
Abstract
Background
Type 2 diabetes is associated with acute and chronic complications and poses a large economic, social, and medical burden on patients and their families as well as society.
Objective
This study aims to evaluate the direct economic burden of type 2 diabetes in China. Data source: systematic review on cost of illness, health care costs, direct service costs, drug costs, and health expenditures in relation to type 2 diabetes was conducted up to 2014 using databases such as Pubmed; EBSCO; Elsevier ScienceDirect, Web of Science; and a series of Chinese databases, including Wanfang Data, China National Knowledge Infrastructure (CNKI), and the China Science and Technology Journal Database. Factors influencing hospitalization and drug fees were also identified. Study eligibility criteria: (1) estimation of the direct economic burden including hospitalization and outpatient cost of type 2 diabetes patients in China; (2) evaluation of the factors influencing the direct economic burden. Articles only focusing on the cost-effectiveness analysis of diabetes drugs were excluded.
Results
The direct economic burden of type 2 diabetes has increased over time in China, and in 2008, the direct medical cost reached $9.1 billion, Both outpatient and inpatient costs have increased. Income level, type of medical insurance, the level of hospital care, and type and number of complications are primary factors influencing diabetes related hospitalization costs. Compared to urban areas, the direct non-medical cost of type 2 diabetes in rural areas is significantly greater.
Conclusions
The direct economic burden of type 2 diabetes poses a significant challenge to China. To address the economic burden associated with type 2 diabetes, measures need to be taken to reduce prevalence rate and severity of diabetes and hospitalization cost.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of diabetes is increasing rapidly worldwide with the influence of expanding economy, abrupt transition of living styles, and social aging [1]. In 2014, there were 387 million people living with diabetes worldwide. The number is predicted to reach 592 million by 2035 of which 46% will still be un-diagnosed [2]. Throughout the world, there exists a large amount of diversity with respect to diabetes prevalence, deaths, and health expenditure [2]. According to the 6th edition (2014 update) of the International Diabetes Federation (IDF) Diabetes Atlas, the Western Pacific (WP) has the largest population with diabetes (137.8 million), which means that 7.9% of the population in this region has diabetes. The region with the second highest prevelance is Southeast Asia (SEA) with 75.0 million patients (Table 1). Asian countries were among the top ten countries for prevalence of diabetes in 2013 [2]. Another fact of spatial distribution is that the prevalence rate of diabetes in developing countries is higher. More than 80% of diabetic patients live in low- and middle-income countries [3]. Globally, 90% of diabetic patients have type 2 diabetes, of which 77% live in developing countries [4, 5]. In China, the number of diabetes patients in China was 96.3 million, 29.5 million more compared to India, in 2014. The prevalence rate of diabetes had reached 9.3% [2].
China carried out five large-scale epidemiological surveys to understand better the prevalence of type 2 diabetes. The prevalence rate of diabetes has been increasing in China from 0.67% in 1980 [6], 2.51% in 1994–1995 [7], 3.21% in 1996 [8], 3.31% in 2002 [9], and 9.7% in 2007–2008 [10]. According to these survey results, the morbidity rate of type 2 diabetes mellitus accounted for 93.70% of all types of diabetes in China where socioeconomic status seems to have influenced the prevalence rate [7]. The prevalence of pre-diabetes among the rural population (16.6%) is far greater compared to urban (13.6%) [11]. This poses a higher risk of diabetes among the rural population.
In addition, the high mortality of diabetes and related complications is also a huge challenge. The premature mortality of patients with diabetes is mostly attributable to related complications, not uniquely related to the condition. One half of the patients die of cardiovascular disease (CVD) [12]. It was recorded in “The global burden of disease: 2004 update” that 508,000 men and 633,000 women died from direct diabetes-related causes, accounting for 1.6% and 2.3% of all deaths in the world, respectively [13]. The International Diabetes Federation in 2007 reported diabetes-related deaths to be 6% of total global mortality in the population aged 20–79 years. Statistics from 2013 assessed 5,096,955 diabetes-related deaths in 20–79 year-olds in the world, of which 1,271,003 were recorded in China [2]. The mortality of diabetes is strongly related to age. In patients with type 2 diabetes under 35 years old, 75% will die from diabetes and related complications. This rate decreases to 59% among 35–64 year-olds, and 29% at 64 years or older [14].
Given the high prevalence rate and mortality rate, understanding the disease burden of diabetes is the first step when formulating an effective control strategy for governments and international organizations.
Diabetes and related complications cause large economic losses [15]. Data from 2013 estimates that worldwide diabetes will contribute $548 billion in health expenditures (11% of the total health expenditure) and $1,437 per person on treating and managing the disease [2]. Diabetes-related health expenditure varies across regions and countries. The estimated health expenditure was $5,621 per person in high-income countries, compared to $356 in low- and middle-income countries. In 2013, the USA spent $239 billion on diabetes, or 36% of global health expenditure, meanwhile, China spent just $38 billion, less than 7% of the global total in the same year [2].
The disease burden resulting from diabetes has direct and indirect impact. The direct burden deals with health resource consumption, such as drug cost, outpatient cost, inpatient cost, and inspection cost. The indirect burden encompasses monetary losses resulting from opportunity costs caused by death, disability, and incapacitation. The indirect burden also includes the transportation expenses incurred by patients and their families, accommodation expenses, nutrition costs of patients, social productivity losses, income losses, and housework labor force losses (non-market productivity losses) [16].
As we know, nearly 90% of diabetic patients have type 2 diabetes. Thus, the objective of this study is to synthesize and analyze the costs of type 2 diabetes. It aims to answer two key questions: (1) Document economic burden of type 2 diabetes in China. (2) Identify main factors affecting the economic burden of type 2 diabetes in China.
Methods
This is a systematic review study.
Data Sources and Search Strategies
The main English databases, including Pubmed and EBSCO, and the Chinese databases, including Wanfang Data, China National Knowledge Infrastructure (CNKI), and the China Science and Technology Journal Database, were explored for relevant articles with the following combination of keywords: (diabetes mellitus and type 2) and (cost of illness or illness burden or cost of disease or economic burden of disease). The last search was conducted on June 30, 2013.
In the searching, studies considered for this review were English- and Chinese-language articles from peer-reviewed publications which focused on the evaluation of the direct economic burden of type 2 diabetes in China and on the comparison between China and other developed countries.
Inclusion Criteria and Exclusion Criteria
Inclusion criteria:
-
Estimation of the direct and indirect medical cost, hospitalization cost, and outpatient fee for type 2 diabetes patients in China;
-
Evaluation of factors influencing direct and indirect medical cost, hospitalization costs, and outpatient fee in China.
Exclusion criteria: articles that focused on the effectiveness evaluation of the diabetic drugs were ineligible for this review.
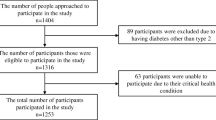
A total of 377 original citations were identified that met all the inclusion and exclusion criteria. After further review and elimination of duplicates, 39 studies (full text) were included for final analysis.
This review article is based on previously conducted studies and does not involve any new studies of human or animal subjects performed by any of the authors.
Results
The Direct Medical Costs
According to Table 2, in China, the direct medical cost of type 2 diabetes in proportion to the gross domestic product (GDP) increased gradually year by year. In 1993, it was reported that direct medical cost was $0.25 billion, accounting for 0.07% of the GDP [17]. In 2002, a national survey in 11 major cities indicated that the direct medical cost had increased $2.27 billion, and the percentage of direct medical cost in the GDP was 0.18% [18]. Some studies concluded, after comparing several national surveys, that the average annual growth rate of the direct medical cost of type 2 diabetes was 19.90% which was more than the average annual growth rate of the GDP (12.77%) and the national health expenditure (12.88%) from 1993 to 2003 [21]. More alarmingly, when it came to 2008, the direct medical cost already increased to $8.65 billion, accounting for 0.21% of the GDP [22].
The direct medical cost included outpatient cost and inpatient cost (hospitalization cost).
Referring back to Table 2, the annual total outpatient and inpatient costs were $0.22 billion and $0.03 billion, respectively, in 1993 [17]. And in 2008, they had risen to $5.53 billion and $3.13 billion, respectively [22]. According to a national survey on the economic burden of type 2 diabetes in China from 2007 to 2008, the average outpatient cost per person at a visit was $46.22 in urban areas. In rural areas, the average outpatient cost per person at a visit was $54.73 [23]. The average inpatient cost per person at a visit was $2,222.77 in urban areas, $1,420.30 more than the normal population. In rural areas, the annual inpatient cost per person at a visit was $499.73 [23]. Although the annul total outpatient cost was more than the total inpatient cost, the average inpatient cost per person at a visit was much more than the average outpatient cost per person at a visit. Thus, most studies focusing on the economic burden of diabetes highlight the proportion of hospitalization cost in direct medical cost as the highest. In recent years, the prevalence of type 2 diabetes in China has also risen rapidly, leading to higher hospitalization cost in direct medical cost, from 12.91% in 1993 [17] to 44.74% in 2003 [21].
The Direct Non-Medical Costs
The direct non-medical cost has also been increasing in recent years, including transportation of patients and their families, accommodation expenses, and nutrition costs of patients. The average direct non-medical cost per inpatient in urban and rural areas was $0.73 and 0.48, respectively in 1998. By 2003, it increased to $0.97, for both urban and rural areas. In 2008, the same cost escalated to $2.74 and 2.04 in urban and rural areas, respectively. Inpatient average direct non-medical cost per patient in urban areas jumped from $81.02 to 96.84 from 1998 to 2008, and from $39.18 to 71.74 in rural areas [24–26].
Factors Influencing Direct Medical Cost
The direct medical cost accounts for the majority of the economic burden. In recent years, there has been a rapid increase in hospitalization, which has contributed to the high overall direct medical cost. Factors influencing hospitalization cost include hospital stay, income level, types of medical insurance, level of hospital, and type and number of complications.
Hospitalization stay for diabetes patients is two times longer than non-diabetics [27, 28], and the length of hospital stay for diabetics has been increasing in the last 5 years. In Shangdong province, the hospitalization stay increased from 10.43 days in 2005 to 16.79 days in 2010 [29]. This increase leads to an increase in hospitalization expenditure [30]. According to a national survey on the economic burden of type 2 diabetes in China in 2007–2008, the hospitalization stay of diabetic patients was double the normal population [31].
Results indicated that hospitalization cost was significantly different among different income level populations [32]. Patients with high income tend to accept a more expensive and longer-term therapy strategy.
The type of medical insurance is also an important factor. In China, patients mainly have four types of medical insurance, including New Rural Cooperative Medical System (NCMS), Medical Insurance for Urban Workers, Medical Insurance for Urban Residents, and “out-of-pocket” payment. The average hospitalization cost per patient with Medical Insurance for Urban Workers ($1,094.53) was more than that with Medical Insurance of Urban Residents ($1,065.50), NCMS ($558.01), and “out-of-pocket” payments ($609.65) in 2005–2010 [29].
The level of hospital also had an important influence on hospitalization costs. In China, the hospitals are mainly divided into three levels including the tertiary hospital, the secondary hospital, and the primary hospital, based on their function, mission, facility, technology, quality of medical services, and scientific management [33]. Comparing the medical expenditure in the three levels of hospital, the higher the level that patients stayed, the more money patients paid [34].
The hospitalization cost increases with the number of complications. Of patients with a diagnosis of diabetes, 76.4% had reported at least one complication. Treatment cost of patients with complications shows a linear relationship where cost was 3.36 times higher for patients with complications compared to those without complications [35]. The complications resulting in a severe state of illness thus also increase the frequency of physical examinations and laboratory tests. To deal with these situations better, doctors prescribe use of better drugs or increase the doses for quick relief of associated symptoms, which has led to a difference in hospitalization costs among patients with different conditions. Type of complication is another factor influencing hospitalization cost. Medical expenditure of patients with microvascular or macrovascular disease or with both was higher than for those without, with an increase of 1.46, 1.75, and 2.38 times, respectively [36]. The average hospitalization cost of a patient with diabetic nephropathy was the highest followed by diabetic foot, and then cerebral infarction or cerebral hemorrhage. The average hospitalization cost per patient with diabetic nephropathy (dialysis patients), diabetic nephropathy (non-dialysis patients), and diabetic foot was $2,446.6, 1,672.5, and 2,305.5, respectively [37].
Discussion
In China, almost 90% of diabetic patients have type 2 diabetes. Most of them are 40–60 years old, and the prevalence rate increases gradually after 40 years old. Disability or death risk leads to catastrophic losses for the family and society. The direct economic burden of type 2 diabetes is increasing over time, with the yearly increment affecting the direct medical costs to GDP ratio. The average annual growth rate of the direct medical cost of type 2 diabetes is proportionately more than the average annual growth rate of the GDP and the national health expenditure. It is the second highest for all chronic diseases after hypertension. The direct medical cost of diabetes in China has approached, or in some instances even exceeded, some developed countries. Thus, we focused on the direct economic burden of type 2 diabetes.
As was mentioned above, hospitalization cost plays a decisive role in direct medical costs. The factors affecting hospitalization cost are income level, type of medical insurance, level of hospital, and related complications. The frequency and severity of complications determines the hospitalization cost. But the relationship between the hospitalization cost and the hospital level needed a further explanation. The tertiary hospitals provide high-level specialist medical services, teaching and research. The secondary one has a full complement of services including pediatrics, obstetrics, general medicine, gynecology, and various branches of surgery and psychiatry. The primary hospitals are the centers of community health services [33]. The high level hospitals often charge more for examination services and drugs than the low level hospitals. In addition, based on the Essential Drug System, the doctors in different level hospitals had different prescription privileges in China. The doctor in primary hospitals can just prescribe limited drugs which were included in the Essential Drug List. It is known that drugs are the main form of treatment for controlling blood glucose and glycosylated hemoglobin and is a significant contributor of costs for diabetes and related causes [38]. Because of the economic growth and more purchasing power, patients are willing to choose more expensive medications primarily because they think the price of the drug is associated with its effectiveness.
Changes in living environment and corresponding lifestyle are major reasons for the increase in prevalence of type 2 diabetes patients [39]. This mainly indicates the change of lifestyle. More and more people tend to enjoy unhealthy foods and with reduced engagement in physical activities; most people are subjected to regular intake of high-calorie, high-fat, and high-protein foods [40].
Incorporating measures related to health education can help reduce the prevalence of diabetes. Designing and implementing cost-effective diagnosis and treatment tools can help to deal with hospitalization and drug costs better. Type 2 diabetes is presently a major contributor of overall health care cost mainly due to poor knowledge about the disease among populations and the time difference between the onset of disease and treatment. The sooner the disease can be diagnosed, the less expensive the treatment and the cost for associated complications, which will further result in efficiency in providing simpler treatments, thus reducing the overall cost [41, 42]. Therefore, the methods for early screening, early diagnosis, and early treatment are necessary for follow-up, management, and monitoring in communities [43].
In this study, we mainly focus on the direct costs related to diabetes, but not the indirect costs because literature is lacking. In addition, diabetes can also result in big disease burdens for people in the form of disability-adjusted life years (DALYs), thus both indirect economic burden and disease burden need further study.
Conclusion
The direct medical burden of type 2 diabetes is a grave economic problem in China. Measures need to be taken to reduce prevalence rate, hospitalization cost, and drug cost in order to reduce the resulting economic burden. Because of the higher economic burden associated with rural areas of China, more rigorous interventions should be considered in these areas.
References
Whiting DR, Guariguata L, Weil C, et al. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract. 2011;94(3):311–21.
International Diabetes Federation. Title of subordinate document. In: Diabetes Atlas 6th ed. 2014 Update. http://www.idf.org/sites/default/files/Atlas-poster-2014_EN.pdf. Accessed 13 Nov 2011.
Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442.
Consultation WHO. Definition, diagnosis and classification of diabetes mellitus and its complications. Geneva, Switzerland: World Health Organization. 1999;31(3):1–59.
Khaltaev NG. Prevention of diabetes mellitus. Prev Diabetes Mellitus. 1994;844:1–100.
National Diabetes Survey Group. Report on diabetes survey of 14 provinces and 300000 residents in China. Chin J Intern Med. 1981;20:678–83.
Pan XR, Yang WY, Li GW, et al. Prevalence of diabetes and its risk factors in China, 1994. National Diabetes Prevention and Control Cooperative Group. Diabetes Care. 1997;20(11):1664–9.
Xiang HD, Liu W, Liu CQ, et al. National baseline survey report on the epidemiology of diabetes in 1996. Chin J Diabetes. 1998;6:131–3.
Li LM, Rao KQ, Kong LZ, et al. A description on the Chinese national nutrition and health survey in 2002. Chin J Epidemiol. 2005;26(7):478–84.
Yang WY, Lu JM, Weng JP, et al. Prevalence of diabetes among men and women in China. N Engl J Med. 2010;362(12):1090–101.
Prevention and control assessment team of diabetes. Title of subordinate document. In: The blue book of Chinese diabetes prevention and control. 2011. http://www.cdschina.org/news_show.jsp?id=1099.html. Accessed 11 Nov 2011.
Gu K, Cowie CC, Harris MI. Mortality in adults with and within diabetes in a national cohort of the US population, 1971–1993. Diabetes Care. 1998;21(7):1138–45.
Mathers CD, Fat DM, Boerma JT. The global burden of disease: 2004 update. World Health Organization; 2008.
Roglic G, Unwin N, Bennett PH, et al. The burden of mortality attributable to diabetes: realistic estimates for the year 2000. Diabetes Care. 2005;8(9):2130–5.
Williams R, Van Gaal L, Lucioni C. Assessing the impact of complications on the costs of Type II diabetes. Diabetologia. 2002;45(7):S13–7.
Hu SL. The research of disease burden. Health Econ Res. 2005;5:22–7.
Shen HB, Yu SZ, Xu YC. A study on morbidity variance and economic burden of diabetes mellitus in China. Shanghai J Prev Med. 1998;10(9):387–90.
Tang L, Chen XB, Chen HY, Zhao LY, Hu SL. The economic burden of type 2 diabetes and its complications in the urban area of China. Chin Health Econ. 2003;22(12):21–3.
Hu JP, Rao KQ, Qian JC, Wu J. The study of economic burden of chronic non-communicable diseases in China. Chin J Prev Contr Chronic Non-Commu Dis. 2007;15(3):189–93.
Wang JS, Jin SG. Contribution of diabetes to the burden of disease. Chin J Prev Med. 2007;41(3):l86–8.
Liu KJ, Wang M. Economic burden of main chronic non-infectious diseases in China. Chin Health Econ. 2005;24:77–80.
Li LN. The study of disease burden of diabetes in China in 2008. Beijing: Beijing University of Chinese Medicine; 2011.
Zhao WH. The study on direct economic burden of diabetes in China [D]. Beijing: Peking Union Medical College; 2012.
Ministry of Health. National health services research: report of the second national health services survey in 1998. 1st ed. Beijing: People’s Health Publishing House; 1999.
Statistical Information Center. National health services research: report of the third national health services survey in 2004. 1st ed. Beijing: Peking Union Medical College Press; 2004.
Statistical Information Center. National health services research: report of the second national health services survey in 2008. 1st ed. Beijing: Peking Union Medical College Press; 2009.
Olsson J, Nilsson S, Persson U, et al. Comparison of excess costs of care and production losses because of morbidity in diabetic patients. Diabetes Care. 1994;17(11):1257–63.
Currie CJ, Williams R, Peters JR. Patterns of inpatient and inpatient activity for diabetes; a district survey. Diabet Med. 1996;1:273–80.
Wang T, Yu BR, Yang F. An analysis on hospitalization costs and days of diabetes patients with different medical insurance types. Health Econ Resour. 2013;2:52–3.
Jiang JH, Zang TH, Yang MG, et al. Analysis on the factors influencing the length of hospital stay in the diabetic inpatients. Chin J Dis. 2001;5(4):313–5.
Chinese Diabetes Society. Chinese clinical guideline for type 2 diabetes (2012) [R]. Chin J Diabetes. 2013;22(8):2–42.
Zhang JL, Sun HM, Liu YQ, et al. A analysis on medical cost and its influencing factors in diabetes patients in Daqing. Theory Pract Chin Med. 2005;15(001):13–6.
Ministry of Health. Hospital classification management in China. 1st ed. Beijing: People’s Health Publishing House; 1989.
Sun HM, Chang BZ, Liu YQ, et al. Multivariate analysis on medical cost of diabetes patients. Health Econ Res. 2001;12:37–40.
Wang H. The relation between the medical cost of diabetes patients and general factors. Med Inform. 2011;24(8):4966–7.
Chen XB, Tang L, Chen HY, et al. Assessing the impact of complications on the costs of type 2 diabetes in urban China. Chin J Diabetes. 2003;11(4):238–41.
Wang JY, Xue YM, Ye XY. Analysis on key factors of the hospitalization cost of type 2 diabetes. Guangdong Med. 2007;28(9):1472–4.
He MZ, Li B, Bian Y. The structure analysis of hospitalization costs on diabetic in-patient. Chin Health Econ. 2009;28(11):22–4.
Guan XQ, Zheng YH, Wu QQ, et al. Investigation on current status of in-patient medical service and patient requirements. J First Mil Med Univ. 2002;22(5):472–5.
Xia SJ, Yang L, Hu SL. Analysis on the inpatient expenditure of diabetes mellitus and its complications. Chin Hosp Manag. 2004;24(9):40–2.
Li GY, Guo YP, Zheng RZ, et al. Screening for diabetes and the risk factors for type 2 diabetes in Daqing community citizens. Chin J Prev Control Chronic Non-Commun Dis. 2008;16(2):176–8.
Xing QL, Cao XG, Zhang Z, et al. The analysis on a correlation between the hospitalization cost and complications in diabetes patients. Chin J Prev Control Chronic Non-Commun Dis. 2003;11(6):283–4.
Lu W, Qiu YL, Ye L, et al. Analysis on the in- patient expenditure of Type 2 diabetes mellitus in Shanghai. Shanghai J Prev Med. 2007;19(2):80–2.
Acknowledgments
No funding or sponsorship was received for this study or publication of this article. Huimei Hu designed, collected data and wrote manuscript. Monika Sawhney, Lizheng Shi, Shengnan Duan, Yunxian Yu, Zhihong Wu and Guixing Qiu edited manuscript. Hengjin Dong designed, wrote and edited the manuscript. We wish to acknowledge the Major Consulting Project of Chinese Academy of Engineering “Strategic Research on Translational Medicine in China”.
Conflict of interest
Huimei Hu, Monika Sawhney, Lizheng Shi, ShengnanDuan,Yunxian Yu, Zhihong Wu, GuixingQiu, Hengjin Dong declare they have no conflict of interest.
Compliance with ethics
This review is based on previously conducted studies, and does not involve any new studies of human or animal subjects performed by any of the authors.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Hu, H., Sawhney, M., Shi, L. et al. A Systematic Review of the Direct Economic Burden of Type 2 Diabetes in China. Diabetes Ther 6, 7–16 (2015). https://doi.org/10.1007/s13300-015-0096-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-015-0096-0