
Abstract
Background and Aims
Type 2 diabetes is one of the leading causes of the development and progression of diabetic kidney disease, culminating in end-stage renal disease. Approximately two decades after successful implementation of the renin–angiotensin–aldosterone blocking system, three classes of agents [sodium glucose cotransporter 2 inhibitors (SGLT-2i), glucagon-like peptide 1 receptor agonists, and nonsteroidal mineralocorticoid receptor antagonists] have shown significant potential to confer renoprotection. This network meta-analysis was undertaken to construct a hierarchy based on indirect pairwise comparisons and rankings among and within these three classes of molecules.
Methods
A Cochrane library-based web search yielded 16 randomized controlled trials for analysis. Stata/BE 17.0 and RStudio 2022.07.1 Build 554 software were used to conduct a frequentist network meta-analysis. The effect size was assessed based on the odds ratio, and the MDS (multidimensional scaling) rank system was used to identify a hierarchy among reno-protective molecules.
Results
Regarding the overall data, the SGLT-2i group of agents ranked higher than the other groups in preventing the progression of renal composite events in patients with T2D. Dapagliflozin ranked the highest among individual molecules.
Conclusions
The SGLT-2i group of agents, especially dapagliflozin, is best suited to complement metabolic control in preventing the progression of renal composite outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this network meta-analysis? |
The management of type 2 diabetes (T2D) has grown beyond metabolic control with organ protective molecules taking the center stage. |
As far as renoprotection is concerned, three groups of drugs (SGLT-2i, GLP1-RA, and MRA) have emerged as recent candidates to complement metabolic control and renin–angiotensin–aldosterone system blockade. |
Although the reno-protective groups have been specified by most guidelines, the choice of agent from within each of these groups remains unexplored. |
What was learned from this study? |
SGLT-2i ranked the highest in terms of choosing between the three reno-protective groups in the backdrop of T2D. |
Regarding individual agents, dapagliflozin scored the highest in the SGLT-2i group and efpeglinatide scored highest in the GLP1-RA group. |
Introduction
Type 2 diabetes (T2D) is one of the leading causes of the development and progression of diabetic kidney disease (DKD), culminating in end-stage renal disease. Approximately 40% of patients with T2D are projected to develop DKD [1]. With the exponential increase in the prevalence of T2D globally, the absolute numbers of T2D patients with DKD are expected to reach alarming proportions [2]. Traditionally, prevention of the development of or progression to diabetic nephropathy is achieved with good metabolic control [3]. Early structural and hemodynamic insults at the level of the glomerulus, as well tubulointerstitial architectural alterations, pave the way for progressive renal insult [4]. Evidence indicating that hemodynamic and structural damage occur even in the absence of metabolic insult underscores the urgent need to search for molecules that specifically target these newly identified pathophysiological defects [5]. Approximately two decades after the success of the renin–angiotensin–aldosterone blocking system (RAASB), two classes of antihyperglycemic agents [sodium glucose cotransporter 2 inhibitors (SGLT-2i) and glucagon-like peptide 1 receptor agonists (GLP1-RA)] have been developed that deliver significant renoprotection in addition to their metabolic benefits [6]. Another group of drugs [nonsteroidal mineralocorticoid receptor antagonists MRA]) was recently identified as delivering renoprotection to patients with T2D [7]. In the absence of head-to-head comparisons among these three classes of molecules, practicing physicians must often make a call based on guidance from consensus statements or by constructing an indirect hierarchy from the available evidence.
This network meta-analysis was undertaken to construct a hierarchy based on an indirect pairwise comparison and ranking among the three classes of molecules. The following question was explored in this analysis: in addition to good metabolic control and RAASB, which molecule should be administered to a patient with T2D to effectively prevent the development or progression of renal composite events?
The meta-analysis was designed following the PICO question format, as follows:
- P (Patient population::
-
patients diagnosed with T2D.
- I (Intervention)::
-
received drugs belonging to the GLP1-RA, SGLT-2i or MRA groups.
- C (Control group)::
-
compared to placebo.
- O (Outcome)::
-
the primary aim was to analyze whether there is a hierarchical choice when selecting one of the agents from the intervention arm (I) based on progression of renal composite events.
Methods
This review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [8]. This analysis consisted of data which were previously published. No authors were involved in carry out experiment on animals or human beings. Therefore, an ethical or board review approval was not required for this analysis.
Search Strategy and Eligibility Criteria
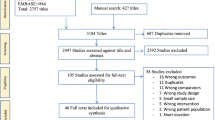
An electronic database search was conducted using the Cochrane library without any limitations on date or language. The major search headings included “type 2 diabetes,” “renal composite,” “diabetic kidney disease,” “sodium glucose cotransporter 2 inhibitors,” “glucagon-like peptide 1 receptor agonists,” and “nonsteroidal mineralocorticoid receptor antagonists.” The full search strategy is detailed in Fig. 1 and in Supplementary Electronic Material (ESM) Text S1.

Flow chart of study selection for inclusion in the meta-analysis
Study Selection and Eligibility Criteria
Citations identified by the preliminary web search were manually reviewed by the authors based on the PICO search criteria as well as prespecified eligibility criteria. The key eligibility criteria for positive selection included: (1) patients with T2D; (2) age of patient ≥ 18 years; (3) randomized controlled trials (RCTs) with placebo as the comparator arm; and (4) studies clearly mentioning the primary outcomes of interest that conformed to our intervention requirements (primary renal composite outcome).
Risk of Bias
The Cochrane Collaboration Risk of Bias 2.0 algorithm was used to assess and report the bias associated with the individual studies, as shown in ESM Figure S1. The citations were circulated among the authors, and any dispute was resolved with consensus. Publication bias was assessed qualitatively using a funnel plot and quantitatively using Peter’s method, as shown in ESM Figure S2).
Statistical Analysis
Two software programs were used to perform the analysis and prepare the graphical data. RStudio 2022.07.1 Build 554 software was used to assess the risk of bias. Stata/BE 17.0 software (StataCorp, College Station, TX, USA) was used to perform the pairwise meta-analysis. Ranking by multidimensional scaling (MDS) was also performed with Stata software. Based on a priori power calculations assuming a minimal difference in effect size of 10% from at least ten studies with 5000 participants in each arm, an alpha of 0.05, and a moderate degree of heterogeneity, the estimated power of this meta-analysis was 100% [ESM Figure S3].
The planned statistical analysis included the following steps:
-
1.
Creating a frequentist network for indirect pairwise comparison. Given that no direct comparisons were performed between the interventions, a network loop could not be formed. Taking into consideration that the point estimates of a pairwise forest plot is proportional to the inverse square of the standard error, the confidence interval is expected to be wider. Hence, we could not derive inferences based on the findings of the pairwise forest plot.
-
2.
The principal goal of this analysis was to create a rank score to establish hierarchical decision-making. This goal was accomplished by creating a frequentist network utilizing the MDS ranking. Initial ranking involves the groups of agents (GLP1-RA, SGLT-2i, and MRA). Subsequently, we split the SGLT-2is group into its respective molecules and reanalyzed the ranking data. The STATA coding is provided in ESM Text S2.
Results
Baseline Characteristics and Risk of Bias
An electronic web search yielded 17 citations/studies that were included in the network meta-analysis [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25]. Of these 17 studies, ten were RCTs that included an SGLT-2i as the intervention arm (n = 30,314 participants) compared to placebo (n = 26,525 participants), two were RCTs comparing finerenone (n = 6519) to placebo (n = 6507), and five were RCTs comparing GLP1-RA (n = 20,238) to placebo (n = 18,854). A total of 108,957 patients were included in this meta-analysis, of whom 57,071 were enrolled in the intervention arm and 51,886 were enrolled in the placebo arm. [ESM Table S1] The mean age of the participants in each study ranged between 63 and 72 years, ignoring the standard difference. There were significant differences in the way the renal composite was defined. Regarding the target estimated glomerular filtration rate (eGFR) component of renal composite events, nine RCTs reported a sustained reduction of ≥ 40% from baseline (EMPA KIDNEY [9], EMPEROR PRESERVED [11] and REDUCED [12], DECLARE TIMI-58 [13], CANVAS [17], FIDELIO-DKD [19], FIGARO-DKD [20], EXSCEL [21], and AMPLITUDE-O [22]), three RCTs reported a ≥ 50% reduction from baseline (DAPA HF [14], DELIVER [15], DAPA CKD [16]), four RCTs (EMPA REG [10], CREDENCE [18], LEADER [23], and SUSTAIN-6 [25]) reported a doubling of serum creatinine levels, and one RCT (REWIND [24]) reported a sustained ≥ 30% reduction from baseline. There was heterogeneity in defining significant albuminuria, with > 200 mg/g and > 300 mg/g representing the two most common definitions. Using > 200 mg/g as the cutoff value for significant baseline albuminuria, six RCTs satisfied the baseline criteria (EMPA KIDNEY, DAPA HF, DAPA CKD, CREDENCE, FIDELIO-DKD, and FIGARO-DKD), whereas seven did not (EMPEROR PRESERVED & REDUCED, CANVAS, EXSCEL, AMPLITUDE-O, REWIND, and SUSTAIN-6). The remaining studies exhibited mixed results (EMPA REG, DECLARE TIMI-58, and LEADER). The mean baseline eGFR ranged from 37.4 to 85.4 ml/min, not taking into account the associated standard deviations. Five RCTs (EMPA KIDNEY, EMPEROR PRESERVED, DAPA CKD, CREDENCE, and FIDELIO-DKD) recruited patients with an eGFR < 60 ml/min, and 11 RCTs (EMPEROR REDUCED, CANVAS, DECLARE TIMI-58, DAPA HF, DELIVER, FIGARO-DKD, EXSCEL, AMPLITUDE-O, LEADER, REWIND, and SUSTAIN-6) recruited patients with an eGFR ≥ 60 ml/min. Approximately 71–99.9% of patients were on some form of RAASB.
The risk of bias associated with individual studies was ascertained using the Cochrane risk-of-bias algorithm. Some concerns related to deviations from intended interventions, missing data, and critical concerns related to the selection of the reported results were noted for the DECLARE TIMI-58 RCT. These observations were related to the way the additional > 5000 patients with increased cardiovascular risk were handled in the latter half of the trial. There were some concerns related to outcome reported and selection of reported results observed in two RCTs (CANVAS and SUSTAIN-6). Publication bias was assessed using a funnel plot. In view of the fact that log(OR) was used as the measuring index, Peter’s test was conducted to detect any asymmetry of data distribution.
Pairwise Meta-analysis
Given the absence of a direct comparison between the interventions, no loop was formed in the network plot. (Fig. 2).

Network plots of groups of interventions (a) and individual agents (b). Empa empagliflozin, Cana canagliflozin, Dapa dapagliflozin, Dula dulaglutide, Efpe efpeglenatide, Exe exenatide-LAR, Fin Finerenone, Flozin Sodium glucose co-transporter-2 inhibitors, GLP1RA glucagon-like peptide 1 receptor agonist, Lira liraglutide, Sema semaglutide
Comparison Between Individual Groups
Compared with placebo, all three groups of agents conferred significant benefits in terms of reducing the renal composite. However, the prediction interval indicated greater generalizability of the outcomes benefit with SGLT-2i [95% prediction interval (PI) 0.51–0.84] in comparison to the other two groups. Indirect comparisons among the groups tended to favor SGLT-2i over MRA (27% greater mean reduction), whereas the other comparisons yielded neutral results (Fig. 3).

Comparisons among individual groups of agents. a Forest plot of direct and indirect pairwise comparison, b multidimensional scaling. CI confidence interval, PrI prediction interval, SGLT1i Sodium glucose cotransporter 2 inhibitor
The MDS ranking results indicated that SGLT-2i occupied the first position followed by GLP1-RA and MRA (Fig. 3).
Comparisons Among Individual Molecules
Compared with placebo, all molecules with the exception of exenatide-LAR and dulaglutide demonstrated significant benefits in preventing the progression of renal composite events. However, when comparing the prediction intervals, the benefits were more generalizable in the dapagliflozin (95% PI 0.45–0.83) arm in comparison to the empagliflozin (95% PI 0.52–0.93), canagliflozin (95% PI 0.51–0.95), efpeglenatide (95% PI 0.47–0.94), liraglutide (95% PI 0.56–1.10), dulaglutide (95% PI 0.63–1.15), semaglutide (95% PI 0.37–0.98), and finerenone (PI 0.64–01.09) arms (Fig. 4).

Comparisons among individual agents. a Forest plot of direct and indirect pairwise comparisons, b multidimensional scaling rank scores
In indirect comparisons, dapagliflozin was better than finerenone (36% greater mean reduction), exenatide-LAR (44% greater mean reduction), and dulaglutide (38% greater mean reduction). All other indirect comparisons between the individual molecules were comparable.
The MDS ranking results revealed that dapagliflozin occupied the first position followed by empagliflozin and canagliflozin (Fig. 4). Epfeglenatide ranked fourth followed by semaglutide. Finerenone occupied the seventh spot.
Discussion
The management of DKD has been enhanced by the addition of reno-protective agents complimenting metabolic control. With the identification of non-proteinuric pathways contributing to a decline in eGFR culminating in end-stage renal disease, it is extremely important to assess both urinary albumin excretion as well as eGFR decline simultaneously [26]. This is exactly why a decline in eGFR is an integral component of the renal composite outcome, which may variably include the urine albumin-creatinine ratio (UACR), renal replacement therapy, or renal death as additional components. The recent American Diabetes Association and Kidney Disease: Improving Global Outcomes (ADA/KDIGO) consensus statement positions these reno-protective agents ahead of the traditional molecules, which can be added later to achieve good metabolic control [27]. The three groups of agents conferring renoprotective effects in addition to good metabolic control and background use of RAASB include SGLT-2i, GLP1-RA, and MRA. In the absence of direct head-to-head comparisons among molecules within individual groups, physicians often face a dilemma when selecting among these agents. Most of the consensus statements leave this aspect open to the physicians who are free to choose among these agents.
Literature Review
In total, nine RCTs with SGLT-2i included in this review reported renal composite outcome as one of the endpoints. Four of these nine RCTs reported the renal composite outcome either as part of the primary endpoint (EMPA KIDNEY, DAPA CKD, and CREDENCE) or as a prespecified secondary endpoint (EMPEROR REDUCED). Seven of these nine RCTs with SGLT-2i (exceptions: EMPEROR PRESERVED and DAPA HF) reported significantly reduced progression of renal composite events. The risk ratio reduction with SGLT-2i ranged between 25% and 47%. Regarding finerenone, the renal composite outcome was reported in two RCTs (FIDELIO DKD and FIGARO DKD), with a reduction in the risk ratio for the renal composite outcome ranging between 22% and 26%. Five RCTs reporting on GLP1-RA reported renal composite events as part of their secondary endpoints (EXSCEL, AMPLITUDE-O, LEADER, REWIND, and SUSTAIN-6). Four of these five RCTs reporting on GLP1-RA (exception: EXCEL) were associated with benefits with a risk ratio reduction ranging between 13% and 38%. A recent network meta-analysis documented that SGLT-2 is superior to GLP1-RA and finerenone based on renoprotective effects but did not elaborate on the differences among the individual molecules [28]. The results of another network meta-analysis comparing SGLT-2i to finerenone led the authors to conclude in favor of the former [29].
Findings from Our Network Meta-analysis
This network meta-analysis was conducted building upon those conducted earlier with the aim to explore the differences between the individual molecules within the reno-protective group (if any). This was the first analysis conducted using the MDS ranking based on indirect pairwise comparison, thereby creating a hierarchy of choice. Regarding groups of agents, SGLT-2i occupied the first position followed by GLP1-RA and finerenone. Regarding individual molecules, dapagliflozin scored the highest, followed by empagliflozin, efpeglenatide, canagliflozin, semaglutide, liraglutide, finerenone, dulaglutide, and exenatide-LAR.
Limitations and Strengths
One of the primary limitations of this analysis is the lack of access to individual patient data. The entire analysis was conducted based on published pooled analyses. Another important limitation is the lack of a uniform definition for the renal composite outcome. The design of the indirect pairwise comparison between agents invariably leads to inflation of the confidence interval, which could have led to an underestimation of the pooled effect size. Although the scoring system seems to provide a sense of hierarchy, it is by no means a substitute for a well-conducted head-to-head comparative study. The paucity of data with MRA with only finerenone being investigated is another limitation. The inclusion of patients receiving SGLT-2i in the control arm of both the FIDELIO-DKD and the FIGARO-DKD trials could have confounded the outcome.
The main strength of this analysis is the very large amount of pooled data included in the analysis. The inclusion of RCTs as well as a large preanalytical power were additional strengths. Although considerable differences were noted between the different parameters used to define the renal composite outcome, the differences in clinical outcomes were too small to have any significant impact on the final outcome. In the absence of planned studies evaluating the reno-protective molecules, network meta-analysis combined with scoring seems to be the best available option.
Conclusion
SGLT-2i, and in particular dapagliflozin, ranked relatively high compared to other renoprotective agents in retarding the progression of DKD. Additional within-molecule comparisons in RCTs are needed to confirm these findings.
References
Alicic RZ, Rooney MT, Tuttle KR. Diabetic kidney disease: challenges, progress, and possibilities. Clin J Am Soc Nephrol. 2017;12(12):2032–45.
Hoogeveen E. The epidemiology of diabetic kidney disease. Kidney Dial. 2022;2:433–42. https://doi.org/10.3390/kidneydial2030038.
Kim MK. Treatment of diabetic kidney disease: current and future targets. Korean J Intern Med. 2017;32(4):622–30.
Sugahara M, Pak WLW, Tanaka T, Tang SCW, Nangaku M. Update on diagnosis, pathophysiology, and management of diabetic kidney disease. Nephrology (Carlton). 2021;26(6):491–500.
Toth-Manikowski S, Atta M. Diabetic kidney disease: pathophysiology and therapeutic targets. J Diabetes Res. 2015. https://doi.org/10.1155/2015/697010.
Ninčević V, Omanović Kolarić T, Roguljić H, Kizivat T, Smolić M, Bilić ĆI. Renal benefits of SGLT 2 inhibitors and GLP-1 receptor agonists: evidence supporting a paradigm shift in the medical management of type 2 diabetes. Int J Mol Sci. 2019;20(23):5831.
Cha DR. Mineralocorticoid receptor blockade for renoprotection. Kidney Res Clin Pract. 2018;37(3):183–4.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;2021:372:n71. https://doi.org/10.1136/bmj.n71.
The EMPA-KIDNEY Collaborative Group. Empagliflozin in patients with chronic kidney disease. N Engl J Med. 2022. https://doi.org/10.1056/NEJMoa2204233?articleTools=true.
Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375:323–34. https://doi.org/10.1056/nejmoa1515920.
Anker SD, Butler J, Filippatos G, et al. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med. 2021;385:1451–61. https://doi.org/10.1056/NEJMoa2107038.
Packer M, Anker SD, Butler J, Fet al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383:1413–24. https://doi.org/10.1056/NEJMoa2022190.
Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380:347–57. https://doi.org/10.1056/NEJMoa1812389.
McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381:1995–2008. https://doi.org/10.1056/NEJMoa1911303.
Solomon SD, McMurray JJV, Claggett B, et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N Engl J Med. 2022;387:1089–98. https://doi.org/10.1056/NEJMoa2206286.
Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383:1436–46. https://doi.org/10.1056/NEJMoa2024816.
Perkovic V, de Zeeuw D, Mahaffey KW, et al. Canagliflozin and renal outcomes in type 2 diabetes: results from the CANVAS Program randomised clinical trials. Lancet Diabetes Endocrinol. 2018;6(9):691–704.
Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380:2295–306. https://doi.org/10.1056/NEJMoa1811744.
Bakris GL, Agarwal R, Anker SD, et al. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med. 2020;383:2219–29. https://doi.org/10.1056/NEJMoa2025845.
Pitt B, Filippatos G, Agarwal R, et al. Cardiovascular events with finerenone in kidney disease and type 2 diabetes. N Engl J Med. 2021;385:2252–63.
Holman RR, Bethel MA, Mentz RJ, et al. Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2017;377:1228–39. https://doi.org/10.1056/nejmoa1612917.
Gerstein HC, Sattar N, Rosenstock J, et al. Cardiovascular and renal outcomes with efpeglenatide in type 2 diabetes. N Engl J Med. 2021;385:896–907. https://doi.org/10.1056/NEJMoa2108269.
Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375:311–22. https://doi.org/10.1056/nejmoa1603827.
Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet. 2019;394(10193):121–30. https://doi.org/10.1016/S0140-6736(19)31149-3.
Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375:1834–44. https://doi.org/10.1056/nejmoa1607141.
Chen Y, Lee K, Ni Z, He JC. Diabetic kidney disease: challenges, advances, and opportunities. Kidney Dis. 2020;6:215–25. https://doi.org/10.1159/000506634.
de Boer I, Caramori LM, Chan J, et al. KDIGO 2020 clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int. 2020;98(4):S1–115. https://doi.org/10.1016/j.kint.2020.06.019.
Kawai Y, Uneda K, Yamada T, et al. Comparison of effects of SGLT-2 inhibitors and GLP-1 receptor agonists on cardiovascular and renal outcomes in type 2 diabetes mellitus patients with/without albuminuria: a systematic review and network meta-analysis. Diabetes Res Clin Pract. 2022;183:109146. https://doi.org/10.1016/j.diabres.2021.109146.
Zhao LM, Zhan ZL, Ning J, Qiu M. Network meta-analysis on the effects of SGLT2 inhibitors versus finerenone on cardiorenal outcomes in patients with type 2 diabetes and chronic kidney disease. Front Pharmacol. 2022;12: 751496.
Acknowledgements
We would like to acknowledge all the investigators and the participating patients in the trials included for this analysis.
Funding
The journal’s Rapid Service Fee was funded by the authors.
Authorship
All named authors take responsibility for the integrity of the work and have given their approval for this version to be published.
Author Contributions
SG and BS conceptualized the study. The meta-analysis was conducted by SG. BS cross validated the data and prepared the manuscript. SG and BS conducted an expanded literature review to contextualize the results from the meta-analysis.
Disclosures
The authors Samit Ghosal and Binayak Sinha declare that they have nothing to disclose.
Compliance with Ethical Guidelines
This analysis consisted of data which were previously published. No authors were involved in carry out experiment on animals or human beings. Therefore, an ethical or board review approval was not required for this analysis.
Data Availability
All data are freely available in all electronic databases. References have been given.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Ghosal, S., Sinha, B. Assessing the Effects of Modern Renoprotective Agents in Preventing Progression of Renal Composite Outcomes in Patients with Type 2 Diabetes: A Network Meta-analysis. Diabetes Ther 14, 415–424 (2023). https://doi.org/10.1007/s13300-022-01359-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-022-01359-0