
Abstract
Background
Patients with diabetes mellitus experience physical health needs, but also psychological health needs, as some studies have suggested that addressing the psychological variables associated with diabetes mellitus may improve the biochemical parameters of the disease.
Objectives
To assess the quality of life (QoL) and therapeutic adherence (TA) in Mexican patients with controlled and uncontrolled type 2 diabetes mellitus (T2DM), as well as related QoL sociodemographic and clinical variables.
Methods
201 people with T2DM answered a battery of psychological tests to assess TA (Therapeutic Adherence Survey or TAS-15), QoL (WHOQOL-BREF-16) and disease-related quality of life (DRQoL-27), aside from an expressly designed questionnaire that gathered sociodemographic data and took information from medical records into consideration. The average age of the participants was 65.12 ± 11.617 years and 57.2% were female, who have suffered from diabetes for 13.4 years on average ± 8.088 and an average 158.84 mg/dL ± 61.913 fasting plasma glucose.
Results
The correlation analyses revealed that a higher perception of QoL, the lower the perception that having diabetes affected QoL (p<0.01); the higher the TA, the lower the QoL (p<0.01); and the higher the TA, the lower the perception that having diabetes affected QoL (p<0.01). The participants with an uncontrolled T2DM exhibited a better QoL than those that manage their glucose levels (p = 0.015). The participants’ level of education had a positive effect on QoL (β = 0.163, IC 95%: 0.429─3.415, p = 0.012), whereas the DRQoL had a negative effect (β = -0.546, IC 95%: -0.127─-0.080, p = 0.001).
Conclusions
If the TA of patients with T2DM increases, the overall QoL as well as the DRQoL will improve. Hence, these variables must be considered as therapeutic targets in clinical practice.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Diabetes Mellitus (DM) is one of the major public health issues worldwide. In 2019 around 463 million people suffered from this disease [1]. Almost 80% of the people that suffer from Type 2 Diabetes Mellitus (T2DM) live in countries with a low-middle income and, most of them live in Latin America [2, 3]. Mexico is listed as the second country with the highest DM prevalence in Latin America and the Caribbean, reaching 15.7% in 2020, equivalent to more than 12.8 million adults over 20 years old [4, 5].
Therapeutic Adherence (TA) is the main issue of these patients. It is characterized by a series of health behaviors that are recommendations according to health staff’s medical criteria, that improve or control clinical results and the individual’s quality of life [6]. Among the factors that contribute to an appropriate TA are: patient education, the presence of macrovascular complications, better emotional health, social and family support, acceptance of the disease, satisfaction with life, positive self-esteem, and self-efficacy [7,8,9], while those that do not contribute to TA are: the beliefs regarding therapy or treatment, the negative impact of the pharmacotherapy, poor communication between doctor-patient, emotional distress, stress, anxiety, depression, and characteristics of the disease (e.g. years of diagnosed T2DM, the severity of the disease and complications) [9, 10].
It is said that when performing TA behaviors, there is an increase in the perceived QoL despite the chronic condition of the disease [11, 12]. Other variables have a direct impact on patients’ QoL such as healthy nutrition habits [13] and glycemic control [14] which are related to a better QoL, whereas the presence of medical and psychological comorbidities (high blood pressure, stress, and/or depression) [15, 16] and complications associated with DM (neuropathies and chronic pain) have a negative impact [17].
In the Mexican population, it has been found that T2DM patients’ TA is poor [18], a little over half have a controlled capillary blood glucose (> 130 mg/dl in the morning on an empty stomach) [3, 19], less than half has a high QoL (42.3%) [20] and the greater the number of comorbidities, a lower QoL [21].
Very less is known and has been analyzed about the association between QoL and TA in T2DM patients in Mexico, as well as the sociodemographic and clinical factors that have an impact on their QoL. Another aspect is that in spite of the advances in QoL assessment, the disease-specific conditions have not been assessed –T2DM in this case, with specific instruments that differ from a scale that measures overall QoL [22, 23]. Consequently, the aim of this study was to assess the QoL and TA in Mexican patients with controlled and uncontrolled T2DM, as well as the sociodemographic and clinical variables associated with QoL.
Materials and Methods
Non-experimental, descriptive, cross-sectional study [24]. Through intentional non-probability sampling, Mexican adults with T2DM were recruited from a public health clinic located in the Gustavo A. Madero municipality in Mexico City. The inclusion criteria were as follows: to be over 18 years of age, to be a patient treated at the hospital, and to have been diagnosed with T2DM at least 6 months before this study. Patients with type 1 diabetes mellitus and diagnosed with any kind of psychological or psychiatric disorder reported in their medical record were excluded. Likewise, those that answered less than 90% of the assessment tests were eliminated.
Instruments
Sociodemographic and clinical data form: Specially prepared questionnaire by the authors comprised of eight questions to collect information on gender, age, education, marital status, occupation, comorbidities, number of years suffering from T2DM, and last pre-prandial capillary blood glucose level.
Therapeutic Adherence Scale (TAS). Psychological test created by Soria, et al [25] to assess TA behaviors in Mexican people suffering from a chronic degenerative disease (e.g. DM, high blood pressure, osteoporosis, heart diseases, arthritis, high blood cholesterol, kidney disease, atherosclerosis, or cancer). It consists of 21 questions distributed in three dimensions: 1. Medication and food intake control; 2. Medical behavioral follow-up and 3. Self-efficacy. It features five Likert-type scale answer options (0, 25, 50, 75, and 100). A confirmatory factor analysis (CFA) with the data of this sample and the scale showed an acceptable fit: χ2 (80) = 137.178, p = .000; χ2 / gl = 1.715, SRMR = .0653; RMSEA = .060, (CI = .042-.076); CFI = .870; AGFI = .880; TLI = .829. Questions 3, 4, 7, 9, 12 and 18 were eliminated since they had more than two mismatch errors and/or a high residual load; leaving 15 questions that explain 42.42% of the variance, with α = .696 (I. C. 95%: .323-.549) and Ω = .753. Hereinafter, the scale shall be referred to as TAS-15.
Diabetes 39 Quality of Life Instrument (DQoLI-39). It was adapted to the Mexican population by López-Carmona and Rodríguez-Moctezuma [26], and it assesses the disease-related quality of life (DRQoL) in T2DM patients. It is composed of 41 questions, two of which assess overall QoL and the perception of the severity of diabetes, while the other 39 are grouped in five dimensions: 1. Management control, 2. Anxiety-concern, 3. Social impact, 4. Sexual function and 5. Energy and mobility. It consists of seven Likert scale answer options (from “nothing affects me at all = 1” up to “Extremely affected = 7”). Through an AFC test with the data of this sample, the scale showed a good fit: χ2 (303) = 667.558, p = .000; χ2 / gl = 2.203, SRMR = .0279; RMSEA = .078, (CI = .070-, 086); CFI = .951; AGFI = .951; TLI = .943. Questions 1, 2, 3, 4, 7, 10, 11, 13, 15, 16, 31 and 34 were eliminated due to the fact that they had more than two association/mismatch errors and/or a high residual load; leaving 27 questions that explain 85.05% of the variance, with α = .988 (I. C. 95%: .985-.990) and Ω = .988. Therefore, the scale shall be identified as Diabetes 27 Quality of Life Instrument (D27QoLI).
A Brief version of the World Health Organization Quality of Life Questionnaire (WHOQOL-BREF): adapted to the Mexican population by González-Celis et al [27], assesses the QoL in Mexican adults. It consists of 26 questions, two of which assess the overall QoL and health satisfaction, and 24 are distributed in four dimensions: 1. Physical health, 2. Psychological health, 3. Social relationships and 4. Environment. It provides five Likert scale answer options (Not at all, A little, Moderately, Very much, and Completely). An AFC with the data of this sample was performed and a good fit was obtained: χ2 (92) = 186.737, p = .000; χ2 / gl = 2.030, SRMR = .0469; RMSEA = .072, (CI = .057- .087); CFI = .934; AGFI = .935; TLI = .914. Questions 3, 4, 5, 6, 7, 14, 15 and 17 were eliminated because some had more than two association/mismatch errors and/or a high residual load; leaving 16 questions that explain 64.07% of the variance, with α = .898 (I. C. 95%: .879-.919) and Ω = .915. Hereinafter, the scale shall be referred to as WHOQOL-BREF-16.
Procedure
The study was conducted between April and July 2021 within the facilities of the public health clinic. Beforethe application (of the questionnaire), the chief researcher trained medical interns to apply the battery of psychological tests (e.g., components to be assessed in each psychometric scale, how to interact with the participants, clarify doubts related to the questions, and how a participant that doesn’t know how to read and write can take the battery of tests). Since the protective measures to prevent the spread of COVID-19 imposed by the health institution did not allow access to staff not working at the clinic, the application was conducted in the form of an interview during participants’ medical appointments, the average application time was 20 minutes.
The parameters indicated by the Federación Mexicana de Diabetes [28] were considered to classify patients with controlled (70-130 ml/dL) and uncontrolled (>130 ml/dL) fasting plasma glucose.
Ethical considerations
The participants were able to answer the battery after having read and signed their informed consent. In this document, the aim and risk of the study were explained, as well as the participants’ rights to cooperate in an informed manner and voluntary basis in scientific research. This study was conducted under the standards for the development of research protocols established in the Code of Ethics for Psychologists [29] and was approved by the Ethics Committee of the Family Medicine Unit No. 49 of the Mexican Social Security Institute (Approval Number 2810-009-013).
Data analysis
The data obtained was entered in the SPSS® 25 statistical software for Windows®. Descriptive statistical analysis of the sample was performed using Kolmogorov-Smirnov-Lilliefors [30] normality tests finding an abnormal distribution of the study variables p> .05 and therefore, non-parametric tests were performed instead. To analyze the differences between TA, QoL, and DRQoL (total score per dimension) the U Mann-Whitney test was used, whereas to analyze the differences, between the constructs, their dimensions, the sociodemographic and medical variables, the Kruskal-Wallis test was used with a post-hoc analysis. In addition, for any significant differences the size of Rosenthal’s r effect was calculated considering the following cut-off points: small effect (.1 to < .3), moderate effect (.3 to < .5), and large effect (≥ .5) [31]; Pearson’s r coefficient was used again to assess the degree of association between the variables.
To analyze the variables that have an effect on the QoL, a multiple regression analysis was carried out, taking into account the variables that showed significant differences. To perform this analysis, multivariate assumptions were considered, starting with multivariate normality, by visual inspection of the scatter plot with the calculation of the predicted values and standardized residuals (ZPRE and ARES), and also calculating the raw residual values (RESID), eliminated residuals (DRESID), standardized residuals (ZRESID), studied residuals (SRESID) and eliminated studied residuals (SDRESID) to identify possible outliers. In addition, the leverage distance, Mahalanobis and Cook's D statistics were obtained, as well as the statistics of influence on the beta value (DfBeta) and DfAdjustment. To test the homoscedasticity assumption, a scatter plot was created with the predicted and residual values. The linearity assumption was tested by visual inspection and the independence assumption was tested using the Durbin-Watson (d) statistic, with an acceptance range between 1.5 and 2.5. Finally, the Collinearity assumption was tested by calculating the tolerance coefficients and the Variance Inflation Factor (VIF) [32]. The results are presented using standardized Betas (β) and 95% confidence intervals. A p ≤ .05 level statistical significance was determined.
Results
Descriptive analysis
The sample comprised 201 adults with T2DM (57.2% female and 42.8% male), between 28 and 87 years of age (\(\overline{{\text{x}} }\)= 65.12, SD = ± 11.617), with a 13.4 year average suffering from T2DM (SD = ± 8.088, Minimum = 1, Maximum = 35) and an average 158.84 mg/dL (DE = ± 61.913, Minimum = 89, Maximum = 380) fasting plasma glucose. Along with the T2DM diagnosis, 61.7% suffered from high blood pressure, while 24.9% from obesity; 50.7% of the participants had at least two chronic-degenerative diseases including T2DM. Table 1 shows the frequency and percentage of the participants’ sociodemographic and clinical characteristics.
Correlation analysis
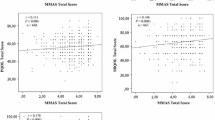
The association between the three main dependent variables was carried out (e.g. TA, QoL and DRQoL), obtaining three significant weak to moderate correlations between QoL and DRQoL (r = -0.538, p< 0.01), TA and QoL (r = 0.222, p< 0.01) and in TA and DRQoL (r = -0.218, p< 0.01).
When analyzing the association between the sociodemographic and clinical variables, three statistically significant correlations were identified: 1) age and years of T2DM diagnosis (r = .440, p< 0.01), 2) fasting plasma glucose and age (r = -0.211, p< 0.05) and 3) years suffering from T2DM and TA (r = 0.188, p< 0.01).
On the other hand, when performing the association between the dimensions of the psychometric scales WHOQOL-BREF-16, TAS-15, and QoLI-27, it was found that the three highest coefficients were obtained in the Environmental dimension of the WHOQOL-16 and the Social Impact dimension of the QoLI-27 (r = -.547, p< 0.01), Sexual Function of the QoLI-17 and Physical Health of the WHOQOL-16 (r = -.547, p< 0.01) and in the Energy-Mobility dimension of the QoLI-27 and the Environmental dimension of the WHOQOL-16 (r = -.546, p< 0.01) as can be observed in Table 2.
Comparative analysis
Marital status and occupation were the sociodemographic variables in which significant differences were found. There were significant TA differences (Z = 11.081, p = 0.026) according to the participants’ marital status, with a large size effect (r = 0.78); when conducting post-hoc analysis it was observed that single people (Me = 53) perform more TA behaviors than people living with a partner (Me = 49). As far as occupation is concerned, significant QoL differences were found (Z = 12.054, p = 0.034), with a large size effect (r = 0.85), the post hoc analysis shows that homemakers (Mdn = 44) have a better QoL than pensioners (Mdn = 40), with a large size effect (r = 1.04). Occupation also showed significant differences in DRQoL (Z = 12.445, p = 0.029), with a large size effect (r = 0.88), nevertheless, when performing a post hoc analysis, the significance was adjusted with the Bonferroni correction was not significant.
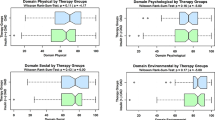
The state of T2DM (controlled or uncontrolled) showed significant differences in QoL (Z = 2.423, p = 0.015), with a small size effect (r = 0.17); patients with an uncontrolled T2DM perceived a higher QoL (Mdn = 43), as opposed to those that have a controlled T2DM (Mdn = 40). In the DRQoL the state of diabetes also showed significant differences (Z = -4.678, p = 0.000), with a moderate size effect (r = 0.33); those who have a controlled T2DM perceived a lower DRQoL (Mdn = 150), in contrast to people with an uncontrolled T2DM (Mdn = 94.5).
In Table 3 all the comparisons between the state of T2DM and the three psychometric scales and their dimensions can be observed. In the total score and the five dimensions of the QoLI-27 it was found that people with a controlled T2DM have a lower DRQoL (p< 0.05), with a moderate size effect. Whereas, in dimension three the WHOQOL-BREF-16 and of the TAS-15 significant differences were found, with a small to moderate size effect.
Multiple linear regression analysis
The tolerance coefficients and the VIF indicated an absence of collinearity between the model variables, ranging between .708 and 1.412. When analyzing the multivariate assumptions, we found that the distance (leverage, Mahalanobis, and Cook's D) and influence (DfBeta and DfAdjustment) statistics did not identify the presence of outliers, therefore, the data had multivariate normality. Homoscedasticity was found and the scatter plot showed that, although the cases were not clustered near the line of best fit, they did show a linear trend in all variables. In addition, the independence assumption was met by obtaining a d=1.812.
After multivariate assumptions were tested, all sociodemographic (gender, age, education, and marital status), clinical variables (years suffering from T2DM, number of comorbidities, and state of glucose) and the total scores obtained in the psychometric scales (QoLI-27 and TAS-15) were entered into the linear regression model using the standard method. In this regard, education was a positive effect on QoL β = 0.163 (CI 95%: 0.429─3.415, p = 0.012), whereas the score obtained on the QoLI-27 scale had a negative effect β = -0.546 (CI 95%: -0.127─-0.080, p = 0.001). This model yielded a correlation of .584 and an explained variance of 31%. The analysis of variance showed that the model was significant F (9, 191) = 10.989, p = 001, making it generalizable to the population. (Table 4). The graphical representation of the model is shown in Fig. 1.

Model of variables that have an effect on quality of life in patients with T2DM. Note: The factor that most explains the quality of life in the patients in this sample is diabetes-specific quality of life followed by level of education; 31% of the quality of life experienced by a patient is explained by the variables presented in this model
Discussion
The aim of this study was to assess the QoL and TA in Mexican patients with controlled and uncontrolled T2DM, as well as the sociodemographic and clinical variables related to patients’ QoL. As for sociodemographic variables, the sample of this study mainly comprised elderly women with an elementary education, who had suffered from T2DM for more than 13 years, with high blood pressure as their main comorbidity and uncontrolled capillary glucose (\(\overline{{\text{x}} }\) = 158.84 mg/dL), higher than the parameters reported by the International Diabetes Federation [1] and the study conducted by Gallardo-Rincón [3] (\(\overline{{\text{x}} }\) = 130 mg/dL). Correlation analyses reveal that age and the number of years living with T2DM has a relationship with glycemic control and the performance of TA behaviors, since as patients that have been diagnosed for more years take better care of themselves and adjust to the demands of their disease, which allows them to keep their blood glucose under control [5, 9]. These findings bolster the proposal of providing better multidisciplinary advice to the newly diagnosed diabetic patient, to promote a TA behavior in such patients, improving glycemic control and reducing complications [6], without neglecting those who have suffered long from the disease.
The findings of this study indicate that marital status has a large effect on TA, following reports in studies such as those of Orozco-Beltrán, et al. [7] and Świątoniowska-Lonc, et al. [9] and considering that more than 85% of the sample had a partner suggests greater social support which, in turn, favors a better TA. Regarding occupation, it has a large effect on the QoL and the DRQoL; in the first, homemakers are those that perceive a better QoL than people that receive a pension. Although not sufficient studies have been found that indicate that a sociodemographic characteristic influence on the QoL, TA, or DRQoL in these types of patients, it is possible to affirm that a better QoL is perceived by those patients that have social and/or family support for the care/management of the disease [9].
Correlation analyses indicate the following: 1) at a greater QoL perception, a lower DRQoL, 2) at a greater TA, a better QoL and 3) at a greater TA, a lower DRQoL; while the comparison analyses note that people with an uncontrolled T2DM perceive a better QoL and a lower impact on their QoL due to T2DM compared to those with controlled glucose levels. On one hand, these findings support the premise that states that the beliefs about the disease and its treatment can have an effect on the QoL and TA and also on the DRQoL in this case [7, 8, 11, 12], since people with controlled glucose levels are more affected in their DRQoL, while people with uncontrolled glucose levels have a better QoL perception. The first, by complying with the different TA behaviors for glycemic control may experience stress or anxiety [15, 16], and the latter, by performing less TA behaviors, carry out more reinforcing and unhealthy behaviors which prevent glycemic control (e.g. intake of foods and beverages high in sugar and fat) but that maintain their QoL [3]. Furthermore, in this study, it was discovered that people with uncontrolled glucose levels perceive a better QoL, a situation that differs from what is reported by Patel, et al. [14] and Aslan, et al. [17], who claim that patients from India and Turkey, respectively, have a better QoL perception when their T2DM is under control. Keeping in mind the results obtained in the correlation analyses –in which at a higher TA, a higher QoL- this study supports the premise that indicates that reinforcing the different TA behaviors will help improve not only patients’ glycemic control but their QoL [4, 11, 12] as well.
Lastly, among the factors that were found to be related to the QoL of T2DM patients, education has a positive effect. It has been noted that having a higher level of education allows patients to better understand the benefits of performing self-care behaviors, as well as to accept their state of health more easily and take better care of themselves as their disease requires and thus favoring their psychological well-being and QoL [5]. In contrast, the perception of impairment in QoL due to suffering from T2DM had a negative effect (score obtained in QoLI-27). Suffering from T2DM can be viewed by some patients as a discriminatory, excluding, limiting and even impairing condition to perform different activities, due to the fact that as more areas are perceived to be affected by T2DM, patients’ QoL will be lower [13, 20, 21].
Conclusion
More than 75% of the sample has an uncontrolled fasting plasma glucose, more than 50% suffers from another chronic disease aside from T2DM and about 50% considers that T2DM affects their QoL. There are clinical factors that threaten not only T2DM patients’ glycemic control but also their QoL and hence, future interventions must consider both aspects as therapeutic targets to be improved.
This study revealed the interaction between glycemic control, TA and QoL. This aspect leads to the need to design multidisciplinary treatments based on the state of diabetes (controlled vs uncontrolled), the level of TA, the level of QoL, the patient's age and even the years of diagnosis with the disease. For this reason, it is pertinent to continue with this proposal to evaluate its effect not only on physical health, but also on mental health.
Limitations
The limitations of this study were: 1) not having access to more information in participants’ medical records due to the COVID-19 pandemic, such as the number of medications taken, if the patient is or is not insulin-dependent, glycosylated hemoglobin and blood pressure measurement; 2) the public health-care system in Mexico lacks sufficient medical supplies to measure fasting plasma glucose per visit due to which it was not possible to measure it together with the application of the battery of psychological tests, the last parameter was taken from the medical record, despite this, it was not possible to ensure consistency of the dates on which measurement was obtained. The proposal for future studies is to implement a longitudinal assessment in which a battery of psychological tests is applied, and the medical parameters are obtained on the same date. Based on these results, we propose to identify and classify patients according to their diabetic status (controlled or uncontrolled), level of AT, level of QoL and age, in order to design a multidisciplinary treatment based on their clinical characteristics.; 3) the QoL is a psychological variable that may change due to internal or dispositional factors such as the state of mind or the existence of a significant event for the patient, such as what has happened during the COVID-19 pandemic, due to which such variables must be considered; 4) there is no consistency in the groups of controlled and uncontrolled T2DM patients and consequently it is suggested to ensure an equal number of participants in order to have equivalent comparison groups.
References
International Diabetes Federation. IDF Diabetes Atlas. Ninth edition 2019. https://www.diabetesatlas.org/upload/resources/material/20200302_133351_IDFATLAS9e-final-web.pdf
Bello-Chavolla OY, Aguilar-Salinas CA. Diabetes in Latin America. In: Dagogo-Jack S, editor. Diabetes Mellitus in Developing Countries and Underserved Communities. Switzerland: Springer; 2017;101─126. https://doi.org/10.1007/978-3-319-41559-8
Gallardo-Rincón H, Cantoral A, Arrieta A, Espinal C, Magnus MH, Palacios C, Tapia-Conyer R. Review: Type 2 diabetes in Latin America and the Caribbean: Regional and country comparison on prevalence, trends, costs and expanded prevention. Prim Care Diabetes. 2021;15:352–9. https://doi.org/10.1016/j.pcd.2020.10.001.
Avilés-Santa ML, Monroig-Rivera A, Soto-Soto A, Lindberg NM. Current State of Diabetes Mellitus Prevalence, Awareness, Treatment, and Control in Latin America: Challenges and Innovative Solutions to Improve Health Outcomes Across the Continent. Curr Diabetes Rep. 2020;20(11):1–44. https://doi.org/10.1007/s11892-020-01341-9.
Basto-Abreu A, López-Olmedo N, Rojas-Martínez R, Aguilar-Salinas CA, De la Cruz-Góngora V, Rivera-Dommarco J, et al. Prevalence of diabetes and glycemic control in Mexico: national results from 2018 and 2020. Salud Publica Mexico. 2021;63(6):1─9. https://doi.org/10.21149/12842
Lugo IV, Villegas A. Adhesión al tratamiento: un problema en las enfermedades crónicas. In: Reynoso L, Becerra L, editors. Medicina Conductual: Avances y Perspectivas. México: Qartuppi; 2021:183─208. https://doi.org/10.29410/QTP.21.11
Orozco-Beltrán D, Mata-Cases M, Artola S, Conthe P, Mediavilla J, Miranda C. Abordaje de la adherencia en diabetes mellitus tipo 2: situación actual y propuesta de posibles soluciones. Aten Prim. 2016;48(6):406–20. https://doi.org/10.1016/j.aprim.2015.09.001.
Marinho FS, Moram CBM, Rodrigues PC, Leite NC, Salles GF, Cardoso CRL. Treatment Adherence and Its Associated Factors in Patients with Type 2 Diabetes: Results from the Rio de Janeiro Type 2 Diabetes Cohort Study. J Diabetes Res. 2018;18:1–8. https://doi.org/10.1155/2018/8970196.
Świątoniowska-Lonc N, Tański W, Polański J, Jankowska-Polańska B, Mazur G. Psychosocial Determinants of Treatment Adherence in Patients with Type 2 Diabetes – A Review. Diabetes, Metabolic Syndrome Obes: Targets Therapy. 2021;14:2701–15. https://doi.org/10.2147/DMSO.S308322.
McGovern A, Tippu Z, Hinton W, Munro N, Whyte M, de Lusignan S. Comparison of medication adherence and persistence in type 2 diabetes: A systematic review and meta-analysis. Diabetes Obes Metab. 2017;20:1040–3. https://doi.org/10.1111/dom.13160.
Khayyat SM, Mohamed MM, Khayyat SMS, Alhazmi RSH, Korani MF, Allugmani EB, et al. Association between medication adherence and quality of life of patients with diabetes and hypertension attending primary care clinics: a cross-sectional survey. Qual Life Res. 2019;28(4):1053–61. https://doi.org/10.1007/s11136-018-2060-8.
Majeed A, Rehman M, Hussain I, Imran I, Saleem MU, Saeed H, et al. The Impact of Treatment Adherence on Quality of Life Among Type 2 Diabetes Mellitus Patients-Findings from a Cross-Sectional Study. Patient Prefer Adherence. 2021;15:475–81. https://doi.org/10.2147/PPA.S295012.
Pamuk G, Kaner G, Koc EM, Toṣur T, Dasdelen S, Aksun S, et al. Assessment of nutritional status and quality of life in individuals with and without diabetes over 65 years of age. Int Diabetes in Dev Ctries. 2021;41:141–7. https://doi.org/10.1007/s13410-020-00855-y.
Patel B, Oza B, Patel K, Malhotra S, Patel V. Health related quality of life in type-2 diabetic patients in Western India using World Health Organization Quality of Life–BREF and appraisal of diabetes scale. Int Diabetes in Dev Ctries. 2014;34(2):100–7. https://doi.org/10.1007/s13410-013-0162-y.
Ramos L, Morato M, Schwerz S, Grou CR, Morais TC, Silva W, et al. Lower quality of life, lower limb pain with neuropathic characteristics, female sex, and ineffective metabolic control are predictors of depressive symptoms in patients with type 2 diabetes mellitus treated in primary care. Int. Diabetes in Dev. Ctries. 2019;39(3):463─470. 0 https://doi.org/10.1007/s13410-018-0667-5
Zurita-Cruz JN, Manuel-Apolinar L, Arellano-Flores ML, Gutierrez-Gonzalez A, Najera-Ahumada AG, Cisneros-González N. Health and quality of life outcomes impairment of quality of life in type 2 diabetes mellitus: a cross-sectional study. Health Qual Life Outcomes. 2018;16(1):1–7. https://doi.org/10.1186/s12955-018-0906-y.
Aslan GY, Tekir Ö, Yildiz H. Relationship between family support and quality of life in individuals with diabetes. Cukurova Med. J. 2021;46(1):299─309. https://doi.org/10.20473/jn.v14i3.17175
Martinez-Vega IP, Doubova, SV, Pérez-Cuevas R. Distress and its association with self-care in people with type 2 diabetes. Salud Men. 2017;40(2):47─55. https://doi.org/10.17711/sm.0185-3325.2017.007
Zurita-Cruz JN, Manuel-Apolinar L, Arrellano-Flores ML, Gutierrez-Gonzalez A, Rivera-Hernandez AJ, Carranza-Muleiro RA, et al. Type 2 diabetes: epidemiological changes at Instituto Mexicano del Seguro Social—associated with complications in Mexico. Int Diabetes in Dev Ctries. 2020;40(2):178–84. https://doi.org/10.1007/s13410-019-00767-6.
Reyes-Jarquín K, Tolentino-Flores F, Guzmán-Saldaña R, Bosques-Brugada LE, Romero-Palencia A, Lerma-Talamantes A, et al. Calidad de vida en pacientes con diabetes mellitus tipo II, en Pachuca Hidalgo. Educación y Salud Boletín Científico Instituto de Ciencias de la Salud. 2019;8(15):1–6.
Salazar JG, Gutiérrez AM, Aranda C, González R, Pando M. La calidad de vida en adultos con diabetes mellitus tipo 2 en centros de salud de Guadalajara, Jalisco (México). Salud Uninorte. 2012;28(2):264–75.
Karimi M, Brazier J. Health, Health-Related Quality of Life, and Quality of Life: What is the Difference? PharmacoEconomics. 2016;34:645–9. https://doi.org/10.1007/s40273-016-0389-9.
Oluchi SE, Manaf RA, Ismail S, Shadar HK, Mahmud A, Udeani TK. Health Related Quality of Life Measurements for Diabetes: A Systematic Review. Int. J. Environ. Res. Public Health. 2021;18:9245. https://doi.org/10.3390/ijerph18179245
Hernández R, Fernández C, Baptista MP. Metodología de la investigación. 4th ed. Mexico: Mc Graw Hill; 2010.
Soria R, Vega CZ, Nava C. Escala de adherencia terapéutica para pacientes con enfermedades crónicas, basada en comportamientos explícitos. Alternativas en Psicología. 2009;14(20).
López-Carmona JM, Rodríguez-Moctezuma R. Adaptación y validación del instrumento de calidad de vida Diabetes 39 en pacientes mexicanos con diabetes mellitus tipo 2. Salud Pública de México. 2006;48:200–11.
González-Celis ALM, Tron R, Chávez M. Evaluación de la calidad de vida: A través del WHOQOL en población de adultos mayores en México. México: Facultad de Estudios Superiores Iztacala, Universidad Nacional Autónoma de México; 2009.
Federación Mexicana de Diabetes. Niveles de glucosa en sangre y automonitoreo. https://fmdiabetes.org/automonitoreo-niveles-glucosa/
Sociedad Mexicana de Psicología. Código Ético del Psicólogo. México: Trillas; 2014.
Ghasemi A, Zahediasl S. Normality tests for statistical analysis: A guide for nonstatisticians. Int J Endocrinol. 2012;10(2):486–9. https://doi.org/10.5812/ijem.3505.
Cohen J. Statistical power analisis for the behavioral sciences. USA: Lawrence Erlbaum Associates; 1988.
Miles J, Shevlin M. Applying Regression & Correlation. USA: SAGE; 2013.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Conceptualization, Research, Formal analysis, Draft-Final writing and Project management were performed by Alejandro Pérez-Ortiz. Formal analysis and Draft-Final writing were performed by Ana Leticia Becerra-Gálvez, Juan Manuel Mancilla Díaz and Isaías Vicente Lugo-González. Finally, Research and Resources were performed by Perla Irán Fernández de la Hoz and Mario Francisco Cancino-Romero. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Sponsors
The first autor was supported by a doctoral scholarship from Consejo Nacional de Humanidades, Ciencias y Tecnologías (CONAHCYT), Scholar No. 996327.
Ethical approval
Ethical approval to report this study was obtained from the Ethics Committee of the Family Medicine Unit No. 49 of the Instituto Mexicano del Seguro Social (Approval Number 2810-009-013).
Research involving human participants and/or animals
According to the Helsinki Declaration and the Code of Ethics for Psychologists, this research was evaluated and approved by Committee of the Family Medicine Unit No. 49 of the Instituto Mexicano del Seguro Social (Approval Number 2810-009-013).
Informed consent
Informed consent was obtained from the patients for their anonymized information to be published in a scientific journal.
Conflict of interest
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pérez-Ortiz, A., Becerra-Gálvez, A.L., Mancilla-Díaz, J.M. et al. Quality of life assessment and therapeutic adherence in Mexican patients with type 2 diabetes. Int J Diabetes Dev Ctries (2024). https://doi.org/10.1007/s13410-024-01331-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s13410-024-01331-7