
Abstract
One-lung ventilation (OLV) is the most commonly used ventilation strategy during esophagectomy. However, two-lung ventilation (TLV) with artificial pneumothorax has been applied in recent years during esophagectomy. It is unclear whether TLV takes advantages over OLV for esophagectomy. Here, we conducted a meta-analysis to compare the effects of TLV and OLV for esophagectomy. We searched relevant studies from the Cochrane Central Register of Controlled Trials, Pubmed, and Embase in November 2020. We included studies that compared the effects of TLV with OLV in esophagectomy and provided sufficient perioperative and postoperative data. We extracted data of postoperative outcomes (postoperative pulmonary complications, anastomotic leak, hospital stay) and surgical variables (thoracic phrase time, blood loss, the number of total resected thoracic lymph nodes). We calculated the risk ratio (RR) for dichotomous data and the weighted mean differences (WMDs) for continuous data. Six studies with 1725 patients were included in this meta-analysis. TLV was associated with significantly lower incidence of postoperative pulmonary complications [RR = 0.714; 95% confidence interval (CI) = (0.534, 0.956); P = 0.023], shorter hospital stay [WMD = − 0.148; 95% CI = (− 0.246, − 0.051); P = 0.003], less blood loss [WMD = − 0.352; 95% CI = (− 0.528, − 0.176); P < 0.001] and more resected thoracic lymph nodes [WMD = 0.207; 95% CI = (0.003, 0.4120); P = 0.047] than OLV. Moreover, TLV consumed similar time for thoracic phrase [WMD = − 0.289; 95% CI = (− 0.661, 0.083); P = 0.128], and yielded a comparable rate of anastomotic leak [RR = 1.086; 95% CI = (0.842, 1.400); P = 0.525] compared with OLV. TLV with artificial pneumothorax resulted in less trauma than OLV. TLV with artificial pneumothorax is safe and could be a choice of ventilation strategy for esophagectomy.



Similar content being viewed by others

References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68:394–424
Sohda M, Kuwano H (2017) Current status and future prospects for esophageal cancer treatment. Ann Thorac Cardiovasc Surg 23:1–11
Low DE, Kuppusamy MK, Alderson D, Cecconello I, Chang AC, Darling G et al (2019) Benchmarking complications associated with esophagectomy. Ann Surg 269:291–298
Lohser J, Slinger P (2015) Lung injury after one-lung ventilation: a review of the pathophysiologic mechanisms affecting the ventilated and the collapsed lung. Anesth Analg 121:302–318
Knoll H, Ziegeler S, Schreiber J-U, Buchinger H, Bialas P, Semyonov K et al (2006) Airway injuries after one-lung ventilation: a comparison between double-lumen tube and endobronchial blockera randomized, prospective, Controlled Trial. Anesthesiology 105:471–477
Palanivelu C, Prakash A, Senthilkumar R, Senthilnathan P, Parthasarathi R, Rajan PS et al (2006) Minimally invasive esophagectomy: thoracoscopic mobilization of the esophagus and mediastinal lymphadenectomy in prone position–experience of 130 patients. J Am Coll Surg 203:7–16
Haagh TJ, Buise MP, Luyer MDP, Nieuwenhuijzen GAP (2019) Two-lung ventilation during prone minimally invasive thorascopic oesophagectomy: a case series. Eur J Anaesthesiol 36:307–309
Saikawa D, Okushiba S, Kawata M, Okubo T, Kitashiro S, Kawarada Y et al (2014) Efficacy and safety of artificial pneumothorax under two-lung ventilation in thoracoscopic esophagectomy for esophageal cancer in the prone position. Gen Thorac Cardiovasc Surg 62:163–170
Singh M, Uppal R, Chaudhary K, Javed A, Aggarwal A (2016) Use of single-lumen tube for minimally invasive and hybrid esophagectomies with prone thoracoscopic dissection: case series. J Clin Anesth 33:450–455
Tanaka S, Kawakami T, Ehara T, Hirabayashi Y (2015) Anesthetic management of patients undergoing single-lumen tracheal tube ventilation with artificial pneumothorax in thoracolaparoscopic esophagectomy. Masui 64:978–980
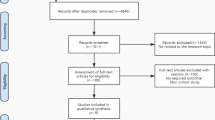
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 62:1006–1012
Wan X, Wang W, Liu J, Tong T (2014) Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 14:135
Luo D, Wan X, Liu J, Tong T (2018) Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res 27:1785–1805
Bonavina L, Laface L, Abate E, Punturieri M, Agosteo E, Nencioni M (2012) Comparison of ventilation and cardiovascular parameters between prone thoracoscopic and Ivor Lewis esophagectomy. Updates Surg 64:81–85
Cai L, Li Y, Sun L, Yang XW, Wang WB, Feng F et al (2017) Better perioperative outcomes in thoracoscopic-esophagectomy with two-lung ventilation in semi-prone position. J Thorac Dis 9:117–122
Lin M, Shen Y, Wang H, Fang Y, Qian C, Xu S et al (2018) A comparison between two lung ventilation with CO (2) artificial pneumothorax and one lung ventilation during thoracic phase of minimally invasive esophagectomy. J Thorac Dis 10:1912–1918
Nomura S, Tsujimoto H, Ishibashi Y, Fujishima S, Kouzu K, Harada M et al (2020) Efficacy of artificial pneumothorax under two-lung ventilation in video-assisted thoracoscopic surgery for esophageal cancer. Surg Endosc 34:5501–5507
Souche R, Nayeri M, Chati R, Huet E, Donici I, Tuech JJ et al (2020) Thoracoscopy in prone position with two-lung ventilation compared to conventional thoracotomy during Ivor Lewis procedure: a multicenter case-control study. Surg Endosc 34:142–152
Zhang R, Liu S, Sun H, Liu X, Wang Z, Qin J et al (2014) The application of single-lumen endotracheal tube anaesthesia with artificial pneumothorax in thoracolaparoscopic oesophagectomy. Interact Cardiovasc Thorac Surg 19:308–310
Licker M, Fauconnet P, Villiger Y, Tschopp JM (2009) Acute lung injury and outcomes after thoracic surgery. Curr Opin Anaesthesiol 22:61–67
Howells P, Thickett D, Knox C, Park D, Gao F, Tucker O et al (2016) The impact of the acute respiratory distress syndrome on outcome after oesophagectomy. Br J Anaesth 117:375–381
Fitzmaurice BG, Brodsky JB (1999) Airway rupture from double-lumen tubes. J Cardiothorac Vasc Anesth 13:322–329
Funding
None.
Author information
Authors and Affiliations
Contributions
H-YD, YZ, and Ying Ren collected data and drafted the manuscript. YZ and YX analyzed the data under H-YD designed the study and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
None declared.
Ethical approval
Our study was approved by the Ethics Committee of West China Hospital, Sichuan University (No. 20201101). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
There is no need for informed consent because Authors just did the literature review without any certain patients.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
13304_2022_1269_MOESM1_ESM.tif
Supplementary file1 Supplementary Fig. 1. the sensitivity analysis based on postoperative pulmonary complications (a), hospital stay (b), anastomotic leak (c), thoracic phrase time (d), blood loss (e) and number of total resected thoracic lymph nodes (f). (TIF 1866 KB)
Rights and permissions
About this article

Cite this article
Deng, HY., Zhang, Y., Ren, Y. et al. Two-lung ventilation or one-lung ventilation for esophagectomy: maybe the more is better from the evidence of meta-analysis. Updates Surg 74, 1199–1207 (2022). https://doi.org/10.1007/s13304-022-01269-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13304-022-01269-7