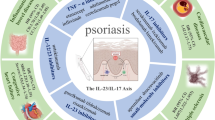
The term “adipokines” classifies all molecules produced by adipose tissue (AT) with endocrine, autocrine and paracrine signaling roles involved in numerous functions, including glucose homeostasis, neuromodulation and regulation of the immune system [23]. Those involved in the latter function are classified into pro- and anti-inflammatory. There is ample evidence that their altered expression may support inflammatory and autoimmune diseases. These include psoriasis, the pathogenesis of which has been partly but not fully elucidated, but there is evidence of a modulating role of adipokines in this disease [24]. The inflamed and scaly patches typical of psoriasis result from the uncontrolled proliferation and altered differentiation of keratinocytes, sustained by a modified interaction between innate and adaptive immunity in the skin. However, it is important to emphasize that the alterations in the keratinocytes themselves are not only the effect of the abnormal activity of T lymphocytes, but they are also key players in the mechanisms that determine psoriatic manifestations. The consequence of this is an inflammatory microenvironment where these two cell types support each other in what can be defined as a true inflammatory loop. Specifically, the early stages of the disease are characterized by the activation of dendritic cells, the antigen-presenting cells (APCs). Among the best-characterized mechanisms are antimicrobial peptides (AMPs), molecules secreted by keratinocytes in response to damage, presumably caused by endogenous and exogenous triggers. These form complexes with genetic material of damaged cells, such as cathelicidin LL-37, which stimulates plasmacytoid dendritic cells (pDC) via their Toll-like receptors (TLRs), followed by increased synthesis of type 1 interferon (IFN), such as IFN-α and IFN-β [25]. The latter activate myeloid dendritic cells to secrete tumor necrosis factor-α (TNF-α), interleukin-12 (IL-12) and IL-23, which in turn modulate the differentiation of T lymphocytes into T-helper 1 (Th1) and Th17, which secrete IFN-γ and IL-17 respectively. These, together with TNF-α, are the main cytokines responsible for the hyperproliferation of keratinocytes, which support the process by producing IL-1, IL-6 and TNF-α, AMPs and inflammatory chemokines [25]. Adipokines are also involved in this complex mechanism. For example, leptin, the most relevant of the proteins produced by AT, is increased in the serum of psoriasis patients compared to controls, and this also applies to the expression of its receptor [26]. Leptin promotes the development of psoriasis by increasing the secretion of the pro-inflammatory cytokines IL-1, IL-6, TNF, IL-23 and IL-17, supporting the differentiation of Th17 lymphocytes [24]. Adiponectin, on the other hand, is an anti-inflammatory protein whose blood levels are reduced in psoriasis. This results in increased production of IL-17 and IL-23, as adiponectin negatively correlates with IL-23 gene expression and inhibits IL-17 production [27, 28]. As adiponectin levels increased, a reduction in human beta-defensin2 (hBD2) in keratinocytes, a protein related to their proliferation and whose expression is stimulated by IL-23, was also observed [24]. Other adipokines involved in the pathogenesis of psoriasis include resistin. It increases the expression of TNF-α, IL-6 and IL-12, and according to a study by Boehncke et al., there is a positive relationship between the PASI of patients with psoriasis and the blood levels of resistin [29]. Chemerin is also involved in the mechanisms underlying psoriasis. In fact, this adipokine promotes the migration through the skin of chemokine-like receptor 1 (CMKLR1)-positive cells, including pDC, whose importance for the pathogenesis of psoriasis we have previously described [30]. Visfatin is another adipokine that several studies have shown to be involved in the onset of psoriasis. It induces TNF-α secretion by keratinocytes and is involved in the regulation of cell proliferation and apoptosis. Moreover, its blood levels are higher in psoriasis patients than in controls and correlate positively with PASI [24]. These are the adipokines for which more studies are reported in the literature in connection with psoriasis. However, further research is required to better characterize their mechanisms involved in this disease and to clarify the possible role of other adipokines. What is certain is that there is an increasing number of data in the literature describing the role of adipokines in cardiovascular disease. For example, high blood levels of leptin are associated with metabolic syndrome, hypertension and atherosclerosis, with increased risk of myocardial infarction and stroke. In addition, intravenous administration of leptin increases blood pressure and heart rate, probably through activation of the sympathetic nervous system [31]. In contrast, adiponectin is considered an anti-atherosclerotic protein and, although further studies are required to better clarify its position, low serum levels are correlated with hypertension and dyslipidemia [31]. For resistin, studies are more conflicting, but levels of this pro-inflammatory molecule correlate positively with the severity of heart failure according to the New York Heart Association (NYHA) classification [31]. Similarly, visfatin is also associated with cardiovascular disease; in particular, one study showed that its blood levels were significantly higher in patients with acute myocardial infarction with ST segment elevation (STEMI) than in controls and correlated positively with cardiac enzymes and thus with the extent of myocardial infarction [31].
Biologic Drugs and Cardiovascular Complications
The understanding of the molecular mechanisms underlying psoriasis has made it possible to introduce biologic drugs into the therapeutic armamentarium against this disease, which over the years have increased and offered more and more solutions for these patients. Since psoriasis is associated with several comorbidities that share some of these mechanisms, the question has always been raised as to whether treatment of the skin disease can reduce the risk of these comorbidities occurring. In particular, the aim of this review is to establish the role of currently approved target therapies for psoriasis in the prevention of cardiovascular disease, the association of which with psoriasis is clearly defined, with an increased incidence of major adverse cardiovascular events (MACE) [7]. The first class of biologic drugs to be approved for psoriasis was anti-TNF-α. Several studies on this class of drugs have evaluated their effects on the cardiovascular system. Wu and Poon observed that patients with psoriasis treated with anti-TNF had a reduced risk of myocardial infarction (hazard ratio 0.26) [32]. Hjuler et al. compared different parameters of coronary artery disease (CAD) between two groups of patients with severe psoriasis, of whom 28 were receiving biologic therapy (25 anti-TNF-α and 3 ustekinumab, an anti-IL-12 and 23) and 28 were controls. All parameters studied during the months of treatment remained stable, while progression of CAD was observed in the controls [33]. In addition, it was observed that treating a group of psoriasis patients with anti-TNF for 36 months improved lipidogram parameters, reduced blood levels of leptin and resistin and increased blood levels of adiponectin [34]. In more detail, etanercept has been shown to reduce blood levels of molecules underlying the mechanisms of psoriasis and atherosclerosis, such as CXCL10, CCL20 and IL-6, already after 4 weeks [35]. Furthermore, according to the findings of Di Minno et al., the cardioprotective effect of etanercept was expressed in improved hemostatic and fibrinolytic parameters compared to patients with active disease or receiving DMARD therapy and in lower levels of carotid intima-media thickness than the latter, a major subclinical marker of atherosclerosis [36]. Adalimumab has also demonstrated beneficial effects on cardiovascular risk factors. A reduction in serum levels of E-selectin and IL-22, biomarkers predictive of atherosclerosis, was observed in patients in whom PASI was significantly reduced after 12 weeks of adalimumab therapy [37]. Furthermore, according to Holzer et al., in psoriasis patients treated with adalimumab there was also a reduction in blood levels of C-reactive protein, a marker of systemic inflammation and predictor of MACE, which was generally higher in affected patients than in the healthy population [38]. In the same study, adalimumab-treated patients showed an improvement in flow-mediated dilation (FMD), a non-invasive measure of endothelial dysfunction, predictive of CVD [38]. Among the anti-TNF-α, an attenuation of inflammation at the level of endothelial cells, whose mechanisms underlie atherosclerosis, was also observed with the use of certolizumab pegol (CZP). In particular, an in vitro study on human aortic endothelial cells showed how TNF-α stimulation induced an increase in the expression of pro-inflammatory factors such as the adhesion molecules E-selectin, V-CAM and I-CAM and endothelial microparticles; contrarily, in cells exposed to TNF-α and CZP, these elements were reduced [39]. Although anti-TNF-α reduces the risk of CVD, it is currently contraindicated in NYHA class 3 or 4 congestive heart failure (CHF) [40]. Studies in this respect are controversial, as an increased risk of hospitalization or death from CHF with infliximab use has been reported, and case reports are published on the occurrence of CHF in patients who had received CZP and adalimumab therapy [41]. On the other hand, an RCT of 47 patients with CHF given etanercept showed significant improvements in left ventricular ejection fraction [41].
Finally, a retrospective cohort study, enrolling data from 8845 psoriasis/PsA patients (1673 received anti-TNF-α inhibitors for at least 2 months, 2097 were bionaïve and received other systemic agents or phototherapy and 5075 were untreated) showed that patients receiving anti-TNF-α inhibitors had approximately half the risk of developing myocardial infarction (hazard ratio [HR] 0.50; 95% CI 0.32–0.81) compared with psoriasis patients treated with topical agents [42]. Moreover, patients receiving TNF-α inhibitors experienced a 21% reduction in myocardial infarction risk compared with the oral or phototherapy group, although this was non-significant [42].
Ustekinumab is an IL-12 and IL-23 inhibitor approved for psoriasis. Initial studies seemed to show an increased risk of MACE associated with this drug but were soon disproved [40]. Contrarily, recent studies show that ustekinumab has a cardioprotective effect, as its use for 12 weeks reduces blood levels of several proteins elevated in psoriasis and associated with inflammation and cardiovascular risk, such as E-selectin, von Willebrand factor, IL-6 and myeloperoxidase [43]. Regarding adipokines, Onsun et al. observed that during 48 weeks of therapy blood levels of leptin, adiponectin and omentin were significantly higher in ustekinumab-treated patients than in anti-TNF-treated patients, although these values correlated positively with response rates to therapy [44].
Finally, a 12-week, phase IV, randomized double-blind placebo-controlled trial investigating the effect of ustekinumab on aortic vascular inflammation (AVI) in 43 patients affected by moderate-to-severe psoriasis (ustekinumab: 22; placebo: 21) showed that ustekinumab-treated patients had a − 18.65% (95% confidence interval = − 29.45 to − 7.85%) reduction in AVI, a reduction in inflammatory biomarkers and an increase in apolipoprotein B lipoproteins compared with placebo [45]. An extension of the study, crossing over all patients to ustekinumab, showed that at the end of 52 weeks of ustekinumab treatment, there was no change in AVI compared with baseline, inflammatory markers were reduced, and there were increases in selected measures of lipids and leptin [45]. To sum up, this trial showed that the blockade of IL-12 and/or IL-23 may transiently reduce AVI, with more durable reduction in inflammatory cytokines associated with cardiovascular disease [45].
The impact of anti-IL-17 on cardiovascular risk prevention is not yet fully clarified and further studies are required. We do know that a randomized, double-blind, placebo-controlled multicenter study in adult psoriasis patients treated with secukinumab showed the drug's neutrality at week 25 on aortic vascular inflammation and CVD biomarkers, including the adipokines, leptin and adiponectin [46]. In contrast, the CARIMA study, also placebo-controlled, observed that at week 52 the FMD of patients receiving secukinumab was significantly higher than in the placebo group [47]. However, a pooled analysis of ten phase II and III studies of patients with psoriasis in 3430 patients treated with secukinumab observed an incidence of MACE at 52 weeks of treatment between 0.35 and 0.42/100 patient years (PYs), comparable to that of etanercept [48]. Regarding ixekizumab, the results from the UNCOVER-1, -2 and -3 RCTs showed that patients with psoriasis treated with this drug for 60 weeks did not undergo any alterations in cardiovascular-related parameters and were comparable to those receiving placebo, thus establishing the neutrality of ixekizumab regarding these parameters [49]. Furthermore, no MACEs were reported from the RCT UNCOVER-1 among > 800 patients treated with ixekizumab or placebo [50]. Another review of 17 clinical trials and > 18,000 PYs of psoriasis patients treated with ixekizumab described a MACE incidence of 0.5 per 100 PY, with non-fatal myocardial infarction and non-fatal stroke as the most frequent events [51]. Notably, a case report from 2020 described a 58-year-old patient with psoriasis who had recently started ixekizumab and presented with acute-onset HF. Subsequent investigations led to the diagnosis of cardiac sarcoidosis. The drug was subsequently discontinued, with following resolution of the condition and restoration of normal ejection fraction [52]. Concerning bimekizumab, the most recent anti-IL-17 approved for psoriasis, there is still a lack of data in relation to CVD. Data from two RCTs on the use of bimekizumab in patients with axial spondyloarthritis have been published jointly, with no MACEs reported [53]. An Italian multicenter study evaluated the efficacy and safety of the drug in psoriasis, reporting no serious adverse events or events leading to discontinuation of bimekizumab [54].
Anti-IL-23s are the latest class of biologics approved for moderate-to-severe psoriasis. The first among them is guselkumab for which we have a 3-year retrospective real-life study available, where out of the 31 patients who completed the study, no MACEs were reported [55]. A more recent analysis of 11 phase II/III clinical trials on the use of guselkumab for a total period of 856 PYs showed that among 2257 patients receiving the drug, the incidence of MACEs was 0.35 PYs, comparable to 0.25 PYs among 1061 patients receiving placebo [56]. Regarding cardiovascular risk factors, dyslipidemia, weight gain and impaired glucose metabolism are not reported with the use of guselkumab [57]. UltIMMa-1 and UltIMMa-2 are two 52-week RCTs that compared efficacy and safety of risankizumab, another anti-IL-23, and ustekinumab. Among the 598 total patients who received risankizumab, the incidence of MACE was < 1% [58]. Subsequently, Gordon et al. evaluated the safety of risankizumab over 17 clinical trials, inferring a MACE incidence of 0.3 PYs among 3072 patients evaluated over the long term [59]. Regarding tildrakizumab, the third IL-23 inhibitor approved for psoriasis, data extrapolated from the reSURFACE-1 and -2 trials and their 1-year extension periods show that the safety profile of this drug regarding cardiovascular events is comparable to that of the placebo and etanercept groups [60]. Subsequently, a 5-year evaluation of the same trials was performed, in which the incidence of MACEs was 0.6 and 0.9 PYs for those taking tildrakizumab 100 mg and 200 mg, respectively, with a number needed to harm (NNH) of 355 with 1 year of tildrakizumab 200 mg and negative with the 100 mg [61]. Finally, Cacciapuoti et al. published preliminary results of a single-center real-life study in which they attested that the pro-inflammatory adipokines leptin and resistin were significantly reduced in patients who were fast responders to tildrakizumab 100 mg, but not in slow responders, suggesting a possible role of the drug on adipokine levels [62].
In addition to biologic drugs, another category of drugs, small molecules, has been approved for psoriasis. These include apremilast, an inhibitor of phosphodiesterase-4 (PDE-4), an intracellular enzyme that functions to degrade cyclic AMP (cAMP) and reduces the expression of pro-inflammatory cytokines, such as IL-23 and TNFα, and increases anti-inflammatory cytokines, such as IL-10 [57]. Some beneficial effects of this drug on cardiovascular risk factors have been demonstrated, such as the approximately 5% reduction in body weight observed in 22% of patients or the increase in insulin production [57]. These data were substantially confirmed in a study by Gelfand et al. where they also observed improvement in some cardiometabolic markers at 16 and 52 weeks of treatment, with, for example, reductions in leptin, IL-1b, IL-17 and triglycerides [63]. Regarding MACEs, Vegas et al. noted that out of 1885 patients observed over 4 years and taking apremilast, 0.4% experienced this type of event, with risk that was not significantly different from those taking anti-TNF-α [64].
Finally, a recent cohort study investigating the association of biologic therapy with coronary inflammation in patients with psoriasis, assessed by the perivascular fat attenuation index (an imaging biomarker which evaluates the coronary inflammation by mapping spatial changes of perivascular fat composition via coronary computed tomography angiography), showed that biologic treatment for moderate-to-severe psoriasis was associated with reduced coronary inflammation [65]. In particular, 134 patients were enrolled. Of these, 82 received biologics (anti–TNF-α, anti–IL-12/23 or anti–IL-17) for 1 year, whereas 52 did not receive any biologic therapy (control group) [65]. This study showed that biologic treatment was significantly associated with a decrease in coronary inflammation. Moreover, a subgroup analysis showed a similar association with each biologic therapy [65].
The latest drug approved for psoriasis is deucravacitinib, an oral tyrosine kinase 2 inhibitor. Current data do not indicate an increased risk of MACEs with this drug, as observed in an RCT of 203 patients with PsA treated with the drug at week 16 where no thromboembolic events occurred [66]. A review by Jin et al. of three phase II and III RCTs showed no cardiovascular events or significant changes in blood levels [67]. A study by Chimalakonda et al. also showed no electrocardiographic changes in patients with psoriasis taking deucravacitinib 12 mg or 36 mg [68]. However, further studies are needed to clarify the relationship of this drug with cardiovascular risk factors.
Conclusion
The pathogenetic mechanism correlating cardiovascular disease in psoriasis patients seems to have a complex nature. On one hand, the atherosclerosis development may be related to the presence of atherosclerotic risk factors as well as of a chronic inflammatory state. Flammer et al. proposed the “two plaques for one syndrome” theory because of the similar molecular mechanisms and pro-inflammatory cytokines in psoriatic lesions and atherosclerotic ones, characterized by a comparable inflammatory infiltrate of T cells, macrophages and monocytes [69].
In this context, our review highlighted the role of adipokines in psoriatic disease as well as the possible impact of systemic drugs. It is well known that conventional systemic treatments for psoriasis should be used with caution in patients with cardiovascular risk (e.g., acitretin can increase the value of triglycerides and cholesterol, and cyclosporine may alter blood pressure) whereas methotrexate has a cardioprotective effect. In this context, biologics seems to be safe and well tolerated [70, 71], also with a cardioprotective role in some cases.
Thus, cardiovascular risk should be considered during treatment choice to offer patients a tailored and personalized approach [72], also considering the possible protective role of biologics in the prevention of cardiovascular comorbidities.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
References
Boehncke WH, Schön MP. Psoriasis. Lancet (London, England). 2015;386(9997):983–94. https://doi.org/10.1016/S0140-6736(14)61909-7.
Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet (London, England). 2007;370(9583):263–71. https://doi.org/10.1016/S0140-6736(07)61128-3.
Kamiya K, Kishimoto M, Sugai J, Komine M, Ohtsuki M. Risk factors for the development of psoriasis. Int J Mol Sci. 2019. https://doi.org/10.3390/ijms20184347.
McDonald CJ, Calabresi P. Occlusive vascular disease in psoriatic patients. N Engl J Med. 1973;288(17):912.
Pearce DJ, Morrison AE, Higgins KB, et al. The comorbid state of psoriasis patients in a university dermatology practice. J Dermatol Treat. 2005;16(5–6):319–23. https://doi.org/10.1080/09546630500335977.
Masson W, Galimberti ML, Anselmi CL, Cagide A, Galimberti RL. Coronary artery disease in patients with psoriasis. Medicina (B Aires). 2013;73(5):423–7.
Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB. Risk of myocardial infarction in patients with psoriasis. JAMA. 2006;296(14):1735–41. https://doi.org/10.1001/jama.296.14.1735.
Kimball AB, Guerin A, Latremouille-Viau D, et al. Coronary heart disease and stroke risk in patients with psoriasis: retrospective analysis. Am J Med. 2010;123(4):350–7. https://doi.org/10.1016/j.amjmed.2009.08.022.
Mehta NN, Azfar RS, Shin DB, Neimann AL, Troxel AB, Gelfand JM. Patients with severe psoriasis are at increased risk of cardiovascular mortality: cohort study using the General Practice Research Database. Eur Heart J. 2010;31(8):1000–6. https://doi.org/10.1093/eurheartj/ehp567.
Masson W, Lobo M, Molinero G. Psoriasis and cardiovascular risk: a comprehensive review. Adv Ther. 2020;37(5):2017–33. https://doi.org/10.1007/s12325-020-01346-6.
Mattei PL, Corey KC, Kimball AB. Psoriasis Area Severity Index (PASI) and the Dermatology Life Quality Index (DLQI): the correlation between disease severity and psychological burden in patients treated with biological therapies. J Eur Acad Dermatol Venereol. 2014;28(3):333–7. https://doi.org/10.1111/jdv.12106.
Fernández-Torres RM, Paradela S, Fonseca E. Long-term response to etanercept monotherapy in moderate to severe psoriasis: assessment in daily practice by the maintenance of low values of PASI and BSA. J Dermatol Treat. 2014;25(1):54–6. https://doi.org/10.3109/09546634.2012.755254.
Gisondi P, Fargnoli MC, Amerio P, et al. Italian adaptation of EuroGuiDerm guideline on the systemic treatment of chronic plaque psoriasis. Ital J Dermatol Venereol. 2022;157(Suppl. 1 to No. 1):1–78. https://doi.org/10.23736/S2784-8671.21.07132-2.
Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)—a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210–6. https://doi.org/10.1111/j.1365-2230.1994.tb01167.x.
Nast A, Smith C, Spuls PI, et al. EuroGuiDerm guideline on the systemic treatment of Psoriasis vulgaris—part 1: treatment and monitoring recommendations. J Eur Acad Dermatol Venereol. 2020;34(11):2461–98. https://doi.org/10.1111/jdv.16915.
Nast A, Smith C, Spuls PI, et al. EuroGuiDerm guideline on the systemic treatment of Psoriasis vulgaris—part 2: specific clinical and comorbid situations. J Eur Acad Dermatol Venereol. 2021;35(2):281–317. https://doi.org/10.1111/jdv.16926.
Megna M, Camela E, Battista T, et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part I: focus on pediatric patients. Expert Opin Drug Saf. 2023;22:1–17 (Published online February).
Megna M, Camela E, Battista T, et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations Part II: focus on elderly patients. Expert Opin Drug Saf. 2023;22:1–16 (Published online February).
Megna M, Potestio L, Battista T, et al. Immune response to COVID-19 mRNA vaccination in psoriasis patients undergoing treatment with biologics. Clin Exp Dermatol. 2022. https://doi.org/10.1111/ced.15395.
Martora F, Villani A, Battista T, Fabbrocini G, Potestio L. COVID-19 vaccination and inflammatory skin diseases. J Cosmet Dermatol. 2023;22(1):32–3. https://doi.org/10.1111/jocd.15414.
Martora F, Fabbrocini G, Marasca C. Pityriasis rosea after Moderna mRNA-1273 vaccine: a case series. Dermatol Ther. 2022;35(2): e15225. https://doi.org/10.1111/dth.15225.
Camela E, Potestio L, Fabbrocini G, Pallotta S, Megna M. The holistic approach to psoriasis patients with comorbidities: the role of investigational drugs. Expert Opin Investig Drugs. 2023. https://doi.org/10.1080/13543784.2023.2219387.
Giardullo L, Corrado A, Maruotti N, Cici D, Mansueto N, Cantatore FP. Adipokine role in physiopathology of inflammatory and degenerative musculoskeletal diseases. Int J Immunopathol Pharmacol. 2021;35:20587384211015030. https://doi.org/10.1177/20587384211015034.
Kiełbowski K, Bakinowska E, Ostrowski P, et al. The role of adipokines in the pathogenesis of psoriasis. Int J Mol Sci. 2023. https://doi.org/10.3390/ijms24076390.
Rendon A, Schäkel K. Psoriasis pathogenesis and treatment. Int J Mol Sci. 2019. https://doi.org/10.3390/ijms20061475.
Zhu KJ, Zhang C, Li M, Zhu CY, Shi G, Fan YM. Leptin levels in patients with psoriasis: a meta-analysis. Clin Exp Dermatol. 2013;38(5):478–83. https://doi.org/10.1111/ced.12171.
Kochumon S, Hasan A, Al-Rashed F, et al. Increased adipose tissue expression of IL-23 associates with inflammatory markers in people with high LDL cholesterol. Cells. 2022. https://doi.org/10.3390/cells11193072.
Shibata S, Tada Y, Hau CS, et al. Adiponectin regulates psoriasiform skin inflammation by suppressing IL-17 production from γδ-T cells. Nat Commun. 2015;6:7687. https://doi.org/10.1038/ncomms8687.
Boehncke S, Thaci D, Beschmann H, et al. Psoriasis patients show signs of insulin resistance. Br J Dermatol. 2007;157(6):1249–51. https://doi.org/10.1111/j.1365-2133.2007.08190.x.
Albanesi C, Scarponi C, Pallotta S, et al. Chemerin expression marks early psoriatic skin lesions and correlates with plasmacytoid dendritic cell recruitment. J Exp Med. 2009;206(1):249–58. https://doi.org/10.1084/jem.20080129.
Smekal A, Vaclavik J. Adipokines and cardiovascular disease: a comprehensive review. Biomed Pap Med Fac Univ Palacky Olomouc Czechoslov. 2017;161(1):31–40. https://doi.org/10.5507/bp.2017.002.
Wu JJ, Poon KYT. Tumor necrosis factor inhibitor therapy and myocardial infarction risk in patients with psoriasis, psoriatic arthritis, or both. J Drugs Dermatol. 2014;13(8):932–4.
Hjuler KF, Bøttcher M, Vestergaard C, Bøtker HE, Iversen L, Kragballe K. Association between changes in coronary artery disease progression and treatment with biologic agents for severe psoriasis. JAMA Dermatol. 2016;152(10):1114–21. https://doi.org/10.1001/jamadermatol.2016.1984.
Olejniczak-Staruch I, Narbutt J, Ceryn J, et al. AntiTNF-alpha therapy normalizes levels of lipids and adipokines in psoriatic patients in the real-life settings. Sci Rep. 2021;11(1):9289. https://doi.org/10.1038/s41598-021-88552-6.
Kim J, Tomalin L, Lee J, et al. Reduction of inflammatory and cardiovascular proteins in the blood of patients with psoriasis: differential responses between tofacitinib and etanercept after 4 weeks of treatment. J Investig Dermatol. 2018;138(2):273–81. https://doi.org/10.1016/j.jid.2017.08.040.
Di Minno MND, Iervolino S, Zincarelli C, et al. Cardiovascular effects of Etanercept in patients with psoriatic arthritis: evidence from the cardiovascular risk in rheumatic diseases database. Expert Opin Drug Saf. 2015;14(12):1905–13. https://doi.org/10.1517/14740338.2015.1111870.
Gkalpakiotis S, Arenbergerova M, Gkalpakioti P, Potockova J, Arenberger P, Kraml P. Impact of adalimumab treatment on cardiovascular risk biomarkers in psoriasis: results of a pilot study. J Dermatol. 2017;44(4):363–9. https://doi.org/10.1111/1346-8138.13661.
Holzer G, Hoke M, Sabeti-Sandor S, et al. Disparate effects of adalimumab and fumaric acid esters on cardiovascular risk factors in psoriasis patients: results from a prospective, randomized, observer-blinded head-to-head trial. J Eur Acad Dermatol Venereol. 2021;35(2):441–9. https://doi.org/10.1111/jdv.16635.
Heathfield SK, Parker B, Zeef LAH, Bruce IN, Alexander MY. Certolizumab pegol attenuates the pro-inflammatory state in endothelial cells in a manner that is atheroprotective. Clin Exp Rheumatol. 2013;31(2):225–33.
Kaushik SB, Lebwohl MG. Psoriasis: Which therapy for which patient: Psoriasis comorbidities and preferred systemic agents. J Am Acad Dermatol. 2019;80(1):27–40. https://doi.org/10.1016/j.jaad.2018.06.057.
Jiang Y, Chen Y, Yu Q, Shi Y. Biologic and small-molecule therapies for moderate-to-severe psoriasis: focus on psoriasis comorbidities. BioDrugs. 2023;37(1):35–55. https://doi.org/10.1007/s40259-022-00569-z.
Famenini S, Sako EY, Wu JJ. Effect of treating psoriasis on cardiovascular co-morbidities: focus on TNF inhibitors. Am J Clin Dermatol. 2014;15(1):45–50. https://doi.org/10.1007/s40257-013-0052-6.
Koschitzky M, Navrazhina K, Garshick MS, et al. Ustekinumab reduces serum protein levels associated with cardiovascular risk in psoriasis vulgaris. Exp Dermatol. 2022;31(9):1341–51. https://doi.org/10.1111/exd.14582.
Onsun N, Akaslan TÇ, Sallahoglu K, Gülcan AS, Bulut H, Yabacı A. Effects of TNF inhibitors and an IL12/23 inhibitor on changes in body weight and adipokine levels in psoriasis patients: a 48-week comparative study. J Dermatol Treat. 2022;33(3):1727–32. https://doi.org/10.1080/09546634.2021.1901845.
Gelfand JM, Shin DB, Alavi A, et al. A phase IV, randomized, double-blind, placebo-controlled crossover study of the effects of ustekinumab on vascular inflammation in psoriasis (the VIP-U Trial). J Invest Dermatol. 2020;140(1):85-93.e2. https://doi.org/10.1016/j.jid.2019.07.679.
Gelfand JM, Shin DB, Duffin KC, et al. A randomized placebo-controlled trial of secukinumab on aortic vascular inflammation in moderate-to-severe plaque psoriasis (VIP-S). J Investig Dermatol. 2020;140(9):1784-1793.e2. https://doi.org/10.1016/j.jid.2020.01.025.
von Stebut E, Reich K, Thaçi D, et al. Impact of secukinumab on endothelial dysfunction and other cardiovascular disease parameters in psoriasis patients over 52 weeks. J Investig Dermatol. 2019;139(5):1054–62. https://doi.org/10.1016/j.jid.2018.10.042.
Lockshin B, Balagula Y, Merola JF. Interleukin 17, inflammation, and cardiovascular risk in patients with psoriasis. J Am Acad Dermatol. 2018;79(2):345–52. https://doi.org/10.1016/j.jaad.2018.02.040.
Egeberg A, Wu JJ, Korman N, et al. Ixekizumab treatment shows a neutral impact on cardiovascular parameters in patients with moderate-to-severe plaque psoriasis: results from UNCOVER-1, UNCOVER-2, and UNCOVER-3. J Am Acad Dermatol. 2018;79(1):104-109.e8. https://doi.org/10.1016/j.jaad.2018.02.074.
Rungapiromnan W, Yiu ZZN, Warren RB, Griffiths CEM, Ashcroft DM. Impact of biologic therapies on risk of major adverse cardiovascular events in patients with psoriasis: systematic review and meta-analysis of randomized controlled trials. Br J Dermatol. 2017;176(4):890–901. https://doi.org/10.1111/bjd.14964.
Griffiths CEM, Gooderham M, Colombel JF, et al. Safety of ixekizumab in adult patients with moderate-to-severe psoriasis: data from 17 clinical trials with over 18,000 patient-years of exposure. Dermatol Ther (Heidelb). 2022;12(6):1431–46. https://doi.org/10.1007/s13555-022-00743-9.
Hatipoglu D, Tanski C, Hachamovitch R, Legha S, Moudgil R. Ixekizumab-induced cardiac sarcoidosis: a case report. CJC open. 2021;3(1):118–20. https://doi.org/10.1016/j.cjco.2020.08.012.
van der Heijde D, Deodhar A, Baraliakos X, et al. Efficacy and safety of bimekizumab in axial spondyloarthritis: results of two parallel phase 3 randomised controlled trials. Ann Rheum Dis. 2023;82(4):515–26. https://doi.org/10.1136/ard-2022-223595.
Gargiulo L, Narcisi A, Ibba L, et al. Effectiveness and safety of bimekizumab for the treatment of plaque psoriasis: a real-life multicenter study-IL PSO (Italian landscape psoriasis). Front Med. 2023;10:1243843. https://doi.org/10.3389/fmed.2023.1243843.
Megna M, Potestio L, Fabbrocini G, Ruggiero A. Long-term efficacy and safety of guselkumab for moderate to severe psoriasis: a 3-year real-life retrospective study. Psoriasis (Auckland, NZ). 2022;12:205–12. https://doi.org/10.2147/PTT.S372262.
Strober B, Coates LC, Lebwohl MG, et al. Long-term safety of guselkumab in patients with psoriatic disease: an integrated analysis of eleven phase II/III clinical studies in psoriasis and psoriatic arthritis. Drug Saf. 2024;47(1):39–57. https://doi.org/10.1007/s40264-023-01361-w.
Chiricozzi A, Gisondi P, Girolomoni G. The pharmacological management of patients with comorbid psoriasis and obesity. Expert Opin Pharmacother. 2019;20(7):863–72. https://doi.org/10.1080/14656566.2019.1583207.
Crowley JJ, Warren RB, Cather JC. Safety of selective IL-23p19 inhibitors for the treatment of psoriasis. J Eur Acad Dermatol Venereol. 2019;33(9):1676–84. https://doi.org/10.1111/jdv.15653.
Gordon KB, Lebwohl M, Papp KA, et al. Long-term safety of risankizumab from 17 clinical trials in patients with moderate-to-severe plaque psoriasis. Br J Dermatol. 2022;186(3):466–75. https://doi.org/10.1111/bjd.20818.
Bissonnette R, Fernández-Peñas P, Puig L, Mendelsohn AM, Rozzo SJ, Menter A. Incidence of cardiovascular events among tildrakizumab-treated patients with moderate-to-severe plaque psoriasis: pooled data from three large randomised clinical trials. J Eur Acad Dermatol Venereol. 2020;34(1):e21–4. https://doi.org/10.1111/jdv.15866.
Egeberg A, Jullien D, GaarnDuJardin K, Thaçi D. Five-year safety of tildrakizumab in patients with moderate-to-severe psoriasis from two phase 3 trials (reSURFACE 1 and reSURFACE 2): number needed to harm for occurrence of adverse events of special interest. J Dermatol Treat. 2023;34(1):2220447. https://doi.org/10.1080/09546634.2023.2220447.
Cacciapuoti S, Megna M, Salza E, Potestio L, Caiazzo G. The effect of tildrakizumab on adipokines production in patients affected by psoriasis and obesity: preliminary results from a single center real-life study. J Dermatol Treat. 2024;35(1):2291323. https://doi.org/10.1080/09546634.2023.2291323.
Gelfand JM, Shin DB, Armstrong AW, et al. Association of apremilast with vascular inflammation and cardiometabolic function in patients with psoriasis: the VIP-A phase 4, open-label, nonrandomized clinical trial. JAMA Dermatol. 2022;158(12):1394–403. https://doi.org/10.1001/jamadermatol.2022.3862.
Pina Vegas L, Le Corvoisier P, Penso L, Paul M, Sbidian E, Claudepierre P. Risk of major adverse cardiovascular events in patients initiating biologics/apremilast for psoriatic arthritis: a nationwide cohort study. Rheumatology (Oxford). 2022;61(4):1589–99. https://doi.org/10.1093/rheumatology/keab522.
Elnabawi YA, Oikonomou EK, Dey AK, et al. Association of biologic therapy with coronary inflammation in patients with psoriasis as assessed by perivascular Fat Attenuation Index. JAMA Cardiol. 2019;4(9):885–91. https://doi.org/10.1001/jamacardio.2019.2589.
Megna M, Potestio L, Ruggiero A, et al. JAK inhibitors in psoriatic disease. Clin Cosmet Investig Dermatol. 2023;16:3129–45. https://doi.org/10.2147/CCID.S433367.
Jin JQ, Spencer RK, Reddy V, Bhutani T, Liao W. Clinical utility of deucravacitinib for the management of moderate to severe plaque psoriasis. Ther Clin Risk Manag. 2023;19:413–23. https://doi.org/10.2147/TCRM.S388324.
Chimalakonda A, Singhal S, Darbenzio R, et al. Lack of electrocardiographic effects of deucravacitinib in healthy subjects. Clin Pharmacol Drug Dev. 2022;11(4):442–53. https://doi.org/10.1002/cpdd.1056.
Flammer AJ, Ruschitzka F. Psoriasis and atherosclerosis: two plaques, one syndrome? Eur Heart J. 2012;33(16):1989–91. https://doi.org/10.1093/eurheartj/ehr425.
Roubille C, Richer V, Starnino T, et al. The effects of tumour necrosis factor inhibitors, methotrexate, non-steroidal anti-inflammatory drugs and corticosteroids on cardiovascular events in rheumatoid arthritis, psoriasis and psoriatic arthritis: a systematic review and meta-analysis. Ann Rheum Dis. 2015;74(3):480–9. https://doi.org/10.1136/annrheumdis-2014-206624.
Gisondi P, Fostini AC, Fossà I, Girolomoni G, Targher G. Psoriasis and the metabolic syndrome. Clin Dermatol. 2018;36(1):21–8. https://doi.org/10.1016/j.clindermatol.2017.09.005.
Camela E, Potestio L, Fabbrocini G, Ruggiero A, Megna M. New frontiers in personalized medicine in psoriasis. Expert Opin Biol Ther. 2022. https://doi.org/10.1080/14712598.2022.2113872.
Acknowledgements
We thank the participants of the study.
Funding
No funding or sponsorship was received for this study or publication of this article.
Author information
Authors and Affiliations
Contributions
Luca Potestio: data curation, formal analysis, investigation, visualization, writing-original draft preparation, writing—review & editing. Nello Tommasino: data curation, formal analysis, investigation, visualization, writing-original draft preparation, writing—review & editing. Giuseppe Lauletta: data curation, formal analysis, investigation, visualization, writing-original draft preparation, writing—review & editing. Fabrizio Martora: data curation, formal analysis, investigation, visualization, writing-original draft preparation, writing—review & editing. Matteo Megna: data curation, formal analysis, investigation, visualization, writing-original draft preparation, writing—review & editing.
Corresponding author
Ethics declarations
Conflict of interest
Luca Potestio, Nello Tommasino, Giuseppe Lauletta, Fabrizio Martora and Matteo Megna have nothing to disclose.
Ethical approval
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Potestio, L., Tommasino, N., Lauletta, G. et al. Psoriasis and Molecular Target Therapies: Evidence of Efficacy in Preventing Cardiovascular Comorbidities. Dermatol Ther (Heidelb) 14, 841–852 (2024). https://doi.org/10.1007/s13555-024-01152-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-024-01152-w