
Abstract
Introduction
Large-scale clinical trials of sodium-glucose cotransporter 2 inhibitors (SGLT2i) demonstrate proteinuria-reducing effects in diabetic kidney disease, even after treatment with renin–angiotensin inhibitors. The precise mechanism for this favorable effect remains unclear. This prospective open-label single-arm study investigated factors associated with a reduction in proteinuria after SGLT2i administration.
Methods
Patients with type 2 diabetes (T2DM) who had glycated hemoglobin (HbA1c) levels ≥ 6.5% despite dietary and/or oral hypoglycemic monotherapy were recruited and administered the recommended daily dose of SGLT2i for 4 months. Dual primary outcomes were changes in the urine albumin-to-creatinine ratio (uACR) and urine liver-type fatty acid-binding protein (L-FABP)-to-creatinine ratio (uL-FABPCR) at month 4 from baseline. Changes in kidney injury, inflammation, and oxidative stress biomarkers were investigated as secondary endpoints to examine the effects of this treatment on the kidney. The correlation between renal outcomes and clinical indicators, including circulating tumor necrosis factor receptors (TNFR) 1 and 2, was evaluated using univariate and multivariate analyses.
Results
Participants (n = 123) had a mean age of 64.1 years (SD 13.4), with 50.4% being male. The median BMI was 25.8 kg/m2 (interquartile range (IQR) 23.1–28.9), and the median HbA1c level was 7.3% (IQR 6.9–8.3). After SGLT2i administration, the uACR declined from 19.2 mg/gCr (IQR 7.1–48.7) to 13.3 mg/gCr (IQR 7.5–31.6), whereas the uL-FABPCR was not influenced. In univariate analysis, the change in log-transformed uACR due to SGLT2i administration showed a positive correlation with the change in serum TNFR1 level (R = 0.244, p < 0.01). Multivariate regression analysis, including confounding factors, showed that the changes in serum TNFR1 level were independently associated with the changes in the log-transformed uACR (independent t = 2.102, p < 0.05).
Conclusion
After the 4-month SGLT2i administration, decreased albuminuria level was associated with decreased serum TNFR level in patients with T2DM.
Trial Registration Number
UMIN000031947.
Plain Language Summary
Previous studies have demonstrated the synergistic proteinuria-reducing effect of sodium-glucose cotransporter 2 inhibitors (SGLT2i) in combination therapy with renin–angiotensin system blockers; however, the underlying mechanisms of this effect are poorly understood. This study was based on our hypothesis that the proteinuria-reducing effect is associated with the anti-inflammatory effects of SGLT2i beyond the effect on glycemic control. In total, 123 patients with type 2 diabetes mellitus (T2DM) were administered the recommended daily dose of SGLT2i for 4 months. Dual primary outcomes were changes in the urine albumin-to-creatinine ratio (uACR) and urine liver-type fatty acid-binding protein (L-FABP)-to-creatinine ratio (uL-FABPCR) as markers of glomerular and proximal tubular damage at 4 months from the baseline. Secondary outcomes included changes in kidney injury biomarkers, inflammation, and oxidative stress to examine the effects of treatment on the kidneys. The correlation between renal outcomes and clinical indicators, including circulating tumor necrosis factor receptors (TNFR) 1 and 2, was evaluated using univariate and multivariate analyses. We found that administration of SGLT2i decreased the urine albumin-to-creatinine ratio but did not affect the urine liver-type fatty acid-binding protein-to-creatinine ratio. Further, SGLT2i may exert a proteinuria-reducing effect dependent on the anti-inflammatory effect in patients with T2DM. The inflammation-reducing and renoprotective mechanisms of SGLT2i remain to be fully clarified, but this study provides novel evidence regarding the mechanism. The study findings can help in developing anti-inflammatory agents for metabolic diseases.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Why carry out this study? |
Sodium-glucose cotransporter 2 inhibitors (SGLT2i) demonstrate a synergistic proteinuria-reducing effect in combination therapy with renin–angiotensin system blockers; however, the underlying mechanisms of the SGLT2i proteinuria-reducing effect remain poorly understood. |
We hypothesized that the proteinuria-reducing effect is associated with the anti-inflammatory effects of SGLT2i beyond the effect on glycemic control. |
What was learned from this study? |
SGLT2i exerts an anti-inflammatory effect in patients with type 2 diabetes mellitus (T2DM). |
SGLT2i may exert proteinuria-reducing effects that are dependent on the inhibition of serum tumor necrosis factor receptors (TNFR). |
The study findings can aid in developing anti-inflammatory agents for metabolic diseases, such as T2DM and diabetic kidney disease. |
Introduction
The general goal of diabetes treatment is to reduce mortality and maintain a quality of life comparable to that of healthy individuals; therefore, it is essential to prevent the onset and progression of diabetic complications. Adverse renal events are the most common and serious complications of type 2 diabetes mellitus (T2DM). Micro- or macroalbuminuria is present in approximately 25% of people with T2DM [1, 2]. The development of albuminuria marks the progression of renal damage [3, 4] and predicts the cardiovascular risk in patients with T2DM [5, 6]. Therefore, evidence-based clinical practice guidelines for chronic kidney disease (CKD) endorse regular evaluation and reduction of albuminuria in patients with T2DM [7, 8]. Both angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs) reduce the progression of albuminuria and even induce regression of microalbuminuria to normoalbuminuria. However, residual risk remains, with approximately 30% of patients with T2DM and the presence of microalbuminuria progressing to macroalbuminuria despite the currently recommended treatment protocols [9].
Sodium-glucose cotransporter 2 (SGLT2) inhibitors (SGLT2i), which were originally designed as hypoglycemic agents for treating T2DM, have increasingly shown renal and cardiovascular protective properties in several randomized controlled trials (RCTs) [10,11,12,13]. Although the underlying mechanisms that provide renal benefits are still poorly understood, in recent post hoc analyses from the EMPA-REG OUTCOME (BI10773 [Empagliflozin]) Cardiovascular Outcome Event Trial, it was suggested that short-term reduction in albuminuria had a statistically significant association with a decreased risk of long-term renal function decline [14]. Additionally, early changes in albuminuria after treatment with SGLT2i were independently associated with long-term kidney and cardiovascular outcomes [15].
Several basic studies have shown that SGLT2i ameliorates albuminuria by attenuating glomerular hyperfiltration [16,17,18]. One possible mechanism could be suppressing the induced inflammatory response and oxidative stress.
Chronic inflammation is increasingly believed to be an essential mechanism for developing macroalbuminuria [19]. Many proinflammatory cytokines and chemokines may play important roles in the initiation and progression of diabetic kidney disease (DKD) [20]. Furthermore, tumor necrosis factor alpha (TNFα) is a well-known proinflammatory cytokine associated with the progression of kidney disease [21]. Cellular responses to TNFα are induced through two receptors, TNF receptor 1 (TNFR1) and TNF receptor 2 (TNFR2) [22]. Both TNFR1 and TNFR2 have cleaved and solubilized extracellular domains that appear in the blood at the initial stage of inflammation. Moreover, progranulin (PGRN) binds to TNFRs [23]. Elevated levels of circulating TNFR1 and PGRN are implicated in the initiation and progression of albuminuria [24, 25]. Higher plasma levels of soluble urokinase plasminogen activator receptor (suPAR) have also been associated with an increased risk of progression of DKD [26]. Although post hoc analyses of several clinical trials showed that SGLT2i decreased the plasma TNFR levels [27, 28], the ambiguity of the causal relationship remains as a result of the lack of intervention trials. Additionally, less attention has been given to the association of soluble TNFR altered by SGLT2i with early changes in albuminuria in patients with T2DM.
Previous clinical data indicated that DKD was also accompanied by renal tubular disorder [29, 30] and that urinary liver-type free fatty acid-binding protein (L-FABP), which is involved in renal tubulointerstitial damage and oxidative stress, might be a predictive factor for renal and cardiovascular prognosis in patients with T2DM [31].
Therefore, this study was designed to test the hypothesis that the blockade of SGLT2 reduces inflammation independent of glycemic control in patients with T2DM and that changes in inflammatory markers are closely associated with renoprotection. As dual primary outcomes, we measured the urinary excretion of albumin and L-FABP before and after the administration of SGLT2i in patients with T2DM. To further characterize the effect of this treatment on the kidney, we also examined changes in biomarkers for kidney injury, inflammation, and oxidative stress as secondary endpoints.
Methods
Ethics Conduct
This study complied with the Declaration of Helsinki and Good Clinical Practice guidelines and was conducted as a collaborative multicenter research effort led by Tokushima University. To ensure a comprehensive ethical approval across all participating facilities, each institution sought consolidated review by the Institutional Review Board of Tokushima University Hospital. Subsequently, the Institutional Review Board of Tokushima University Hospital granted approval for all study sites involved in this multicenter study (approval date April 23, 2018; approval ID 3149). The research proceeded after securing the necessary approvals from each research institution. Additional matters requiring approval, such as protocol amendments, were evaluated and approved by the institutional review boards as per need. The trial was registered with the University Hospital Medical Information Network (UMIN No. 000031947). The patients were provided with detailed explanations of the study protocol. All participants provided written informed consent for participation in the study and publication of the study results. Nonetheless, all patient records and information were anonymized before the analysis.
Study Design and Population
This was a multicenter, prospective, open-label, single-arm study. Overall, 123 Japanese participants (62 men and 61 women) were selected for this study from outpatients with T2DM who visited the Department of Endocrinology and Metabolism at Tokushima University Hospital, Anan Medical Center, or Tamaki Aozora Hospital between August 2018 and July 2023. The diagnosis of T2DM was based on the criteria of the Japan Diabetes Society [32]. Participants were considered eligible if they were at least 20 years old; patients with T2DM whose glycated hemoglobin (HbA1c) level was ≥ 6.5% via diet therapy; and/or patients received monotherapy of oral hypoglycemic agents (OHA) such as sulfonylureas (SU), biguanides, α-glucosidase inhibitors, thiazolidine, or dipeptidyl peptidase 4 (DPP4) inhibitors for 12 weeks or longer. The exclusion criteria were as follows: (1) hypersensitivity or a contraindication to SGLT2i; (2) type 1 diabetes; (3) severe diabetic metabolic complications, such as ketoacidosis; (4) treatment with SGLT2i within 12 weeks before screening; (5) treatment with insulin or glucagon-like peptide 1 receptor agonist therapy within 12 weeks before screening; (6) taking steroids, nonsteroidal anti-inflammatory drugs, or antibiotics; (7) poorly controlled or unstable diabetes (an increase in HbA1c level > 3% in the 12 weeks before screening); (8) various inflammatory autoimmune diseases; (9) estimated glomerular filtration rates (eGFR) ≤ 30 mL/min/1.73 m2 and hemodialysis; (10) infectious diseases; (11) pregnancy or breastfeeding; or (12) inappropriate for this study as assessed by the investigators. Eligible patients received SGLT2i of either canagliflozin, tofogliflozin, ipragliflozin, luseogliflozin, dapagliflozin, or empagliflozin at a constant dosage in addition to their previous treatment for 12 weeks. SGLT2i therapy was initiated at the lowest recommended daily dose (100 mg canagliflozin, 20 mg tofogliflozin, 50 mg ipragliflozin, 2.5 mg luseogliflozin, 5 mg dapagliflozin, and 10 mg empagliflozin). Notably, no dose escalations were observed. Other medications remained unchanged during the study period. These drugs were formulated at least 12 weeks before this study.
Measures, Definitions, and Outcomes
The dual primary outcomes were changes in urinary albumin and L-FABP excretion from the baseline measurements. The secondary endpoints included changes in the laboratory data. The following parameters were measured in random urine samples, and the results were expressed as a ratio to urinary creatinine (Cr) as follows: albumin, L-FABP, 8-hydroxy-2′-deoxyguanosine (8-OHdG), neutrophil gelatinase-associated lipocalin (NGAL), type IV collagen (Col4), and Cr. Blood samples were collected from each patient and used to determine blood cell counts and HbA1c, serum Cr, cystatin C (cys-C), uric acid (UA), aspartate aminotransferase (AST), alanine aminotransferase (ALT), γ-glutamyl transpeptidase (γ-GTP), low-density lipoprotein cholesterol (LDL-C), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), erythropoietin (Epo), N-terminal pro-brain natriuretic peptide (NT-proBNP), C-reactive protein (CRP), TNFR1, TNFR2, PGRN, and NGAL levels. HbA1c levels were measured using an automated analyzer (ADAMS A1c HA-8181; Arkray, Kyoto, Japan). Serum Cr and UA levels were measured using enzyme reactions (Kinos Co, Tokyo, Japan). Serum levels of AST, ALT, and γ-GTP were measured using the Japan Society of Clinical Chemistry advised methods (Kanto Chemical Co., Tokyo, Japan). Serum TC, HDL-C, and TG levels were measured directly using an enzymatic method (Sekisui Medical, Tokyo, Japan). The serum LDL-C levels were calculated using the Friedewald equation. Serum cys-C, Epo, NT-proBNP, urinary albumin, L-FABP, NGAL, and Col4 levels were measured by a central measurement laboratory (SRL, Inc., Tokyo, Japan). The serum cys-C levels were measured using a colloidal gold assay. Serum Epo and NT-proBNP levels were measured using a chemiluminescent enzyme immunoassay (CLEIA). Urinary albumin levels were measured by immunoturbidimetry. Furthermore, urinary L-FABP levels were measured using an immunoturbidimetry CLEIA. Urine NGAL levels were measured using a chemiluminescent immunoassay. Urinary Col4 level was measured by enzyme immunoassay. Furthermore, we used an enzyme-linked immunosorbent assay to measure the levels of serum CRP, TNFR1, TNFR2, PGRN, suPAR, and NGAL (R&D Systems, Minneapolis, Minnesota, USA). The concentration of urinary 8-OHdG was analyzed using an oxidative stress analyzer, ICR–001 (Techno Medica Co., Ltd. Yokohama, Japan). The eGFR values based on serum Cr (eGFRcreat) and serum cys-C (eGFRcys) levels were calculated using the Japanese Society of Nephrology equations [33, 34]. Urine albumin level less than 30 mg/gCr was considered normal, microalbuminuria was defined as urine albumin level between 30 and 300 mg/gCr, and urine albumin level greater than 300 mg/gCr was considered macroalbuminuria.
Statistical Analysis
Continuous variables are expressed as mean ± standard deviation (SD) or median (interquartile range, IQR). The Shapiro–Wilk test was used to determine if the values were normally distributed. Differences between the baseline and follow-up measurements were assessed using paired t tests or Wilcoxon signed-rank sum test (as appropriate). Prior to regression analyses, the urine albumin-to-creatinine ratio (uACR) and serum CRP level were log-transformed (uACR (log) and CRP (log)) to adjust for the measure’s highly skewed distribution. The relationships between the changes in uACR (log) by SGLT2i administration and the changes in secondary endpoints during the study were examined using a single linear regression analysis. All statistical analyses were performed using Microsoft Office Excel 2019 (Microsoft, Richmond, CA, USA), GraphPad Prism 8 software (GraphPad Software, San Diego, CA, USA), and EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan). A two-sided p value less than 0.05 was considered statistically significant. The G*Power software supports sample size and power calculations for various statistical methods.
Results
Baseline Characteristics of Participants
A total of 146 participants initially enrolled in this study and initiated therapy with SGLT2i, including canagliflozin, tofogliflozin, ipragliflozin, luseogliflozin, dapagliflozin, and empagliflozin. Over the course of the 4-month intervention period, 23 patients dropped out of the study for various reasons: urinary tract infection (n = 1), rapid GFR decline (n = 1), stroke (n = 1), worsening of dementia (n = 1), acute myocardial infarction (n = 1), loss to follow-up (n = 7), and not meeting the inclusion criteria (n = 11). A complete case analysis was conducted. Table 1 provides a comprehensive overview of baseline clinical and biochemical characteristics, including lipid levels, liver enzyme (ALT) levels, and renal function (eGFRcreat and eGFRcys). Participants (n = 123) had a mean age of 64.1 years (SD 13.4), with 50.4% being male. The median BMI was 25.8 kg/m2 (IQR 23.1–28.9), and the median HbA1c level was 7.3% (IQR 6.9–8.3). The mean/median eGFRcreat and eGFRcys at baseline were 73.8 mL/min/1.73 m2 (IQR 65.1–88.0) and 83.8 mL/min/1.73 m2 (SD 22.6), respectively. Low eGFRcys (< 60 mL/ min/1.73 m2) was observed in 17 (13.8%) participants, while 18 participants (14.6%) had a low eGFRcreat < 60 mL/min/1.73 m2. The median uACR at the baseline was 19.2 mg/gCr (IQR 7.1–48.7). Notably, 35 (28.5%) patients had microalbuminuria, and 6 (4.9%) had macroalbuminuria when tested by uACR.
Among the 123 participants, 44 (35.8%) were taking renin–angiotensin system inhibitors, including ARBs (n = 44), while 42 participants (34.1%) were on statin therapy at baseline. Thirty-eight patients were following diet therapy, whereas others were on an OHA. The most common class of oral OHA concomitantly used was metformin (42%), followed by DPP4 inhibitors (19.5%), SUs (14%), pioglitazone (3.3%), and α-GI (0.8%). Importantly, these treatments remained unchanged in the 12 weeks leading up to the study. The details of the SGLT2i used in this study are shown in Table 2.
Outcomes
Changes in laboratory variables are presented in Table 3. In dual primary study outcomes, the uACR levels were significantly reduced from 19.2 mg/gCr (IQR 7.1–48.7) to 13.3 mg/gCr (IQR 7.5–31.6) 4 months after initiation of SGLT2i, whereas no significant change was observed in urinary L-FABP excretion throughout the study. Compared with the baseline level, the patients’ BMI, SBP, DBP, and pulse pressure (PP) were significantly decreased, with no increase in pulse rate at 4 months after the start of the daily SGLT2i regimen. Hematocrit levels were elevated, and HbA1c level was significantly decreased 4 months after the start of the daily SGLT2i regimen. The eGFRcys, rather than the eGFRcreat, significantly decreased by 4.0 mL/min/1.73 m2. A significant decrease was observed in the UA, AST, ALT, γ-GTP, and TG levels. The HDL-C and LDL-C levels were significantly increased. The Epo levels were significantly increased, whereas the NT-proBNP levels were significantly decreased. There was a significant decrease in the levels of the inflammatory markers, such as serum CRP (from 552.8 ng/mL (IQR 256.0–1367.8) to 387.6 ng/mL (IQR 201.0–899.6); p = 0.002), TNFR1 (from 936.7 pg/mL (IQR 721.3–1138.8) to 876.6 pg/mL (IQR 669.1–1067.0); p < 0.001), and TNFR2 (from 3646.1 pg/mL (IQR 3057.3–4509.1) to 3257.9 pg/mL (IQR 2879.3–3970.3); p < 0.001). The PRGN levels were also decreased, whereas the NGAL levels were significantly increased. The suPAR levels were not changed. Urinary NGAL was measured as a tubular damage marker, and urinary 8-OHdG levels were measured as an oxidative stress marker at baseline and 4 months. No significant changes were found in the patients’ urinary NGAL levels throughout the observation period. We observed a significant increase in the urinary excretion of Col4 and 8-OHdG after 4 months of treatment with SGLT2i.
Changes in Laboratory Data Stratified by Albuminuria Status
When participants were stratified into three groups by the albuminuria status at baseline (Table S1), the uACR (log) levels were significantly reduced in patients with microalbuminuria from 4.4 (IQR 3.8–5.0) to 3.7 (IQR 3.2–5.2) 4 months after the initiation of SGLT2i (p = 0.006). In patients with macroalbuminuria, the uACR (log) levels tended to decrease from 6.6 (IQR 6.3–7.4) to 6.5 (IQR 5.7–7.2) 4 months after the initiation of SGLT2i (p = 0.094). No significant change was observed in the uACR (log) levels in the patients with normoalbuminuria. After the initiation of SGLT2i, the levels of serum TNFR1 and TNFR2 were significantly decreased from 1105.3 pg/mL (SD 548.3) to 1020.0 pg/mL (SD 487.0) and from 3810.6 pg/mL (IQR 3264.5–4566.9) to 3287.2 pg/mL (IQR 2909.9–4159.2), p < 0.05, and p < 0.001, respectively (Table S2) in the microalbuminuria subgroup.
Association Changes in uACR (log) with Those of Other Parameters
The single linear regression analysis showed a significant correlation between the changes in uACR (log) and those in Nt-proBMP (r = 0.218, p = 0.016), TNFR1 (r = 0.244, p = 0.007), and urinary Col4 (r = 0.271, p = 0.002; Table 4 and Fig. 1). In contrast, the single linear regression analysis did not show a significant correlation between the changes in uACR (log) and those in BMI, SBP, DBP, PP, Hct, HbA1c, eGFRcys, UA, AST, ALT, γ-GTP, LDL-C, TG, HDL-C, Epo, CRP (log), TNFR2, PGRN, NGAL, and urinary 8-OHdG. After all the relevant variables in the multivariate regression model were adjusted for, changes in TNFR1 were significantly associated with those in uACR (log) (independent t = 2.102, p < 0.05; Table 5). These variables were selected on the basis of well-known risk factors for chronic kidney disease. In patients with microalbuminuria, the changes in uACR (log) were positively correlated with the changes in TNFR1 (r = 0.483, p = 0.003) or TNFR2 (r = 0.346, p = 0.039; Table S2). Furthermore, the changes in uACR (log) were inversely correlated with those in eGFRcys in patients with microalbuminuria (r = − 0.449, p = 0.006; Table S2).

Correlation between the changes in log-transformed uACR and those in serum a Nt-proBNP, b TNFR1, or c uCol4. The correlation coefficient, regression equation, and p values are shown at the bottom of each panel. uACR (log) log-transformed urine albumin-to-creatinine ratio, NT-proBNP N-terminal pro-brain natriuretic peptide, TNFR1 tumor necrosis factor receptor 1, uCol4 urine type IV collagen
Associations of Changes in uACR (log) with Baseline Parameters
There was a positive linear association between the change in uACR (log) and the baseline levels of SBP (r = 0.179, p < 0.05). In contrast, there was an inverse linear association between the change in uACR (log) and the baseline levels of uACR (log) or urinary NGAL (r = − 0.254, p < 0.01; r = − 0.226, p < 0.05, respectively; Table S3). After all the relevant variables in the multivariate regression model were adjusted for, the baseline levels of SBP or uACR (log) were significantly associated with the change in uACR (log) (independent t = 2.314, p < 0.05; independent t = − 3.616, p < 0.001; Table S4).
Associations of Changes in TNFR1 with Those of Other Parameters
The changes in TNFR1 were significantly correlated with those in eGFRcys, ALT, CRP (log), TNFR2, PGRN, and uACR (log) according to the single linear correlation analysis (r = − 0.311, p < 0.001; r = 0.220, p = 0.014; r = 0.432, p < 0.001; r = 0.620, p < 0.001; r = 0.352, p < 0.001; and r = 0.244, p = 0.007, respectively; Table S5 and Fig. S1), and the association of changes in eGFRcys, CRP(log), TNFR2, PGRN, and uACR (log) with TNFR1 was maintained using multiple regression analysis (Table S6).
Associations of Changes in Urinary 8-Hydroxy-2′-deoxyguanosine (8–8-OHdG) with Those of Other Parameters
The reticulocyte count was significantly reduced from 1.4% (IQR 1.1–1.7) to 1.2% (IQR 1.0–1.6) 4 months after the initiation of SGLT2 treatment (Fig. S2a), and the changes in u8-8-OHdG were inversely correlated with those in the reticulocytes (r = − 0.191, p = 0.041; Fig. S2b).
Discussion
The decision to focus on the reduction in albuminuria during the early stages of treatment with SGLT2i as the primary endpoint in our study can be attributed to several reasons. This approach aligns with findings from Oshima et al.’s study that highlighted the independent association between early changes in albuminuria (from baseline to week 26) and long-term kidney and cardiovascular outcomes [15]. Therefore, assessing the early response to SGLT2i treatment by examining albuminuria reduction is a relevant and clinically significant parameter. Moreover, the rationale behind conducting a short-term, single-arm observational pilot study lies in the exploratory nature of our research. Several clinical trials have previously demonstrated the proteinuria-reducing effects of SGLT2i in individuals with diabetic kidney disease [13]. However, there remains a need to better understand the factors associated with the early response to SGLT2i treatment, as well as to identify potential predictors of treatment success. By focusing on the short-term impact of SGLT2i treatment in a single-arm observational pilot study, we aimed to gather preliminary data on the factors influencing early albuminuria reduction. This initial investigation can serve as a foundation for future research, potentially guiding the design of larger, controlled trials that explore the long-term effects of SGLT2i treatment and its impact on kidney and cardiovascular outcomes in a more comprehensive manner.
This study showed that a 4-month administration of SGLT2i significantly reduced urinary albumin excretion in Japanese patients with T2DM. In contrast, tubular damage markers remained unchanged over the 4-month follow-up period. Furthermore, important renal risk factors, including hyperglycemia, obesity, hypertension, and hyperuricemia, were reduced by SGLT2i. However, the albuminuria-reducing effects were not associated with these improvements. This suggests that the mechanism of reducing albuminuria by SGLT2i extends beyond its glucose-, weight-, and blood pressure-lowering effects. In addition, this effect on albuminuria was independent of age, sex, body weight, renal function, and the presence or absence of renin–angiotensin inhibitors at the start of SGLT2i administration. SGLT2i appear to possess a proteinuria-reducing effect in T2DM, primarily due to their inhibitory effects on inflammation. However, the reduction in the levels of renal oxidative stress markers did not correlate with the proteinuria-reducing effect.
Consistent with the results of previous non-Japanese studies [35,36,37], the changes in HbA1c level, blood pressure, and body weight did not correlate with the changes in uACR (log) after 4 months of SGLT2i administration. Therefore, it may be reasonable to speculate that the reduction in albuminuria was strongly affected by factors other than the glucose-, weight-, and blood pressure-lowering effects of SGLT2i.
Previous meta-analyses have demonstrated that SGLT2i significantly altered some circulating inflammation-related biomarkers [38,39,40]. However, remedies that modulate TNFR levels remain to be fully elucidated. Baricitinib, a Janus kinase 1/2 inhibitor, is the only other agent shown to lower TNFR levels in patients with T2DM and chronic kidney disease [39]. In contrast, resin–angiotensin system inhibitor treatment did not alter the TNFR levels in patients with early DKD [27, 28, 41]. Although a previous study examining SGLT2i canagliflozin demonstrated slight attenuation of the increase in TNFR1 level [28], this study showed that SGLT2i significantly decreased the serum CRP, TNFR1, TNFR2, and PGRN levels after 4 months of treatment with SGLT2i. Previous studies [42] support a potential role for SGLT2i in attenuating inflammatory processes in individuals with T2DM. The changes in serum CRP (log) did not correlate with the changes in uACR (log), possibly because the serum CRP level reflects the presence of inflammation not only in the kidneys but also in the systemic circulation. In patients with normoalbuminuria, no significant change was observed in the uACR (log) levels. In the microalbuminuria subgroup, the changes in uACR were well correlated with the changes in TNFR2 as well as TNFR1. Purohit et al. reported that TNFRs may play an important role in the development of microalbuminuria in type 1 diabetes [43]. SGLT2i may exert an anti-inflammatory effect in the patients with T2DM at any stage, and the reduction in proteinuria was dependent on the inhibitory effects of inflammation after the onset of microalbuminuria.
We observed that the eGFRcys of patients decreased at 4 months compared to that at baseline. This phenomenon may reflect the early eGFR decline and eGFR dip observed in several randomized trials of SGLT2i [44]. SGLT2i are believed to exert renoprotective effects through enhanced tubuloglomerular feedback, resulting in decreased hyperfiltration and albuminuria [45]. However, in this study, eGFRcys showed a decrease after 4 months of SGLT2i treatment, whereas the changes in eGFRcys were not associated with the changes in uACR (log). This suggests that the improvement in inflammation contributes to the reduction of albuminuria more than that of intraglomerular hemodynamics by SGLT2i.
Increased oxidative stress generation may play an essential role in the functional and structural changes in the kidneys of patients with diabetes [46]. A high glucose exposure significantly increased the oxidative stress in the proximal tubular cells of humans, which was inhibited by treatment with SGLT2i tofogliflozin [47]. SGLT2i reduced the oxidative stress and reversed the endothelial dysfunction in type 2 diabetic mice [48]. The above findings were mainly obtained from basic research, and not many studies show that SGLT2i reduces oxidative stress, which relates to a decrease in urinary albumin excretion. In this study, urinary levels of 8-OHdG increased after treatment with SGLT2i. However, we did not observe any association between the changes in the uACR (log) and 8-OHdG levels. A previous study reported that iron utilization for erythropoiesis contributes to a reduction in iron-induced oxidative stress [49]. However, the present study revealed that the reticulocyte count was significantly reduced 4 months after the initiation of SGLT2 and that the changes in u8-OHdG were inversely correlated with the changes in the reticulocytes. The aforementioned findings suggest the possible involvement of reduced erythropoiesis in SGLT2i-mediated increase in u8-OHdG.
The changes in uACR (log) were significantly correlated with the changes in the serum Nt-proBNP levels. Previous studies have demonstrated that the biomarkers of renal disease progression, such as TNFR1, also predict composite heart failure outcomes [50]. This suggests the possibility that common mechanisms exist for renal injuries and cardiovascular dysfunction.
The renoprotective effect of the SGLT2i empagliflozin was more pronounced in patients with macroalbuminuria at the beginning of the study [11]. The results from that study similarly showed an association between the higher uACR value at baseline and the greater reduction in the urinary albumin excretion rate by SGLT2i, which is also supported by the present study.
This study has several important limitations that should be acknowledged. Firstly, the use of multiple SGLT2i without specification of the agents employed introduces variability due to the differing effects of medications, thereby potentially impacting the results. Secondly, the absence of a control group hinders the ability to compare outcomes with those of individuals not receiving SGLT2i, thereby complicating the determination of treatment-specific effects. Furthermore, the blood glucose levels were not analyzed because the preprandial and postprandial blood samples were pooled. Additionally, excluding patients who discontinued treatment with SGLT2i may have led to overestimation of the treatment effect due to lack of response to the drug. Lastly, the relatively short follow-up period of 4 months may have restricted the evaluation of long-term and side effects of the treatment. Recognizing these limitations and providing suggestions for future research and study design improvements is crucial for accurate interpretation of study outcomes, while offering a balanced assessment.
Conclusion
This study may provide the first evidence which supports the finding that reductions in serum TNFR1 levels are independently associated with a degree of albuminuria reduction in patients with T2DM after treatment with SGLT2i. Although the inflammation-reducing and renoprotective mechanisms of SGLT2i have not yet been fully clarified, this study provides novel evidence regarding the mechanism. This research would also significantly contribute to the development of anti-inflammatory agents for metabolic diseases, including T2DM.
Data Availability
The datasets generated and analyzed during the current study are not publicly available due to the principle of confidentiality of patient information.
References
Eder S, Leierer J, Kerschbaum J, et al. A prospective cohort study in patients with type 2 diabetes mellitus for validation of biomarkers (PROVALID)—study design and baseline characteristics. Kidney Blood Press Res. 2018;43:181–90.
Afkarian M, Zelnick LR, Hall YN, et al. Clinical manifestations of kidney disease among US adults with diabetes, 1988–2014. JAMA. 2016;316:602–10.
Katayama S, Moriya T, Tanaka S, et al. Low transition rate from normo- and low microalbuminuria to proteinuria in Japanese type 2 diabetic individuals: The Japan Diabetes Complications Study (JDCS). Diabetologia. 2011;54:1025–31.
Ninomiya T, Perkovic V, de Galan BE, et al. Albuminuria and kidney function independently predict cardiovascular and renal outcomes in diabetes. J Am Soc Nephrol. 2009;20:1813–21.
de Zeeuw D, Remuzzi G, Parving HH, et al. Albuminuria, a therapeutic target for cardiovascular protection in type 2 diabetic patients with nephropathy. Circulation. 2004;110:921–7.
Rawshani A, Rawshani A, Franzén S, et al. Risk factors, mortality, and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2018;379:633–44.
Kimura K. Preface: Evidence-based clinical practice guidelines for CKD: An abridged English version. Clin Exp Nephrol. 2014;18:339–40.
American Diabetes Association. 3. Comprehensive medical evaluation and assessment of comorbidities: standards of medical care in Diabetes–2018. Diabetes Care. 2018; 41(Suppl 1):S28–S37.
Gaede P, Lund-Andersen H, Parving HH, et al. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008;358:580–91.
Neal B, Perkovic V, Matthews DR. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377:2099.
Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375:323–34.
Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380:347–57.
Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380:2295–306.
Waijer SW, Xie D, Inzucchi SE, et al. Short-term changes in albuminuria and risk of cardiovascular and renal outcomes in type 2 diabetes mellitus: a post-hoc analysis of the EMPA-REG OUTCOME trial. J Am Heart Assoc. 2020;9: e016976.
Oshima M, Neuen BL, Li J, et al. Early change in albuminuria with canagliflozin predicts kidney and cardiovascular outcomes: a PostHoc analysis from the CREDENCE trial. J Am Soc Nephrol. 2020;31:2925–36.
Gembardt F, Bartaun C, Jarzebska N, et al. The SGLT2 inhibitor empagliflozin ameliorates early features of diabetic nephropathy in BTBR ob/ob type 2 diabetic mice with and without hypertension. Am J Physiol Renal Physiol. 2014;307:F317–25.
Vallon V. The mechanisms and therapeutic potential of SGLT2 inhibitors in diabetes mellitus. Annu Rev Med. 2015;66:255–70.
Vallon V, Gerasimova M, Rose MA, et al. SGLT2 inhibitor empagliflozin reduces renal growth and albuminuria in proportion to hyperglycemia and prevents glomerular hyperfiltration in diabetic Akita mice. Am J Physiol Renal Physiol. 2014;306:F194-204.
Caramori ML, Mauer M. Diabetes and nephropathy. Curr Opin Nephrol Hypertens. 2003;12:273–82.
Mora C, Navarro JF. Inflammation and diabetic nephropathy. Curr Diab Rep. 2006;6:463–8.
Ramseyer VD, Garvin JL. Tumor necrosis factor-α: regulation of renal function and blood pressure. Am J Physiol Renal Physiol. 2013;304:F1231–42.
Speeckaert MM, Speeckaert R, Laute M, et al. Tumor necrosis factor receptors: biology and therapeutic potential in kidney diseases. Am J Nephrol. 2012;36:261–70.
Tang W, Lu Y, Tian QY, et al. The growth factor progranulin binds to TNF receptors and is therapeutic against inflammatory arthritis in mice. Science. 2011;332:478–84.
Wu TH, Chang LH, Chu CH, et al. Soluble tumor necrosis factor receptor 2 is associated with progressive diabetic kidney disease in patients with type 2 diabetes mellitus. PLoS ONE. 2022;17:e0266854.
Nicoletto BB, Krolikowski TC, Crispim D, et al. Serum and urinary progranulin in diabetic kidney disease. PLoS ONE. 2016;11:e0165177.
Zhou Y, Ren J, Li P, et al. Expression of urokinase-type plasminogen activator receptor and its soluble form in type 2 diabetic kidney disease. Arch Med Res. 2019;50:249–56.
Niewczas MA, Pavkov ME, Skupien J, et al. A signature of circulating inflammatory proteins and development of end-stage renal disease in diabetes. Nat Med. 2019;25:805–13.
Heerspink HJL, Perco P, Mulder S, et al. Canagliflozin reduces inflammation and fibrosis biomarkers: a potential mechanism of action for beneficial effects of SGLT2 inhibitors in diabetic kidney disease. Diabetologia. 2019;62:1154–66.
Thomas MC, Burns WC, Cooper ME. Tubular changes in early diabetic nephropathy. Adv Chronic Kidney Dis. 2005;12:177–86.
Tang SC, Lai KN. The pathogenic role of the renal proximal tubular cell in diabetic nephropathy. Nephrol Dial Transplant. 2012;27:3049–56.
Kamijo-Ikemori A, Sugaya T, Yasuda T, et al. Clinical significance of urinary liver-type fatty acid-binding protein in diabetic nephropathy of type 2 diabetic patients. Diabetes Care. 2011;34:691–6.
Committee of the Japan Diabetes Society on the Diagnostic Criteria of Diabetes Mellitus, Seino Y, Nanjo K et al. Report of the committee on the classification and diagnostic criteria of diabetes mellitus. J Diabetes Investig. 2010;1:212–28.
Matsuo S, Imai E, Horio M, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Horio M, Imai E, Yasuda Y, et al. GFR estimation using standardized serum cystatin C in Japan. Am J Kidney Dis. 2013;61:197–203.
Heerspink HJ, Johnsson E, Gause-Nilsson I, et al. Dapagliflozin reduces albuminuria in patients with diabetes and hypertension receiving renin–angiotensin blockers. Diabetes Obes Metab. 2016;18:590–7.
Petrykiv SI, Laverman GD, de Zeeuw D, et al. The albuminuria-lowering response to dapagliflozin is variable and reproducible among individual patients. Diabetes Obes Metab. 2017;19:1363–70.
Cherney D, Lund SS, Perkins BA, et al. The effect of sodium glucose cotransporter 2 inhibition with empagliflozin on microalbuminuria and macroalbuminuria in patients with type 2 diabetes. Diabetologia. 2016;59:1860–70.
Wang D, Liu J, Zhong L, et al. The effect of sodium-glucose cotransporter 2 inhibitors on biomarkers of inflammation: a systematic review and meta-analysis of randomized controlled trials. Front Pharmacol. 2022;13:1045235.
Theofilis P, Sagris M, Oikonomou E, et al. The impact of SGLT2 inhibitors on inflammation: a systematic review and meta-analysis of studies in rodents. Int Immunopharmacol. 2022;111:109080.
Cao Y, Liang N, Liu T, et al. Effect of SGLT2 inhibitors and metformin on inflammatory and prognostic biomarkers in type 2 diabetes patients. Endocr Metab Immune Disord Drug Targets. 2023;23:530–47.
Tuttle KR, Brosius FC 3rd, Adler SG, et al. JAK1/JAK2 inhibition by baricitinib in diabetic kidney disease: results from a phase 2 randomized controlled clinical trial. Nephrol Dial Transplant. 2018;33:1950–9.
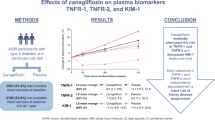
Sen T, Li J, Neuen BL, et al. Effects of the SGLT2 inhibitor canagliflozin on plasma biomarkers TNFR-1, TNFR-2 and KIM-1 in the CANVAS trial. Diabetologia. 2021;64:2147–58.
Purohit S, Sharma A, Zhi W, et al. Proteins of TNF-α and IL6 pathways are elevated in serum of type-1 diabetes patients with microalbuminuria. Front Immunol. 2018;9:154.
De Nicola L, Gabbai FB, Garofalo C, et al. Nephroprotection by SGLT2 inhibition: back to the future? J Clin Med. 2020;9:2243.
Cherney DZ, Perkins BA, Soleymanlou N, et al. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patients with type 1 diabetes mellitus. Circulation. 2014;129:587–97.
Yamagishi S, Matsui T. Advanced glycation end products, oxidative stress and diabetic nephropathy. Oxid Med Cell Longev. 2010;3:101–8.
Ishibashi Y, Matsui T, Yamagishi S. Tofogliflozin, a highly selective inhibitor of SGLT2 blocks proinflammatory and proapoptotic effects of glucose overload on proximal tubular cells partly by suppressing oxidative stress generation. Horm Metab Res. 2016;48:191–5.
Kamezaki M, Kusaba T, Komaki K, et al. Comprehensive renoprotective effects of ipragliflozin on early diabetic nephropathy in mice. Sci Rep. 2018;8:4029.
Noguchi-Sasaki M, Sasaki Y, Matsuo-Tezuka Y, et al. Reduction of a marker of oxidative stress with enhancement of iron utilization by erythropoiesis activation following epoetin beta pegol administration in iron-loaded db/db mice. Int J Hematol. 2016;103:262–73.
Tye SC, Jongs N, Coca SG, et al. Initiation of the SGLT2 inhibitor canagliflozin to prevent kidney and heart failure outcomes guided by HbA1c, albuminuria, and predicted risk of kidney failure. Cardiovasc Diabetol. 2022;21:194.
Acknowledgements
The authors are grateful to the clinical staff for their assistance in the execution of the study and would also like to thank all the study participants.
Medical Writing/Editorial Assistance
Medical writing support in the preparation of this article was provided by Editage (www.editage.com), and funded by the authors.
Funding
This work was supported by the Japan Society for the Promotion of Science KAKENHI (Grant no. 18K16204 to TO). The Rapid Service Fee was funded by the authors.
Author information
Authors and Affiliations
Contributions
This study was designed by Toshiki Otada. Formal analysis was performed by Toshiki Otada, Akiko Sekine, and Ryoko Uemoto. Data collection was performed by Toshiki Otada, Seijiro Tsuji, Tomoyo Hara, Motoyuki Tamaki, Tomoyuki Yuasa, Toshiaki Tamaki, and Ken-ichi Aihara. Data resource management and data curation were performed by Toshiki Otada, Akiko Sekine, Ryoko Uemoto, Motoyuki Tamaki, Toshiaki Tamaki, and Ken-ichi Aihara. The results of the analysis were validated by Toshiki Otada, Tomoyuki Yuasa, and Kenichi Aihara. The first draft of the manuscript was written by Toshiki Otada, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
Toshiki Otoda received lecture fees from Taisho Pharmaceutical Holdings Co., Ltd. and Kowa Company, Ltd. and received speaker fees from Astellas Pharma, Inc., Nippon Boehringer Ingelheim Co., Ltd., and Mitsubishi Tanabe Pharma Corporation. Motoyuki Tamaki received speaker fees from Eli Lilly Japan K.K. Tomoyuki Yuasa received speaker fees from Eli Lilly Japan K.K., Nippon Boehringer Ingelheim Co., Ltd., and Mitsubishi Tanabe Pharma Corporation. Toshiaki Tamaki received speaker fees from Astellas Pharma, Inc., Ono Pharmaceutical Co., Ltd., and Mitsubishi Tanabe Pharma Corporation. Munehide Matsuhisa received speaker fees from Nippon Boehringer Ingelheim Co., Ltd., Eli Lilly Japan K.K., Novo Nordisk Pharma Ltd., Sumitomo Pharma Co., Ltd., Sanofi K.K., and Kyowa Kirin Co., Ltd. Akiko Sekine, Ryoko Uemoto, Seijiro Tsuji, Tomoyo Hara, and Ken-ichi Aihara declare that they have no conflicts of interest to disclose.
Ethical Approval
This study complied with the Declaration of Helsinki and Good Clinical Practice guidelines and was conducted as a collaborative multicenter research effort led by Tokushima University. To ensure comprehensive ethical approval across all participating facilities, each institution sought a consolidated review by the Institutional Review Board of Tokushima University Hospital. Subsequently, the Institutional Review Board of Tokushima University Hospital granted approval for all study sites involved in this multicenter study (approval date April 23, 2018; approval ID 3149). The research proceeded after securing the necessary approvals from each research institution. Additional matters requiring approval, such as protocol amendments, were evaluated and approved by the institutional review boards on the basis of need. The trial was registered with the University Hospital Medical Information Network (UMIN No. 000031947). The patients were provided with detailed explanations of the study protocol. All participants provided written informed consent for participation in the study and for publication of the study results. Nonetheless, all patient records and information were anonymized before the analysis.
Additional information
Prior Presentation: This manuscript is based on work that has previously been presented at the 66th Annual Meeting of the Japan Diabetes Society, 12–14 May 2022, in Kobe, Japan, in the form of an oral presentation (Abstract II-80–2).
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Otoda, T., Sekine, A., Uemoto, R. et al. Albuminuria and Serum Tumor Necrosis Factor Receptor Levels in Patients with Type 2 Diabetes on SGLT2 Inhibitors: A Prospective Study. Diabetes Ther 15, 127–143 (2024). https://doi.org/10.1007/s13300-023-01488-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-023-01488-0