
Abstract
Background
After decades of use, methotrexate displays an established safety and efficacy profile in both in-hospital and outpatient settings. Despite its widespread use, there is surprisingly little clinical evidence to guide daily practice with methotrexate in dermatology.
Objectives
To provide guidance for clinicians in daily practice for areas in which there is limited guidance.
Methods
A Delphi consensus exercise on 23 statements was carried out on the use of methotrexate in dermatological routine settings.
Results
Consensus was reached on statements that cover six main areas: (1) pre-screening exams and monitoring of therapy; (2) dosing and administration in patients naïve to methotrexate; (3) optimal strategy for patients in remission; (4) use of folic acid; (5) safety; and (6) predictors of toxicity and efficacy. Specific recommendations are provided for all 23 statements.
Conclusions
In order to optimize methotrexate efficacy, it is essential to optimize treatment using appropriate dosages, carrying out a rapid drug-based step-up on a treat-to-target strategy and preferably using the subcutaneous formulation. To manage safety aspects appropriately, it is essential to evaluate patients’ risk factors and carry out proper monitoring during the course of treatment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Methotrexate (MTX) is actual, safe and efficient to treat inflammatory dermatoses. |
MTX treatment should be started at 15 mg per week, preferably subcutaneously. |
Lung and liver fibrosis due to MTX are idiosyncratic non-dose-dependent rare side effects. |
There is no cumulative dose threshold to consider for safety. |
Introduction
Methotrexate (MTX) has been used for decades to treat a wide variety of both inflammatory and neoplastic skin diseases and still remains an important drug in the therapeutic management of psoriatic disease [1]. Nowadays, MTX is regarded as the first-line drug in patients with moderate-severe psoriasis who are candidates for systemic treatment, in the absence of specific contraindications [2]. In addition to psoriasis, many other diseases (e.g. pityriasis rubra pilaris, chronic spontaneous urticaria, pityriasis lichenoides, atopic dermatitis, and vasculitides or connective tissue diseases) are treated with MTX in both in-label and off-label uses (see Electronic Supplementary Table [ESM} 1) [1].
By changing the posology of MTX from daily to weekly, this drug drastically modifies its effect from anti-proliferative to immunomodulatory/anti-inflammatory by activating T-regulatory lymphocytes and preventing the biosynthesis/release of interleukin (IL)-17, tumor necrosis factor alpha (TNF-α) and interferon gamma (IFN-γ) [3]. Remarkably, MTX displays prominent anti-inflammatory activity through several mechanisms, including the inhibition of dihydrofolate reductase and aminoimidazole-4-carboxamide ribonucleotide transformylase (ATIC), thereby increasing intracellular adenosine to prevent nuclear factor-κB (NF-κB) activation, or augmenting the expression of lincRNA-p21 [3].
In over 50 years of use, MTX has demonstrated a favorable profile in terms of both safety and efficacy, as well as a therapeutic versatility in-hospital and on an outpatient basis. In this article, we summarize current overall knowledge on MTX in dermatology with the aim to shed light on the remaining dermatological areas in which its use is directed mainly by the real-life clinical management.
Materials and methods
Rationale
Methotrexate is widely used in both hospitals and private practices by board-certified dermatologists for different dermatoses that often do not have dedicated guidelines. Guidelines also do not often give specific recommendations for patients who differ from the ideal real-world setting. For these reasons, the aims of this study were to: (1) explore real-life data present in literature; and (2) consolidate current evidence with the clinical experience derived from a group of Italian healthcare providers and dermatologists with > 5 years of experience using MTX. We carried out a Delphi consensus exercise on 23 statements focusing on MTX in dermatology with the overall aim to provide guidance for clinicians in daily practice.
Ethical approval for this Delphi consensus was waived by the local Ethics Committees.
Delphi Technique
The Delphi technique method allows the generation of consensus through a working group of experts on a specific topic, using an interactive process of individual feedback. The method is widely used in many fields of medicine to obtain consensus when formal recommendations are lacking or for areas in which clinical evidence is insufficient [4, 5]. A scale from 1 to 10, with 1 indicating complete disagreement and 10 indicating complete agreement, was used, with a cut-off of 7 considered to indicate approval with 70% of participants voting on the summary synthesis for all rounds of voting. Discrete variables were expressed as counts (percentage), and continuous variables were expressed as means with the standard deviation or medians with the 25–75th percentiles, as appropriate. Statistical analyses were performed using IBM SPSS Statistics 25.0 for Macintosh (IBM Corp., Armonk, NY, USA).
Delphi Round 1
A scientific committee was established comprising 19 Italian HCPs who fulfilled the following inclusion criteria: (1) board-certified dermatologist; (2) Italian as mother language; (3) > 10 years of experience managing patients with MTX; and (4) having managed/currently managing > 50 patients with MTX. The Italian Healthcare System (SSN) is a universal public healthcare system for all citizens and residents of Italy that uses a mixed public–private system administered on a regional basis; therefore, stakeholders were chosen to represent all Italian regions. The scientific committee met during the period February–May 2021 to individually draft a series of 37 open questions/summary syntheses on specific topics in six main areas based on clinical experience. A detailed literature search was then performed in the PubMed, EMBASE and Google databases to identify and collect all relevant studies on MTX in dermatology using search terms appropriate for each question with the keywords being “methotrexate,” “skin,” “dermatology” and “dermatoses.” After a general assessment by two dermatologists (GD and PP), all material found with the research strings was uploaded in a common cloud to allow free access to all stakeholders.
The statements were developed first individually and then discussed on June 2021 in two webinar sessions. Finally, the statements were reduced to 23 statements, considering only the most relevant, voted upon to achieve consensus and included in the present Delphi exercise.
Delphi Round 2
On September 2021, 85 dermatologists with > 5 years of experience managing MTX were invited to participate in the Delphi exercise (ESM Table 2). Of these, 69 agreed to participate. During this round, the 23 statements were presented and voted upon remotely. The steering committee then revised the statements for which agreement was not reached, which were voted upon in the next Delphi round.
Delphi Round 3
On October 2021, the eight statements for which agreement was not reached in the previous Delphi round were carefully re-assessed by the scientific committee and voted upon again. In this round, 54 dermatologists participated in the voting.
Results
Pre-Delphi Exercise and Definition of Cores and Statements
A total of 23 statements were drafted that covered six areas of treatment (Table 1), including: (1) pre-screening exams and monitoring of therapy (9 statements); (2) dosing and administration in patients naïve to MTX (5 statements); (3) optimal strategy for patients in remission (2 statements); (4) use of folic acid (1 statement); (5) safety (3 statements); (6) predictors of toxicity and efficacy (3 statements). Statements in each core area are discussed in the following sections.
Pre-screening Exams and Monitoring of Therapy
The MTX monitoring regimen, in addition to the renal-function test, differs between rheumatologists and dermatologists, ultimately leading to a higher estimation of side effects by dermatologists who monitor the patient more closely with laboratory tests [6]. At the present time, sampling carried out 5–7 days after the first dose to evaluate for adverse reactions is controversial and deemed to be not highly useful. There is some disagreement over the timing of monitoring during the first 2 months of therapy with two main proposals: every 2 weeks versus only at week 2 and then once a month [7, 8]. Both proposals are derived from expert opinion and not from clinical data. The participants supported the proposal that blood counts should be monitored 2 weeks after initiation of MTX therapy (statement 1). Patients should be monitored with blood counts, hepatic function tests and creatinine level every 4 weeks for the first 2 months of MTX initiation and then every 3 months. The practice of monitoring blood parameters in the maintenance phase every 3 months is well consolidated [9, 10].
Participants were asked their opinion on how to initiate MTX in patients with latent hepatitis B virus (HBV) or hepatitis C virus (HCV) infection. Regarding the initiation of MTX for those patients with HBV, consensus was reached that the risk for viral reactivation is low and thus prophylactic therapy is not mandatory (statement 2). For those patients who are HCV positive, since the long-term effects of MTX on HCV are not known, it was held that MTX should be avoided in patients with hepatic fibrosis (statement 3). Moreover, in those patients positive for tuberculosis (TBC), it was concluded that there is no need to carry out prophylaxis for TBC (statement 4); indeed, from the discussion it merged that it may even be safer not to carry out prophylaxis. There is currently no evidence to indicate the need for TBC prophylaxis for patients with latent TB infection who are candidates for treatment with MTX alone. There are only anecdotal cases that present TB disease undergoing treatment with MTX without prophylaxis [11].
Statement 5 focused on the use of hepatic elastography in monitoring patients. Monitoring patients using regular liver tests and keeping vigilant for risk factors are currently the best way to assess and limit MTX-based liver toxicity. Liver biopsy is no longer considered in any current recommendations, and there is no cumulative dose threshold [12]. Considering that the association between the cumulative dose of MTX and hepatic fibrosis is not supported by clinical evidence [13], the current trend is to prefer non-invasive monitoring (elastography and procollagen type III N-terminal peptide (P3NP)) over liver biopsy. Several studies have confirmed the long-term safety of MTX treatment in patients with immune-mediated diseases, including psoriasis. A meta-analysis of 32 randomized clinical studies involving a total of 13,177 patients with rheumatoid arthritis, psoriatic arthritis, psoriasis, and Crohn’s disease (6877 patients on MTX and 6300 treated with other conventional disease-modifying anti-rheumatic drugs [DMARDs] or biologic-DMARDs or placebo) reported the absence of major hepatic events (fibrosis, liver cirrhosis or death from liver injury) in patients treated with MTX [9]. On the other hand, patients receiving MTX had a higher incidence of elevated transaminases of a different entity compared to those receiving the other treatments. A precise estimate of the incidence of MTX-related fibrosis in the dosages commonly used for psoriasis and psoriatic arthritis (< 25 mg/week) is not available and, therefore, such events can be assumed to be a rare event.
P3NP monitoring is not recommended in patients aged < 20 years and > 70 years with arthritis since its level was found to persistently increase to > 8 mg/mL [14]. In patients who do not fall into these categories, P3NP level might be a good early biomarker for psoriatic arthritis and liver fibrosis, with monitoring to be performed every 3 months in patients at risk (body mass index [BMI] > 28 kg/m2) and high alcohol use [> 14 drinks per week]) [15]. Thus, elastography is recommended in non-obese patients every 1–3 years or if P3NP data are not available [15].
Regarding the possibility to monitor blood levels of MTX in the case of concomitant and prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs), salicylates, antibiotics or diphenylhydantoin, based on the scarce evidence available [16, 17, 18, 19], consensus was reached that evaluation of plasma levels of MTX is advisable before and after the introduction of a drug at risk of interaction in selected categories of patients (renal insufficiency, folate deficiency, hypoalbuminemia, elderly) (statement 6). As for NSAIDs, same-day administration with the above-mentioned agents should be avoided to prevent adverse reactions attributable to drug interactions [20].
Statements 7 and 8 concern the administration of MTX in patients who test positive for severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and in patients with a history of interstitial pneumonia from coronavirus disease-2019 (COVID-19), respectively. Consensus was reached that there is no evidence in the literature suggesting that MTX should be contraindicated in the former group of patients [21, 22]. In those patients with history of interstitial pneumonia from COVID-19 and initiating MTX, it was noted that there is no evidence suggesting that MTX is safe in patients with interstitial lung disease, and the only relevant publication in patients with inflammatory bowel disease did not identify MTX as a risk factor for hospitalization and death due to COVID-19 [23]; this finding was confirmed in a case–control study [24]. In addition, the authors of another study reported that MTX appears to inhibit the replication of SARS-CoV-2 in vitro [25]. Given the above results, it was held that the patient’s clinical status should be closely examined not only with the routine exams normally carried out, but also with instrumental and laboratory tests that confirm the resolution of COVID-19-related pneumonia. During the consensus, stakeholders agreed that only pre-existing lung fibrosis or interstitial disease may force the discontinuation MTX in patients with COVID-19. Lastly, greater knowledge of COVID-19 should be encouraged to prevent discontinuation of systemic therapies [26].
During the discussion of statement 9, many expert participants reported having administered MTX to a patient with severe psoriasis or with involvement of sensitive areas and a recent history of neoplasia (< 5 years), always in agreement with the patient’s oncologist. In these cases, no adverse events or relapse of the tumor was seen, and MTX was effective in controlling symptoms of psoriasis and skin manifestations.
MTX is a drug used for the treatment of many neoplasms at much higher dosages than those used to treat psoriasis, and its use in patients with current or recent neoplasia is not contraindicated. Regarding patients with recent previous cancer, there are two cohort studies in the literature, one on women with Crohn’s disease or rheumatoid arthritis with previous breast cancer [27] and one on patients with rheumatoid arthritis and previous non-melanoma skin cancer (squamous and/or basal cell tumors) [28]. In the former group, there was no increased risk of neoplastic recurrence in patients exposed to MTX in the year following cancer surgery compared to those not exposed to MTX (adjusted hazard ratio [HR] 1.07; 95% confidence interval [CI] 0.67–1.69), while in the latter group, treatment with MTX may have increased—albeit at the limits of statistical significance—the risk of recurrence of non-melanomatous skin cancer (HR 1.60; 95% CI 1.08–2.37).
In a recently published review on systemic drugs for psoriasis, only adalimumab, etanercept and infliximab (i.e. anti-TNFs) were found to have the potential to increase the risk of melanoma [29]. In the same review, it was noted that MTX does not increase the risk of melanoma.
A recent case–control study conducted in Sweden has shown that MTX therapy in psoriatic patients does not represent a risk factor for the onset of cutaneous melanoma [30]. Even an observational study conducted on data from the PSOLAR registry (Psoriasis Longitudinal Assessment and Registry) on over 12,000 patients with psoriasis did not detect an increase in melanoma in psoriatic patients treated with MTX for > 12 months [31]. Exposure to MTX, on the other hand, can increase the risk of developing basal cell carcinoma, but not squamous cell carcinoma. More generally, regarding the alleged oncological risk of MTX, a recent cohort study of 21,699 patients with rheumatoid arthritis showed that MTX users had a lower 12-year incidence of all cancers than non-users. The protective effect was more evident in users of higher cumulative doses [32].
Dosing and Administration in Patients Naïve to Methotrexate
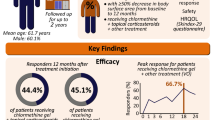
Regarding statement 10, on the basis of the available literature, MTX is now considered to be the traditional drug of first choice in the treatment of moderate/severe psoriasis, at the doses commonly approved in the treatment of psoriasis (7.5–25 mg/week), with a progressive clinical response associated with an acceptable level of safety for the patient [8]. The use of MTX at a reduced initial dosage of < 15 mg per week, in addition to determining a lower efficacy in terms of the Psoriasis Area Severity Index (PASI) 75 response (≥ 75% improvement in PASI from baseline) achieved at week 16 compared to the initial dosage of 15 mg/week (40% vs. 60%), does not protect the patient from adverse events [20, 33, 34].
The possibility of hepatic damage caused by iatrogenic toxicity (histologically diagnosed nonalcoholic fatty liver [NAFL] and nonalcoholic steatohepatitis [NASH]) during therapy with MTX has been reported [35, 36], although this risk was significantly linked to the patient’s clinical characteristics (e.g. age > 60 years, BMI > 30 kg/m2, type 2 diabetes, previous HBV-HCV liver disease and alcohol abuse) [37]. Therefore, in the absence of relative contraindications, the participants held that patients with psoriasis would benefit from a higher dose of MTX (≥ 15 mg/week), albeit with close monitoring.
It was also suggested that obese patients would benefit from a higher dose of MTX to obtain a good clinical response. It was noted, however, that there are some conditions that should be treated with caution. Considering the risk of hepatotoxicity related to the use of MTX even at low doses and a further increase in the risk of hepatic fibrosis in patients who are overweight, it would not be advisable to use initial doses > 15 mg/week (statement 11). Frequent monitoring of liver function should also be carried out in the first months of therapy [38, 39, 40].
MTX can be administered orally or subcutaneously. Subcutaneous administration appears to provide greater bioavailability, particularly at high doses [41, 42, 43, 44, 45, 46] (statement 12). A switch from oral to subcutaneous MTX may therefore be beneficial for patients who have suboptimal disease control. Furthermore, some studies have reported that in patients with moderate-severe psoriasis, a subcutaneous route of administration is associated with a higher response rate, more rapid onset, prolonged efficacy and fewer side effects [41, 42, 43, 44, 46, 47]. The use of a subcutaneous formulation of MTX should therefore be used as a first choice in patients starting treatment with MTX; however, the use of the subcutaneous formulation should also be attempted in patients who have not responded to the oral formulation in single or divided doses or have suspended its use due to side effects, before establishing the failure of treatment with MTX. A possible limitation is represented by its use in some patients with blenophobia.
MTX is generally administered at doses between 7.5 mg and 20 mg/week in adult patients, preferably subcutaneously [1, 20, 34]. If PASI 50 is not achieved at 8 weeks, the dose of MTX in selected patients can be increased up to 25 mg/week and carefully evaluating the risk–benefit profile (statements 12 and 13). When administered orally, it can be administered in a single dose or divided into 2 or 3 doses over a 24-h period. Further dose increases of no more than 25 mg per week can be considered only in selected patients by carefully evaluating the risk–benefit profile (statement 13).
The last statement in this area concerned the possibility of continuing MTX in association with a biological agent in the case of inadequate response to MTX alone (statement 14). The greater efficacy of MTX in combination with a biologic agent versus biologic monotherapy was confirmed in a recent meta-analysis [48]. In a randomized trial by Zacharie et al., patients with inadequate response to MTX who started etanercept without stopping MTX achieved the therapeutic goal of “clear/almost clear” at a significantly higher percentage than that observed in patients who discontinued MTX, with a similar adverse event profile in the two groups [49]. Experience in the combination of MTX and biologics for psoriasis from clinical trials is limited and mainly related to the combination with etanercept, with the combination therapy generally found to be more effective than monotherapy [50, 51, 52, 53]. Data on the treatment of psoriatic arthritis with a combination of MTX and biological agent are limited and do not allow definitive conclusions to be drawn [54, 55, 56]. The EuroGuiDerm Guidelines on Systemic Treatment of Psoriasis Vulgaris report that treatment with anti-TNF-α and MTX may be associated and may reduce the risk of anti-drug antibodies. The most common such combination is MTX + infliximab as its use is associated with a higher risk of anti-drug antibody formation [57]. EuroGuiDerm Guidelines also hypothesize the possibility of a greater risk of infections with combined therapy, in particular with respect to monotherapy with MTX, while underlining that definitive data are lacking [20]. This was summarized in statement 14.
Optimal Strategy for Patients in Remission
Statement 15 refers to the strategy to adopt in patients who are in remission after combination treatment with MTX and a biological agent. Even if not supported by the literature, the participating experts supported the recommendation that in patients on biologic treatment in combination with MTX and in remission, a step-down dose strategy of MTX is generally preferred up to the minimum effective dose or complete suspension of therapy, instead of dose changes in biologic therapy, to evaluate whether the patient maintains the remission when continuing with the biologic alone or if a new relapse occurs.
There is a higher percentage of obesity among patients with psoriasis compared with the general population, and obese patients have a higher incidence of NAFLD and resistance to therapy. Although the incidence of hepatic fibrosis is relatively low overall, patients with obesity, diabetes and significant alcohol use have a higher incidence of hepatic fibrosis. MTX per se does not appear to cause severe fibrosis, but is an important risk factor in patients with obesity and type 2 diabetes, and can also lead to elevation of liver enzymes in patients with obesity and NAFLD. From this evidence, it was reasonably concluded that a step-down strategy in patients with obesity is likely to be safer, although the exact strategy to adopt is unclear (statement 16).
Use of Folic Acid
The statement for this subject concerned the dose of folic acid to prescribe in patients with psoriasis and being treated with MTX. Clinical studies have shown that supplementation of the MTX therapy with folic acid is safe and significantly reduces the incidence of adverse effects by improving the tolerability of MTX [58, 59]. However, in dermatological disorders, the proportion of patients in whom folate is administered during MTX therapy appears to be low, and there is a lack of specific and shared data in the literature relating to the choice of the type of folate, the recommended dose and the frequency of administration, because few clinical trials have been conducted in this area [60]. Moreover, clinical trials comparing the effectiveness of folic acid administration at 5.0–27.5 mg/week have not shown any significant difference in efficacy [60]. Given this background, the participants agreed that folic acid should be administered during therapy with MTX at a dose of 5–10 mg/week in order to prevent side effects without loss of efficacy (statement 17).
Safety
The first statement in the area of safety considered the possibility of dose modification during radiotherapy/chemotherapy (statement 18). It was noted that there are no published data that would provide guidance for this, and the statement was based on expert opinion. If it is necessary to start chemotherapy/radiotherapy in patients with psoriasis/psoriatic arthritis currently on MTX therapy, MTX should not be interrupted/changed unless there is a clear indication from the oncologist/radiotherapist. If it is necessary to start MTX during chemotherapy/radiotherapy, the relevant oncologist/radiotherapist should be consulted.
Statement 19 addressed the question of which precautions should be taken in male patients who desire to father a child. MTX is widely used in male subjects of childbearing age with various diseases, including psoriasis. Among the reported effects at the testicular level, MTX has been associated with reversible oligospermia [61]. A rapid reduction in sperm parameters has been observed to occur after the initiation of therapy with MTX, which is attributable to interference with the final stages of spermatogenesis (transformation of spermatids into spermatozoa) [62, 63].
It should be pointed out that psoriasis, due to the effect of systemic inflammation and its comorbidities (metabolic syndrome, obesity, arterial hypertension, smoking habit, depression), may also affect spermatogenesis as well as sperm quality and number [64]. The participants agreed that before starting therapy with MTX it is important and appropriate to carry out counseling and guide the patient in the choice of therapy by informing him of the possible transient alterations of the sperm parameters. Discontinuation of MTX generally leads to a normalization of sperm parameters usually within 3 months of discontinuation, as reported in the literature (statement 19) [65]. Of note, a recent study reported that the sperm quality of patients treated with low-dose MTX is similar to that of healthy volunteers and that MTX does not increase sperm DNA fragmentation [66].
In the last statement on safety (statement 20), consensus was reached that the risk of infection, excluding TBC, SARS-CoV-2 and HBV/HCV, in patients with MTX at a non-oncological dosage is negligible and that the risk of death from infectious disease is comparable to that of the general population [67]. It was therefore not recommended to discontinue the drug in the presence of infections, other than those mentioned, as discontinuation would only affect the efficacy of the treatment.
Predictors of Toxicity and Efficacy
Considering statement 21, reviews in the literature have not found differences in the efficacy of MTX in the treatment of psoriasis by gender [34, 68]. Only one recent observational study reported that male gender is associated with clinical response to MTX treatment [69]. A systematic review of the literature on gender differences associated with response to treatment for psoriatic arthritis found no differences between men and women on long-term therapy with MTX [70]. Similarly, no gender differences were observed in another study comparing the response to MTX in psoriatic arthritis and rheumatoid arthritis [71]. Thus, statement 21 stresses the absence of evidence in the literature, albeit limited, to support the hypothesis that MTX may be more effective in male patients.
In statement 22, it was highlighted that there is scarce data in the literature on whether the presence of comorbid lung disease, such as COPD, would place the patient at higher risk of adverse events. The relevant literature refers almost exclusively to patients treated for rheumatoid arthritis. MTX is known to induce inflammatory subacute hypersensitivity pneumonitis unpredictable, which is potentially fatal [72, 73]. Risk factors include pre-existing lung diseases (patient age > 60 years, female sex, hypoalbuminemia, diabetes, previous use of DMARDs or anti-TNF-α) [74]. There is no evidence that the use of MTX is associated with an increased risk of developing chronic interstitial fibrotic lung disease [74, 75].
Statement 23 considers predisposing factors for pulmonary fibrosis, such as smoking, that would limit the prescribing of MTX. Recent reviews have questioned the role of MTX in the onset of pulmonary interstitial disease [74, 75]. On the other hand, MTX appears to slow the progression of pulmonary fibrosis in patients with rheumatoid arthritis. Cigarette smoking is responsible for idiopathic pulmonary fibrosis. Caution was recommended when prescribing MTX to smokers, but smoking should not be considered as a contraindication.
In recent years, the safety profile has been the subject of new re-analyses, which have led to the realization that the actual risks of MTX treatment for patients are lower than previously believed, especially regarding hepatic and pulmonary safety and infectious risk [9, 67, 76]. The safety profile can be further optimized through individual risk assessment and adequate monitoring of treated patients. An important advantage of MTX over other systemic treatments for psoriasis lies in the effects that the drug has on the main comorbidities that can frequently occur in the psoriatic patient. MTX is, in fact, effective in the treatment of psoriatic arthropathy and can also be useful in the case of inflammatory bowel disease, being indicated in the treatment of Crohn's disease [77]. In addition, in patients with high levels of systemic inflammation and therefore at high cardiovascular risk, such as in patients with psoriasis, MTX has been shown to reduce cardiovascular risk, mainly thanks to its anti-inflammatory action [78]. Indeed, a systematic review and meta-analysis of patients with immune-mediated inflammatory diseases, including psoriasis, who were treated with MTX demonstrated that the incidence of major adverse cardiovascular events (stroke, myocardial infarction, coronary artery disease and sudden cardiac death) was significantly reduced (21%) compared to that of patients undergoing other treatments; the risk of myocardial infarction was also 18% lower [79].
Despite its widespread use, there is surprisingly little clinical evidence to guide daily practice with MTX in dermatology. Although generally considered to be safe and efficacious, in dermatological conditions MTX is used at lower doses compared to those used in rheumatology. The more confident use of MTX in rheumatology, with higher dosages and less fear of safety aspects, allows for better outcomes in terms of efficacy and compliance. Indeed, in a retrospective follow-up study, patients with psoriatic arthritis managed by rheumatologists were generally treated with higher doses of MTX and underwent fewer liver enzyme monitoring controls than patients managed by dermatologists [80]. Patients managed by dermatologists also reported a higher rate of discontinuation, increased liver enzymes, loss of response and drug intolerance. These findings may be explained by the high use of oral versus subcutaneous MTX, with an increased prevalence of nausea associated with the former, and heterogenous interpretation of data on transaminases, often leading to a discontinuation of MTX or a decrease in MTX dose that limits drug efficacy. The clinical relevance of hepatic alterations has been overestimated by dermatologists, while in reality clinically relevant adverse hepatic events did not differ between the two groups. Moreover, the optimal starting dose has not been established in clinical studies, and only a handful of researchers have investigated the use of different doses of MTX for psoriasis [81, 82]. Despite some recommendations having been made on initial dose and treatment escalation, summarized in a recent international Delphi procedure [83], several aspects that impact daily practice in patients with psoriasis are far from being fully elucidated.
Conclusions
Many patients with moderate-severe psoriasis are still not treated, and among those being treated, some are still not adequately treated with systemic agents, although guidelines recommend the use of such agents to manage the systemic inflammation generated by this immune-mediated disease. Current guidelines for the management of patients with moderate-to-severe psoriasis recommend first-line use of MTX, cyclosporine or acitretin, while biologics should be considered if there is no response, intolerance or contraindication to first-line medications [20, 33, 34]. It should be noted that in Italy, the EuroGuiDerm Guidelines for psoriasis [20] were adapted but it was not reported that biologics may be considered the “first choice in severe disease when success can not be expected with conventional drugs” [85].
MTX is an effective and safe treatment for patients with moderate to severe psoriasis in the long term. Due to the chronicity of psoriasis, it is essential to consider that patients need to be treated systematically for many years, and thus more demanding treatments regarding safety and efficacy should be taken into consideration only when the first-line treatments are no longer sufficient to manage the disease. To obtain better efficacy from MTX, it is essential to optimize the treatment using appropriate dosages, carrying out a rapid step-up of the drug based on a treat-to-target strategy and preferably using the subcutaneous formulation. The latter allows improvement of patient compliance due to a better gastrointestinal tolerability and higher efficacy. To manage safety aspects appropriately, it is essential to evaluate the patient’s risk factors and carry out proper monitoring during the course of treatment [84].
References
Warren RB, Weatherhead SC, Smith CH, et al. British Association of Dermatologists’ guidelines for the safe and effective prescribing of methotrexate for skin disease 2016. Br J Dermatol. 2016;175(1):23–44.
National Institute for Health and Clinical Excellence (NICE). Psoriasis: assessment and management of psoriasis. Clinical guideline. Methods, evidence and recommendations. 2012. http://www.nice.org.uk/guidance/cg153/evidence/full-guideline-188351533. Accessed 1 Mar 2023.
Yan K, Xu W, Huang Y, et al. Methotrexate restores the function of peripheral blood regulatory T cells in psoriasis vulgaris via the CD73/AMPK/mTOR pathway. Br J Dermatol. 2018;179(4):896–905.
Dalkey N, Helmer O. An experimental application of the Delphi method to the use of experts. Mang Sci. 1963;9:458–457.
Meshkat CS, Gethin G, Ryan K, Wiley M, Brick A, Clarke E, Mulligan E. Using an e-Delphi technique in achieving consensus across disciplines for developing best practice in day surgery in Ireland. J Hosp Adm. 2014;3:1–8.
Dupuis EC, Bhole VM, Dutz JP. Differing patterns of methotrexate use for psoriatic disease among dermatologists and rheumatologists. Br J Dermatol. 2012;167(2):448–50.
Nast A, Jacobs A, Rosumeck S, et al. Methods report: European S3-guidelines on the systemic treatment of psoriasis vulgaris—update 2015—EDF in cooperation with EADV and IPC. J Eur Acad Dermatol Venereol. 2015;29(12):e1–22.
Rademaker M, Gupta M, Andrews M, et al. The Australasian Psoriasis Collaboration view on methotrexate for psoriasis in the Australasian setting. Australas J Dermatol. 2017;58(3):166–70.
Conway R, Carey JJ. Risk of liver disease in methotrexate treated patients. World J Hepatol. 2017;9(26):1092–100.
Conway R, Low C, Coughlan RJ, et al. Risk of liver injury among methotrexate users: a meta-analysis of randomised controlled trials. Semin Arthritis Rheum. 2015;45(2):156–62.
Burgos D, Membriani ES, Limongi L, et al. Use of immunosuppressants in patients with autoimmune diseases and latent tuberculosis. American Thoracic Society Conference Abstracts C62. Tuberculosis: bench to bedside. Am J Respir Crit Car Med. 2018;197:A5562.
Clary DD, Reid AT, Kiani R, et al. Methotrexate hepatotoxicity monitoring guidelines in psoriasis and rheumatoid arthritis: is there a consensus? S D Med. 2021;74(8):363–6.
Maybury CM, Jabbar-Lopez ZK, Wong T, et al. Methotrexate and liver fibrosis in people with psoriasis: a systematic review of observational studies. Br J Dermatol. 2014;171(1):17–29.
Lindsay K, Fraser AD, Layton A, et al. Liver fibrosis in patients with psoriasis and psoriatic arthritis on long-term, high cumulative dose methotrexate therapy. Rheumatology (Oxford). 2009;48(5):569–72.
Laharie D, Seneschal J, Schaeverbeke T, et al. Assessment of liver fibrosis with transient elastography and FibroTest in patients treated with methotrexate for chronic inflammatory diseases: a case-control study. J Hepatol. 2010;53(6):1035–40.
Liddle BJ. Methotrexate interactions. Clin Exp Dermatol. 1991;16(4):311–2.
Mayall B, Poggi G, Parkin JD. Neutropenia due to low-dose methotrexate therapy for psoriasis and rheumatoid arthritis may be fatal. Med J Aust. 1991;155(7):480–4.
Saurat JH, Guerin A, Yu AP, et al. High prevalence of potential drug-drug interactions for psoriasis patients prescribed methotrexate or cyclosporine for psoriasis: associated clinical and economic outcomes in real-world practice. Dermatology. 2010;220(2):128–37.
Thomas DR, Dover JS, Camp RD. Pancytopenia induced by the interaction between methotrexate and trimethoprim-sulfamethoxazole. J Am Acad Dermatol. 1987;17(6):1055–6.
Nast A, Smith C, Spuls PI, et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris—part 1: treatment and monitoring recommendations. J Eur Acad Dermatol Venereol. 2020;34(11):2461–98.
Favalli EG, Bugatti S, Klersy C, et al. Impact of corticosteroids and immunosuppressive therapies on symptomatic SARS-CoV-2 infection in a large cohort of patients with chronic inflammatory arthritis. Arthritis Res Ther. 2020;22(1):290.
Fernandez-Gutierrez B, Leon L, Madrid A, et al. Hospital admissions in inflammatory rheumatic diseases during the peak of COVID-19 pandemic: incidence and role of disease-modifying agents. Ther Adv Musculoskelet Dis. 2021;13:1759720X20962692. https://doi.org/10.1177/1759720X20962692.
Gilissen LPL, Heinen SGH, Rijpma-Jacobs L, et al. Neither inflammatory bowel disease nor immunosuppressants are associated with an increased risk of severe COVID-19: an observational Dutch cohort study. Clin Exp Med. 2021;22(3):465–76.
Schalter F, Durholz K, Bucci L, et al. Does methotrexate influence COVID-19 infection? Case series and mechanistic data. Arthritis Res Ther. 2021;23(1):166.
Caruso A, Caccuri F, Bugatti A, et al. Methotrexate inhibits SARS-CoV-2 virus replication “in vitro.” J Med Virol. 2021;93(3):1780–5.
Bragazzi NL, Ricco M, Pacifico A, et al. COVID-19 knowledge prevents biologics discontinuation: data from an Italian multicenter survey during RED-ZONE declaration. Dermatol Ther. 2020;33(4): e13508.
Mamtani R, Clark AS, Scott FI, et al. Association between breast cancer recurrence and immunosuppression in rheumatoid arthritis and inflammatory bowel disease: a cohort study. Arthritis Rheumatol. 2016;68(10):2403–11.
Scott FI, Mamtani R, Brensinger CM, et al. Risk of nonmelanoma skin cancer associated with the use of immunosuppressant and biologic agents in patients with a history of autoimmune disease and nonmelanoma skin cancer. JAMA Dermatol. 2016;152(2):164–72.
Semaka A, Salopek TG. Risk of developing melanoma with systemic agents used to treat psoriasis: a review of the literature. J Cutan Med Surg. 2022;26(1):87–92.
Polesie S, Gillstedt M, Paoli J, et al. Methotrexate treatment for patients with psoriasis and risk of cutaneous melanoma: a nested case-control study. Br J Dermatol. 2020;183(4):684–91.
Fiorentino D, Ho V, Lebwohl MG, et al. Risk of malignancy with systemic psoriasis treatment in the Psoriasis Longitudinal Assessment Registry. J Am Acad Dermatol. 2017;77(5):845–54 (e845).
Perng WT, Hung YM, Chang R, et al. Methotrexate at middle and high accumulative doses might be associated with lower risk of new-onset cancers in patients with rheumatoid arthritis: a nationwide population-based cohort study. Ther Adv Musculoskelet Dis. 2020;12:1759720X20981221. https://doi.org/10.1177/1759720X20981221.
Gisondi P, Altomare G, Ayala F, et al. Italian guidelines on the systemic treatments of moderate-to-severe plaque psoriasis. J Eur Acad Dermatol Venereol. 2017;31(5):774–90.
Yelamos O, Puig L. Systemic methotrexate for the treatment of psoriasis. Expert Rev Clin Immunol. 2015;11(5):553–63.
Meunier L, Larrey D. Chemotherapy-associated steatohepatitis. Ann Hepatol. 2020;19(6):597–601.
Patel V, Sanyal AJ. Drug-induced steatohepatitis. Clin Liver Dis. 2013;17(4):533–46 (vii).
Paul C, Gallini A, Maza A, et al. Evidence-based recommendations on conventional systemic treatments in psoriasis: systematic review and expert opinion of a panel of dermatologists. J Eur Acad Dermatol Venereol. 2011;25(Suppl):22–11.
Cheng HS, Rademaker M. Monitoring methotrexate-induced liver fibrosis in patients with psoriasis: utility of transient elastography. Psoriasis (Auckl). 2018;8:21–9.
Chiricozzi A, Gisondi P, Girolomoni G. The pharmacological management of patients with comorbid psoriasis and obesity. Expert Opin Pharmacother. 2019;20(7):863–72.
Taylor WJ, Korendowych E, Nash P, et al. Drug use and toxicity in psoriatic disease: focus on methotrexate. J Rheumatol. 2008;35(7):1454–7.
Attwa EM, Elkot RA, Abdelshafey AS, et al. Subcutaneous methotrexate versus oral form for the treatment and prophylaxis of chronic plaque psoriasis. Dermatol Ther. 2019;32(5):e13051.
Hollywood A, O’Keeffe C, Boggs J, et al. The utility of subcutaneous methotrexate for chronic plaque psoriasis in a real-world setting. Br J Dermatol. 2020;182(5):1290–1.
Pichlmeier U, Heuer KU. Subcutaneous administration of methotrexate with a prefilled autoinjector pen results in a higher relative bioavailability compared with oral administration of methotrexate. Clin Exp Rheumatol. 2014;32(4):563–71.
Reich K, Sorbe C, Griese L, et al. The value of subcutaneous vs. oral methotrexate: real-world data from the German psoriasis registry PsoBest. Br J Dermatol. 2021;184(4):765–7.
Schiff MH, Jaffe JS, Freundlich B. Head-to-head, randomised, crossover study of oral versus subcutaneous methotrexate in patients with rheumatoid arthritis: drug-exposure limitations of oral methotrexate at doses ≥ 15 mg may be overcome with subcutaneous administration. Ann Rheum Dis. 2014;73(8):1549–51.
Yesudian PD, Leman J, Balasubramaniam P, et al. Effectiveness of subcutaneous methotrexate in chronic plaque psoriasis. J Drugs Dermatol. 2016;15(3):345–9.
Dogra S, Singh N, Kumar S, et al. Comparison of overall efficacy and safety of oral versus subcutaneous methotrexate in severe psoriasis. Dermatol Ther. 2022;35(8): e15656.
Xie Y, Liu Y, Liu Y. Are biologics combined with methotrexate better than biologics monotherapy in psoriasis and psoriatic arthritis: a meta-analysis of randomized controlled trials. Dermatol Ther. 2021;34(3): e14926.
Zachariae C, Mork NJ, Reunala T, et al. The combination of etanercept and methotrexate increases the effectiveness of treatment in active psoriasis despite inadequate effect of methotrexate therapy. Acta Derm Venereol. 2008;88(5):495–501.
Gottlieb AB, Langley RG, Strober BE, et al. A randomized, double-blind, placebo-controlled study to evaluate the addition of methotrexate to etanercept in patients with moderate to severe plaque psoriasis. Br J Dermatol. 2012;167(3):649–57.
Liu LF, Chen JS, Gu J, et al. Etanercept biosimilar (recombinant human tumor necrosis factor-α receptor II: IgG Fc fusion protein) and methotrexate combination therapy in Chinese patients with moderate-to-severe plaque psoriasis: a multicentre, randomized, double-blind, placebo-controlled trial. Arch Dermatol Res. 2020;312(6):437–45.
van den Reek JM, van Lumig PP, Kievit W, et al. Effectiveness of adalimumab dose escalation, combination therapy of adalimumab with methotrexate, or both in patients with psoriasis in daily practice. J Dermatolog Treat. 2013;24(5):361–8.
Yu Q, Tong Y, Cui L, et al. Efficacy and safety of etanercept combined plus methotrexate and comparison of expression of pro-inflammatory factors expression for the treatment of moderate-to-severe plaque psoriasis. Int Immunopharmacol. 2019;73:442–50.
Baranauskaite A, Raffayova H, Kungurov NV, et al. Infliximab plus methotrexate is superior to methotrexate alone in the treatment of psoriatic arthritis in methotrexate-naive patients: the RESPOND study. Ann Rheum Dis. 2012;71(4):541–8.
Behrens F, Koehm M, Arndt U, et al. Does concomitant methotrexate with adalimumab influence treatment outcomes in patients with psoriatic arthritis? Data from a large observational study. J Rheumatol. 2016;43(3):632–9.
Mease PJ, Gladman DD, Collier DH, et al. Etanercept and methotrexate as monotherapy or in combination for psoriatic arthritis: primary results from a randomized, controlled phase III. Trial Arthritis Rheumatol. 2019;71(7):1112–24.
Davila-Seijo P, Dauden E, Descalzo MA, et al. Infections in moderate to severe psoriasis patients treated with biological drugs compared to classic systemic drugs: findings from the BIOBADADERM registry. J Invest Dermatol. 2017;137(2):313–21.
Prey S, Paul C. Effect of folic or folinic acid supplementation on methotrexate-associated safety and efficacy in inflammatory disease: a systematic review. Br J Dermatol. 2009;160(3):622–8.
van Ede AE, Laan RF, Rood MJ, et al. Effect of folic or folinic acid supplementation on the toxicity and efficacy of methotrexate in rheumatoid arthritis: a forty-eight week, multicenter, randomized, double-blind, placebo-controlled study. Arthritis Rheum. 2001;44(7):1515–24.
Al-Dabagh A, Davis SA, Kinney MA, et al. The effect of folate supplementation on methotrexate efficacy and toxicity in psoriasis patients and folic acid use by dermatologists in the USA. Am J Clin Dermatol. 2013;14(3):155–61.
French AE, Koren G, Motherisk T. Effect of methotrexate on male fertility. Can Fam Physician. 2003;49:577–8.
Gutierrez JC, Hwang K. The toxicity of methotrexate in male fertility and paternal teratogenicity. Expert Opin Drug Metab Toxicol. 2017;13(1):51–8.
Mouyis M, Flint JD, Giles IP. Safety of anti-rheumatic drugs in men trying to conceive: a systematic review and analysis of published evidence. Semin Arthritis Rheum. 2019;48(5):911–20.
Brenaut E. Planifier une grossesse chez une patiente avec un psoriasis. Eur J Dermatol. 2020;30(S1):18–24.
Grosen A, Kelsen J, Hvas CL, et al. The influence of methotrexate treatment on male fertility and pregnancy outcome after paternal exposure. Inflamm Bowel Dis. 2017;23(4):561–9.
Grosen A, Bellaguarda E, Nersting J, et al. Low-dose methotrexate therapy does not affect semen parameters and sperm DNA. Inflamm Bowel Dis. 2022;28(7):1012–8.
Ibrahim A, Ahmed M, Conway R, et al. Risk of infection with methotrexate therapy in inflammatory diseases: a systematic review and meta-analysis. J Clin Med. 2018;8(1):15. https://doi.org/10.3390/jcm8010015.
Raaby L, Zachariae C, Ostensen M, et al. Methotrexate use and monitoring in patients with psoriasis: a consensus report based on a Danish expert meeting. Acta Derm Venereol. 2017;97(4):426–32.
Pongparit K, Chularojanamontri L, Limphoka P, et al. Effectiveness of and factors associated with clinical response to methotrexate under daily life conditions in Asian patients with psoriasis: a retrospective cohort study. J Dermatol. 2018;45(5):540–5.
Generali E, Scire CA, Cantarini L, et al. Sex differences in the treatment of psoriatic arthritis: a systematic literature review. Isr Med Assoc J. 2016;18(3–4):203–8.
Lie E, van der Heijde D, Uhlig T, et al. Effectiveness and retention rates of methotrexate in psoriatic arthritis in comparison with methotrexate-treated patients with rheumatoid arthritis. Ann Rheum Dis. 2010;69(4):671–6.
Kinder AJ, Hassell AB, Brand J, et al. The treatment of inflammatory arthritis with methotrexate in clinical practice: treatment duration and incidence of adverse drug reactions. Rheumatology (Oxford). 2005;44(1):61–6.
Sathi N, Chikura B, Kaushik VV, et al. How common is methotrexate pneumonitis? A large prospective study investigates. Clin Rheumatol. 2012;31(1):79–83.
Conway R, Low C, Coughlan RJ, et al. Methotrexate use and risk of lung disease in psoriasis, psoriatic arthritis, and inflammatory bowel disease: systematic literature review and meta-analysis of randomised controlled trials. BMJ. 2015;350:h1269.
Cottin V, Bendstrup E, Bonniaud P, et al. The case of methotrexate and the lung: Dr Jekyll and Mr Hyde. Eur Respir J. 2021;57(2):2100079.
Malaviya AN. Does methotrexate cause interstitial lung disease in rheumatoid arthritis: What is the evidence? Int J Rheum Dis. 2020;23(6):713–6.
Mikhaylov D, Hashim PW, Nektalova T, et al. Systemic psoriasis therapies and comorbid disease in patients with psoriasis: a review of potential risks and benefits. J Clin Aesthet Dermatol. 2019;12(6):46–54.
Verhoeven F, Prati C, Chouk M, et al. Methotrexate and cardiovascular risk in rheumatic diseases: a comprehensive review. Expert Rev Clin Pharmacol. 2021;14(9):1105–12.
Micha R, Imamura F, Wyler von Ballmoos M, et al. Systematic review and meta-analysis of methotrexate use and risk of cardiovascular disease. Am J Cardiol. 2011;108(9):1362–70.
Busger OP, Vollenbroek FTM, Doggen CJM, Janssens RWA, et al. Dermatological guidelines for monitoring methotrexate treatment reduce drug-survival compared to rheumatological guidelines. PLoS ONE. 2018;13(3):e0194401.
Dogra S, Krishna V, Kanwar AJ. Efficacy and safety of systemic methotrexate in two fixed doses of 10 mg or 25 mg orally once weekly in adult patients with severe plaque-type psoriasis: a prospective, randomized, double-blind, dose-ranging study. Clin Exp Dermatol. 2012;37(7):729–34.
Menting SP, Dekker PM, Limpens J, et al. Methotrexate dosing regimen for plaque-type psoriasis: a systematic review of the use of test-dose, start-dose, dosing scheme, dose adjustments, maximum dose and folic acid supplementation. Acta Derm Venereol. 2016;96(1):23–8.
van Huizen AM, Menting SP, Gyulai R, et al. International eDelphi study to reach consensus on the methotrexate dosing regimen in patients with psoriasis. JAMA Dermatol. 2022;158(5):561-72.
Corazza V, Cusano F, De Pita O, et al. Methotrexate in the therapeutic pathway of patients with psoriasis. Analysis of clinical practice data and comparison with guidelines. Dermatol Rep. 2022;14(1):9454.
Gisondi P, Fargnoli MC, Amerio P, et al. Italian adaptation of EuroGuiDerm guideline on the systemic treatment of chronic plaque psoriasis. Ital J Dermatol Venerol. 2022;157(Suppl 1, No. 1):1–78.
Acknowledgements
Springer Healthcare is not responsible for the validity of guidelines it publishes.
METHOD study working group
Giuseppe Alessandrini1; Gabriella Andreassi2; Veronica Arese3; Nicoletta Bernardini4; Maria Rita Bongiorno5; Riccardo Borroni6; Alexandra MG Brunasso Vernetti7; Pier Luigi Bruni8; Giacomo Caldarola9; Elena Campione10; Antonio Carpentieri11; Martino Carriero12; Franco Castelli13; Marina Castriota14; Angelo Cattaneo15; Emilia Cerulli16; Karin Chersi17; Michela Cicoletti8; Paola Colasanti18; Monica Corazza19; Mario Cordedda20; Emanuele Claudio Cozzani21; Aldo Cuccia22; Domenico D'Amico23; Stefano Dastoli24; Anna Rita Dell’Anna25; Antonella Di Cesare26; Vito Giuseppe Di Lernia27; Valentina Dini28; Maria Esposito29; Carmen Silvia Fiorella30; Santo Raffaele Mercuri31; Maria Francesca Gaiani32; Giovanna Galdo33; Lucia Gallo34; Marco Galluzzo35,36; Matteo Claudio Garavaglia37; Alessandro Gatti38; Claudia Giofrè39; Claudio Guarneri40; Jacqueline Kussini41; Serena Lembo42; Luigi Ligrone43; Cinzia Masini44; Giampiero Mazzocchetti45; Matteo Megna 34; Gennaro Melchionda46; Antonio Miracapillo47; Pietro Morrone48; Cristina Mugheddu49; Maria Letizia Musumeci50; Patrizia Nespoli51; Giulia Odorici52; Gloria Orlando53; Giovanni Domenico Palazzo54; Fabrizio Panarese55; Salvatore Panduri56; Massimiliano Pazzaglia57; Alexia Pedron58; Michele Pezza59; Angelo Piccirillo60; Federigo Pioli61; Federico Pirro9; Miriam Pizzolato62; Roberto Porciello63; Francesca Prestinari64; Nella Maria Grazia Pulvirenti65; Andrea Romani66; Francesca Romano67; Luigi Rossiello68; Sandra Schianchi69; Genoveffa Scotto di Luzio70; Zelda Seia71; Stefania Sorbara72; Davide Luigi Strippoli64; Elena Stroppiana73; Franca Taviti74; Pompilio Trevisi75; Emanuele Trovato76; Maria Teresa Uzzauto77; Anna Verrone78; Silvia Vichi79; Leonardo Zichichi80
METHOD study working group affiliations
1Dermatology and Venereology Private Practice, Gallipoli, Lecce, Italy; 2Dermatologic Clinic, Department of Medicine and Aging Science, University G D'Annunzio Chieti-Pescara, Chieti, Italy; 3Unit of Dermatology, Department of Medical Sciences, Molinette Hospital, Città della Salute e della Scienza, Turin, Italy; 4Department of Medico-surgical Sciences and Biotechnologies, Sapienza University of Rome, Polo Pontino, Italy; 5Section of Dermatology, Department of Health Promotion, Mother and Child Care, Internal Medicine and Medical Specialties, University of Palermo, Palermo, Italy; 6Unit of Dermatology, IRCCS Humanitas Clinic, Rozzano, Milan, Italy; 7Department of Dermatology, Galliera Hospital, Genoa, Italy; 8UOC Clinical Dermatology, Azienda Ospedaliera S. Maria, Terni, Italy; 9Department of Dermatology, IRCCS A. Gemelli University Polyclinic Foundation, Rome, Italy; 10Dermatologic Unit, Department of Systems Medicine, University of Rome Tor Vergata, Rome, Italy; 11Department of Biomedical Sciences and Human Oncology, Section of Dermatology, University of Bari, Bari, Italy; 12Dermatology Unit, Poliambulatorio Grottaglie, Grottaglie, Italy; 13Dermatology Unit, Koelliker Hospital, Turin, Italy; 14Dermatology Private Practice, Caprarica di Lecce, Italy; 15IRCCS Fondazione Ca'Granda, Ospedale maggiore Policlinico, Milan, Italy; 16Hospital Pharmacy Unit, Santa Maria della Misericordia Hospital, Hospital of Perugia, Perugia, Italy; 17Dermatological Clinic, ASUGI—Azienda Sanitaria Universitaria Giuliano Isontina, Trieste, Italy; 18Dermatology Unit, “Ospedale del Mare”, Naples, Italy; 19Section of Dermatology and Infectious Diseases, Department of Medical Sciences, University of Ferrara, Ferrara, Italy; 20UOC Dermatology, San Gennaro Hospital, Naples, Italy; 21Section of Dermatology, Department of Health Sciences (DISSAL), University of Genoa, Genoa, Italy; 22Dermatology, San Donato Hospital, Arezzo, Surgical Department, Usl Toscana Sudest, Italy; 23Clinical Dermatology, Azienda Ospedaliera “Pugliese Ciaccio”, Catanzaro, Italy; 24Department of Health Sciences, University Magna Graecia of Catanzaro, Catanzaro, Italy; 24Department of Health Sciences, University Magna Graecia of Catanzaro, Catanzaro, Italy; 25Clinical Dermatology, ASL Bari, Bari, Italy; 26Department of Health Sciences, Section of Dermatology, University of Florence, Florence, Italy; 27Dermatology Unit, Arcispedale Santa Maria Nuova, Azienda USL-IRCCS di Reggio Emilia, Reggio Emilia, Italy; 28Department of Dermatology, University of Pisa, Pisa, Italy; 29Department of Biotechnological and Applied Clinical Sciences, University of L’Aquila, L’Aquila, Italy; 30Clinical Dermatology, Ospedale Dimiccoli di Barletta, Barletta, Italy; 31Unit of Dermatology, IRCCS San Raffaele Hospital, Milan, Italy; 32Dermatology Unit, Azienda Ospedaliera San Donato Milanese, Milan, Italy; 33Dermatology Unit, Moscati Hospital, Avellino, Italy; 34Section of Dermatology, Department of Clinical Medicine and Surgery, University of Naples Federico II, Naples, Italy; 35Department of Systems Medicine, University of Rome “Tor Vergata”, Rome, Italy; 36Dermatology Unit, Fondazione Policlinico “Tor Vergata”, Rome, Italy; 37Clinical Dermatology, IRCCS Istituto Ortopedico Galeazzi, Milan, Italy; 38ULSS 2 Marca Trevigiana Ospedale Ca' Foncello Treviso, Treviso, Italy; 39U.O.C. Dermatologia, A.O. Papardo, Messina, Italy; 40Department of Biomedical and Dental Sciences and Morpho Functional Imaging, University of Messina, Messina, Italy; 41Dermatology and Laserklink, Biberach, Germany; 42Department of Medicine, Surgery and Dentistry, “Scuola Medica Salernitana”, University of Salerno, Salerno, Italy; 43Dermatology Unit, San Giovanni di Dio e Ruggi D'Aragona University Hospital, Scuola Medica Salernitana, Salerno, Italy; 44UOC Dermatology, Ospedale dei Castelli, Rome, Italy; 45UOSD Dermatologia ASL1 Pescara, Pescara, Italy; 46Dermatology Unit, Casa Sollievo della Sofferenza-IRCCS, San Giovanni Rotondo, Italy; 47Dermatology Unit, Ospedale Generale Regionale “F. Miulli”, Acquaviva delle Fonti, Italy; 48UOC Dermatology, Azienda Ospedaliera di Cosenza, Cosenza, Italy;49Section of Dermatology, Department of Medical Sciences and Public Health, University of Cagliari, Cagliari, Italy; 50Dermatology Clinic, University of Catania, Catania, Italy; 51UOS Dermatology, ASL Teramo, Teramo, Italy; 52Section of Dermatology and Infectious Diseases, Department of Medical Sciences, University of Ferrara, Ferrara, Italy; 53Unit of Dermatology, Department of Medicine, University of Padua, Padua, Italy; 54Clinical Dermatology, Azienda Sanitaria Locale di Matera, Matera, Italy; 55Department of Dermatology, University “G D’Annunzio” University of Chieti-Pescara, Chieti, Italy; 56UO Dermatologia, Azienda Ospedaliero Universitaria Pisana, Pisa, Italy; 57Dermatology Division IRCCS Sant'Orsola Policlinico University of Bologna, Bologna, Italy; 58Dermatology Unit, Ospedale Carlo Poma, Mantova, Italy; 59Dermatology Department, ASL Benevento, Benevento, Italy; 60AO Ospedale San Carlo di Potenza, Italy; 61Clinical Dermatology, ASL Toscana NordOvest, Cecina, Italy; 62Dermatology Unit, Azienda Ospedaliera Universitaria Integrata di Verona, Verona, Italy; 63Dermatology Unit, Ospedale “Sandro Pertini”, Rome, Italy; 64Dermatology Unit, Ospedale Manzoni, Lecco, Italy; 65Private Practice, Giarre, Italy;66Dermatology Unit, Istituto Dermoclinico Vita Cutis, Milan, Italy;67Dermatology Unit, University of Campania Luigi Vanvitelli, Naples, Italy; 68Department of Dermatology, A.O.R.N. “A. Cardarelli”, Naples, Italy; 69Centro Grandi Ustionati, Cesena, Italy; 70AO Caserta San Sebastiano e Sant Anna UOS Di Dermatologia, Caserta, Italy; 71Clinical Dermatology, asl CN1, Cuneo, Italy; 72Clinical Dermatology, Azienda Socio Sanitaria Ligure n. 4, Chiavari, Italy; 73Department of Medical Science, Dermatology Clinic, “Città della Salute e della Scienza of Turin,” Turin, Italy; 74UOSD Dermatology, USL Toscana Centro-Prato Hospital, Prato, Italy; 75Private Practice, Campi Salentina, Italy; 76Department of Medical, Surgical and Neurological Science, Dermatology Section, University of Siena, S. Maria alle Scotte Hospital, Siena, Italy; 77U.O.C. Dermatologia, ASL Salerno, Ospedale “A:Tortora”-Pagani, Salerno, Italy; 78Department of Medical Sciences, Section of Dermatology, University of Turin, Turin, Italy; 79AUSL Romagna Infermi Hospital, Rimini, Italy; 80Unit of Dermatology, San Antonio Abate Hospital, Trapani, Italy.
Funding
The METHOD project was developed with the unconditional support of Alfasigma. Alfasigma funded the rapid service fee for the publication of the present manuscript.
Medical Writing
The authors thank Patrick Moore, an independent medical writer, who provided medical writing support that was funded by Alfasigma.
Author Contributions
Conceptualization: Giovanni Damiani and Paolo Pigatto. Methodology: Giovanni Damiani; Software: Giovanni Damiani. Validation: Giovanni Damiani and Paolo Pigatto. Formal analysis: Giovanni Damiani. Investigation: Giovanni Damiani and Paolo Pigatto. Resources: Giovanni Damiani and Paolo Pigatto. Data curation: Giovanni Damiani. Writing–original draft: Giovanni Damiani. Writing–review and editing: Giovanni Damiani, Paolo Amerio, Federico Bardazzi, Carlo Carrera, Andrea Conti, Francesco Cusano, Paolo Dapavo, Clara DeSimone, Maya ElHachem, Gabriella Fabbrocini, Paolo Gisondi, Francesco Loconsole, Giuseppe Micali, Iria Neri, Aurora Parodi, Stefano Piaserico, Marco Romanelli, Luca Stingeni and Paolo Pigatto. Visualization: Giovanni Damiani. Supervision: Giovanni Damiani and Paolo Pigatto. Project administration: Giovanni Damiani and Paolo Pigatto.
Disclosures
Giovanni Damiani, Paolo Amerio, Federico Bardazzi, Carlo Carrera, Andrea Conti, Francesco Cusano, Paolo Dapavo, Clara DeSimone, Maya ElHachem, Gabriella Fabbrocini, Paolo Gisondi, Francesco Loconsole, Giuseppe Micali, Iria Neri, Aurora Parodi, Stefano Piaserico, Marco Romanelli, Luca Stingeni and Paolo Pigatto declared no conflict of interests.
Compliance with Ethics Guidelines
Guidelines are waived to the Ethical approval.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, G.D., upon reasonable request.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
The names and affiliations of the members of the “METHOD study working group” are provided in the Acknowledgements section.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Damiani, G., Amerio, P., Bardazzi, F. et al. Real-World Experience of Methotrexate in the Treatment of Skin Diseases: an Italian Delphi Consensus. Dermatol Ther (Heidelb) 13, 1219–1241 (2023). https://doi.org/10.1007/s13555-023-00930-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-023-00930-2