
Abstract
Conventional X-ray is commonly used for pelvic fracture follow-ups, but has a precision of only ± 5 mm. Implantation of tantalum beads together with RSA has shown high precision but not applicable in clinical practice. CT scan has been shown a suitable substitute for RSA to follow the metal markers. We aimed to assess whether implantation of metal markers could be avoided using CT scan and merging of bone surface anatomy. A human cadaveric pelvis marked with 0.8 mm tantalum beads was fixed over the symphysis and the right SI-joint. Left hemi-pelvis was subsequently distracted using plastic spacers. Sequential CT exams was conducted and data were analyzed using Sectra® (Sectra AB), CTMA package. Examinations were repeated after 2 weeks. Bone registration showed better precision than registration based on tantalum beads. However, only the difference in angular changes was statistically significant (p = 0.008). The confidence interval of the repeatability was ± 0.5 mm for translation and ± 0.5° for rotation. This new non-invasive technique showed good precision and repeatability and might be a future option in clinical practice for post-operative follow-ups of patients with pelvic fractures.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
By tradition, conventional X-rays have been used for evaluating the post-operative outcome and for the follow-up of pelvic fractures. However, previous studies using plain radiographs have shown poor inter- and intra-observer reliability, a low level of reproducibility and a measurement error of at least ± 5 mm [3, 4, 11]. Introduction of Computed Tomography (CT) has added to better understanding of the fractures pre-operative and better description of post-operative radiological outcome [1]. As an alternative the Radiostereometric Analysis (RSA) technique has been encouraged because of its accuracy and precision for fracture follow-ups, but the technique is cumbersome to use in clinical settings and demands additional implants (tantalum beads) [3, 22].
A new promising method using CT examinations and volume registration in conjunction with mathematical routines was introduced by Olivecrona et al. [13]. This image post-processing method addresses how two rigid bodies shifts position relative to each other using volume registration. Movements are expressed at the geometrical center of the moving object and/or at any arbitrary user defined points of interest, such as an orthopedic implant or a fracture line. This technique has been shown to be accurate, precise, reliable and repeatable in several studies on hip arthroplasty models and in hip arthroplasty patients [5,6,7, 9, 13,14,15,16,17,18,19].
The aim of this study was to validate a new CT based migration method in a human pelvic fracture model bone using distraction levels below the precision limitation of X-ray (± 5 mm), and to evaluate whether implantation of tantalum beads could be avoided.
2 Materials and Methods
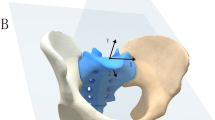
A denuded human pelvic bone that has previously been used for educational purposes at the department was used. The right SI-joint was immobilized using a 3.5 mm cortical screw (DePuy/Synthes, West Chester, USA). An anterior symphyseal plate (DePuy/Synthes, West Chester, USA) was applied over the symphysis with 3 cortical screws on each side. The screws on the left side of the symphysis were backed two revolutions to allow some gap for consequent placement of plastic spacers either in the symphysis or in the left SI-joint. The model was marked with 0.8 mm diameter tantalum beads, two on each side of the symphysis pubis (apical and caudal) and in the same manner four beads was placed anteriorly on the superior and inferior margin of the left SI-joint. The right and left sides of the pelvis were further marked with tantalum beads in each acetabulum and over the superior margin of each iliac wing (totally six beads on right side and six beads on the left side and two beads over the left side of the sacrum in agreement with Solomon et al. [22] (Fig. 1).

Human pelvis used in this study. The pelvis is fixed with Osteosynthesis in the front and over the right SI-joint. The left SI-joint is expandable. Tantalum beads are implanted over the right and left iliac wings, over both acetabulum and over the symphysis and the left SI-joint
CT examinations were acquired using a clinical CT scanner (Toshiba Aquilion ONE, Toshiba Medical Systems, Tochigi-ken, Japan). SEMAR (single-energy metal artefact reduction) was used to reduce artefact effect. Low dose CT-scanning with 137 kV and 0.5 mm thick slices was conducted.
Before each CT examination, the distance between two tantalum beads over the superior portion of the anterior symphysis pubis and two tantalum beads over superior portion of the left SI-joint were measured using Calipers (Cocraft, Clas Ohlson, Stockholm, Sweden, Article Number 40-8745) in order make sure an actual displacement was occurred. The pelvis was always examined in two different positions on the CT bed (position a and b). Between these positions the pelvis was lifted from the CT bed and reoriented to mimic different patient positioning on repeated examinations. Stability of the construct was manually tested before each pair of CT examination. The pelvic sides were displaced in relation to each other by using one, two, and three plastic spacers over the symphysis initially and then over the left SI-joint, again using one, two, and three plastic spacers. This resulted in seven pairs of CT volumes (denominated 1a–7b) where the a- and b-scans represented the same pelvic anatomy but acquired in different position in the scanner. Sectra (Linköping, Sweden) CTMA program was used for analyzing the CT data. We made the assumption that the right side of the pelvis was the stable part of the system and used this as reference during the study and analysis. The sacrum was not regarded as a part of the pelvic sides.
Two experiments comprising volume registration and measurements where performed. In experiment one the volume registration was based on the implanted tantalum markers. In experiment two the registration is based on the bone surface.
Each experiment comprised:
-
1.
Registration of right side of pelvis as stationary object (Fig. 2).
Fig. 2 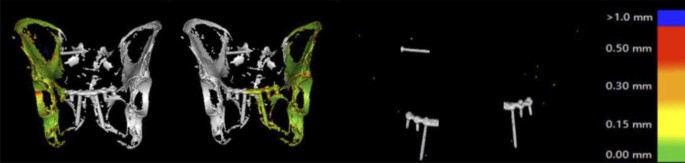
Registration of right and left side of pelvis using bone registration in the left and tantalum registration to the right
-
2.
Registration of left side of pelvis as moving object (Fig. 2).
-
3.
Designation of two points of interest for expressing the movement of the moving object; one on the left side of the symphysis and one on the iliac side of the left SI-joint.

The registration in experiment 1 used registration between mesh data extracted from the bone surfaces and experiment 2 used mesh data representing the tantalum beads (Fig. 2).
To test repeatability, procedures 1–3 were repeated after 2 weeks.
The CTMA software automatically calculates the shift of position of the moving object relative to the stationary across the two CT volumes. This generates a rotation matrix and a translation matrix. The rotation of a moving rigid object is universal, but the translation varies depending on where in the object this is measured. This can be visualized by rotating the earth around the north–south axis. The rotation is the same for the entire globe but the translation on the surface varies and decreases the farther north or south from the equator it is measured. Therefore, migration must be expressed at specified points (Fig. 3). Numerical data was expressed and saved in a spreadsheet format in six degrees of freedom (rotations and translations around orthogonal coordinate axes) using Euler decompositions with Tait–Bryant angles with the order of rotation x–y–z in original CT grid coordinates or relative to an arbitrary chosen multi-planar reconstruction coordinate system. Total angle in space of rotation of the moving object along with length of translation vector at any specified point were also expressed.

Automated report on translation over the symphysis, SI-joint and angular change of the left side of the pelvis
Precision was defined as “the closeness of agreement between independent test results obtained under same conditions” [20]. To calculate precision, the dual CT-examinations at each displacement level were compared, as, per definition, no movement should occur. Repeatability was defined as “precision under repeatability conditions” [20].
3 Ethics
A question was raised to the Stockholm´s local ethical committee regarding using this human pelvis and answer was received that as this specimen was not traceable to an existing physical body, there were no ethical concerns.
4 Statistics
Paired Student T test was used for comparison analysis of scale variables with normal distribution. Normality of datasets was tested based on plotting the data and Shapiro–Wilks test. Precision was measured in mean, median and 95% CI of the mean as recommended by the ASTM standard E177-90a [2]. SPSS (IBM SPSS Statistics for Windows, Version 25.0. Armonk, USA) program was used for statistical calculations.
5 Results
5.1 Precision
Results of the precision calculation comparing bone registration versus registration based on tantalum beads are presented in Table 1a, b. In all measurements bone registration showed better precision, however only measurements of angular deformity were significantly different (mean difference − 0.12, CI − 0.2 to − 0.05, p = 0.008).
5.2 Measurements in Distraction
Translational measurements and angular measurements of the left side of the pelvis following distraction using bone registration versus registration based on tantalum are presented in Table 2a, b. Calipers measurements showed translation of symphysis ranging 0–4 mm (mean 1.4 mm, median 0.9 mm, CI 0.9–1.9 mm). Calipers measurements showed translation of the left SI-joint ranging from 0 to 5 mm (mean 2.6 mm, median 3 mm, CI 1.8–3.4 mm). There were no statistically significant differences between bone registration and tantalum registration to report angular changes or translation at the symphysis or at the SI-joint. Overall confidence interval of mean difference to report translation during distraction was ± 0.2 mm, and for angular changes ± 0.2° (Table 2a, b).
5.3 Repeatability
Comparison of repeated measurements showed only significant difference between the first and second measurements regarding precision in Z-axis of translation at the symphysis pubis with bone registration with a mean difference of − 0.06 mm (CI − 0.1 to − 0.16, p = 0.016). The overall 95% CI of repeatability between first and second run were ± 0.2 mm while these were not statistically significant.
Measurements in distraction between first and second run showed significant differences between absolute values of translation over the SI-joint using bone registration with a mean difference of 0.08 mm (CI 0.02–0.15, p = 0.01), translation in the Z-axis over the SI-joint using tantalum registration with a mean difference of − 0.17 mm (CI − 0.28 to − 0.06, p = 0.004) and translation in the Z-axis over the SI-joint using bone registration with a mean difference of − 0.14 mm (CI − 0.26 to − 0.02, p = 0.03). The overall CI of repeatability for reporting distance changes during distraction for remaining measurements (according to Table 2) were ± 0.5 mm but these were not statistically significant. In all measurements 95% CI of repeatability for reporting rotational changes between the first run and the second run was ± 0.5 degree while these differences were not statistically significant.
6 Discussion
The main finding of our study was that CT examination using bone registration was more precise than registration with tantalum beads. Both techniques were repeatable. Implantation of tantalum beads while using CT examination with motion analysis seems unnecessary.
Orthopedic surgeons traditionally use plain X-rays to report their post-operative results and to monitor healing over time. However, this technique has a reported measurement error of at least ± 5 mm [3, 4, 11]. Still, the most common radiographic outcome measurement technique following pelvic fracture surgery according to the literature is the method presented by Matta and Tornetta using conventional X-rays including pelvic antero-posterior (AP), inlet and outlet views. In this method the distance in the SI-joint and the symphysis is reported. The maximum reported distance in any plane is graded as excellent if it is under 4 mm, as good if the distance is under 10 mm, as fair if the distance is between 10 and 20 mm and if any measurement is over 20 mm the result is considered as poor [10]. However, Matta and Tornetta´s technique has been criticized because of lack of reproducibility as finding anatomical landmarks between two observers or two separate examinations has been shown difficult [8]. We applied a modified Matta and Tornetta technique as we used distance changes at the symphysis pubis and at the SI-Joint when comparing a point to its previous position. Our results showed that appropriate imaging modality together with appropriate automated interpretations technique minimizes the level of uncertainty and might contribute to better precision and accuracy with a method that can be used in a clinical setting. The distance changes for each point is automatically reportable with respect to its previous position in a 3D manner and not with respect to the contralateral side. Automatic merging of 3D CT generated volumes, with a precision of ± 0.2 mm for translation and ± 0.2° for rotation reduces the risk of observer induced measurement bias. Further, reporting angular deformity of unstable parts of the pelvis, which has been difficult previously, is possible with this technique [12]. Other measurement techniques with higher precision, such as RSA, have been proposed as an alternative to plain X-rays. RSA technique has been used in fracture research. Solomon et al. studied tibia plateau fractures using RSA technique and found that implantation of 6 tantalum beads in each fragment section was sufficient. The authors showed promising results to report deformity over time with a reported precision of ± 0.05 mm for translation and ± 0.2° of rotation [22]. The authors concluded that RSA technique, because of its precision and accuracy justifies implantation of tantalum beads in fracture surgery research [22]. The technique is however invasive and cumbersome and demands implantation of tantalum beads around the fracture and is not feasible to conduct in daily practice [3].
Olivecrona et al. have previously studied CTMA extensively as explained before. The authors were able to show that using CT-examination and fusion of the volumes on hip replacements, tantalum beads were as traceable as RSA and the technique was not inferior to RSA [13].
Bone registration showed superior results compared to registration with metal markers. This might reflect the fact that using entire meshed surface of the bone is superior to use outspread points (metal markers), as the numbers of metal markers are limited.
Concerns about increased radiation doses for CT scans compared to conventional X-rays have been raised. However, low-dose CT scan using volume fusion technique has been shown possible with radiation dosage as low as 0.7 mSv, which is comparable to conventional X-rays [21].
The major strength of our study was its novelty when introducing a new technique that might be feasible for clinicians to use in daily practice when reporting their outcome over time. A non-invasive method with a precision better than 1 mm for translation and one degree for rotation would improve the ability to monitor and better understand how to manage these often complex fractures. We had several limitations in our study. One obvious limitation was its model character. The human pelvic model we used was without soft tissue, spinal column and femurs. We used only six metal markers over each side of the pelvis, as proposed by Solomon et al. [22], the question remains whether implantation of more tantalum beads could improve precision of volume registration using tantalum beads. Radiation dosage using CT scan is another issue implementing this technique in daily practice. However, implementing protocols for low dose CT scan in collaboration with radiology department and application of SEMAR would be practical options.
7 Conclusion
This new non-invasive technique showed good precision and repeatability and might be a future option in clinical practice for post-operative follow-ups of patients with pelvic fractures. Future clinical in vivo studies are encouraged to further study its practical application and advantages in comparison to conventional X-rays. Implantation of tantalum beads while using 3D CT with merging of the volumes seems unnecessary.
References
Abdelfattah, A. A., & Moed, B. R. (2016). CT-generated radiographs in patients with pelvic ring injury: Can they be used in lieu of plain radiographs? Journal of Orthopaedic Surgery and Research, 11, 26. https://doi.org/10.1186/s13018-016-0361-6.
ASTM. (2018). ASTM. Accessed 4 September 2018.
Augat, P., Faschingbauer, M., Seide, K., Tobita, K., Callary, S. A., Solomon, L. B., et al. (2014). Biomechanical methods for the assessment of fracture repair. Injury, 45(Suppl 2), S32–S38. https://doi.org/10.1016/j.injury.2014.04.006.
Borrelli, J., Jr., Goldfarb, C., Catalano, L., & Evanoff, B. A. (2002). Assessment of articular fragment displacement in acetabular fractures: a comparison of computerized tomography and plain radiographs. Journal of Orthopaedic Trauma, 16, 449–456. (discussion 456–447).
Broden, C., Olivecrona, H., Maguire, G. Q., Jr., Noz, M. E., Zeleznik, M. P., & Skoldenberg, O. (2016). Accuracy and precision of three-dimensional low dose CT compared to standard RSA in acetabular cups: An experimental study. BioMed Research International, 2016, 5909741. https://doi.org/10.1155/2016/5909741.
Goldvasser, D., et al. (2014). In vivo and ex vivo measurement of polyethylene wear in total hip arthroplasty: Comparison of measurements using a CT algorithm, a coordinate-measuring machine, and a micrometer. Acta Orthopaedica, 85, 271–275. https://doi.org/10.3109/17453674.2014.913225.
Jedenmalm, A., et al. (2011). Validation of a 3D CT method for measurement of linear wear of acetabular cups. Acta Orthopaedica, 82, 35–41. https://doi.org/10.3109/17453674.2011.552777.
Lefaivre, K. A., Slobogean, G., Starr, A. J., Guy, P., O’Brien, P. J., & Macadam, S. A. (2012). Methodology and interpretation of radiographic outcomes in surgically treated pelvic fractures: a systematic review. Journal of Orthopaedic Trauma, 26, 474–481. https://doi.org/10.1097/BOT.0b013e3182323aa2.
Maguire, G. Q., Jr., Noz, M. E., Olivecrona, H., Zeleznik, M. P., & Weidenhielm, L. (2014). A new automated way to measure polyethylene wear in THA using a high resolution CT scanner: Method and analysis. The Scientific World Journal, 2014, 528407. https://doi.org/10.1155/2014/528407.
Matta, J. M., & Tornetta, P., 3rd. (1996). Internal fixation of unstable pelvic ring injuries. Clinical Orthopaedics and Related Research, 329, 129–140.
Nystrom, L. M., McKinley, T. O., & Marsh, J. L. (2013). Accuracy in radiographic assessment of pelvic ring fracture deformity: Analysis of current methods. Journal of Orthopaedic Trauma, 27, 708–715. https://doi.org/10.1097/BOT.0b013e318298e6cf.
Nystrom, L. M., McKinley, T. O., & Marsh, J. L. (2015). Radiographic measurement of rotational deformity in pelvic fractures: A novel method with validity and reliability testing. Journal of Orthopaedic Trauma, 29, 365–369. https://doi.org/10.1097/BOT.0000000000000306.
Olivecrona, H., Maguire, G. Q., Jr., Noz, M. E., Zeleznik, M. P., Kesteris, U., & Weidenhielm, L. (2016). A CT method for following patients with both prosthetic replacement and implanted tantalum beads: preliminary analysis with a pelvic model and in seven patients. Journal of Orthopaedic Surgery and Research, 11, 27. https://doi.org/10.1186/s13018-016-0360-7.
Olivecrona, H., et al. (2003). Stability of acetabular axis after total hip arthroplasty, repeatability using CT and a semiautomated program for volume fusion. Acta Radiologica, 44, 653–661.
Olivecrona, H., et al. (2004). A new CT method for measuring cup orientation after total hip arthroplasty: A study of 10 patients. Acta Orthopaedica Scandinavica, 75, 252–260. https://doi.org/10.1080/00016470410001169.
Olivecrona, H., et al. (2003). Spatial component position in total hip arthroplasty. Accuracy and repeatability with a new CT method. Acta Radiologica, 44, 84–91.
Olivecrona, L., et al. (2002). Acetabular component migration in total hip arthroplasty using CT and a semiautomated program for volume merging. Acta Radiologica, 43, 517–527.
Olivecrona, L., Olivecrona, H., Weidenhielm, L., Noz, M. E., Maguire, G. Q., Jr., & Zeleznik, M. P. (2003). Model studies on acetabular component migration in total hip arthroplasty using CT and a semiautomated program for volume merging. Acta Radiologica, 44, 419–429.
Otten, V., Maguire, G. Q., Jr., Noz, M. E., Zeleznik, M. P., Nilsson, K. G., & Olivecrona, H. (2017). Are CT scans a satisfactory substitute for the follow-up of RSA migration studies of uncemented cups? A comparison of RSA double examinations and CT datasets of 46 total hip arthroplasties. BioMed Research International, 2017, 3681458. https://doi.org/10.1155/2017/3681458.
Ranstam, J., Ryd, L., & Onsten, I. (2000). Accurate accuracy assessment: Review of basic principles. Acta Orthopaedica Scandinavica, 71, 106–108.
Sandgren, B., Skorpil, M., Nowik, P., Olivecrona, H., Crafoord, J., Weidenhielm, L., et al. (2016). Assessment of wear and periacetabular osteolysis using dual energy computed tomography on a pig cadaver to identify the lowest acceptable radiation dose. Bone & Joint Research, 5, 307–313. https://doi.org/10.1302/2046-3758.57.2000566.
Solomon, L. B., Stevenson, A. W., Callary, S. A., Sullivan, T. R., Howie, D. W., & Chehade, M. J. (2010). The accuracy and precision of radiostereometric analysis in monitoring tibial plateau fractures. Acta Orthopaedica, 81, 487–494. https://doi.org/10.3109/17453674.2010.487930.
Author information
Authors and Affiliations
Contributions
LW and AE designed the study and contributed to manuscript writing. HE has long experience of volume registration using CT-scan and contributed to examination, calculations and manuscript writing. PB has participated in design of the study and writing the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflict of interest. PE and HO have consultant duties with Sectra®.
Data availability
All data would be available on request.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Bakhshayesh, P., Olivecrona, H., Weidenhielm, L. et al. A New CT Based Method for Post-operative Motion Analysis of Pelvic Fractures. 3D Res 10, 7 (2019). https://doi.org/10.1007/s13319-019-0217-z
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s13319-019-0217-z