
Abstract
Introduction
Trimethylamine N-oxide (TMAO), a gut microbiota metabolite from dietary phosphatidylcholine, is involved in the pathogenesis of atherosclerosis and cardiovascular diseases. Psoriasis is associated with increased cardiovascular risk that is not captured by traditional biomarkers. The aim of the present study was to assess TMAO concentration in psoriasis and evaluate the relationship between TMAO and cardiovascular risk in psoriatic patients.
Methods
In 72 patients with psoriasis and 40 age- and sex-matched non-psoriatic controls, we evaluated fasting plasma TMAO, measured by high-performance liquid chromatography, and cardiovascular risk assessed by various scoring systems such as Framingham, QRISK2, AHA/ACC, and Reynolds risk scores.
Results
In patients with psoriasis, TMAO concentration was significantly higher than in the control group (195.68 [133.54–332.58] ng/ml versus 126.06 [84.29–156.88] ng/ml, respectively; p < 0.001). Plasma TMAO concentration was significantly correlated with age, total cholesterol, triglycerides, systolic and diastolic blood pressure. Furthermore, the receiver-operating characteristic (ROC) and multiple regression analysis showed that TMAO is an independent predictor of cardiovascular risk.
Conclusion
TMAO is a valuable candidate for biomarker and a translational link between dysbiosis and atherosclerosis in psoriasis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
A growing amount of evidence suggests a role of gut microbiota in the development of atherosclerosis and cardiovascular diseases. Specifically, a gut microbial metabolite, trimethylamine N-oxide (TMAO), has been intensively studied as a mediator between intestinal dysbiosis and vascular pathology. |
The disrupted gut barrier in psoriasis may promote translocation of bacterial metabolites into systemic circulation. |
The aim of our study was to assess plasma concentration of TMAO in patients with psoriasis and investigate its potential connection with cardiovascular risk. |
What was learned from the study? |
Plasma TMAO concentration is significantly increased in patients with psoriasis compared with age-, sex-, and body mass index (BMI)-matched nonpsoriatic subjects. |
Concentrations of TMAO were found to be an independent predictor of higher Framingham cardiovascular risk score in patients with psoriasis, even after adjustment for traditional risk factors. |
Digital Features
This article is published with digital features, including a summary slide, to facilitate understanding of the article. To view digital features for this article, go to https://doi.org/10.6084/m9.figshare.14510130.
Introduction
Psoriasis is a chronic inflammatory skin disease associated with accelerated development of atherosclerotic lesions and, consequently, a high incidence of cardiovascular diseases [1]. Large population studies suggest that patients with moderate-to-severe plaque psoriasis have an up to threefold higher risk of cardiovascular events, and significantly reduced life expectancy when compared with matched controls [2,3,4]. Importantly, even mild psoriasis increases the risk of myocardial infarction [4].
Several studies confirmed aortic vascular inflammation in psoriasis [5,6,7]. Endothelial inflammatory activation is an established feature of the atherosclerosis process, which may be measured by [18F]-fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT). However, high cost, complex and time-consuming methodology, and patient’s exposure to a prolonged radiation limit the use of this diagnostic test in clinical practice. Therefore, there is an urgent need to identify circulating biomarkers for more precise stratification of psoriatic patients who are at increased risk for developing major adverse cardiovascular events.
A growing amount of evidence suggests a role of gut microbiota in the development of atherosclerosis and cardiovascular diseases [8, 9]. Specifically, a gut microbial metabolite, trimethylamine N-oxide (TMAO), has been intensively studied as a mediator between intestinal dysbiosis and vascular pathology. Plasma TMAO is a metabolite derived from dietary precursors (choline, phosphatidylcholine, and l-carnitine), through the activity of gut microbiota [10]. Several studies have revealed a relation between plasma TMAO concentration and cardiovascular diseases, such as myocardial infarction, chronic heart failure, atrial fibrillation, or stroke [11,12,13,14]. Fecal microbial transplantation in a murine model demonstrated the role of intestinal microbiota in transmission of atherosclerosis susceptibility and overall TMAO production [15].
Our previous study confirmed altered intestinal barrier integrity in patients with chronic plaque psoriasis [16,17,18]. The disrupted gut barrier may promote translocation of bacterial metabolites into the systemic circulation. However, this hypothesis has not yet been evaluated in patients with psoriasis. The aim of our study was to assess plasma concentration of TMAO in patients with psoriasis and investigate its potential connection with cardiovascular risk.
Methods
Subject
All adult patients diagnosed with plaque psoriasis at least 6 months prior to the study visit and not receiving systemic treatment or phototherapy in the previous 3 months were screened for inclusion in this cross-sectional study. Patients were recruited from the Department of Dermatology at Medical University of Warsaw between January 2019 and December 2019.
Exclusion criteria included concomitant chronic gastrointestinal disorder, gastrointestinal infection during the last 3 months prior to the study, dietary restrictions during the last 3 months, intake of agents modulating gut microbiota (proton pump inhibitors, antibiotics, probiotics or prebiotics) within the previous 3 months, unexplained weight loss and major surgery (previous 6 months), chronic liver and pancreatic disease, other autoimmune diseases aside form psoriasis and/or psoriatic arthritis, congestive heart failure (NYHA class III or IV), estimated glomerular filtration rate (eGFR) of < 60 ml/min/1.73 m2, pregnancy, and breastfeeding.
The control group consisted of individuals matched for age, sex, and body mass index (BMI). Control group subjects followed the same exclusion criteria.
Clinical Assessment
All patients underwent a complete physical examination, and detailed medical history was obtained for all participants. Demographic and clinical data including sex, age, height, weight, blood pressure, psoriasis duration, abuse history, comorbidities, and use of medications were recorded for all subjects.
Psoriasis severity was measured according to Psoriasis Area and Severity Index (PASI). To rule out interobserver variations, PASI was assessed by the same dermatologist in all cases.
Various validated cardiovascular risk scores were calculated, such as Framingham Risk Score (FRAM) [19], QRISK2 [20], Atherosclerotic Cardiovascular Disease 2013 Risk Calculator from AHA/ACC (American Heart Association/American College of Cardiology) [21] Systematic COronary Risk Evaluation (SCORE) [22], and Reynolds Risk Score (RRS) [23].
Laboratory Assessment
The laboratory measurements included complete blood count (CBC), C-reactive protein, fasting blood glucose, total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, creatinine, aspartate aminotransferase (AST), and alanine aminotransferase (ALT).
Routine clinical laboratory tests were performed in the Hospital Clinical Laboratory. The estimated glomerular filtration rate (eGFR) was calculated using the Cockcroft–Gault equation.
Blood samples were taken from the cubital vein of all subjects after 8–10 h of fasting. Serum was immediately separated and stored at −70 °C until analysis.
Plasma TMAO concentration was determined using liquid chromatography coupled with triple-quadrupole mass spectrometry as described previously [24, 25]. Briefly, 10 μl of sample was mixed with 100 μl of acetone containing internal standards. After centrifugation, an aliquot was analyzed. The mass spectrometer operated in the multiple-reaction monitoring–positive electrospray ionization mode. The ion transitions used for TMAO quantitation were m/z 76 → 58. The TMAO calibration curve range was 0.1–60 μg/ml, and the limit of quantification was 0.1 μg/ml.
Ethics
The study was approved by the Regional Bioethical Committee (RBC) at Medical University of Warsaw. A written informed consent was obtained from all participants. The study was carried out in accordance with the Declaration of Helsinki and was approved by the Bioethical Committee of the Medical University of Warsaw.
Statistical Analysis
Continuous data are presented as mean ± standard deviation (SD) for normal or median with interquartile range (IQR) for non-normally distributed data. Categorical data are expressed as frequencies (number of cases and percentages). The Shapiro–Wilk test was used to assess the normality assumption of continuous variables. Normally distributed continuous variables were assessed with Student’s t test or one-way analysis of variance (ANOVA), while non-normally distributed continuous variables were assessed through Mann–Whitney U test or Kruskal–Wallis test, as appropriate. For comparing categorical data, χ2 test was performed. Spearman’s correlation coefficient was used to evaluate the correlation between two continuous variables. Multiple linear regression analysis with a forward-stepwise procedure was applied to determine the parameters most predictive of cardiovascular risk score. Regression analysis data are reported as a beta coefficient with standard error and p value. The receiver-operating characteristic (ROC) curve analysis was applied for testing sensitivity and specificity. A p value < 0.05 was considered statistically significant. All statistical analyses were performed with STATISTICA 13 software (StatSoft, Inc., USA).
Results
In total, 72 patients with psoriasis and 40 nonpsoriatic controls were enrolled in the present study. Table 1 presents the demographic and clinical characteristics of the two groups. Subjects were well matched for age, sex, BMI, and comorbidities.
TMAO concentration was significantly higher in psoriasis patients than in the control group: 195.68 [133.54–332.58] ng/ml and 126.06 [84.29–156.88] ng/ml, respectively; p < 0.001 (Fig. 1). Psoriatic patients with nonalcoholic fatty liver disease (NAFLD) had significantly higher TMAO in comparison with patients without liver disease (243.69 [165.55–382.45] ng/ml and 140.82 [95.53–238.16] ng/ml, respectively; p < 0.001). A similar trend was observed in patients with psoriasis and concomitant hypertension (333.12 [224.39–450.65] ng/ml) compared with normotensive psoriatic patients (145.69 [100.24–237.22] ng/ml; p < 0.001).

Plasma concentration of trimethylamine N-oxide (TMAO). Results presented as median and interquartile range
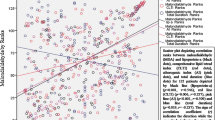
Plasma TMAO concentration was strongly correlated with all analyzed cardiovascular risk scores (FRAM r = 0.68, p < 0.001; QRISK2 r = 0.66, p < 0.001; AHA/ACC r = 0.55, p < 0.001; SCORE r = 0.51, p < 0.001; RRS r = 0.65, p < 0.001). Other characteristics significantly correlated with TMAO included age, total cholesterol, triglycerides, and systolic and diastolic blood pressure. A detailed list of correlations is presented in Table 2.
Further, patients with psoriasis were categorized according to the tertiles of plasma TMAO concentration. As presented in Table 3, subjects with higher TMAO were more likely to be older, be obese, and have hypertension or NAFLD. Cardiovascular risk scores showed a significantly higher value with increased TMAO tertiles. In contrast, a history of smoking, concomitance of psoriatic arthritis, and PASI score were similar across three groups.
When patients were grouped according to Framingham Risk Score, low cardiovascular risk was seen in 53% (38/72) and intermediate-to-high risk in 47% (34/72) of psoriatic patients. Statistically significant differences were observed between groups with respect to age, smoking, comorbidities (NAFLD, hyperlipidemia, hypertension, diabetes), lipid profile, and systolic and diastolic blood pressure, as well as concentration of TMAO (Table 4). The results of multiple regression analyses to identify factors associated with Framingham Score in patients with psoriasis are presented in Table 5 and confirmed a significant association of TMAO with cardiovascular risk.
At last, to assess the predictive power of TMAO for cardiovascular risk, we performed an ROC analysis. Our results showed that the area under curve (AUC) of TMAO was 0.913 (95% CI 0.848–0.979, p < 0.001, Fig. 2). Plasma TMAO concentration around 210.63 ng/ml is a cutoff for intermediate-to-high cardiovascular risk score. Patients with TMAO concentration above the cutoff threshold showed higher values of age, total cholesterol, triglycerides, systolic blood pressure, and estimated cardiovascular risk (Table 6).

ROC for predictive values of plasma TMAO concentration in detecting intermediate-to-high cardiovascular risk according to Framingham Risk Score
Discussion
This is the first study demonstrating that plasma TMAO concentration is significantly increased in patients with psoriasis compared with age-, sex-, and BMI-matched nonpsoriatic subjects. Increased TMAO level was associated with age, NAFLD, hypertension, hyperlipidemia, and risk of cardiovascular diseases as assessed by various cardiovascular risk scoring systems. Furthermore, concentrations of TMAO were found to be an independent predictor of higher Framingham cardiovascular risk score in patients with psoriasis, even after adjustment for traditional risk factors.
Patients with psoriasis are at greater risk for developing and dying from a myocardial infarction [2]. The risk of other vascular complications in psoriasis is also increased, including stroke [26], peripheral vascular disease [27], and thromboembolism [28]. Additionally, this increased cardiovascular risk is more pronounced in younger patients than in the general population. Therefore, there is a need for novel biomarkers that, in combination with traditional cardiovascular risk assessment, may improve risk stratification and enhance the selection of patients for preventative strategies [29].
Premature atherosclerosis in psoriasis is associated with endothelial dysfunction caused by an inflammatory process and concomitant diseases, such as insulin resistance, obesity, hyperlipidemia, or hypertension [30, 31]. Recent studies suggest that alteration in gut microbiome composition is another factor that may influence formation and progression of atherosclerotic plaque [32]. Moreover, gut dysbiosis has also been linked to psoriasis and its comorbidities [33]. One of the current hypotheses for the pathophysiological mechanism linking alteration in gut microbiome with increased cardiovascular risk states that the bacterial metabolites are translocated via impaired gut barrier into the circulation and exert systemic effects [14]. Several studies confirmed intestinal barrier damage in psoriasis [16,17,18] as well as increased blood concentration of bacterial components (lipopolysaccharide, DNA) in psoriatic patients [34, 35].
One of the biologically active metabolites of gut microbiota, which has been extensively studied recently, is trimethylamine N-oxide. Intestinal microbial enzymes metabolize dietary l-carnitine, choline, and lecithin into a trimethylamine (TMA), which is subsequently oxidized to TMAO in the liver [10]. This is the first study comparing TMAO concentration in patients with psoriasis and nonpsoriatic controls. However, in psoriatic arthritis, TMAO concentration correlates significantly not only with joint involvement but also with severity of skin lesions [36]. We found no significant relationship between TMAO levels and the PASI score. It cannot be ruled out that the damage of the intestinal barrier increases not only because of the severity of psoriasis but also the duration of high disease activity.
It was shown that TMAO is involved in all stages of atherogenesis, from the initial plaque formation to the terminal stage of thrombotic complications [37]. Several mechanisms for the role of TMAO in the development of atherosclerosis have been proposed, including the modulation of inflammation, cholesterol metabolism, and platelet activity.
An increase in TMAO concentration stimulates the inflammatory response within endothelial and vascular smooth muscle cells by activation of mitogen-activated protein kinase (MAPK), a signaling cascade of nuclear factor-kB (NF-kB), activation of NLRP3 inflammasome, release of proinflammatory cytokines, and expression of adhesion molecules [38, 39]. In addition, TMAO significantly triggers oxidative stress, contributing to the decrease of nitric oxide availability and endothelial dysfunction [40, 41]. Other findings have reported that TMAO promotes atherosclerosis through formation of foam cells [42].
Hepatic flavin monooxygenase 3 (FMO3), the enzyme responsible for forming TMAO from gut microbe-generated TMA, appears to have a regulating function on lipid metabolism. Knockdown of FMO3 in mice on a high-cholesterol diet lowered intestinal lipid absorption and hepatic cholesterol production, and stimulated reverse cholesterol transport [43], while TMAO administration significantly increased concentrations of triglyceride, total cholesterol, and low-density lipoprotein cholesterol [44].
Lastly, TMAO was reported to augment the intracellular release of Ca2+ through adenosine diphosphate (ADP), thrombin, arachidonic acid, and collagen, increasing platelet reactivity, which promotes thrombosis [45].
Most of the cited studies were carried out in vitro or on animal models; however, clinical studies confirmed increased plasma TMAO concentration in myocardial infarction [13], stroke [11], and peripheral artery disease [46]. There is a growing number of articles suggesting that not TMAO itself, but rather its precursor—TMA, is responsible for toxic effects on the cardiovascular system [47, 48]. TMAO, as the product of oxygenation, may be a biomarker of the increased intestinal translocation of TMA. We assume that translocation of bacterial metabolites by altered intestinal barrier in psoriasis is a potential mechanism linking gut dysbiosis with increased cardiovascular risk.
Limitations of the study include its small sample size and cross-sectional nature. It should be mentioned that there are a number of other factors that influence cardiovascular risk, such as diet. The classic risk scoring scales may underestimate cardiovascular risk in patients with inflammatory disorders.
Conclusion
We showed increased concentration of TMAO in patients with psoriasis. A measurement of plasma TMAO can be a valuable biomarker for assessing cardiovascular risk in psoriasis. A better understanding of the causal relationship between psoriasis and TMAO may highlight several pathophysiological pathways for targeted therapies to reduce cardiovascular risk in psoriatic patients.
References
Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323:1945–60.
Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB. Risk of myocardial infarction in patients with psoriasis. JAMA. 2006;296:1735–41.
Valaiyaduppu Subas S, Mishra V, Busa V, et al. Cardiovascular involvement in psoriasis, diagnosing subclinical atherosclerosis, effects of biological and non-biological therapy: a literature review. Cureus. 2020;12:e11173.
Armstrong EJ, Harskamp CT, Armstrong AW. Psoriasis and major adverse cardiovascular events: a systematic review and meta-analysis of observational studies. J Am Heart Assoc. 2013;2:e000062.
Kim BS, Lee WK, Pak K, et al. Ustekinumab treatment is associated with decreased systemic and vascular inflammation in patients with moderate-to-severe psoriasis: feasibility study using (18)F-fluorodeoxyglucose PET/CT. J Am Acad Dermatol. 2019;80:1322–31.
Gelfand JM, Shin DB, Alavi A, et al. A phase IV, randomized, double-blind, placebo-controlled crossover study of the effects of ustekinumab on vascular inflammation in psoriasis (the VIP-U Trial). J Invest Dermatol. 2020;140:85–93.
Gelfand JM, Shin DB, Duffin KC, et al. A randomized placebo-controlled trial of secukinumab on aortic vascular inflammation in moderate-to-severe plaque psoriasis (VIP-S). J Invest Dermatol. 2020;140:1784–93.
Verhaar BJH, Prodan A, Nieuwdorp M, Muller M. Gut microbiota in hypertension and atherosclerosis: a review. Nutrients. 2020;12:2982.
Zhou W, Cheng Y, Zhu P, Nasser MI, Zhang X, Zhao M. Implication of gut microbiota in cardiovascular diseases. Oxid Med Cell Longev. 2020;2020:5394096.
Nowinski A, Ufnal M. Trimethylamine N-oxide: a harmful, protective or diagnostic marker in lifestyle diseases? Nutrition. 2018;46:7–12.
Farhangi MA, Vajdi M, Asghari-Jafarabadi M. Gut microbiota-associated metabolite trimethylamine N-oxide and the risk of stroke: a systematic review and dose-response meta-analysis. Nutr J. 2020;19:76.
Buttner P, Okun JG, Hauke J, et al. Trimethylamine N-oxide in atrial fibrillation progression. Int J Cardiol Heart Vasc. 2020;29:100554.
Bin Waleed K, Lu Y, Liu Q, et al. Association of trimethylamine N-oxide with coronary atherosclerotic burden in patients with non-ST-segment elevation myocardial infarction. Medicine (Baltimore). 2020;99:e20794.
Zhang Y, Wang Y, Ke B, Du J. TMAO: how gut microbiota contributes to heart failure. Transl Res. 2021;228:109–25.
Gregory JC, Buffa JA, Org E, et al. Transmission of atherosclerosis susceptibility with gut microbial transplantation. J Biol Chem. 2015;290:5647–60.
Sikora M, Chrabaszcz M, Maciejewski C, et al. Intestinal barrier integrity in patients with plaque psoriasis. J Dermatol. 2018;45:1468–70.
Sikora M, Chrabaszcz M, Waskiel-Burnat A, Rakowska A, Olszewska M, Rudnicka L. Claudin-3—a new intestinal integrity marker in patients with psoriasis: association with disease severity. J Eur Acad Dermatol Venereol. 2019;33:1907–12.
Sikora M, Stec A, Chrabaszcz M, et al. Intestinal fatty acid binding protein, a biomarker of intestinal barrier, is associated with severity of psoriasis. J Clin Med. 2019;8:1021.
Hemann BA, Bimson WF, Taylor AJ. The Framingham Risk Score: an appraisal of its benefits and limitations. Am Heart Hosp J. 2007;5:91–6.
Collins GS, Altman DG. An independent and external validation of QRISK2 cardiovascular disease risk score: a prospective open cohort study. BMJ. 2010;340:c2442.
Goff DC Jr, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S49-73.
Trzeciak B, Siebert J, Gutknecht P, Molisz A, Filipiak KJ, Wozakowska-Kaplon B. Cardiovascular risk factors determined via the Internet in 2 periods of time: 2004–2009 and 2010–2015 in Poland. Int J Occup Med Environ Health. 2017;30:499–510.
Ridker PM, Buring JE, Rifai N, Cook NR. Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: the Reynolds Risk Score. JAMA. 2007;297:611–9.
Jaworska K, Huc T, Samborowska E, et al. Hypertension in rats is associated with an increased permeability of the colon to TMA, a gut bacteria metabolite. PLoS ONE. 2017;12:e0189310.
Skrzypecki J, Izdebska J, Kaminska A, et al. Glaucoma patients have an increased level of trimethylamine, a toxic product of gut bacteria, in the aqueous humor: a pilot study. Int Ophthalmol. 2021;41:341–7.
Gelfand JM, Dommasch ED, Shin DB, et al. The risk of stroke in patients with psoriasis. J Invest Dermatol. 2009;129:2411–8.
Kimball AB, Robinson D Jr, Wu Y, et al. Cardiovascular disease and risk factors among psoriasis patients in two US healthcare databases, 2001–2002. Dermatology. 2008;217:27–37.
Rhee TM, Lee JH, Choi EK, et al. Increased risk of atrial fibrillation and thromboembolism in patients with severe psoriasis: a nationwide population-based study. Sci Rep. 2017;7:9973.
Sunbul M, Agirbasli M. Psoriasis and atherosclerosis: is there a need for novel biomarkers assessing cardiovascular risk? Curr Pharm Des. 2014;20:529–35.
Eder L, Gladman DD. Atherosclerosis in psoriatic disease: latest evidence and clinical implications. Ther Adv Musculoskelet Dis. 2015;7:187–95.
Puig L. Cardiometabolic comorbidities in psoriasis and psoriatic arthritis. Int J Mol Sci. 2017;19:58.
Yeh CF, Chen YH, Liu SF, et al. Mutual interplay of host immune system and gut microbiota in the immunopathology of atherosclerosis. Int J Mol Sci. 2020;21:8729.
Sikora M, Stec A, Chrabaszcz M, et al. Gut microbiome in psoriasis: an updated review. Pathogens. 2020;9:463.
Romani J, Caixas A, Escote X, et al. Lipopolysaccharide-binding protein is increased in patients with psoriasis with metabolic syndrome, and correlates with C-reactive protein. Clin Exp Dermatol. 2013;38:81–4.
Ramirez-Bosca A, Navarro-Lopez V, Martinez-Andres A, et al. Identification of bacterial DNA in the peripheral blood of patients with active psoriasis. JAMA Dermatol. 2015;151:670–1.
Coras R, Kavanaugh A, Boyd T, et al. Choline metabolite, trimethylamine N-oxide (TMAO), is associated with inflammation in psoriatic arthritis. Clin Exp Rheumatol. 2019;37:481–4.
Duttaroy AK. Role of gut microbiota and their metabolites on atherosclerosis, hypertension and human blood platelet function: a review. Nutrients. 2021;13:144.
Yang S, Li X, Yang F, et al. Gut microbiota-dependent marker TMAO in promoting cardiovascular disease: inflammation mechanism, clinical prognostic, and potential as a therapeutic target. Front Pharmacol. 2019;10:1360.
Boini KM, Hussain T, Li PL, Koka S. Trimethylamine-N-oxide instigates NLRP3 inflammasome activation and endothelial dysfunction. Cell Physiol Biochem. 2017;44:152–62.
Sun X, Jiao X, Ma Y, et al. Trimethylamine N-oxide induces inflammation and endothelial dysfunction in human umbilical vein endothelial cells via activating ROS-TXNIP-NLRP3 inflammasome. Biochem Biophys Res Commun. 2016;481:63–70.
Brunt VE, Gioscia-Ryan RA, Casso AG, et al. Trimethylamine-N-oxide promotes age-related vascular oxidative stress and endothelial dysfunction in mice and healthy humans. Hypertension. 2020;76:101–12.
Geng J, Yang C, Wang B, et al. Trimethylamine N-oxide promotes atherosclerosis via CD36-dependent MAPK/JNK pathway. Biomed Pharmacother. 2018;97:941–7.
Warrier M, Shih DM, Burrows AC, et al. The TMAO-generating enzyme flavin monooxygenase 3 is a central regulator of cholesterol balance. Cell Rep. 2015;10:326–38.
Ding L, Chang M, Guo Y, et al. Trimethylamine-N-oxide (TMAO)-induced atherosclerosis is associated with bile acid metabolism. Lipids Health Dis. 2018;17:286.
Zhu W, Gregory JC, Org E, et al. Gut microbial metabolite TMAO enhances platelet hyperreactivity and thrombosis risk. Cell. 2016;165:111–24.
Senthong V, Wang Z, Fan Y, Wu Y, Hazen SL, Tang WH. Trimethylamine N-oxide and mortality risk in patients with peripheral artery disease. J Am Heart Assoc. 2016;5:e004237.
Jaworska K, Bielinska K, Gawrys-Kopczynska M, Ufnal M. TMA (trimethylamine), but not its oxide TMAO (trimethylamine-oxide), exerts haemodynamic effects: implications for interpretation of cardiovascular actions of gut microbiome. Cardiovasc Res. 2019;115:1948–9.
Jaworska K, Hering D, Mosieniak G, et al. TMA, a forgotten uremic toxin, but not TMAO, is involved in cardiovascular pathology. Toxins (Basel). 2019;11:490.
Acknowledgements
The authors would like to thank the studies participants for their involvement in the trial.
Funding
This research and the journal’s Rapid Service Fee were funded by the Polish Ministry of Science and Higher Education, grant number MNiSW/2020/220/DIR/NN4.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Authorship Contributions
Conceptualization (M. Sikora, N. Kiss); Methodology (M. Sikora, J. Giebultowicz, E. Samborowska, R. Jazwiec, and M. Dadlez); investigation (M. Sikora, A. Stec, J. Giebultowicz, E. Samborowska, R. Jazwiec, and M. Dadlez); writing—original draft preparation (M. Sikora, N. Kiss, A. Stec); writing—review and editing, (J. Giebultowicz, E. Samborowska, R. Jazwiec, M. Dadlez, M. Olszewska and L. Rudnicka); supervision (M. Olszewska and L. Rudnicka).
Disclosures
Mariusz Sikora, Norbert Kiss, Albert Stec, Joanna Giebułtowicz, Emilia Samborowska, Radoslaw Jazwiec, Michal Dadlez, Malgorzata Olszewska and Lidia Rudnicka have nothing to disclose.
Compliance with Ethics Guidelines
The study was conducted according to the guidelines of the Declaration of Helsinki, and ap-proved by the Bioethical Committee of the Medical University of Warsaw (KB/106/2017 of 04 July 2017). Informed consent was obtained from all subjects involved in the study.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Sikora, M., Kiss, N., Stec, A. et al. Trimethylamine N-Oxide, a Gut Microbiota-Derived Metabolite, Is Associated with Cardiovascular Risk in Psoriasis: A Cross-Sectional Pilot Study. Dermatol Ther (Heidelb) 11, 1277–1289 (2021). https://doi.org/10.1007/s13555-021-00547-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-021-00547-3