
Abstract
Background and Objectives
Rebaudioside A, a steviol glycoside, is deglycosylated by intestinal microflora prior to the absorption of steviol and conjugation to steviol glucuronide. While glucose-lowering properties are observed for rebaudioside A in mice, they have been attributed to the metabolites steviol and steviol glucuronide. We aimed to characterize the pharmacokinetic and pharmacodynamic properties of rebaudioside A and its metabolites in patients with early-onset type 2 diabetes mellitus (T2DM).
Methods
This randomized, placebo-controlled, open-label, two-way crossover trial was performed in subjects with T2DM on metformin or no therapy at the University Hospitals Leuven, Belgium. Following oral rebaudioside A (3 g), plasma concentrations of rebaudioside A, steviol and steviol glucuronide were determined. The effect on glucose homeostasis was examined by an oral glucose tolerance test (OGTT) performed 19 h following rebaudioside A administration, i.e. the presumed time of maximal steviol and steviol glucuronide concentrations. The primary pharmacodynamic endpoint was the difference in area under the blood glucose concentration–time curve during the first 2 h of the OGTT (AUCGlucose(0–2h)) for rebaudioside A vs. placebo.
Results
In total, 30 subjects [63.5 (57.8–69.0) years of age, 86.7% male] completed the trial. Rebaudioside A was detected as early as 1 h after administration in nearly all subjects. As expected, steviol and steviol glucuronide reached their maximal concentrations at 19.5 h following rebaudioside A administration. Rebaudioside A did not lower the AUCGlucose(0–2h) compared to placebo (− 0.7 (95% CI − 22.3; 20.9) h·mg/dL, P = 0.95). Insulin and C-peptide concentrations were also comparable between both conditions (P > 0.05).
Conclusion
Rebaudioside A is readily absorbed after oral administration and metabolized to steviol and steviol glucuronide. However, no effect on glucose nor insulin or C-peptide excursion was observed during the OGTT at the time of maximal metabolite concentrations. Thus, no antidiabetic properties of rebaudioside A could be observed in patients with T2DM after single oral use.
Clinical Trial Registration
Registered on ClinicalTrials.gov (NCT03510624).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Rebaudioside A is absorbed in the blood circulation without prior deglycosylation to steviol. |
Rebaudioside A does not lower blood glucose at the time when its metabolites, steviol and steviol glucuronide, are maximally present. |
1 Introduction
Rebaudioside A is one of the major diterpenoid steviol glycosides isolated from Stevia rebaudiana Bertoni [1]. Given its naturally high sweetness potency, it is approved for use as a low-caloric sweetener in food and beverages throughout the world [2, 3]. Moreover, animal research suggests that steviol glycosides and its metabolites possess glucose-lowering properties, making it an interesting candidate for the treatment of diabetes [4,5,6,7,8,9].
The metabolic fate of rebaudioside A has been considered equal to stevioside, another steviol glycoside [10]. Following oral intake, rebaudioside A is resistant to degradation by the digestive enzymes and gastric acid of the upper gastrointestinal tract [11, 12] (Fig. 1a). In the colon, rebaudioside A encounters the intestinal microflora, which remove the glycosyl moieties, resulting in steviol [13, 14] (Fig. 1b). Steviol is subsequently absorbed and conjugated in the liver to steviol glucuronide, which is excreted via the urine [15, 16] (Fig. 1c). Very little is known about the plasma concentrations of steviol glycosides, steviol and steviol glucuronide following rebaudioside A or stevioside ingestion. The absorption of the parent steviol glycosides in vitro and in vivo is presumably very low [12, 17]. Steviol, on the other hand, has higher absorptive transport characteristics, but plasma concentrations in humans remain very low after oral intake [12, 16,17,18]. In contrast, steviol glucuronide is the primary circulating compound when rebaudioside A or stevioside is consumed [12, 18, 19].

Chemical structures of (a) rebaudioside A, (b) steviol and (c) steviol glucuronide
Type 2 diabetes mellitus (T2DM) is characterized by chronic hyperglycemia, which can lead to micro- and macrovascular complications [20]. Diabetes therapy is focused on glycemic management [21]. Rebaudioside A is a natural high-intensity sweetener and thus interesting as a replacement for sugar in this patient population. In addition, rebaudioside A and stevioside enhance the glucose-induced insulin secretion by potentiation of the transient receptor potential melastatin 5 (TRPM5) ion channel in the pancreatic β-cells and reduce glycemia in mouse and rat diabetes models [4,5,6,7,8,9]. Although the glycemic effects of steviol glycosides and its underlying mechanism seem promising in animals, clinical trials do not unveil unambiguous evidence for a direct insulinotropic and anti-hyperglycemic effect in T2DM. Only one acute trial has demonstrated a reduced postprandial glucose following a test meal with 1 g of stevioside [22]. Moreover, trials with chronic exposure to steviol glycosides showed no glucose-lowering effects [23, 24]. A meta-analysis concluded that steviol glycosides caused non-significant reductions of fasting blood glucose and glycated hemoglobin A1c (HbA1c) in individuals with T2DM when compared to placebo [25]. However, significant heterogeneity was found for some analyses, and previous clinical trials have had methodological limitations, making it challenging to draw a firm conclusion. First, there has been substantial diversity in trial design, administered dose, duration of intervention and (dis)continuation of antidiabetic medication. Second, if the anti-hyperglycemic effect is established to be β-cell dependent, attention should be given to those individuals with well-preserved β-cell function. Third, there is evidence that steviol and steviol glucuronide, which are absorbed and could reach the pancreatic β-cells, pose insulinotropic effects on their own [7, 9, 26, 27]. Moreover, the literature suggests that steviol glucuronide is the active metabolite responsible for the effect of steviol glycosides [27]. Consequently, the glycemic outcome should be measured at an adequate time after oral ingestion, i.e. when steviol and steviol glucuronide are most present.
In this study, we aim to determine the circulating plasma concentrations of rebaudioside A, steviol and steviol glucuronide. Moreover, we set out to investigate the effect of rebaudioside A on glucose homeostasis in humans with T2DM at the presumed maximal plasma concentrations of steviol and steviol glucuronide.
2 Methods
2.1 Study Design
This was a phase I, randomized, placebo-controlled, open-label, two-way crossover study performed at the University Hospitals Leuven, Belgium, investigating the pharmacokinetics and effects on glucose homeostasis of a single dose of rebaudioside A in subjects with T2DM (N = 30). The study was reviewed by the Ethics Committee Research UZ/KU Leuven and the Federal Agency for Medicines and Health Products (EudraCT 2017-004428-31). The study was registered on ClinicalTrials.gov (NCT03510624) and conducted according to the principles of the Declaration of Helsinki.
2.2 Subjects
To be eligible, men and women (35–75 years) were required to be diagnosed with T2DM (≥ 3 months), receive metformin monotherapy or no drug therapy, and have a HbA1c of 6.5–8% and a body mass index (BMI) of 25–40 kg/m2. All eligibility criteria are summarized in Table S1 of the Supplementary Information. Subjects were recruited from the unit of Endocrinology of the University Hospitals Leuven, general practices in Flanders and advertisement via Diabetes Liga, flyers and social media.
2.3 Study Product
Rebaudioside A (≥ 97.0% purity, Stevial® Pharma RebA Pur, Stevia Natura, France) powder was encapsuled in hard gelatin capsules (500 mg per capsule) by the Center of Clinical Pharmacology, Leuven, Belgium. Placebo pills consisted of empty hard gelatin capsules.
2.4 Study Procedures and Assessments
The overall study design is presented in Fig. 2a. For the screening visit, subjects were asked to present after an overnight fast. The subject’s general health status was assessed by medical history review, medication use, physical examination (height, weight, waist circumference, body composition, 12-lead electrocardiogram), vital signs (blood pressure, heart rate, temperature, respiration rate) and fasting blood samples. Use of nicotine-containing products was determined with a cotinine test. Inclusion and exclusion criteria were checked. Eligible subjects were randomized for treatment sequence with an allocation of 1:1 using a randomization list and were invited for two treatment periods (first period ≤ 6 weeks after screening). Each period consisted of 2 consecutive days. Subjects received rebaudioside A or placebo on day 1 and underwent an OGTT on day 2. The treatment periods were separated by 7–14 days, equating to ≥ 5 × the longest half-life found for steviol and steviol glucuronide following rebaudioside A or stevioside intake in humans, to allow effective systemic elimination before initiation of the subsequent treatment [18, 19]. Subjects were instructed to follow restrictions, including those on confounders of glucose homeostasis (metformin intake, changes in habitual diet, strenuous physical activities), TRPM5 ion channel activity (nicotine, steviol glycosides, quinine) and pharmacokinetics or analysis (grape fruit, alcohol, caffeine, ibuprofen) (Fig. 2a). Compliance to all restrictions was checked by questioning and reviewing a 5-day food diary.

Schematic representation of the AREBAG trial. (a) Study design and restrictions. (b) Day 1 of each period for both rebaudioside A (top panel) and placebo (bottom panel). (c) Day 2 of each period for both rebaudioside A (top panel) and placebo (bottom panel). OGTT oral glucose tolerance test, RebA rebaudioside A
On day 1 of each period (Fig. 2b), subjects were asked to present fasted for 5 h. Concomitant medication was reviewed and vital signs (blood pressure, heart rate, temperature, blood glucose) were measured. Subjects received either six capsules of 500 mg rebaudioside A (total dose 3 g) or six empty capsules, to be taken orally with 240 mL tap water. In the case of rebaudioside A administration, blood samples were collected 1 and 2 h after administration. Water consumption was allowed ad libitum 1 h after drug administration, and a standardized lunch meal was provided 2 h after administration.
On day 2 of each period (Fig. 2c), subjects were asked to present fasted for 10 h. Concomitant medication was reviewed and vital signs (blood pressure, heart rate, temperature, blood glucose) were measured. An intravenous catheter was placed in the subject’s arm. At 19 h after drug administration, subjects were instructed to drink a 75 g glucose beverage (Glucomedics®, Lambra, Spain) within 5 min. Based on a previous trial, the time point of 19 h is when the maximal plasma concentrations of steviol are reached [19], and this was confirmed by our pharmacokinetic results. Blood samples were collected before and after the glucose challenge at specified time points. During the entire visit, subjects were kept in-house, asked to rest in terms of sitting or lying down, and were not allowed to eat or drink. A standardized meal was provided after the last blood sample collection.
2.5 Pharmacokinetics
2.5.1 Outcome Measures
Pharmacokinetic analysis was performed (i) shortly after administration (1–2 h) to determine the immediate absorption of rebaudioside A, steviol and steviol glucuronide and (ii) during the OGTT (18.5–23 h, i.e. when maximal concentrations of steviol and steviol glucuronide were presumed to occur) to substantiate the pharmacodynamic effects by pharmacokinetic data. Blood was collected and the concentrations of rebaudioside A, steviol and steviol glucuronide were determined at 1, 2, 18.5, 19, 19.5, 20, 20.5, 21, 21.5, 22 and 23 h after the dosing of rebaudioside A (Fig. 2b, c). The maximal plasma concentration (Cmax), the time to reach the maximal plasma concentration (Tmax) and AUCs during the OGTT were analyzed.
2.5.2 Blood Collection
For each time point, blood (4 mL) was collected in a K2-EDTA tube. After centrifugation at 4 °C and 1950 × g for 10 min, plasma was collected and stored at − 80 °C.
2.5.3 Sample Preparation
The plasma samples were analyzed for rebaudioside A, steviol and steviol glucuronide. Analytical standards were used for rebaudioside A (Sigma–Aldrich, Belgium) and steviol (ChromaDex, LGC Standards, France). For steviol glucuronide, however, no analytical standard was readily available. We circumvented this by performing a dual analysis for every sample. First, we quantified the free steviol content using the steviol analytical standard. Second, we subjected the sample to β-glucuronidase, which cleaves the glucuronic acid from steviol glucuronide, resulting in “cleaved steviol”. Therefore, in the second analysis, we obtained a “total steviol” content which is the sum of (i) the free steviol and (ii) the cleaved steviol originally attached to a glucuronic acid from steviol glucuronide. Subsequently, we subtracted the free steviol content from the total steviol content, which allowed us to quantify the original concentration of steviol glucuronide [28]. The plasma samples were thawed to room temperature (RT) before initializing the sample preparation procedure.
For the determination of the rebaudioside A and free steviol concentration, 750 µL methanol was added to 75 µL plasma. The sample was vortexed and kept overnight at − 20 °C. After centrifugation at 5 °C at 14 000 × g for 5 min, the supernatant was collected and dried under nitrogen at RT. The extract was reconstituted in 250 µL methanol prior to analysis by ultra performance liquid chromatography with tandem mass spectrometry (UPLC-MS/MS).
For the determination of the steviol glucuronide concentration, the total steviol concentration was first determined using a separate procedure that included an enzymatic hydrolysis step. The total steviol concentration was subsequently subtracted by the free steviol concentration. For total steviol, 10 µL of β-glucuronidase (Helix pomatia, Roche Diagnostics, Switzerland) and 500 µL of ammonium acetate buffer (pH 5) were added to 75 µL of plasma. The sample was vortexed for 10 min, placed in a thermomixer at 37 °C and 1000 rpm for 6 h, and then cooled down. Next, the sample was extracted twice with 410 µL methyl tert-butyl ether by vortexing for 10 min. The organic phases were combined and dried under nitrogen at RT. The extract was reconstituted in 250 µL methanol prior to analysis by UPLC-MS/MS.
2.5.4 Quantification with HPLC-MS/MS
The extracts were analyzed using an UPLC-MS/MS instrument (Acquity Xevo TQ-S triple quadrupole®, Waters, USA). The injection volume was 5 µL and chromatographic separations were achieved using an Acquity UPLC BEH C18 column (1.7 μm particle size, 2.1 mm I.D. × 100 mm) set at 45 °C. The mobile phases consisted of water with 0.1% formic acid (A) and acetonitrile with 0.1% formic acid (B) at a flow rate of 0.4 mL/min. A linear gradient was programmed from 25 to 95% B in 4 min, which was kept constant for 0.5 min. Finally, the column was conditioned for 1.5 min with the initial mobile phase composition. The corresponding retention times were 2.23 min for rebaudioside A and 4.14 min for steviol.
Mass spectrometric detection was carried out in negative electrospray ionization mode with a capillary voltage of 3.0 kV and a cone voltage of 30 V. The desolvation and source temperature were set at 500 °C and 120 °C, respectively. High-purity nitrogen was used as cone gas with a flow of 50 L/h and as desolvation gas with a flow of 600 L/h. Collision-induced dissociation was performed using argon as the collision gas at a pressure of 4 × 10-3 mbar in the collision cell. The multiple reaction monitoring (MRM) transitions as well as the cone voltages and collision energies were optimized to MRM = 965.50 Da > 803.50 Da with 27.0 eV collision energy and MRM = 965.50 Da > 317.50 Da with 65.0 eV collision energy at 2.23 min retention time for rebaudioside A; MRM = 317.20 Da > 317.20 Da with 15.0 eV collision energy at 4.14 min retention time for steviol. Instrument control, data acquisition and data analysis were performed by Masslynx software (version 4.1, Waters). During data analysis, all chromatograms were processed using the TargetLynx™ software (Waters), and quantification was performed using matrix-matched calibration curves with the concentration ranging from 1 ng/mL to 100 ng/mL. The lower limit of quantification (LLOQ) for rebaudioside A, steviol and steviol glucuronide was 3.3 ng/mL in plasma. The extracts were diluted if necessary.
2.5.5 Validation Study and Quality Control
The method was fully validated in-house regarding selectivity, linearity and precision (recovery). The methods were considered selective, as no detection was observed at the retention times of rebaudioside A and steviol using blank plasma samples. The matrix effect was studied based on two calibration curves for each method. The first was built in the solvent, while the second was built by spiking blank plasma extracts, and their slopes were compared using a Student’s t-test at the 95% confidence level. The statistical analysis showed matrix effects for both methods. Hence the calibration curves had to be matrix matched. Then, the responses from the curve done with matrix extract were submitted to a Mandel’s fitting test, which showed that a linear regression model was preferred. Precision was assessed by analyzing spiked blank plasma at four different concentrations in quadruplicates for each level on 3 different days. The repeatability (r) and intermediate precision (Rw) were evaluated by calculating the coefficients of variation (CV) obtained for these two parameters, and were considered satisfactory if the CVs did not exceed the maximum allowed values from the Horwitz equation. The calculated CVs for each spiked level, presented in Table 1, are below the Horwitz limits. The apparent recoveries from the same assays ranged from 91 to 98% for rebaudioside A and from 95 to 106% for steviol. Hence, the bias for rebaudioside A and steviol was below 10% at each concentration level.
For each analytical batch, the parameters had to meet the associated criteria presented in Table 2 before the corresponding results were accepted.
2.6 Glucose Homeostasis
2.6.1 Outcome Measures
Blood was collected and glucose, insulin and C-peptide concentrations were determined at 18.5, 19, 19.5, 20, 20.5, 21, 21.5, 22 and 23 h after drug administration (i.e. − 0.5, 0, 0.5, 1, 1.5, 2, 2.5, 3 and 4 h after the glucose challenge of the OGTT) (Fig. 2c). The primary outcome was the area under the blood glucose concentration–time curve from 0 to 2 h after glucose challenge (AUCGlucose(0–2h)) for rebaudioside A vs. placebo. Secondary outcomes were AUCGlucose(– 0.5 to 0h/0–0.5h/0–4h), AUCInsulin(– 0.5 to 0h/0–0.5h/0–2h/0–4h), AUCC–peptide(–0.5–0h/0–0.5h/0–2h/0–4h), glucose excursion (ΔGlucose), maximal glucose (MaxGlucose), insulin (MaxInsulin) and C-peptide (MaxC–peptide).
2.6.2 Blood Collection
Blood was collected in a fluoride/oxalate tube for glucose (4 mL) and a serum separation tube (SST) for insulin (5 mL) and immediately sent for analysis. For C-peptide, blood (5 mL) was collected in a SST tube. The sample was rested at RT for 30 min to coagulate. After centrifugation at RT and 1950 × g for 10 min, serum was collected and stored at − 80 °C until analysis.
2.6.3 Analysis
Glucose concentrations were determined using the hexokinase/glucose-6-phosphate dehydrogenase method by ultraviolet colorimetry (Cobas® 6000/8000, Roche Diagnostics). Insulin and C-peptide concentrations were determined by electrochemiluminescence immunoassay (ECLIA, Cobas® 6000/8000, Roche Diagnostics). All analyses were performed in the Department of Laboratory Medicine of the University Hospitals Leuven, Belgium.
2.7 Adverse Events
The subjects were questioned about adverse events (AE) during the study visits, and the AEs were reported using the Medical Dictionary for Regulatory Activities (MedDRA). If necessary, vital signs or blood glucose, using a standard glucometer, were measured.
2.8 Data and Statistical Analysis
The sample size was calculated based on the hypothesis that the AUCGlucose(0–2h) would be lower after rebaudioside A compared to placebo. The study was designed to provide 90% power (two-sided α = 0.05) to detect a 10% difference assuming a SD of 16.51% from a preliminary study in mice [9]. Baseline characteristics were described as mean ± SD, median (25th and 75th interquartile) or n (%). Pharmacokinetic data are reported as mean ± SD, except for Tmax, which is presented as median (minimum; maximum). For pharmacodynamic data, mean ± SEM is used in figures and the estimate effect and corresponding 95% confidence interval are used in text. The AUC was calculated with the trapezoidal rule using OriginPro v9.0 (OriginLab Corporation, USA). For the pharmacokinetics, the average concentration at each time point was calculated for those above the LLOQ. For the AUC summary statistics, concentrations below the LLOQ (BLOQ) were substituted. A BLOQ concentration before the first measurable concentration was assigned a value of zero. BLOQ values occurring in a profile that were preceded and followed by a measurable concentration were assigned the average of the preceding and subsequent concentration. BLOQ values that occurred after a measurable concentration but were not followed by a measurable concentration were assigned the preceding concentration divided by 2. The effect of rebaudioside A vs. placebo on AUCs, glucose excursion or maximal glucose, insulin and C-peptide concentrations was evaluated using a linear mixed model with treatment and sequence as fixed factors and individuals within sequence as a random factor. Statistical analysis was performed with SPSS v28 (IBM, USA). Graphs were created with GraphPad Prism v9.2.0 software (GraphPad Software Inc., USA). The schematic overview of the trial was created with BioRender.com.
3 Results
3.1 Subject Characteristics
In total, 42 subjects were assessed for eligibility, 31 were randomized and 30 completed the trial (Fig. S1 of the Supplementary Information). One subject (placebo/rebaudioside A sequence) discontinued on day 2 of the first treatment period due to impossible intravenous catheter placement. Subject recruitment was performed between March 2019 and March 2021, with a temporary halt from December 2019 to June 2020 for interim analysis and due to COVID-19 precautions. Baseline subject characteristics are described in (Table 3).
3.2 Pharmacokinetics
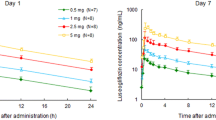
Rebaudioside A was detected in plasma at 1 h and 2 h after administration in, respectively, 28 and 29 subjects (Table 4). From 18.5 to 23 h following administration, rebaudioside A was still observed in the plasma of at least 19 subjects. The average plasma concentrations were 10-fold lower compared to those shortly after administration and declined over time. Steviol was detected as early as 1 h after administration in two subjects. However, from 18.5 to 21.5 h and at 23 h, steviol was detected in all subjects. Steviol glucuronide was already observed at 1 and 2 h in, respectively, 4 and 7 subjects, but was present in all subjects from 18.5 to 23 h.
The summary pharmacokinetics of rebaudioside A, steviol and steviol glucuronide are described in Table 5. While the maximal rebaudioside A plasma concentrations were observed at 2.0 h (Cmax = 178.5 ± 86.0 ng/mL), the Tmax of steviol and steviol glucuronide occurred at 19.5 h (Cmax = 119.0 ± 87.6 ng/mL and 3440.7 ± 1817.8 ng/mL, respectively).
3.3 Effect on Blood Glucose Homeostasis
Rebaudioside A administration did not result in lower glycemia nor higher insulin or C-peptide concentrations compared to placebo, neither in the fasting state nor during the OGTT (Fig. 3a–c). The AUCs, glucose excursion and maximal glucose, insulin and C-peptide concentrations were also comparable for all these parameters in both conditions (Figs. 3d–f, 4a–d and Table S2 of the Supplementary Information).

Glucose homeostasis parameters following rebaudioside A administration vs. placebo. (a–c) Concentration–time profiles of (a) blood glucose, (b) serum insulin and (c) serum C-peptide. (d–e) AUCs from − 0.5 to 0 h, 0 to 0.5 h, 0 to 2 h and 0 to 4 h of (d) glucose, (e) insulin and (f) C-peptide. Data are expressed as mean ± SEM. AUC area under the blood glucose/serum insulin/serum C-peptide concentration–time curve

Maximal glucose, insulin and C-peptide concentrations following rebaudioside A administration vs. placebo. (a) Maximal blood glucose excursion, (b) maximal glucose, (c) maximal insulin and (d) maximal C-peptide. Data are expressed as mean ± SEM. Δ excursion, Max maximum concentration
3.4 Safety
Oral administration of 3 g rebaudioside A was well tolerated and no serious AEs were identified. Treatment-emergent AEs were reported in three subjects and included headache (three events) and diarrhea (one event). Following placebo administration in two subjects, reported AEs were back pain (one event) and vagal reaction (one event). All AEs were mild in severity and were not (one event) or were unlikely (five events) to have been related to the study drug administered.
4 Discussion
Our study is the first to demonstrate the fate of orally administered rebaudioside A and its metabolites in patients with T2DM. We observed a rapid absorption of rebaudioside A, whereas steviol and steviol glucuronide reached their peak plasma concentrations 18.5 h after the ingestion of rebaudioside A. Although these metabolites are presumed to have an insulinotropic effect and were, theoretically, sufficiently present to engage the TRPM5 receptor on the β-cell, no glucose-lowering effect or enhanced insulin secretion could be demonstrated.
The rapid absorption of rebaudioside A in nearly all subjects is in contrast to previous research suggesting that the parent steviol glycosides are not absorbed or are absorbed to only a very small extent. In vitro, only a minor fraction of the rebaudioside A was transported through a Caco-2 cell monolayer and, in an ex vivo model of everted rat gastrointestinal sacs, no significant absorption of a stevia mixture occurred [16, 17]. Moreover, most in vivo studies in animals and humans did not observe absorption of steviol glycosides following oral exposure [12, 17]. We propose that the magnitude of the dose we used, the pharmacokinetic analysis method applied and the lower detection limit of our quantification method explain why we can detect and quantify rebaudioside A in plasma, in contrast to others [12, 17, 29]. Nevertheless, the absorption of rebaudioside A was still very low in our study. This poor absorption has been attributed to the molecular size and hydrophilic nature of steviol glycosides [15, 16]. In contrast, steviol is highly lipophilic, postulating a higher absorptive transport and suggesting more absorption into the systemic circulation than its parent compounds [17].
Following the ingestion of rebaudioside A, steviol was present in all subjects during the time window of 18.5–23 h, and its concentration peaked at 19.5 h. Previous research, however, did not consistently detect steviol after steviol glycoside intake. Two trials administering a lower steviol-equivalent dose compared to ours either did not detect steviol or observed it in only one out of eight subjects [12, 18]. In contrast, Roberts et al. administered stevioside at a higher steviol-equivalent dose and detected steviol in nine out of ten subjects, with a peak occurring around the same time, i.e. 19.2 h, but with a lower maximal concentration (77.2 ng/mL) than in our study (119.0 ng/mL) [19].
Obviously, our data concur that after intake of rebaudioside A, steviol glucuronide is the main circulating compound. Also in previous pharmacokinetic trials, steviol glucuronide was present in all subjects in the same concentration range as in our study [12, 18, 19]. Likewise, the time to reach the maximal concentration was comparable between our study (median: 19.5 h; mean: 20.1 h) and the one of Roberts et al. (mean: 21.6 h) [19].
At the onset of the study, we hypothesized that rebaudioside A would exert insulinotropic and anti-hyperglycemic effects at the time when steviol and steviol glucuronide were maximally present in the systemic circulation, as these compounds could potentiate TRPM5 ion channel activity in the pancreatic β-cells. However, despite the presence of steviol and steviol glucuronide, no glucose-lowering effect nor enhancement of insulin or C-peptide secretion could be observed in our subjects. Theoretically, the applied dose of rebaudioside A in the current study could be considered adequate to result in an anti-hyperglycemic effect. The amount of rebaudioside A that we administered (~ 32.6 mg/kg) is in the same range as the human equivalent dose of 500 mg/kg stevioside (~ 46.7 mg/kg rebaudioside A) applied in diabetic mice, which resulted in a profoundly reduced glycemia [9, 30], and is close to the dose used in a preliminary study in healthy volunteers (40 mg/kg stevioside ~ 48 mg/kg rebaudioside A) where no AEs were reported [19]. Practically, however, there are some uncertainties in the translational aspects of previous research in vitro and in mice that should be considered. First, it is debatable whether the exposure to the bioactive metabolite steviol glucuronide that we observe is sufficient to engage the TRPM5 ion channels. Philippaert et al. have shown that 10 µM steviol, rebaudioside A or stevioside efficiently potentiates TRPM5 activity [9]. Gu et al. showed that the application of 0.1 µM steviol glucuronide significantly increased glucose-induced insulin secretion in isolated mouse pancreatic islets [27]. In our subjects, the plasma concentration of steviol glucuronide at the start of the OGTT was on average 5.8 µM. This might still be lower than necessary for maximal potentiation of TRPM5 activity. Second, we cannot exclude the possibility that TRPM5 plays a different role in human pancreatic β-cells than in mice and that even an higher exposure of steviol glucuronide is necessary for maximal potentiation. Third, there is still the question of when a clinically relevant and significant insulinotropic and anti-hyperglycemic effect can be obtained if TRPM5 activity is potentiated in human subjects with T2DM.
Previous human data on anti-hyperglycemic effects of steviol glycosides in T2DM are limited. Concerning the glycemic effects of single steviol glycoside administration, there is only one trial that found a significant reduction of postprandial glucose after stevioside [22]. That study, however, examined the effect immediately after stevioside intake. Considering that the metabolites of steviol glycosides are actually responsible for its glycemic effects [7, 9, 26, 27], one may question how effects can be observed immediately after steviol glycoside intake and what the effect would be at maximal metabolite presence. Following chronic administration, the meta-analyses of Onakpoya et al. and Anker et al. suggested, respectively, a significant lower fasting blood glucose overall and non-significant reductions in fasting blood glucose and HbA1c in T2DM subgroups after intake of steviol glycosides, but they concluded that more studies are needed regarding the effect of steviol glycosides on T2DM biomarkers [25, 31]. For a follow-up study, one could consider that higher exposure to steviol and steviol glucuronide could be reached by chronic administration of high doses of steviol glycosides, resulting in a glycemic benefit in those subjects with well-preserved β-cell function. Moreover, the direct administration of steviol or steviol glucuronide itself could also be a more convenient way to achieve a faster and higher exposure to the bioactive compound steviol glucuronide.
A limitation of our study is the difficult subject recruitment, which resulted from the focus on a narrow targeted population that we expected would benefit most from potential anti-hyperglycemic effects. Considering the fundamental pathway by which steviol glycosides potentiate the β-cells [9], we focused on the subjects with the most possible residual β-cell mass and incorporated restrictions for possible confounding factors. Other strengths were the detection method and the limits developed for the characterization of rebaudioside A, steviol and steviol glucuronide and the right timing of the OGTT to measure the glycemic outcome.
5 Conclusion
Following rebaudioside A intake, rebaudioside A is absorbed and is present in blood shortly after administration. Steviol and steviol glucuronide are consistently present in all individuals. Rebaudioside A does not exert an insulinotropic or anti-hyperglycemic effect in patients with T2DM after single oral use, though steviol and steviol glucuronide are maximally present.
References
Kennelly EJ. Sweet and non-sweet constituents of Stevia rebaudiana. In: Kinghorn AD, editor. Stevia: the genus Stevia, medicinal and aromatic plants—industrial profiles. London: Taylor & Francis; 2002. p. 68–85.
European Commission. Amending Annex II to Regulation (EC) No. 1333/2008 of the European Parliament and of the council with regard to steviol glycosides. L 295; 2011.
FDA. Agency response letter. GRAS notice no. GRN 000395; 2012.
Chang JC, Wu MC, Liu IM, Cheng JT. Increase of insulin sensitivity by stevioside in fructose-rich chow-fed rats. Horm Metab Res. 2005;37(10):610–6. https://doi.org/10.1055/s-2005-870528.
Chen TH, Chen SC, Chan P, Chu YL, Yang HY, Cheng JT. Mechanism of the hypoglycemic effect of stevioside, a glycoside of Stevia rebaudiana. Planta Med. 2005;71(2):108–13. https://doi.org/10.1055/s-2005-837775.
Jeppesen PB, Gregersen S, Alstrup KK, Hermansen K. Stevioside induces antihyperglycaemic, insulinotropic and glucagonostatic effects in vivo: studies in the diabetic Goto-Kakizaki (GK) rats. Phytomedicine. 2002;9(1):9–14. https://doi.org/10.1078/0944-7113-00081.
Jeppesen PB, Gregersen S, Rolfsen SE, Jepsen M, Colombo M, Agger A, et al. Antihyperglycemic and blood pressure-reducing effects of stevioside in the diabetic Goto-Kakizaki rat. Metabolism. 2003;52(3):372–8. https://doi.org/10.1053/meta.2003.50058.
Myint KZ, Chen JM, Zhou ZY, Xia YM, Lin J, Zhang J. Structural dependence of antidiabetic effect of steviol glycosides and their metabolites on streptozotocin-induced diabetic mice. J Sci Food Agric. 2020;100(10):3841–9. https://doi.org/10.1002/jsfa.10421.
Philippaert K, Pironet A, Mesuere M, Sones W, Vermeiren L, Kerselaers S, et al. Steviol glycosides enhance pancreatic beta-cell function and taste sensation by potentiation of TRPM5 channel activity. Nat Commun. 2017;8:14733. https://doi.org/10.1038/ncomms14733.
EFSA. Scientific opinion on the safety of steviol glycosides for the proposed uses as a food additive. EFSA J. 2010;8(4):1537. https://doi.org/10.2903/j.efsa.2010.1537
Hutapea AM, Toskulkao C, Buddhasukh D, Wilairat P, Glinsukon T. Digestion of stevioside, a natural sweetener, by various digestive enzymes. J Clin Biochem Nutr. 1997;23(3):177–86. https://doi.org/10.3164/jcbn.23.177.
Geuns JM, Buyse J, Vankeirsbilck A, Temme EH. Metabolism of stevioside by healthy subjects. Exp Biol Med (Maywood). 2007;232(1):164–73.
Gardana C, Simonetti P, Canzi E, Zanchi R, Pietta P. Metabolism of stevioside and rebaudioside A from Stevia rebaudiana extracts by human microflora. J Agric Food Chem. 2003;51(22):6618–22. https://doi.org/10.1021/jf0303619.
Koyama E, Kitazawa K, Ohori Y, Izawa O, Kakegawa K, Fujino A, et al. In vitro metabolism of the glycosidic sweeteners, stevia mixture and enzymatically modified stevia in human intestinal microflora. Food Chem Toxicol. 2003;41(3):359–74. https://doi.org/10.1016/s0278-6915(02)00235-1.
Geuns JMC, Buyse J, Vankeirsbilck A, Temme EHM, Compernolle F, Toppet S. Identification of steviol glucuronide in human urine. J Agric Food Chem. 2006;54(7):2794–8. https://doi.org/10.1021/jf052693e.
Koyama E, Sakai N, Ohori Y, Kitazawa K, Izawa O, Kakegawa K, et al. Absorption and metabolism of glycosidic sweeteners of stevia mixture and their aglycone, steviol, in rats and humans. Food Chem Toxicol. 2003;41(6):875–83. https://doi.org/10.1016/s0278-6915(03)00039-5.
Geuns JM, Augustijns P, Mols R, Buyse JG, Driessen B. Metabolism of stevioside in pigs and intestinal absorption characteristics of stevioside, rebaudioside A and steviol. Food Chem Toxicol. 2003;41(11):1599–607. https://doi.org/10.1016/s0278-6915(03)00191-1.
Wheeler A, Boileau AC, Winkler PC, Compton JC, Prakash I, Jiang X, et al. Pharmacokinetics of rebaudioside A and stevioside after single oral doses in healthy men. Food Chem Toxicol. 2008;46(Suppl 7):S54-60. https://doi.org/10.1016/j.fct.2008.04.041.
Roberts A, Lynch B, Rogerson R, Renwick A, Kern H, Coffee M, et al. Chemical-specific adjustment factors (inter-species toxicokinetics) to establish the ADI for steviol glycosides. Regul Toxicol Pharmacol. 2016;79:91–102. https://doi.org/10.1016/j.yrtph.2016.05.017.
Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol. 2018;14(2):88–98. https://doi.org/10.1038/nrendo.2017.151.
Davies MJ, D’Alessio DA, Fradkin J, Kernan WN, Mathieu C, Mingrone G, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;41(12):2669–701. https://doi.org/10.2337/dci18-0033.
Gregersen S, Jeppesen PB, Holst JJ, Hermansen K. Antihyperglycemic effects of stevioside in type 2 diabetic subjects. Metabolism. 2004;53(1):73–6. https://doi.org/10.1016/j.metabol.2003.07.013.
Barriocanal LA, Palacios M, Benitez G, Benitez S, Jimenez JT, Jimenez N, et al. Apparent lack of pharmacological effect of steviol glycosides used as sweeteners in humans. A pilot study of repeated exposures in some normotensive and hypotensive individuals and in type 1 and type 2 diabetics. Regul Toxicol Pharmacol. 2008;51(1):37–41. https://doi.org/10.1016/j.yrtph.2008.02.006.
Maki KC, Curry LL, Reeves MS, Toth PD, McKenney JM, Farmer MV, et al. Chronic consumption of rebaudioside A, a steviol glycoside, in men and women with type 2 diabetes mellitus. Food Chem Toxicol. 2008;46(Suppl 7):S47-53. https://doi.org/10.1016/j.fct.2008.05.007.
Bundgaard Anker CC, Rafiq S, Jeppesen PB. Effect of steviol glycosides on human health with emphasis on type 2 diabetic biomarkers: a systematic review and meta-analysis of randomized controlled trials. Nutrients. 2019. https://doi.org/10.3390/nu11091965.
Jeppesen PB, Gregersen S, Poulsen CR, Hermansen K. Stevioside acts directly on pancreatic beta cells to secrete insulin: actions independent of cyclic adenosine monophosphate and adenosine triphosphate-sensitive K+-channel activity. Metabolism. 2000;49(2):208–14. https://doi.org/10.1016/s0026-0495(00)91325-8.
Gu W, Rebsdorf A, Anker C, Gregersen S, Hermansen K, Geuns JMC, et al. Steviol glucuronide, a metabolite of steviol glycosides, potently stimulates insulin secretion from isolated mouse islets: studies in vitro. Endocrinol Diabetes Metab. 2019;2(4):e00093. https://doi.org/10.1002/edm2.93.
Guilbert A, De Cremer K, Heene B, Demoury C, Aerts R, Declerck P, et al. Personal exposure to traffic-related air pollutants and relationships with respiratory symptoms and oxidative stress: a pilot cross-sectional study among urban green space workers. Sci Total Environ. 2019;649:620–8. https://doi.org/10.1016/j.scitotenv.2018.08.338.
Nikiforov AI, Rihner MO, Eapen AK, Thomas JA. Metabolism and toxicity studies supporting the safety of rebaudioside D. Int J Toxicol. 2013;32(4):261–73. https://doi.org/10.1177/1091581813492828.
FDA. Estimating the maximum safe starting dose in initial clinical trials for therapeutics in adult healthy volunteers. Silver Spring, MD: FDA; 2005.
Onakpoya IJ, Heneghan CJ. Effect of the natural sweetener, steviol glycoside, on cardiovascular risk factors: a systematic review and meta-analysis of randomised clinical trials. Eur J Prev Cardiol. 2015;22(12):1575–87. https://doi.org/10.1177/2047487314560663.
Acknowledgements
We would like to thank all individuals for their interest, time and enthusiasm in participating in this clinical trial. We wish to acknowledge the team of endocrinology at University Hospitals Leuven, general practitioners, and Diabetes Liga for helping with the recruitment of patients and Kaat Beunen for her practical assistance in conducting this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The study was funded by a KU Leuven Grant (TRPLe: TRP Research Platform Leuven - C14/17/091) and FWO Vlaanderen (G0C2420N and GOE0217N).
Conflict of interest
There is no conflict of interest for any of the authors.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Code availability
Not applicable.
Ethics approval
The study was approved by the institutional review board (Ethics Committee Research UZ/KU Leuven, Leuven, Belgium) and the national competent authority (Federal Agency for Medicines and Health Products (FAMPH), Belgium). The study was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments.
Consent to participate
Informed consent was obtained from all individual participants prior to the initiation of any study-related procedure.
Consent for publication
Not applicable.
Author contributions
CS, KP, RV and BVdS contributed substantially to the conceptualization of the study. CS, RVG, AM and BVdS recruited subjects, conducted the experiments and collected data. JdH coordinated the clinical team involved in practical assistance for the trial and the manufacturing of the drug. EA manufactured the drug. CS, SG, EVH and JVL analyzed the pharmacokinetic samples. CS, CW and JB analyzed the pharmacodynamic samples. CS and BVdS did the formal analysis. RV provided funding. BVdS supervised the project. CS drafted the manuscript, and RV and BVdS reviewed and edited the manuscript. All authors contributed to the interpretation of the data and critically revised the manuscript.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Simoens, C., Philippaert, K., Wuyts, C. et al. Pharmacokinetics of Oral Rebaudioside A in Patients with Type 2 Diabetes Mellitus and Its Effects on Glucose Homeostasis: A Placebo-Controlled Crossover Trial. Eur J Drug Metab Pharmacokinet 47, 827–839 (2022). https://doi.org/10.1007/s13318-022-00792-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13318-022-00792-7