
Abstract
Introduction
There has been no nationwide health (diabetes) survey in Nigeria since 1992, when a diabetes mellitus (DM) prevalence of 2.2% was reported. We aimed to determine the prevalence of and risk factors for DM in Nigeria by performing a systematic review and meta-analysis.
Methods
We searched Medline, EMBASE, PubMed, PapersFirst, the Cochrane Library, Scopus, Bioline, African Journals Online, Institute of Scientific Information, and Google Scholar from the year 1990 to 2017. Using MeSH headings, the terms “diabetes mellitus,” “risk factors,” “prevalence,” and “Nigeria” as well as variations thereof were searched for. The last search was performed on 26 November 2017. We only included studies that utilized the random plasma glucose test, the fasting plasma glucose test, the oral glucose tolerance test (OGTT), or HbA1c to diagnose DM. A total of 23 studies (n = 14,650 persons) were evaluated. A random effects model was used to estimate the pooled prevalence of DM. We estimated the overall pooled prevalence of DM and subgroup-specific DM prevalences while accounting for inter-study and intra-study variability/heterogeneity.
Results
The overall pooled prevalence of DM was 5.77% (95% CI 4.3–7.1). The pooled prevalences of DM in the six geopolitical zones of Nigeria were 3.0% (95% CI 1.7–4.3) in the north-west, 5.9% (95% CI 2.4–9.4) in the north-east, 3.8% (95% CI 2.9–4.7) in the north-central zone, 5.5% (95% CI 4.0–7.1) in the south-west, 4.6% (95% CI 3.4–5.9) in the south-east, and 9.8% (95% CI 7.2–12.4) in the south-south zone. Risk factors for the pooled prevalence of DM were a family history of DM (4.6%; 95% CI 3.5–5.6); urban dwelling (6.0%; 95% CI 4.3–7.8); unhealthy dietary habits (8.0%; 95% CI 5.4–10.5); cigarette smoking (4.4%; 95% CI 1.3–10.2); older age (6.6%; 95% CI 4.5–8.7); physical inactivity (4.8%; 95% CI 3.2–6.4); and obesity (5.3%; 95% CI 3.8–6.9).
Conclusion
There has been an increase in the prevalence of DM in Nigeria. All regions of the country have been affected, with the highest prevalence seen in the south-south geopolitical zone. Urban dwelling, physical inactivity, advanced age, and unhealthy diet are important risk factors for DM among Nigerians. A national diabetes care and prevention policy is highly recommended.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Diabetes mellitus (DM) is a metabolic disorder of chronic hyperglycemia characterized by disturbances to carbohydrate, protein, and fat metabolism resulting from absolute or relative insulin deficiency with dysfunction in organ systems [1]. This disease has shown a tremendous increase in prevalence with a demographic transition in its epidemiology in recent years. Populations previously unaffected or minimally affected by DM are now reporting soaring prevalence figures, which poses a real challenge to health financing by governments and nongovernmental organizations. The latest prevalence figure published by the International Diabetes Federation (IDF) is 425 million persons living with DM worldwide, with nearly 50% of these undiagnosed [2]. The developing economies of Africa and Asia contribute a significant fraction of this figure. There is also a rising burden from the complications of DM alongside the ever-increasing prevalence of the disease [3]. We now see high rates of DM-related amputations, cerebrovascular disease, heart-related problems, and kidney disease in populations that were not previously known for these challenging health problems.
In Nigeria, the current prevalence of DM among adults aged 20–69 years is reported to be 1.7% [2]. It is widely perceived that prevalence figures reported by the IDF grossly under-report the true burden of DM in Nigeria, given that they are derived through the extrapolation of data from other countries. Various researchers have reported prevalences ranging from 2% to 12% across the country in recent years [4,5,6,7]. The last time a nationwide population estimate of DM was undertaken in Nigeria was during the 1992 Nigerian National Non-communicable Diseases (NCD) survey, where DM was said to occur in 2.2% of the population [8]. There has been no nationwide health (diabetes) survey in Nigeria since then. However, it is important to determine the actual burden of DM in Nigeria to facilitate appropriate health resource allocation, advocacy, and planning. Thus, in the work reported in the present paper, we aimed to determine the prevalence of and risk factors for DM in Nigeria using a systematic review and meta-analysis.
Methods
Data Search
We searched Medline, EMBASE, PubMed, PapersFirst, the Cochrane Library, Scopus, Bioline, African Journals Online, the Institute of Scientific Information, and Google Scholar from the year 1990 to 2016. Using MeSH headings, the terms “diabetes mellitus,” “risk factors,” “prevalence,” and “Nigeria” as well as variations thereof were searched for. We contacted the authors of articles in journals that were not available online. The last search was performed on 26 November 2017. Studies included in the meta-analysis were those that utilized the oral glucose tolerance test (OGTT), the random plasma glucose (RPG) test, the fasting plasma glucose (RPG) test, or glycated hemoglobin (HbA1c) to diagnose DM. In all, a total of 23 studies involving 14,650 persons were evaluated.
Inclusion Criteria
Only population-based studies that were executed between 1990 and 2017 and in which FPG, RPG, OGTT, or HbA1C was used to diagnose DM were included in the meta-analysis.
Exclusion Criteria
Clinic/hospital-based studies and those performed before 1990 or after 2017 were excluded from the meta-analysis.
Compliance with Ethics Guidelines
This review and meta-analysis is based on previously conducted studies and does not involve any study with human participants or animals performed by the authors.
Data Extraction
Various data were extracted from eligible studies, such as the prevalence of DM, risk factors for DM, method of diagnosing DM, study design, and Nigerian geopolitical zone in which the study was carried out. A summary of the data extracted is shown in Table 1. We coded the data based on the name of the first author of the study and the year that the study was published. Multiple coder agreement was assessed using Cohen’s kappa [9].
Operational Definitions
DM was diagnosed based on the 1999 WHO diagnostic criteria for DM or the ADA 2010 diagnostic criteria for DM [1, 10]. According to the 1999 WHO diagnostic criteria [1], the cut-off plasma glucose values for diagnosing DM are as follows:
-
Fasting plasma glucose ≥ 7.0 mmol/L
-
Random plasma glucose ≥ 11.1 mmol/L
-
Plasma glucose 2-h post-glucose load (75 g) ≥ 11.1 mmol/L
The 2010 ADA diagnostic criteria [10] for DM states that a glycated hemoglobin (HbA1c) value of ≥ 6.5% is diagnostic of DM if the assay technique is based on high-performance liquid chromatography (HPLC). The HPLC assay technique potentially adjusts for hemoglobinopathies and provides information on hemoglobin variants. In populations such as the Nigerian population, where there is a high prevalence of hemoglobinopathies and factors that diminish red blood cell survival, the HPLC platform adequately and accurately provides HbA1c values. In this meta-analysis, only studies that utilized the HPLC platform to evaluate HbA1c were included.
Quality of the Studies Included
Two authors separately assessed the quality of the studies included using the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies [11]. The studies were assessed with questions appropriate to the study design. We graded the quality of the study as good (G) if its rating was at least 70%, fair (F) if its rating was at least 50%, and poor (P) if its rating was less than 50%.
Statistical Analyses
The primary outcome measure was the prevalence of DM. The standard error in the prevalence was estimated using the binomial probability distribution. A random effects model based on the DerSimonian-Laird [12] method was used to estimate the pooled prevalence of DM and the confidence interval via weighted least squares (weighting was based on the reciprocal sum of the between- and within-study variances). The inter-study heterogeneity was evaluated using Cochran’s Q test [13]. We defined low, medium, and high heterogeneity a priori as Cochrane Q values of 25%, 50%, and 75%, respectively. We estimated the overall pooled prevalence of DM and the subgroup-specific prevalences accounting for the inter-study and intra-study variability/heterogeneity. An assessment of risk factors was undertaken.
Publication bias was appraised using Begg’s [14] rank correlation methods and Egger’s [15] weighted regression test. All analyses were performed using the STATA software (version 11). A level of significance of 0.05 was adopted for Cochran’s Q test.
The null hypothesis of this study assumed that all of the studies reported the same prevalence in the various populations studied.
Results
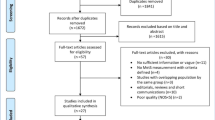
The total number of records initially identified during the database searches was 149, but only 23 studies (total number of persons: 14,650) were eventually found to be eligible for inclusion in the meta-analysis, as shown in Fig. 1. The overall pooled prevalence of DM was 5.77% (95% CI 4.3–7.1). The overall prevalence and the prevalences of DM in subgroups categorized by diagnostic method are shown in Fig. 2. Figure 3 shows the pooled prevalence of DM in each of the six geopolitical zones of Nigeria, which indicates that the highest prevalence occurred in the south–south zone (9.8%; 95% CI 7.2–12.4) and the lowest in the north-west zone (3.0%; 95% CI 1.7–4.3). Assessment of the risk factors for DM (see Fig. 4) revealed that unhealthy dietary habits (8.0%; 95% CI 5.4–10.5), older age (6.6%; 95% CI 4.5–8.7), and urban dwelling (6.0%; 95% CI 4.3–7.8) were the leading risk factors for DM in Nigeria.

Flow diagram of the studies included in the meta-analysis

Forest plot showing the overall prevalence of diabetes and the prevalences of diabetes in subgroups categorized by method of diagnosis

Prevalence of diabetes in each geopolitical zone of Nigeria

Prevalences of risk factors for diabetes mellitus
Discussion
The United Nation estimates that the population of Nigeria as of September 2017 was 193.3 million [16]. The pooled DM prevalence of 5.77% observed in our meta-analysis suggests that 11.2 million Nigerians (1 out of every 17 adults) are living with the disease. Regional differences in the prevalence of DM, with the highest rate observed in the south–south zone and the lowest rate seen in the north-western zone, mirror a similar finding for obesity, which is a major risk factor for type 2 diabetes [17].
To the best of our knowledge, this is the first study to determine the prevalence of and risk factors for diabetes in Nigeria using a systematic review and meta-analysis. The pooled DM prevalence of 5.77% found in our study is quite similar to the 2013 IDF estimate derived from extrapolations from populations with similar sociodemographic characteristics [18]. Our diagnostic methods also differ from those of the IDF, which mainly promotes the use of the OGTT. Although the OGTT is the gold standard for the diagnosis of DM, FPG and RPG are also good tools that are cheaper and easier to apply, even in remote settings where an OGTT may not be feasible. In 2010, the ADA recommended the use of the glycosylated hemoglobin (HbA1c) test in the diagnosis of DM [10]. We found only one study that used HbA1c measured using high-performance liquid chromatography (HPLC) to diagnose DM based on a cutoff of ≥ 6.5%.
Compared with the 1992 NCD population estimate of 2.2% [8], the prevalence of DM obtained in this meta-analysis suggests a 2.6-fold increase in prevalence over the past two and half decades. We found urban dwelling, physical inactivity, advancing age, and an unhealthy diet to be the leading risk factors for DM among Nigerians. It has been demonstrated that sub-Saharan Africa has one of the fastest annual rates of change in the number of urban dwellers in the world [19]. Studies have reported a two- to fivefold increase in the risk of diabetes and pre-diabetes in association with urban residence [20, 21]. Urbanization is also associated with decreased physical activity energy expenditure (PAEE), an independent risk factor for metabolic syndrome [22].
The modest improvement in living standards witnessed over the past few years in Nigeria has resulted in the aging of its populace. Insulin resistance tends to worsen with advancing age [23]. This, coupled with decreased physical activity among the aged, increases the risk of type 2 diabetes. Among the risk factors for DM found in our study, unhealthy dietary habits was the most prevalent, which is not surprising considering the proliferation of fast food outlets in many cities across the country. An unhealthy diet consisting mainly of high-fat, energy-dense foods contributes to the development of obesity and DM.
The strength of our study is that it is the first to determine the prevalence of and risk factors for diabetes in Nigeria based on a systematic review of the literature and meta-analyses. In addition, the selected studies cover the six geopolitical zones of Nigeria, making it possible to pinpoint regional differences in the prevalence of DM.
Limitations of our study include the cross-sectional design of the selected studies, making causal associations between diabetes and the identified risk factors difficult. Our study also did not consider other potential risk factors for diabetes, such as gender and socioeconomic status. Finally, the fact that we selected studies which used different screening methods for the diagnosis of diabetes means that some people with the disease could have been missed.
Conclusions
There has been a significant increase in the prevalence of DM in Nigeria, affecting all regions of the country, with the highest prevalence noted in the south-south geopolitical zone. Urban dwelling, physical inactivity, advancing age, and unhealthy diet are important risk factors for DM among Nigerians. A national diabetes care and prevention policy is highly recommended.
References
WHO. Definition, diagnosis and classification of diabetes mellitus and its complications, part 1. Geneva: WHO; 1999.
International Diabetes Federation. Diabetes atlas. 8th ed. Brussels: International Diabetes Federation; 2017.
Uloko AE, Ofoegbu EN, Chinenye S, Fasanmade OA, Fasanmade AA, Ogbera AO, et al. Profile of Nigerians with diabetes mellitus—Diabcare Nigeria study group (2008): results of a multicenter study. Indian J Endocrinol Metab. 2012;16(4):558–564. (ERRATUM IN: Indian J Endocrinol Metab. 2012;16(6):981).
Nyenwe EA, Odia OJ, Ihekwaba AE, Ojule A, Babatunde S. Type 2 diabetes in adult Nigerians: a study of its prevalence and risk factors in Port Harcourt, Nigeria. Diabetes Res Clin Pract. 2003;62(3):177–85.
Puepet FH, Ohwovoriole AE. Prevalence of risk factors for diabetes mellitus in a non-diabetic population in Jos, Nigeria. Niger J Med. 2008;17(1):71–4.
Sabir AA, Isezuo SA, Ohwovoriole AE. Dysglycaemia and its risk factors in an urban Fulani population of northern Nigeria. West Afr J Med. 2011;30(5):325–30.
Gezawa ID, Puepet FH, Mubi BM, Uloko AE, Bakki B, Talle MA, et al. Socio-demographic and anthropometric risk factors for type 2 diabetes in Maiduguri, North-Eastern Nigeria. Sahel Med J. 2015;18(5):1–7.
Akinkugbe OO, editor. Non-communicable disease in Nigeria. Final report of National Survey. Lagos: Federal Ministry of Health and Social Services; 1997. p. 64–90.
Cohen J. Weighted kappa: normal scale agreement with provision for scaled disagreement or partial credit. Psychol Bull. 1968;70(4):2133–220.
American Diabetes Association. Diagnosis and classification of diabetes: diabetes care. Diabetes Care. 2010;33(Suppl 1):S62–9.
NHLBI. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Available from: https://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/cohort. Accessed 28 May 2017.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–88.
Cochran William G. The comparison of percentages in matched samples. Biometrika. 1950;37(3/4):256–66.
Beggs CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–101.
Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by simple graphical test. BMJ. 1997;315(7109):629–34.
Worldometers.info. Worldometers live counters (based on information from the United Nations document “World population prospects: the 2017 revision”). Available from: http://www.worldometers.info.
Gezawa ID, Puepet FH, Mubi BM, Uloko AE, Haliru I. Prevalence of overweight and obesity in Maiduguri North-Eastern Nigeria. Nigerian J Med. 2013;22(3):171–4.
International Diabetes Federation. Diabetes atlas. 6th ed. Brussels: IDF; 2014. Available from: http://www.idf.org/diabetesatlas. Accessed 10 Mar 2016.
Hove M, Ngwerume ET, Muchemwa C. The urban crises in sub-Saharan Africa: a threat to human security and sustainable development. Stability. 2013;2(1):Art.7. http://doi.org/10.5334/sta.ap.
Saquib N, Saquib J, Ahmed T, Khanam MA, Cullen MP. Cardiovascular diseases and type 2 diabetes in Bangladesh: a systematic review and meta-analysis of studies between 1995 and 2010. BMC Public Health. 2012;12:434.
Chatterjee R, Narayan KM, Lipscomb J, Phillips LSS. Screening adults for pre-diabetes and diabetes may be cost-saving. Diabetes Care. 2010;33(7):1484–90.
Assah FK, Ekelund U, Brage S, Mbanya JC, Wareham NJ. Urbanization, physical activity, and metabolic health in sub Saharan Africa. Diabetes Care. 2011;34(2):491–6.
Gerch JE. Contributions of insulin-resistance and insulin-secretory defects to the pathogenesis of type 2 diabetes mellitus. Mayo Clin Proc. 2003;78(4):447–56. https://doi.org/10.4065/78.4.447.
Kyari F, Tafida A, Sivasubramaniam S, Murthy GV, Peto T, Nigeria National Blindness and Visual Impairment Study Group. Prevalence and risk factors for diabetes and diabetic retinopathy: results from the Nigeria National Blindness and Visual Impairment survey. BMC Public Health. 2014;18(14):1299. https://doi.org/10.1186/1471-2458-14-1299.
Omorogiuwa A, Oaikhena GA, Okioya P, Akubueze D, Owobu E. Diabetes mellitus: prevalence amongst university staff in Southern Nigeria and attitude towards routine glycemic/glucosuric checkup. Int J Biomed Health Sci. 2010;6(1):25–29.
Ekpenyong CE, Akpan UP, Ibu JO, Nyebuk DE. Gender and age specific prevalence and associated risk factors of type 2 diabetes mellitus in Uyo Metropolis, South Eastern Nigeria. Diabetologia Croatica 2012;41:17–23.
Oyegbade OO, Abioye-kuti EA, Kolawole BA, Ezeoma IT, Bello IS. Screening for diabetes mellitus in a Nigerian family practice population. SA Fam Prac. 2007;49(8):15.
Opeodu OI, Adeyemi BF. Undiagnosed diabetes mellitus: a survey of dental outpatients in a tertiary hospital. Afr J Med Med Sci. 2013;42(1):39–45.
Gabriel UP, Amadi AN, Ebirim CI. Type 2 diabetes mellitus in ambulatory adult Nigerians: prevalence and associated family biosocial factors in a primary care in Eastern Nigeria: a cross-sectional study. BJMMR. 2015;9(3):1–12.
Dahiru T, Jibo A, Hassan AA, Mande AT. Prevalence of diabetes in a semi-urban community in Northern Nigeria. Niger J Med. 2008;17(4):414–6.
Anzaku AS, Musa J. Prevalence and associated risk factors for gestational diabetes in Jos, North-central, Nigeria. Arch Gynecol Obstet. 2013:287(5):859–63.
Adeniyi AF, Uloko AE, Musa NH. Prevalence of non-invasive risk factors of type 2 diabetes among higher education teachers in North-Western Nigeria. Sudan J Med Sci. 2010;5(2):137–43.
Etukumana EA, FH Puepet FH, Obadofin MO. Prevalence of diabetes mellitus among adults in rural north central Nigeria. Highl Med Res J. 2013;13(2):98–100. ISSN: 1596-2407.
Nwafor A, Owhoji A. Prevalence of diabetes mellitus among Nigerians in Port Harcourt correlates with socio-economic status. J Appl Sci Environ Manag. 2001;5(1):75–7.
Sabir A, Ohwovoriole A, Isezuo S, Fasanmade O, Abubakar S, Iwuala S. Type 2 diabetes mellitus and its risk factors among the rural Fulanis of northern Nigeria. Ann Afr Med. 2013;12(4):217–22.
Chukwunonso ECC, Nnamdi KU. Diabetes and pre-diabetes in adult Nigerians: prevalence, and correlations of blood glucose concentrations with measures of obesity. Afr J Biochem Res. 2015;9(3):55–60.
Bakari AG, Onyemelukwe GC, Sani BG, Aliyu TM, Hassan SS. Prevalence of diabetes in suburban northern Nigeria: results of a public health screening survey. Available from: http://www.abu.edu.ng/publications/2010-09-25-043819_4407.pdf.
Isara AR and Okundia PO. The burden of hypertension and diabetes mellitus in rural communities in southern Nigeria. Pan Afr Med J. 2015;20:103. https://doi.org/10.11604/pamj.2015.20.103.5619.
Enang OE, Otu AA, Essien OE, Okpara H, Fasanmade OA, et al. Prevalence of dysglycemia in Calabar: a cross-sectional observational study among residents of Calabar, Nigeria. BMJ Open Diabetes Res Care. 2014;2(1):e000032.
Ramalan MA. Glycated haemoglobin in the screening and diagnosis for type 2 diabetes mellitus in Nigeria. FMCP dissertation part 2. Lagos: National Postgraduate Medical College of Nigeria; 2016. In process.
Olamoyegun MA, Iwuala SO, Olamoyegun KD. Insulin-related knowledge of healthcare professionals in a Nigerian tertiary health institution. Int J Diabetes Dev Ctries. 2015;35:84.
Acknowledgements
We thank the participants of this study and all of the researchers of the studies included in the analysis.
Funding
No funding or sponsorship was received for this study or the publication of this article.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Disclosures
All authors of this article (Andrew E. Uloko, Baba M. Musa, Mansur A. Ramalan, Ibrahim D. Gezawa, Fabian H. Puepet, Ayekame T. Uloko, Musa M. Borodo, and Kabiru B. Sada) have nothing to disclose.
Compliance with Ethics Guidelines
This meta-analysis is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
Data Availability
The datasets obtained during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced Digital Features
To view enhanced digital features for this article go to https://doi.org/10.6084/m9.figshare.6216518.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Uloko, A.E., Musa, B.M., Ramalan, M.A. et al. Prevalence and Risk Factors for Diabetes Mellitus in Nigeria: A Systematic Review and Meta-Analysis. Diabetes Ther 9, 1307–1316 (2018). https://doi.org/10.1007/s13300-018-0441-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-018-0441-1