
Abstract
Introduction
Although dimethyl fumarate (DMF) has been approved since 2017 for treatment of moderate-to-severe plaque psoriasis, limited data on its safety and efficacy are available in clinical practice. The objective was to assess the efficacy and safety of DMF in patients with moderate-to-severe plaque psoriasis through 52 weeks in conditions close to real clinical practice.
Methods
DIMESKIN 1 was a 52-week, open-label, phase IV clinical trial conducted at 36 Spanish sites. Adults with diagnosis of moderate-to-severe plaque psoriasis, treated with DMF as per its summary of product characteristics and with ≥ 1 post-baseline Psoriasis Area and Severity Index (PASI) value were included [intention-to-treat (ITT) population]. Efficacy analyses were performed for ITT population and are based on multiple imputation.
Results
Overall, 282 and 274 patients were included in the safety and ITT populations, respectively. At week 24, 46.0%/24.8%/10.9% of patients achieved PASI 75/90/100 response, respectively. At week 52, these percentages were 46.0%/21.9%/10.9%, respectively. Mean body surface area affected decreased from 17.4% to 6.9%/7.3% after 24/52 weeks (p < 0.001, both). A total of 42.9%/49.4% of patients had a Physician’s Global Assessment 0–1 at week 24/52, respectively. Mean pruritus visual analogue scale (VAS) significantly decreased after 24 and 52 weeks (p < 0.001, both), with 56.5% and 67.6% of patients, respectively, rating a pruritus VAS < 3. At week 24/52, 61.3%/73.4% patients had a Dermatology Life Quality Index (DLQI) ≤ 5 and 34.7%/32.1% had a DLQI 0-1. The most frequent adverse events were gastrointestinal disorders (mainly diarrhea/abdominal pain in 50.0%/35.1% of patients, respectively), flushing (28.0%), and lymphopenia (31.2%), mostly mild/moderate.
Conclusions
DMF significantly improves main severity and extension indexes and rates, as well as patient-reported outcomes such as pruritus and quality of life in patients with moderate-to-severe psoriasis after 24 weeks of treatment. These improvements are sustained through 52 weeks. The safety profile of DMF is similar to that previously described for fumarates.
EudraCT number
2017-00136840.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Dimethyl fumarate (DMF), a fumaric acid ester (FAE), is an oral formulation approved by the European Medicines Agency in 2017 to treat moderate-to-severe plaque psoriasis among adult patients requiring systemic therapy. However, limited data on its safety and efficacy are available in clinical practice apart from a few European countries. |
We assessed the efficacy and safety of DMF in patients with moderate-to-severe plaque psoriasis through 52 weeks in conditions similar to routine clinical practice in Spain, a country with no prior therapeutic experience with FAEs among dermatologists. |
What was learned from the study? |
The results presented herein confirm the favorable DMF efficacy and safety profiles for treating moderate-to-severe psoriasis throughout 52 weeks. |
An individualized adjustment of the DMF dosing based on patient tolerance and DMF effectiveness will eventually reduce dropout rates. |
Introduction
Psoriasis is a chronic, immune-mediated inflammatory skin disease with multifactorial etiology [1]. In Europe, the prevalence of psoriasis was approximately 2% [2], and about one-third of patients have moderate-to-severe psoriasis, which has been frequently associated to several comorbidities [3,4,5,6,7,8]. An estimated 80–90% of patients diagnosed with psoriasis have plaque psoriasis [9]. There are several available treatments for moderate-to-severe psoriasis, including biologics and non-biological systemic agents [10,11,12].
Dimethyl fumarate (DMF), a fumaric acid ester, is an oral formulation approved by the European Medicines Agency (EMA) to treat moderate-to-severe plaque psoriasis among adult patients requiring systemic therapy [13]. Although the EMA did not approve the use of DMF until 2017, fumaric acid esters (FAEs) have been extensively used in Germany since 1959, and the combination consisting of DMF and three salts of monoethyl fumarate (Fumaderm) was already registered by the German Drug Administration (BfArM) for treating severe psoriasis in 1994 [14]. Since its official registration, this FAE mixture has become the most frequently used systemic therapy for psoriasis in Germany. Clinical data from a phase 3 double-blind, placebo-controlled trial indicated that DMF was effective and comparable to the FAE mixture in treating adults with moderate-to-severe plaque psoriasis [15]. In addition, DMF showed a favorable safety with a comparable treatment-emergent adverse events (AEs) occurrence and severity, primarily mild, reported in the FAE mixture group [15]. Recently, DMF has shown a particularly interesting efficacy profile in special localizations such as the scalp, nails, palms, and/or soles, and in terms of itch relief [16].
Although DMF has been approved since 2017, limited data on its safety and efficacy are available in clinical practice apart from Germany and a few other European countries [17,18,19,20,21]. In addition, clinical studies evaluating treatments in routine clinical practice settings evaluate safety over more extended treatment periods and detect uncommon AEs, providing external validation to clinical trial data. Hence, the present study evaluated the efficacy of DMF in conditions similar to routine clinical practice for the first time in Spain, a country with no prior therapeutic experience with FAEs among dermatologists. The primary objective of this study was to assess the efficacy and safety of DMF in patients with moderate-to-severe plaque psoriasis through 52 weeks.
Methods
Study Design
DIMESKIN 1 was a 52-week, multicenter, open-label, phase IV clinical trial (EudraCT 2017-001368-40) conducted at 36 sites throughout Spain in adult patients with moderate-to-severe plaque psoriasis. This study was conducted according to the Declaration of Helsinki principles and approved by the ethics committee at each site, with the Hospital Universitario de la Princesa (Madrid, Spain) being the ethics committee of reference. All patients provided written informed consent.
Patients
Eligible patients were aged 18 years or older, with moderate-to-severe plaque psoriasis diagnosis for at least 6 months prior to baseline [defined as either Psoriasis Area and Severity Index (PASI) ≥ 10, body surface area (BSA) affected ≥ 10%, and PASI ≥ 5, or Dermatology Life Quality Index (DLQI) ≥ 10 and PASI ≥ 5], and candidates for systemic therapy. Women of childbearing potential were required to have a negative serum pregnancy test at screening and had to use medically accepted contraception methods during the trial. Main exclusion criteria were diagnosis of guttate, erythrodermic, or pustular psoriasis; white blood cell count less than 3000/µL or lymphocyte count less than 1000/µL; previous malignancy (except for non-melanoma skin cancer); significant gastrointestinal disorders (ulcers, diarrhea) at screening; severe renal impairment [glomerular filtration rate less than 30 mL/min/1.73 m2, using the Chronic Kidney Disease Epidemiology Collaboration equation [22] or significant proteinuria (3 + or higher), using test strip] at screening; abnormal liver enzymes (levels of aspartate aminotransferase, alanine aminotransferase, gamma-glutamyl transferase, or alkaline phosphatase greater than three times the upper limits of normal, or bilirubin levels greater than two times the upper limits of normal); active infectious disease; alcohol or drug abuse history; any other autoimmune disorder or current treatment with any immunosuppressive drug; previous use of biological drugs with antipsoriatic activity; conventional systemic antipsoriatic treatments (methotrexate, cyclosporine, acitretin), apremilast or phototherapy within 4 weeks of the study screening; and topical corticosteroids, vitamins A and D analogs, tar-based and salicylic acid preparations within 2 weeks of the screening.
Treatment
Patients were treated with DMF as per its summary of product characteristics, simulating conditions close to routine clinical practice. During the first 9 weeks of treatment, DMF was administered with gradual dose increases (Table 1). From weeks 10 to 52, patients could receive up to two tablets of DMF 120 mg three times daily. The maximum daily dose allowed was 720 mg of DMF. If ≥ 90% improvement in PASI (PASI 90) was observed before the maximum dose was reached, no further dose increase was recommended. If a dose increase was not tolerated, it might be temporarily reduced to the last tolerated dose. If white blood cell count was less than 3000/µL or lymphocyte count was less than 700/µL, the treatment must be discontinued. From week 24 onward, if PASI 75 or PASI ≤ 3 response was achieved, the daily dose might be reduced by one tablet less per day every 2 months until the required individual maintenance dose was reached.
Outcomes
Efficacy was assessed on the basis of PASI 50, PASI 75, PASI 90, and PASI 100 response rates (proportions of patients achieving ≥ 50%, ≥ 75%, ≥ 90%, and 100% improvement in PASI, respectively), absolute PASI scores ≤ 1, ≤ 3, and ≤ 5, BSA affected, and Physician’s Global Assessment (PGA) 0/1. Patient-reported outcomes were evaluated on the basis of pruritus visual analogue scale (VAS), DLQI (0/1 and ≤ 5), and treatment satisfaction VAS (i.e., 10-point scale, where a value of 10 represents maximum satisfaction with treatment and a value of 0 represents no satisfaction at all). Safety assessments consisted of frequency of AEs, serious AEs, and AEs leading to treatment discontinuation.
Statistical Analysis
The primary endpoint was the proportion of patients achieving PASI 75 response at week 24. Efficacy analyses were performed for the intention-to-treat (ITT) population, which included safety population patients with at least one post-baseline PASI value.
Post hoc efficacy analyses were performed for the following subgroups of patients from the ITT population: patients with a baseline VAS of pruritus ≥ 3, patients with moderate psoriasis at baseline (defining moderate disease according to PASI and DLQI thresholds proposed by Llamas-Velasco et al. [23], DLQI < 5 and absolute PASI 7–15 or DLQI ≥ 5 and absolute PASI ≤ 15), systemic-naïve patients, and patients with a baseline body mass index (BMI) ≥ 30 kg/m2.
Efficacy of DMF was also assessed per body region (head and neck, upper extremities, trunk, and lower extremities) by mean regional absolute PASI, mean percent improvement in regional PASI from baseline and percentage of patients achieving a severity level of 0–1 in signs of psoriasis (erythema, induration, and desquamation) at week 52, and excluding from the assessments those patients with PASI 0 at baseline for the body region. Each of the signs was rated on a 5-level scale of severity, ranging from 0 (absence) to 4 (very marked).
The presented analyses are based on multiple imputations (MI). Observed cases (OC) is presented as sensitivity analysis. Safety analyses were conducted on all patients who received at least one DMF dose (safety population). Medical Dictionary for Regulatory Activities system organ classes and preferred terms for AEs occurring at a frequency ≥ 5% are reported.
Sample Size
On the basis of 16-week data from the prior phase III DMF trial [15], a sample size of 300 patients was planned to offer a minimum precision (maximum margin of error considering the maximum indetermination [p = q = 50]) of 5.7% for estimating the primary endpoint (PASI 75 at week 24) with a confidence level of 95%.
Results
Study Population
Out of 300 patients enrolled in the trial, 18 were excluded owing to screening failure. Overall, 282 patients received at least one dose of the study medication (safety population), and 274 were included in the ITT population (Fig. 1).

Patient flowchart. AE adverse event, ITT intention-to-treat, PASI Psoriasis Area and Severity Index
Baseline patient characteristics are summarized in Table 2. A total of 66.1% of patients were male, and the mean [standard deviation (SD)] age was 46.6 (13.0) years. The mean (SD) time since diagnosis at the start of DMF was 18.2 (13.6) years, and patients had approximately two relapses in the last year. Overall, 89.8% of patients had received previous topical therapy for psoriasis, whereas 56.6% and 41.2% had received systemic therapy and phototherapy, respectively. Only 6.6% of patients did not receive any topical or systemic treatment in the past (Table 2).
Efficacy Outcomes
At weeks 24/52 (MI), a total of 46.0%/46.0% of patients treated with DMF achieved PASI 75 responses, 24.8%/21.9% achieved PASI 90 responses, and 10.9%/10.9% PASI 100 responses, respectively (Fig. 2). After 24/52 weeks of DMF treatment, mean absolute PASI decreased from 13.3 to 4.4/4.2 (MI) (p < 0.001, both) (Fig. 3a). The proportions of patients achieving absolute PASI ≤ 5, ≤ 3, and ≤ 1 are shown in Fig. 3b. Again, responses achieved at week 24 were maintained for up to 52 weeks. At weeks 24/52 (MI), patients with PASI ≤ 5, ≤ 3, ≤ 1 were 64.2%/67.9%, 46.4%/46.7%, and 21.5%/19.7%, respectively (Fig. 3b). Similar trends were obtained with OC analysis.

Evolution of PASI 50, PASI 75, PASI 90, and PASI 100 responses through week 52. MI multiple imputation, OC observed cases, PASI Psoriasis Area and Severity Index

PASI score at baseline and weeks 24/52 (a). Evolution of absolute PASI ≤ 1, ≤ 3, and ≤ 5 responses through week 52 (b). MI multiple imputation, OC observed cases, PASI Psoriasis Area and Severity Index
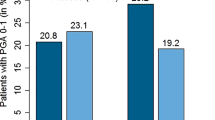
Mean BSA affected (MI) decreased from 17.4% at baseline to 6.9% after 24 weeks, and it was maintained up to week 52 (7.3%) (p < 0.001, both) (Fig. 4a). The proportion of patients who had a PGA 0–1 (MI) was 42.9% and 49.4% at week 24 and week 52, respectively (Fig. 4b).

BSA score at baseline and weeks 24/52 (a). Proportion of patients with PGA 0–1 at weeks 24/52 (b). *One patient had no BSA value at baseline. BSA body surface area, MI multiple imputation, OC observed cases, PGA Physician’s Global Assessment
Patient-Reported Outcomes
At baseline, a total of 64.6% of patients had a VAS of pruritus ranging from 7 to 10 (45.9% of patients after 4 weeks), with an overall mean (SD) of 6.9 (2.4), and a total of 254 patients (92.7%) had a baseline VAS of pruritus ≥ 3. After 24 and 52 weeks (MI), the mean VAS of pruritus decreased to 3.5 and 3.3, respectively (p < 0.001, both) (Fig. 5a), with most of the patients (56.5% and 67.6%, respectively) rating a VAS of pruritus < 3 (Fig. 5a, b). For those patients with a baseline VAS of pruritus ≥ 3 (n = 254), the mean VAS of pruritus decreased from 8.3 to 3.2 and 2.8 (MI) after 24 and 52 weeks of treatment, respectively.

Pruritus VAS score at baseline and weeks 24/52 (a). Evolution of mean pruritus VAS (MI and OC) and proportion of patients with pruritus VAS < 3 (OC) through week 52 (b). MI multiple imputation, OC observed cases, VAS visual analogue scale
Mean DLQI scores significantly improved from baseline to week 24 and were maintained through week 52 (Fig. 6a). After 24 weeks (MI), 61.3% of patients had a DLQI ≤ 5 and 34.7% had a DLQI 0–1. At week 52 (MI), the proportions of patients with DLQI ≤ 5 and DLQI ≤ 1 were 73.4% and 32.1%, respectively (Fig. 6b).

DLQI mean score at baseline and weeks 24/52 (a). Proportions of patients (MI) with DLQI ≤ 5 and 0–1 at baseline and weeks 24/52 (b). DLQI Dermatology Life Quality Index, MI multiple imputation, OC observed cases
Mean (SD) VAS of treatment satisfaction (OC) was 7.6 (2.7) and 8.4 (2.1) at week 24 and week 52, respectively.
Patients with Moderate Psoriasis
This subgroup of patients included 201 patients with moderate psoriasis at baseline. PASI scores improved from baseline to week 24 and were maintained until week 52. At week 24/52 (MI), a total of 50.2% and 62.5% of patients treated with DMF achieved PASI 75 responses, respectively. At weeks 24 and 52, mean (SD) absolute PASI decreased from 10.5 (0.5) to 3.7 (0.8) and 2.7 (0.6) (MI), respectively.
Mean (SD) VAS of pruritus (MI) at baseline was 7.7 (0.5), and after week 24/52 (MI), the mean (SD) VAS of pruritus decreased to 3.2 (0.6) and 2.7 (0.6), respectively. Baseline mean (SD) DLQI (MI) was 11.8 (1.4) and mean DLQI scores improved during the 52 weeks of treatment [mean DLQI 4.0 (1.1) and 2.4 (0.6) at weeks 24 and 52, respectively]. Mean (SD) VAS of treatment satisfaction (MI) was 8.4 (1.6) and 8.5 (1.7) at week 24 and week 52, respectively.
Systemic-Naïve Patients
A total of 119 patients were systemic-naïve at baseline. PASI scores improved from baseline to week 24 and week 52. At weeks 24 and 52, mean (SD) absolute PASI score decreased from 14.0 (1.3) to 4.1 (0.9) and 2.8 (0.7) (MI), respectively (Fig. 7). The proportions of patients achieving absolute PASI < 5 and < 3 showed that responses achieved at week 24 were maintained for up to 52 weeks. At weeks 24/52 (MI), patients with PASI < 5 and < 3 were 70.2%/82.3% and 51.8%/66.4%, respectively. Mean (SD) DLQI score (MI) at baseline was 13.3 (1.4) and mean DLQI scores improved during the 52 weeks of treatment [mean DLQI 4.2 (1.1) and 2.3 (0.6) at weeks 24 and 52, respectively]. After 24 weeks (MI), 72.1% of patients had a DLQI ≤ 5 and 46.0% had a DLQI 0-1. At week 52 (MI), the proportions of patients with DLQI ≤ 5 and DLQI ≤ 1 were 87.4% and 59.0%, respectively.

PASI score at baseline and weeks 24/52 among systemic-naïve patients. MI multiple imputation, OC observed cases, PASI Psoriasis Area and Severity Index
Patients with a BMI ≥ 30 kg/m2
There were 90 patients with a BMI ≥ 30 kg/m2 at baseline. PASI scores improved from baseline to week 24 and week 52. At weeks 24 and 52, mean (SD) absolute PASI score decreased from 13.5 (1.0) to 4.6 (1.0) and 3.0 (0.7) (MI), respectively. The proportions of patients achieving absolute PASI < 5 and < 3 showed that responses achieved at week 24 were maintained or increased at week 52. At weeks 24/52 (MI), patients with PASI < 5 and < 3 were 65.3%/81.2% and 52.3%/62.6%, respectively. Mean (SD) DLQI score (MI) at baseline was 11.0 (1.3) and mean DLQI scores improved during the 52 weeks of treatment [mean DLQI 4.2 (1.2) and 2.4 (0.7) at weeks 24 and 52, respectively]. After 24 weeks (MI), 74.0% of patients had a DLQI ≤ 5 and 44.4% had a DLQI 0-1. At week 52 (MI), the proportions of patients with DLQI ≤ 5 and DLQI ≤ 1 were 86.8% and 61.4%, respectively.
Efficacy Per Body Region
Regional PASI scores for patients treated with DMF improved from baseline to week 52 at all studied body regions (head, trunk, upper and lower extremities). Mean percent improvements in regional PASI scores (MI) increased from baseline up to week 24 (mean percentage improvement of 55.2%, 60.0%, 58.0%, and 62.4% for head, trunk, upper and lower extremities, respectively). These mean percent improvements were maintained or even increased after 52 weeks of treatment: 74.7% in the head, 76.7% in the trunk, 76.1% in the upper extremities, and 69.3% in the lower extremities. Regarding severity of erythema, induration, and desquamation by body region, at baseline more than half of the patients had moderate to very marked symptoms in all regions/symptoms except for head desquamation (45.3%). The proportion of patients with no symptoms or mild symptoms (MI) increased for all body regions, reaching at least 75% of the patients at weeks 24 and 52 (Table 3).
Safety Outcomes
During the 52-week treatment period, a total of 1586 AEs were recorded in 272 patients (i.e., 96.5% of the safety population). The most frequent AEs were gastrointestinal disorders (41.7% of all AEs), mainly diarrhea and abdominal pain (50.0% and 35.1% of patients, respectively), followed by flushing (28.0% of patients) and lymphopenia (31.2% of patients). Those AEs occurring at a frequency ≥ 5% are summarized by system organ class and preferred term in Table 4.
Most AEs were mild (69.2%) or moderate (27.1%) in intensity. Five serious AEs were reported: appendicitis, eosinophilia, acute hepatitis, ischemic stroke, and renal cell carcinoma, of which only eosinophilia was assessed as related to DMF. Patients were completely recovered in 82.3% of cases, and 87.4% of AEs did not require a temporary or permanent interruption of treatment. On the basis of the investigator’s opinion, 40.2% and 30.9% of AEs were considered related or possibly related to DMF, respectively (Table 5).
Reasons for Treatment Discontinuation
A total of 77 patients completed the 52-week treatment period, with clinically significant AEs (n = 101, 51.3% of patients) and consent withdrawal (n = 44, 22.3%) being the main reasons for study withdrawal (Fig. 1). The most common AEs leading to the withdrawal of therapy were gastrointestinal disorders (n = 48), with the majority (n = 43) occurring before study week 12, and lymphopenia (< 700 cells/µL, n = 42), with the majority (n = 41) occurring between weeks 12 and 52.
Discussion
Currently, many effective and well-established treatments for treating moderate-to-severe plaque psoriasis are available. Among them, FAEs represent a valuable treatment option with favorable efficacy and safety for adults with moderate-to-severe chronic plaque psoriasis. FAEs have been broadly used for many years in some European countries for treating psoriasis [17,18,19,20]. To our knowledge, few studies were performed in countries without prior therapeutic experience with FAEs, such as Spain. In this study we evaluated the efficacy and safety of DMF in conditions close to routine clinical practice in patients with moderate-to-severe psoriasis.
Overall, our results showed that almost half of the patients treated with DMF achieved PASI 75 response at week 24, and this response was sustained through 52 weeks (MI). These results are in line with those previously published showing that 37.5% and 40.3% of patients treated with DMF and FAE mixture, respectively, achieved PASI 75 response after 16 weeks of treatment [15]. In addition, PASI 90 and PASI 100 responses as well as absolute PASI response rates increased until week 24 and were also well maintained until week 52. The efficacy of DMF was similar regardless of the type of analysis (MI or OC). However, more conservative MI analysis resulted in lower response rates compared with OC due to dropout rates at the beginning of the study. In the recently published DIMESKIN 2 study [21], a multicenter, open-label study that aimed to evaluate the efficacy and long-term tolerability of DMF treatment in adults with moderate-to-severe chronic plaque psoriasis for up to 52 weeks in Italy, higher rates of patients achieved PASI 75, PASI 90, and PASI 100 (87.7%, 56.9%, and 24.6% of patients, respectively). In DIMESKIN 2, PASI 75 at 52 weeks was 86.7% in the MI approach.
In this study, DMF significantly improved both the BSA and PGA scores after 24 weeks of treatment, maintaining it up to week 52. The statistically significant decrease in BSA was aligned with that previously found in the BRIDGE trial, in which a decrease of BSA affected in patients treated with DMF was observed from week 3 onward, with continuous improvement by week 16 [15], and that recently found in DIMESKIN 2 [21]. Regarding the PGA, the BRIDGE trial reported 33.0% and 37.4% of patients treated with DMF and FAE mixture, respectively, who had a PGA score 0 or 1 (“clear” or “almost clear”) at week 16, percentages close to that found in our study at week 24 (around 40%) [15]. The DIMESKIN 2 study reported 81.5% of patients treated with DMF who had a PGA score of 0 or 1 [21].
A cut-off value for the VAS of pruritus < 3 points represents mild pruritus [24]. The impact of DMF treatment on pruritus was already observed after 4 weeks, showing an early effect of DMF on itch relief. DMF strongly improved pruritus after 24 weeks of treatment, maintaining a high proportion of patients rating a VAS of pruritus < 3 up to week 52. DMF had also a positive impact on quality of life of patients and treatment satisfaction. Mean DLQI scores improved significantly during the first 24 weeks of DMF treatment and were maintained through week 52. At week 24, two out of three patients showed a DLQI ≤ 5 and one out of three had a DLQI between 0 and 1. In addition, treatment satisfaction was in line with previous published data in psoriasis patients treated with FAEs [21, 25].
For obese patients, similar values for mean absolute PASI and DLQI after DMF treatment versus overall study population were observed, suggesting that DMF improves the main severity and extension indexes as well as quality of life in obese patients with moderate-to-severe psoriasis after 24 weeks of treatment and maintained up to 52 weeks. These results differ from those previously published for other psoriatic drugs, which showed that obese patients with psoriasis often experience a decreased efficacy compared with those who were not obese [26, 27]. However, a favorable and body-weight-independent response to FAEs has also been described [28].
This analysis through 52 weeks also suggests that DMF is effective for systemic-naïve patients in clinical practice and improves their quality of life. Mean absolute PASI scores described here at week 24 are in line with those previously published for FAEs [4.1 for DMF versus 4.6/5.1 (OC/mixed model repeated measures) for FAEs] [29]. Of note, a higher proportion of systemic-naïve patients achieved DLQI ≤ 1 (46.0%) at week 24 compared with previous published data for FAEs (14.8%) [30].
Regarding body region, our results showed DMF treatment efficacy for the four studied body regions (head, trunk, upper extremities, and lower extremities) and the three different signs (erythema, induration, and desquamation) among patients with moderate-to-severe plaque psoriasis in clinical practice. Mean percent improvement ranges in regional PASI at week 24 (55.2–62.4%) and at week 52 (69.3–76.7%) are close to those reported for the BRIDGE trial (from 62.2 to 69.2% at week 16) [16].
Compared with the BRIDGE study, the proportion of patients with AEs in our study was slightly higher (96.5% of patients versus 83.9% and 84.1% of patients in the DMF and FAE mixture groups, respectively, in the BRIDGE study) although the severity was similar (for instance, 69.2% AEs of mild severity versus 66.7% and 67.1% in the DMF and FAE mixture groups, respectively) [15]. In both studies, the most frequently reported AEs were gastrointestinal disorders (mainly diarrhea, abdominal pain, abdominal discomfort, vomiting, and nausea) [15]. Similarly, in an 8-month study with FAEs, 68% of patients had gastrointestinal and/or flushing AEs, which settled without intervention in most cases [17]. Overall, the safety profile of DMF was similar to that previously described with FAEs and DMF (with the most frequently reported AEs being gastrointestinal disorders, flushing, and white blood cell count abnormalities such as lymphopenia) [15, 31,32,33,34,35,36].
A European consensus group considered that FAEs have a favorable long-term safety profile but recommended managing patient expectations before starting treatment because AEs are mostly experienced during the onset of therapy [13]. In this study, clinically significant AEs represented the leading cause for treatment discontinuation (around 50% of study withdrawals) with this proportion being higher than that previously reported with DMF and FAEs among patients with psoriasis (around 20%) [15]. This discrepancy could be explained by our limited experience in the management of these drugs compared with that of countries that have used them for decades, as this study represents our first experience with DMF management.
Previous findings have reported lymphopenia as one of the most frequent AEs during DMF initiation or dose increase, leading to treatment discontinuation in some cases [13, 37, 38]. Lymphopenia was reported in 10.0% of patients receiving DMF for 16 weeks in the BRIDGE study [15]. These results slightly differ from those reported herein, as we found that the 31.2% of patients developed lymphopenia after 52 weeks of treatment, of which almost half (14.9% of the safety population) discontinued treatment owing to a lymphocyte count below 700 cells/µL. This increase could be explained through the DMF dose-escalation strategy and by the fact that in the current study, lymphopenias mainly started from week 12 onward, after the dose-increase phase, and we performed a longer follow-up (52 weeks versus 16 weeks). Concerning the gastrointestinal AEs, our results are in line with those published previously [15]. The BRIDGE study found that gastrointestinal symptoms were usually most bothersome during the first weeks of FAE treatment, decreasing their intensity in the subsequent weeks [15]. A non-interventional, retrospective analysis of data from 200 adult patients with psoriasis also found that gastrointestinal AEs were the main reason for DMF discontinuation during the first 6 months of treatment [39].
Overall, our results are also in accordance with recent real-world data in the use of DMF showing good effectiveness and safety in routine practice [40,41,42].
Some of the main limitations of this work arise from the inherent weakness associated with an open-label design, such as the risk of reporting bias, which may overestimate AEs because patients may have a greater tendency to report AEs associated with the drug. This fact could explain why we found a higher proportion of patients with AEs than previous studies with a blinded design. However, the longer follow-up should also be considered. Another limitation would be the attrition bias, which is introduced by the fact that patients leaving the study were likely to be different from those who completed. For instance, those with more severe AEs usually find it harder to adhere or continue to treatment and, therefore, are more likely to discontinue the study.
Conclusions
The results presented herein confirm the favorable DMF efficacy and safety profiles for treating moderate-to-severe psoriasis. DMF significantly improves the main severity and extension scores used in daily practice to assess psoriasis, as well as pruritus and quality of life after 24 weeks of treatment, maintaining these improvements through 52 weeks. The safety profile of DMF is similar to that previously described for fumarates, with gastrointestinal disorders being the majority of AEs during the first weeks of treatment. However, an individualized adjustment of the DMF dosing based on patient tolerance and DMF effectiveness will eventually reduce dropout rates in our setting.
References
Enamandram M, Kimball AB. Psoriasis epidemiology: the interplay of genes and the environment. J Invest Dermatol. 2013;133(2):287–9.
Parisi R, Iskandar IYK, Kontopantelis E, Augustin M, Griffiths CEM, Ashcroft DM, et al. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. Br Med J. 2020;369: m1590.
Armstrong EJ, Harskamp CT, Armstrong AW. Psoriasis and major adverse cardiovascular events: a systematic review and meta-analysis of observational studies. J Am Heart Assoc. 2013;2(2): e000062.
Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB. Risk of myocardial infarction in patients with psoriasis. JAMA. 2006;296(14):1735–41.
Candia R, Ruiz A, Torres-Robles R, Chávez-Tapia N, Méndez-Sánchez N, Arrese M. Risk of non-alcoholic fatty liver disease in patients with psoriasis: a systematic review and meta-analysis. J Eur Acad Dermatol Venereol. 2015;29(4):656–62.
Coto-Segura P, Eiris-Salvado N, González-Lara L, Queiro-Silva R, Martinez-Camblor P, Maldonado-Seral C, et al. Psoriasis, psoriatic arthritis and type 2 diabetes mellitus: a systematic review and meta-analysis. Br J Dermatol. 2013;169(4):783–93.
Gisondi P, Tessari G, Conti A, Piaserico S, Schianchi S, Peserico A, et al. Prevalence of metabolic syndrome in patients with psoriasis: a hospital-based case-control study. Br J Dermatol. 2007;157(1):68–73.
Conti A, Giovannini L, Mandel VD, Odorici G, Lasagni C, Bigi L, et al. Chronic kidney disease in psoriasis: a cohort study. J Dtsch Dermatol Ges. 2020;18(5):438–45.
Wilson FC, Icen M, Crowson CS, McEvoy MT, Gabriel SE, Kremers HM. Incidence and clinical predictors of psoriatic arthritis in patients with psoriasis: a population-based study. Arthritis Rheum. 2009;61(2):233–9.
Nast A, Gisondi P, Ormerod AD, Saiag P, Smith C, Spuls PI, et al. European S3-Guidelines on the systemic treatment of psoriasis vulgaris—update 2015—short version—EDF in cooperation with EADV and IPC. J Eur Acad Dermatol Venereol. 2015;29(12):2277–94.
Nast A, Spuls PI, van der Kraaij G, Gisondi P, Paul C, Ormerod AD, et al. European S3-Guideline on the systemic treatment of psoriasis vulgaris—update apremilast and secukinumab—EDF in cooperation with EADV and IPC. J Eur Acad Dermatol Venereol. 2017;31(12):1951–63.
Sbidian E, Chaimani A, Afach S, Doney L, Dressler C, Hua C, et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database Syst Rev. 2020;1:CD011535.
Mrowietz U, Barker J, Boehncke WH, Iversen L, Kirby B, Naldi L, et al. Clinical use of dimethyl fumarate in moderate-to-severe plaque-type psoriasis: a European expert consensus. J Eur Acad Dermatol Venereol. 2018;32(Suppl 3):3–14.
Mrowietz U, Asadullah K. Dimethylfumarate for psoriasis: more than a dietary curiosity. Trends Mol Med. 2005;11(1):43–8.
Mrowietz U, Szepietowski JC, Loewe R, van de Kerkhof P, Lamarca R, Ocker WG, et al. Efficacy and safety of LAS41008 (dimethyl fumarate) in adults with moderate-to-severe chronic plaque psoriasis: a randomized, double-blind, Fumaderm® - and placebo-controlled trial (BRIDGE). Br J Dermatol. 2017;176(3):615–23.
Mrowietz U, Van De Kerkhof P, Schoenenberger A, Ryzhkova A, Pau-Charles I, Llamas-Velasco M, et al. Efficacy of dimethyl fumarate treatment for moderate-to-severe plaque psoriasis: presentation extracts from the 29th EADV virtual congress, 29–31. Expert Rev Clin Immunol. 2020;2021:1–11.
Burden-Teh E, Lam M, Cohen S. Fumaric acid esters to treat psoriasis: Experience in a UK teaching hospital. J Am Acad Dermatol. 2013;68(4):AB52.
Carboni I, De Felice C, De Simoni I, Soda R, Chimenti S. Fumaric acid esters in the treatment of psoriasis: an Italian experience. J Dermatolog Treat. 2004;15(1):23–6.
Balasubramaniam P, Stevenson O, Berth-Jones J. Fumaric acid esters in severe psoriasis, including experience of use in combination with other systemic modalities. Br J Dermatol. 2004;150(4):741–6.
Heelan K, Markham T. Fumaric acid esters as a suitable first-line treatment for severe psoriasis: an Irish experience. Clin Exp Dermatol. 2012;37(7):793–5.
Pellacani G, Bigi L, Parodi A, Burlando M, Lanna C, Campione E, et al. Efficacy and safety of dimethyl fumarate in patients with moderate-to-severe plaque psoriasis: DIMESKIN-2, a multicentre single-arm phase IIIb study. J Clin Med. 2022;11(16):4778.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–12.
Llamas-Velasco M, de la Cueva P, Notario J, Martínez-Pilar L, Martorell A, Moreno-Ramírez D. Moderate psoriasis: a proposed definition. Actas Dermosifiliogr. 2017;108(10):911–7.
Reich A, Chatzigeorkidis E, Zeidler C, Osada N, Furue M, Takamori K, et al. Tailoring the cut-off values of the visual analogue scale and numeric rating scale in itch assessment. Acta Derm Venereol. 2017;97(6):759–60.
Fallah Arani S, Balak DMW, Neumann HaM, Kuipers MV, Thio HB. Treatment of psoriasis with non-registered fumaric acid esters in the Netherlands: a nationwide survey among Dutch dermatologists. J Eur Acad Dermatol Venereol. 2014;28(7):972–5.
Enos CW, Ramos VL, McLean RR, Lin TC, Foster N, Dube B, et al. Comorbid obesity and history of diabetes are independently associated with poorer treatment response to biologics at 6 months: a prospective analysis in Corrona Psoriasis Registry. J Am Acad Dermatol. 2022;86(1):68–76.
Blauvelt A, Armstrong AW, Langley RG, Gebauer K, Thaçi D, Bagel J, et al. Efficacy of guselkumab versus secukinumab in subpopulations of patients with moderate-to-severe plaque psoriasis: results from the ECLIPSE study. J Dermatol Treat. 2022;33(4):2317–24.
Reich K, Mrowietz U, Sorbe C, von Kiedrowski R, Diemert S, Schaeffer L, et al. Response to fumaric acid esters for plaque type psoriasis in real-world practice is largely independent of patient characteristics at baseline—a multivariable regression analysis from the German Psoriasis Registry PsoBest. J Dermatol Treat. 2022;1–8.
Pinter A, Hoffmann M, Reich K, Augustin M, Kaplan K, Gudjónsdóttir SD, et al. A phase 4, randomized, head-to-head trial comparing the efficacy of subcutaneous injections of brodalumab to oral administrations of fumaric acid esters in adults with moderate-to-severe plaque psoriasis (CHANGE). J Eur Acad Dermatol Venereol. 2021;35(3):701–11.
Reich K, Augustin M, Thaçi D, Pinter A, Leutz A, Henneges C, et al. A 24-week multicentre, randomized, open-label, parallel-group study comparing the efficacy and safety of ixekizumab vs. fumaric acid esters and methotrexate in patients with moderate-to-severe plaque psoriasis naive to systemic treatment. Br J Dermatol. 2020;182(4):869–79.
Wain EM, Darling MI, Pleass RD, Barker JNWN, Smith CH. Treatment of severe, recalcitrant, chronic plaque psoriasis with fumaric acid esters: a prospective study. Br J Dermatol. 2010;162(2):427–34.
Harries MJ, Chalmers RJG, Griffiths CEM. Fumaric acid esters for severe psoriasis: a retrospective review of 58 cases. Br J Dermatol. 2005;153(3):549–51.
Brück J, Dringen R, Amasuno A, Pau-Charles I, Ghoreschi K. A review of the mechanisms of action of dimethylfumarate in the treatment of psoriasis. Exp Dermatol. 2018;27(6):611–24.
van Hezik DFC, Bovenschen HJ. Association of lymphopenia and eosinophilia with dimethylfumarate treatment efficacy and tolerability in psoriasis: a retrospective study. J Dermatolog Treat. 2020;31(4):378–81.
Reszke R, Szepietowski JC. A safety evaluation of dimethyl fumarate in moderate-to-severe psoriasis. Expert Opin Drug Saf. 2020;19(4):373–80.
Balak DMW, Gerdes S, Parodi A, Salgado-Boquete L. Long-term safety of oral systemic therapies for psoriasis: a comprehensive review of the literature. Dermatol Ther (Heidelb). 2020;10(4):589–613.
Mrowietz U, Christophers E, Altmeyer P. Treatment of psoriasis with fumaric acid esters: results of a prospective multicentre study. German Multicentre Study. Br J Dermatol. 1998;138(3):456–60.
Mrowietz U, Altmeyer P, Bieber T, Röcken M, Schopf RE, Sterry W. Treatment of psoriasis with fumaric acid esters (Fumaderm). J Dtsch Dermatol Ges. 2007;5(8):716–7.
Termeer C, Reinhold U, Dirschka T, von Kiedrowski R, Kurzen H. Long-term use of fumaric acid esters for the treatment of psoriasis in daily practice. J Dermatol Treat. 2021;32(6):610–6.
Augustin M, Landeck L, Diemert S, Asadullah K, Hammann U, Ertner K, et al. Long-term treatment with dimethyl fumarate for plaque psoriasis in routine practice: good overall effectiveness and positive effect on impactful areas. Dermatol Ther (Heidelb). 2022;12(5):1121–31.
Pezzolo E, Cazzaniga S, Di Leo S, Naldi L, PsoReal Study Group. Efficacy and safety of Dimethyl fumarate in comparison with conventional therapy for psoriasis: an Italian real-world clinical experience. J Eur Acad Dermatol Venereol. 2022;36(7):e534–7.
Rosés Gibert P, de la Torre Gomar FJ, Saenz Aguirre A, Gimeno Castillo J, González PR. Dimethyl fumarate as therapeutic alternative in moderate-to-severe psoriasis: our experience. Psoriasis (Auckl). 2022;12:177–85.
Acknowledgements
The authors would like to acknowledge both the patients and physicians without whom this DIMESKIN-1 Study would not have been possible.
Funding
Sponsorship for this study, and the journal’s Rapid Service Fee, were funded by Almirall S.A., Barcelona, Spain.
Medical Writing, Editorial, and Other Assistance
Editorial assistance and medical writing support were provided by Anaïs Estrada-Gelonch, TFS HealthScience and Paula Casajust, TFS HealthScience. Support for this assistance was funded by Almirall S.A., Barcelona, Spain.
Author Contributions
Esteban Daudén and José Manuel Carrascosa contributed to the conception and study design, data collection, analysis and interpretation, and draft manuscript preparation. Pablo de la Cueva, Laura Salgado-Boquete, Mar Llamas-Velasco and Eduardo Fonseca contributed to the data collection and draft manuscript preparation. Ignasi Pau-Charles, David Asensio and Meritxell Guilà contributed to the writing of the manuscript. All authors read and approved the final manuscript.
Disclosures
Esteban Daudén received payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Abbvie/Abbott, Almirall, Amgen, Astellas, Centocor Ortho Biotech Inc., Galderma, Glaxo, Janssen-Cilag, Leo Pharma, Novartis, Pfizer, MSD-Schering-Plough, Celgene, Lilly, and UCB; and support for attending meetings and/or travel from Abbvie/Abbott, Almirall, Amgen, Astellas, Centocor Ortho Biotech Inc., Galderma, Glaxo, Janssen-Cilag, Leo Pharma, Novartis, Pfizer, MSD-Schering-Plough, Celgene, Lilly, and UCB. Pablo de la Cueva received consulting fees from Abbvie, Almirall, Pfizer, Lilly, UCB, Novartis, Leo Pharma, and Janssen; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Abbvie, Almirall, Pfizer, Lilly, UCB, Novartis, Leo Pharma, and Janssen; payment for expert testimony from Abbvie; support for attending meetings and/or travel from Abbvie, Almirall, Pfizer, Lilly, UCB, Novartis, Leo Pharma and Janssen; and participation on a Data Safety Monitoring Board or Advisory Board from Abbvie, Almirall, Pfizer, Lilly, UCB, Novartis, Leo Pharma and Janssen. Laura Salgado-Boquete received grants or contracts from Abbvie, Almirall, Amgen, Janssen Cilag, Leo Pharma, Novartis, Pfizer, Celgene, Lilly, Sandoz, Gebro, UCB, Bristol-Myers Squibb, and Eucerin; consulting fees from Abbvie, Almirall, Amgen, Janssen-Cilag, Leo Pharma, Novartis, Celgene, Lilly, Sandoz, UCB, Bristol-Myers Squibb, and Eucerin; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Abbvie, Almirall, Amgen, Janssen-Cilag, Leo Pharma, Novartis, Celgene, Lilly, Sandoz, UCB, Bristol-Myers Squibb, and Eucerin; support for attending meetings and/or travel from Abbvie, Almirall, Amgen, Janssen-Cilag, Leo Pharma, Novartis, Celgene, Lilly, and UCB; and participation on a Data Safety Monitoring Board or Advisory Board from Abbvie, Almirall, Amgen, Janssen-Cilag, Leo Pharma, Novartis, Celgene, Lilly, Sandoz, UCB, and Bristol-Myers Squibb. Mar Llamas-Velasco received payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Abbvie, Amgen, Janssen-Cilag, Leo Pharma, Novartis, Lilly and Celgene; support for attending meetings and/or travel from Abbvie, Amgen, Janssen-Cilag, Leo Pharma, Novartis, Lilly and Celgene; and participation on a Data Safety Monitoring Board or Advisory Board from Abbvie, Amgen, Janssen-Cilag, Leo Pharma, Novartis, Lilly and Celgene. Eduardo Fonseca received payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Abbvie, Novartis, Amgen, Leo, and Almirall; and participation on a Data Safety Monitoring Board or Advisory Board from Pfizer. Ignasi Pau-Charles, David Asensio and Meritxell Guilà are employees of Almirall. José Manuel Carrascosa received grants or contracts from Janssen, Novartis, and Almirall; consulting fees from Janssen, Novartis, Almirall, Abbvie, Pfizer, Lilly, Amgen, Leo, Sandoz, UCB, IM, UMS, Galderma, and Sanofi; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Janssen, Novartis, Almirall, Abbvie, Pfizer, Lilly, Amgen, Leo, Sandoz, UCB, IM, UMS, Galderma, and Sanofi; payment for expert testimony from Janssen, Novartis, Almirall, Abbvie, Pfizer, Lilly, Amgen, Leo, Sandoz, UCB, IM, UMS, Galderma, and Sanofi; support for attending meetings and/or travel from Lilly, and Almirall; and receipt of equipment, materials, drugs, medical writing, gifts or other services from Pfizer, and Leo.
Prior Presentation
Partial results presented in this paper were displayed at the 30th EADV Congress, which took place from September 29 to October 2, 2021.
Compliance with Ethics Guidelines
This study was performed in accordance with good clinical practice guidelines and the Helsinki Declaration of 1964 and its later amendments. The study received approval from the ethics committee at each site, being the Hospital Universitario de la Princesa (Madrid, Spain) the ethics committee of reference. All participants provided written informed consent to participate in the study.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Study Investigators
The full list of study investigators included: Mario Linares, Hospital Puerta del Mar; Antonio Vélez, Complejo Hospitalario Reina Sofía; Mireia Yébenes, Hospital Parc Taulí; Jordi Mollet, Hospital Universitari Vall d’Hebron; Jesús Gardeazabal, Hospital Universitario de Cruces; Ángeles Flórez, Complejo Hospitalario Universitario de Pontevedra; José Suárez, Complejo Hospitalario Universitario Nuestra Señora de Candelaria; Susana Armesto, Hospital Universitario de Valdecilla; Almudena Fernández, Complejo Hospitalario Virgen Macarena; José Carlos Ruiz, Complejo Hospitalario Universitario de Granada; Enrique Herrera, Complejo Hospitalario Virgen de la Victoria; Lourdes Rodríguez, Complejo Hospitalario Regional Virgen del Rocío; Mariano Ara, Hospital Universitario Lozano Blesa; Gregorio Carretero, Complejo Hospitalario Universitario de Gran Canaria Dr. Negrín; Carmen Delgado, Hospital Clínico Universitario de Valladolid; Noemí Eiris, Complejo Asistencial Universitario de León; Carlos Ferrandiz, Hospital Universitari Germans Trias i Pujol de Badalona; Lluís Puig, Hospital de la Santa Creu i Sant Pau; Ramón María Pujol, Hospital del Mar; Ander Zulaica, Hospital Meixoeiro; Raquel Rivera, Hospital Universitario 12 de Octubre; Natalia Jiménez, Hospital Ramón y Cajal; Pedro Herranz, Complejo Universitario La Paz; María Carmen Fariña, Hospital Universitario Fundación Jiménez Díaz; Rosa María Izu, Hospital de Basurto; Isabel Belichón-Romero, Hospital General Universitario de Alicante; Rafael Botella, Hospital Universitari i Politècnic La Fe; José Luis Sánchez-Carazo, Consorcio Hospital General Universitario de Valencia; Mercè Alsina, Hospital Clínic de Barcelona; José Luis López Estebaranz, Hospital Universitario Fundación Alcorcón; Beatriz Pérez, Hospital General Universitario Morales Meseguer; and Juan Ignacio Yanguas, Complejo Hospitalario de Navarra.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Daudén, E., de la Cueva, P., Salgado-Boquete, L. et al. Efficacy and Safety of Dimethyl Fumarate in Patients with Moderate-to-Severe Plaque Psoriasis: Results from a 52-Week Open-Label Phase IV Clinical Trial (DIMESKIN 1). Dermatol Ther (Heidelb) 13, 329–345 (2023). https://doi.org/10.1007/s13555-022-00863-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-022-00863-2