
Abstract
Introduction
Previous studies have shown that psoriasis has a significant effect on patients’ health-related quality of life. The impact of psoriasis on household chores and the need for assistance with such tasks are not well documented. The aim of this study was to estimate the impact of psoriasis on the ability to carry out household chores, the time spent on skin care at home and the assistance that patients with psoriasis require with these activities.
Methods
In a questionnaire study 262 patients with moderate-to-severe psoriasis, visiting a tertiary level dermatological clinic during a 1-year study period, listed household chores which they considered were particularly affected by psoriasis. This was done without a predefined list of chores. Questions on their ability to perform household chores as well as time spent on skin care at home were asked. The need for outside assistance with household chores and help received were also determined.
Results
More than half of the patients (57.8%) reported difficulties with household chores because of psoriasis. Psoriasis affected a wide range of everyday household activities, with physically demanding tasks and those involving contact with water mentioned most often. Most of the patients (84.6%) reported that they have increased the time spent on skin care because of psoriasis, on average by 87 min per week. A quarter of patients received assistance in household chores. Women received more assistance than men (p < 0.01). The need for additional assistance was reported by a fifth of patients, women more often than men (p < 0.05).
Conclusion
When estimating the overall burden of psoriasis, considering only the economic and productivity consequences may underestimate the impact of the disease. The impact on everyday life events such as the ability to perform household chores should also be taken into account.
Funding
This study was supported by unconditional grants from the research funds of the Hospital District of Southwest Finland. Hospital District of Southwest Finland’s research permission K44/10/EVO13043.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
Introduction
The prevalence of psoriasis is 2–3% worldwide; approximately, 10–30% of patients with psoriasis also have arthritis and nail lesions [1]. Due to the chronic nature of the disease, psoriasis affects patients’ everyday life resulting in considerable burden both to the patients and to the community [2, 3].
Previous studies [3–8] have shown that psoriasis has a significant effect on patients’ health-related quality of life. The impact on quality of life was similar to that of many other chronic diseases and psychiatric conditions, and psoriasis has been estimated to cause as much disability as heart disease, diabetes, depression, cancer and chronic lung disease [7]. Psoriasis has been shown to have an impact on patients’ daily activities, occupation, sexual functioning and general behavior [5, 8, 9]. Patients may experience an adverse impact on emotional and social life, and on physical functioning due to the disease [4–7, 9]. Psoriasis has been reported to have a negative impact on different leisure time activities [9–11]. However, the impact of psoriasis on household chores and the need for assistance with such tasks remain unclear.
Psoriasis has considerable impact not only on patients but also on close family and friends. The secondary impact on the lives of family members and partners that has been identified included extra time spent on housework, social disruption, and limitations to holiday plans, sport, leisure activities and daily activities [12].
The aim of this study was to find out the type of household chores that were particularly affected by psoriasis and those where assistance is required. Also, our aim was to estimate the impact of psoriasis on the ability to perform household chores, time spent on skin care at home and the need of additional assistance.
Methods
Patient Sample
The sample was based on patients who had visited the Department of Dermatology in Turku University Hospital over a 1-year period. Patients were all diagnosed with psoriasis and some with psoriatic arthritis. In the Finnish health care system, patients with mild psoriasis are treated at primary health care settings and only moderate-to-severe cases are referred to tertiary level hospital for further treatment. The patients were sent a pretested and piloted questionnaire by mail; those who did not respond initially were sent the mailing again. A total of 498 patients attended the clinic during the study period (428 with psoriasis and 70 with psoriatic arthritis). Of them 262 completed the questionnaire (52.6%). Both groups of patients with psoriasis participated equally (patients with psoriatic arthritis comprised 12.9% of the original sample and 12.7% of the respondents). The mean age of the original sample (55.0 years) was lower (p < 0.05) than that of respondents (58.4 years). Women comprised 45% of both the original sample and the respondents. Details about the patient sample, diagnosis, age and gender distributions have been reported previously [10].
The ethics committee of the Hospital District of Southwest Finland approved the study, and the potential participants received information about the study purpose, as well as about the planned storage and use of the questionnaires. This was followed by a description of the subject’s rights according to the Declaration of Helsinki of 1964, as revised in 2013. Participation was voluntary. The patients were asked to give written consent to use their medical records for the study.
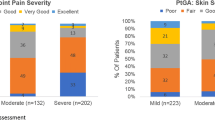
From the patient records of the respondents who had given consent, Psoriasis Area Severity Index (PASI, n = 72), Dermatology Life Quality Index (DLQI, n = 36) and diagnosis (ICD-10, n = 262) were collected to study the effects of the severity, burden and type of psoriasis on household chores. If there were many PASI or DLQI values from the same patient, the mean value for the study period was calculated and used in the analyses. Clinical status or other patient register data could not be retrieved without written consent, and more detailed comparison of the respondents and non-respondents was not possible.
Questionnaire
Current ability to perform household chores was assessed using a 10-cm-long visual analog scale from 0 to 100, where 0 on the left was labeled as an inability to perform at all and 100 on the right as an ability to perform without any difficulty. Respondents were asked: Mark an ‘X’ on the line, which corresponds to your current ability to perform household chores.
In the next stage, they were asked to mark an ‘X’ on the line corresponding to their ability to perform household chores in a hypothetical situation if they did not have psoriasis. The score indicating the perceived effect of psoriasis on the ability to perform household chores was defined as the difference between the scores currently and in a hypothetical situation without psoriasis.
The subjects were asked to list household chores that had been particularly affected by psoriasis, using their own words, i.e., they were neither provided with a predefined list of household chores nor given any restrictions which activities they could consider as household chores. The household chores listed were later analyzed and grouped into categories.
Next, the subjects were asked the time they spent on skin care, in general terms without specifying any particular type of care, by asking: How many minutes do you estimate you spent on skin care during the past week? After that, the patients were asked to estimate how many minutes they would have spent on skin care in a hypothetical situation if they did not have psoriasis. The difference in minutes used for skin care with and without psoriasis was computed.
In an identical manner, the time spent on cleaning and on laundry during the past week was assessed, as well as the time the patients would have spent on these household chores in a hypothetical situation without psoriasis. The differences in times spent on cleaning and laundry associated with having psoriasis was defined in the same manner as for skin care.
In the next stage, the patients were asked about assistance by asking: Do you get assistance for household chores from relatives or other helpers? Alternative answers being (a) no, and (b) yes, followed by: If yes, list the chores you are helped with_____. The household chores listed were later analyzed and grouped into categories.
Next patients were asked how many minutes of outside assistance with household chores they received per week.
The need for additional assistance was determined by asking: Do you get enough assistance with your household chores? Alternative answers being (a) yes, and (b) no, followed by: If no, how many more minutes of help per week do you need?
In addition to background socio-demographic information, the questionnaire examined years since the psoriasis diagnosis and work status.
Statistical Analysis
The statistical evaluation of the data was based on Fisher’s exact test and Chi-square test for proportions, and Student’s t test and one-way analysis of variance for means. Pearson’s coefficients of correlation were used to examine the degree of relationship between two continuous variables. Psoriasis and psoriatic arthritis diagnoses were used as background characteristic in all statistical comparisons. However, as there were no statistically significant differences between these diagnostic groups in any of the analyses conducted, these two patient groups were analyzed as one psoriasis group, using SPSS version 22 (SPSS Inc., Chicago, IL, USA).
Results
In total, 19 different aspects of household chores that were particularly affected by psoriasis were identified and assigned to four different domains: physically demanding chores and those requiring manual dexterity, chores with skin contact with water, social intercourse and other (Table 1). Women perceived significantly more often than men that activities related to cleaning were affected by psoriasis. Otherwise, differences between sexes were small (Table 1). In the same manner, household chores for which the patients received assistance were identified and assigned to three distinct categories: skin care, physically demanding chores and chores with skin contact with water (Table 2).
More than half of the patients (57.8%) reported disadvantage in performing household chores because of psoriasis. Among them, the mean score indicating the effect of psoriasis on the ability to perform household chores was −28.3. Almost a third (30.4%) reported that psoriasis had no impact on performing household chores and a tenth (11.8%) observed that they could perform tasks better with psoriasis. Patients with a more severe inability to perform household chores felt that the influence of psoriasis was more crucial (Table 3). Recorded DLQI values were on average 10.9 (SD 8.3) and PASI values 6.4 (SD 3.9). Patients who perceived a disadvantage in ability to perform household chores because of psoriasis had significantly (p < 0.05) higher DLQI (14.2) than those with no perceived disadvantage (7.7). There was no statistical difference in PASI values between these two groups (6.7 vs. 6.2). However, there was no statistically significant association between PASI or DLQI and the need for assistance in household chores.
Most of the patients (84.6%) reported that they had increased the time spent on skin care because of psoriasis. Patients estimated that they currently use 87 more minutes per week on skin care than if they did not have psoriasis (women estimated 73 min and men 98 min more; statistically non-significant). The average time spent on skin care with psoriasis was estimated at 116 min per week (ranging from 0 to 840 min) with no difference between sexes. A quarter of the patients (27.4%) had increased the time they spent cleaning and 15.3% had increased the time spent on laundry because of psoriasis. The overall amount of time spent performing cleaning and laundry when having psoriasis was estimated at 107 min and 66 min per week, respectively, with a significant difference between sexes for laundry (women 108 min and men 35 min, p < 0.05). On average, cleaning was performed for 4 min more per week and laundry 3 min more per week because of psoriasis.
Because of their psoriasis, more than a quarter of the patients received assistance with household chores, including skin care. Women received significantly more assistance than men, and women felt the need for additional assistance significantly more often than men (Table 2).
The impacts of patients’ age, the duration of the disease and work status were marginal and statistically non-significant in all analyzed characteristics of psoriasis and household chores.
Discussion
This study shows that psoriasis seems to have a mostly negative effect on the performance of household chores. In a large European study, the greatest impact of psoriasis was on activities of daily living, especially affecting clothing choice, bathing routine and sporting activities [13]. Another study of 330 outpatients with psoriasis showed that the majority reported reduction in one or more physical activity [14]. In this study, the household chores that were most affected by psoriasis were those that needed physical functioning, manual dexterity or skin contact with water. The physical symptoms of psoriasis (skin lesions and also joint symptoms in psoriatic arthritis) may cause difficulties and pain when moving and touching. Lesions could worsen when in contact with water and patients may feel uncomfortable, which may at least partly explain our findings. Psoriasis is also often a highly visible disease, e.g., with lesions on the scalp, neck and hands, and this could cause cosmetic disturbance and changes in patients’ social behavior. According to Sampogna et al. [9], feelings of shame because of psoriasis can have a strong impact on social life, since they can result in avoidance of public places, thus reducing social opportunities. This may have a potential impact on employment and relationships. Stigma may have been a factor for some patients in our study who reported an impact of psoriasis on some household chores (Table 1). However, relatively few patients mentioned any activities that could be categorized as social intercourse. If they had been provided with a predefined prompt list of activities that included mention of social life, it is possible that it would have been mentioned by a greater proportion of patients.
Those who reported performing household chores better with psoriasis than without have probably adapted well to living with their disease. Also, they may have succeeded in developing working methods that help them to perform household chores despite disease symptoms. Although the questionnaire was based on similar questionnaire that had been used among rheumatoid arthritis patients earlier [15] and it was piloted among psoriasis patients before use, there is still a possibility that some respondents have misunderstood the questions. However, the role of such source of bias cannot be determined.
Psoriasis symptoms vary over time. When we asked about the performance of household chores with psoriasis, we used the time frame “currently” to minimize the effects of symptom variation and recall bias. It may be difficult to remember the performance or the time used in certain household chores before psoriasis had started. Some patients may have had psoriasis all of their lives and others may have developed the disease in older age. Also, the burden of psoriasis on household chores could have changed during the years. Thus, for the situation without psoriasis, we used a hypothetical question in which the patient imagines that he/she does not have psoriasis, without a definite time frame, which was expected to decrease the variance caused by recall bias. Our aim was to study the magnitude and different types of burden caused by psoriasis. As healthy controls could be expected to have such burden only very rarely, no control group was included. Other types of studies need to be performed to estimate, for example, how much more or less time healthy subjects spend on performing household chores compared to patients with psoriasis.
In this study, the negative impact of psoriasis on the ability to perform household chores was associated with higher DLQI but not with higher PASI. The burden of the disease on the patient might be different even if the clinical severity of the disease is the same. Clinical disease severity and patient perception of disease severity have been shown in previous studies to be uncorrelated and patients reported that other people and even their physicians fail to assess accurately the negative impact psoriasis has on their lives [4, 16–19]. Our study findings that DLQI better differentiated the patients with the burden of psoriasis than PASI corroborate the earlier study of Delfino et al. [6]. However, in our study, only 36 patients had DLQI and 72 patients had PASI values in their medical record. Furthermore, patient sample comprised patients who had visited the Department of Dermatology within the previous year. The exact DLQI and PASI values for the time of questionnaire could not be detected and arithmetic mean values for the entire year period were used. Thus, caution should be exercised when generalizing these findings. On the other hand, self-reported severity of psoriasis has been shown to correlate with quality of life and how well patients manage to live with their disease [7, 13].
In this study, patients listed in their own words the household chores that had been specially affected by psoriasis and those for which they received assistance; prompt lists devised by professionals were not used. Such lists could have included household chores that were unimportant to the patients that may have been selected if relevant chores were not provided in the list. There would also have been a possibility that some chores of importance to the patients could have been omitted. This would make quantification of the impact more difficult and decrease the reliability of the assessment. Our method of open-ended listing probably produced lists of household chores that more accurately reflected the household chores most relevant to the everyday lives of patients with psoriasis.
The burden of psoriasis affects not only the patient but also the patient’s relatives and other helpers. In a study by Eghlileb et al. [12], 70% of the relatives and partners of patients with psoriasis stated that the treatment resulted in them having to do extra housework (including extra laundry and washing) because of the messy, greasy treatment and extra vacuuming (including cleaning skin flakes off furniture). In their study, the authors reported that relatives and partners of patients with psoriasis spent considerable time helping to apply topical treatment. These findings should not be directly compared, as Eghlileb et al. focused on the duration of time that relatives and partners spent. In this study, cleaning and laundry were also solicited separately. Prior to the study, it was assumed that these household chores were particularly affected by psoriasis. The chores listed by the patients confirmed this assumption and corroborated the earlier finding [12].
We have reported earlier that patients with a chronic disease (such as low back pain) may receive considerable assistance with household chores [20]. This was seen also among patients with psoriasis. Our findings confirm previous findings that large number of patients received assistance with household chores from relatives or other helpers. Nevertheless, in our study, the assistance received was not considered sufficient by a fifth of the patients and the duration of additional assistance needed was considerable. Men could be expected to receive more assistance in household chores from wives and partners, which might explain why women felt more need for additional assistance than men. There is obviously a hidden need for more assistance with household chores, which indicates that our estimates of the burden created by the disease are underestimates. In this study, patients with psoriasis mentioned receiving assistance with skin care, cleaning and laundry. These chores were also mentioned in the study by Eghlileb et al. [12]. In that study, 55% of the relatives and partners described social disruption, e.g., time required for care duties resulted in less time for social activities such as visiting friends, and 37% described limitations in their daily activities such as shopping. The findings of Eghlileb et al. [12] and our results suggest that when patients with psoriasis receive adequate treatment the beneficiaries are also relatives and other helpers, not only the patient.
In previous studies, the estimated time patients used for skin care/topical treatment ranged from 4 min [21] to 57.5 min per day [22]. Our finding of approximately 2 h of skin care per week, on average, is somewhere in the middle of the range. However, it is worth noting that our sample showed considerable variation in time spent on skin care. In any study, patient selection may strongly affect the time patients report spending on skin care. A sample of patients with slightly worse skin condition may report much more time on skin care than a sample of patients with less severe disease. In a study by Krueger et al. [5], patients with severe psoriasis spent approximately 3 h per week on topical therapy. However, in our study, the patients had relatively low psoriasis severity and that is a probable reason for the lower estimated time spent on skin care in our study compared with findings by Krueger et al. [5].
The present study sample comprised patients with relatively well-managed psoriasis, which may be one reason why the effect of age remained non-significant in all analyses. A previous study among hospitalized patients in Italy showed significant impairment among the older patients in all Skindex-29 scales and more psychological distress than in younger patients [19]. According to the study by Krueger et al. [5], older patients experienced more difficulties with different activities of daily living due to psoriasis than younger patients. Lack of such relationship in our study may be due to differences in sampling and determination of disease status.
Conclusion
When estimating the overall burden of psoriasis, considering only economic and productivity consequences may underestimate the impact of the disease. The impact on everyday life events like the ability to perform household chores should also be taken into account.
References
Nickoloff BJ, Nestle FO. Recent insights into the immunopathogenesis of psoriasis provide new therapeutic opportunities. J Clin Invest. 2004;113:1664–75.
Fowler JF, Duh MS, Rovba L, et al. The impact of psoriasis on health care costs and patient work loss. J Am Acad Dermatol. 2008;59:772–80.
Raho G, Koleva DM, Garattini L, Naldi L. The burden of moderate to severe psoriasis: an overview. Pharmacoeconomics. 2012;30:1005–13.
Bhosle MJ, Kulkarni A, Feldman SR, Balkrishnan R. Quality of life in patients with psoriasis. Health Qual Life Outcomes. 2006;4:35.
Krueger G, Koo J, Lebwohl M, Menter A, Stern RS, Rolstad T. The impact of psoriasis on quality of life: results of a 1998 National Psoriasis Foundation patient-membership survey. Arch Dermatol. 2001;137:280–4.
Delfino M Jr, Holt EW, Taylor CR, Wittenberg E, Qureshi AA. Willingness-to-pay stated preferences for 8 health-related quality-of-life domains in psoriasis: a pilot study. J Am Acad Dermatol. 2008;59:439–47.
Rapp SR, Feldman SR, Exum ML, Fleischer AB Jr, Reboussin DM. Psoriasis causes as much disability as other major medical diseases. J Am Acad Dermatol. 1999;41:401–7.
Finlay AY, Coles EC. The effect of severe psoriasis on the quality of life of 369 patients. Br J Dermatol. 1995;132:236–44.
Sampogna F, Tabolli S, Abeni D, IDI Multipurpose Psoriasis Research on Vital Experiences (IMPROVE) investigators. Living with psoriasis: prevalence of shame, anger, worry, and problems in daily activities and social life. Acta Derm Venereol. 2012;92:299–303.
Leino M, Mustonen A, Mattila K, Koulu L, Tuominen R. Perceived impact of psoriasis on leisure-time activities. Eur J Dermatol. 2014;24:224–8.
Manjula VD, Sreekiran S, Surendran Saril P, Sreekanth MP. A study of psoriasis and quality of life in a tertiary care teaching hospital of Kottayam, Kerala. Indian J Dermatol. 2011;56:403–6.
Eghlileb AM, Davies EE, Finlay AY. Psoriasis has a major secondary impact on the lives of family members and partners. Br J Dermatol. 2007;156:1245–50.
Dubertret L, Mrowietz U, Ranki A, et al. European patient perspectives on the impact of psoriasis: the EUROPSO patient membership survey. Br J Dermatol. 2006;155:729–36.
Al-Mazeedi K, El-Shazly M, Al-Ajmi HS. Impact of psoriasis on quality of life in Kuwait. Int J Dermatol. 2006;45:418–24.
Tuominen R, Tuominen S, Suominen C, Möttönen T, Azbel M, Hemmilä J. Perceived functional disabilities among rheumatoid arthritis patients. Rheumatol Int. 2010;30:643–9.
Chren MM, Lasek RJ, Quinn LM, Mostow EN, Zyzanski SJ. Skindex, a quality-of-life measure for patients with skin disease: reliability, validity, and responsiveness. J Invest Dermatol. 1996;107:707–13.
Choi J, Koo JY. Quality of life issues in psoriasis. J Am Acad Dermatol. 2003;49:57–61.
Fortune DG, Richards HL, Main CJ, Griffiths CE. What patients with psoriasis believe about their condition. J Am Acad Dermatol. 1998;39:196–201.
Sampogna F, Chren MM, Melchi CF, Italian Multipurpose Psoriasis Research on Vital Experiences (Improve) Study Group, et al. Age, gender, quality of life and psychological distress in patients hospitalized with psoriasis. Br J Dermatol. 2006;154:325–31.
Mattila K, Leino M, Kemppi C, Tuominen R. Perceived disadvantages caused by low back pain. J Rehabil Med. 2011;43:684–8.
Meyer N, Paul C, Feneron D, et al. Psoriasis: an epidemiological evaluation of disease burden in 590 patients. J Eur Acad Dermatol Venereol. 2010;24:1075–82.
Sohn S, Schoeffski O, Prinz J, et al. Cost of moderate to severe plaque psoriasis in Germany: a multicenter cost-of-illness study. Dermatology. 2006;212:137–44.
Acknowledgments
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published. This study was supported by unconditional grants from the research funds of the Hospital District of Southwest Finland.
Conflict of interest
M. Leino, A. Mustonen, K. Mattila, L. Koulu and R. Tuominen declare that they have no conflict of interest.
Compliance with ethics guidelines
The ethical committee of the Hospital District of Southwest Finland approved the study. The patients received a written description of the sampling procedure and study purpose, as well as the planned storage and use of the questionnaires. This was followed by a description of the subject’s rights according to the Helsinki Declaration. Participation was voluntary. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964, as revised in 2013. Informed consent was obtained from all patients for being included in the study.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Leino, M., Mustonen, A., Mattila, K. et al. Influence of Psoriasis on Household Chores and Time Spent on Skin Care at Home: A Questionnaire Study. Dermatol Ther (Heidelb) 5, 107–116 (2015). https://doi.org/10.1007/s13555-015-0076-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-015-0076-3