
Abstract
Background
The purpose of this study was to test the stereology method using several grid sizes for measuring liver volume and to find which grid provides an accurate estimate of liver volume.
Materials and methods
Liver volume was measured by volumetry in 41 sets of liver MRI. MRI was performed before and after different weight-reducing regimens. Grids of 3, 4, 5, and 6 cm were used to measure liver volume on different occasions by stereology. The liver volume and the changes in volume before and after treatment were compared between stereology and volumetry.
Results
There was no significant difference in measurements between stereology methods and volumetry (p > 0.05). The mean differences in liver volume between stereology based on 3-, 4-, 5-, and 6-cm grids and volumetry were 37, 3, 132, and 23 mL, respectively, and the differences in measurement of liver volume change were 21, 2, 19, and 76 mL, respectively. The mean time required for measurement by stereology was 59–190 s.
Conclusion
Stereology employing 3- and 4-cm grids can rapidly provide accurate results for measuring liver volume and changes in liver volume.
Main Messages
• Statistical methods can be used for measuring area/volume in radiology.
• Measuring liver volume by stereology by 4-cm grids can be done in less than two minutes.
• Follow-up of liver volume is highly accurate with stereological methods.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
The regenerative capacity of the liver has been known since ancient times. Liver volume can be of prognostic value prior to liver surgery in certain patients [1, 2]. This is one of the many reasons that liver volume measurement has attracted much attention, with more than 200 results in PubMed when searching for “liver volumetry.” Measuring liver volume, however, is time-consuming and cumbersome [3]. There are several semi-automated software programs available for accomplishing the task, and most are used for computerized tomography (CT) images. Knowledge of attenuation on CT is very helpful for delineating the liver in semi-automated programs. Measurement of attenuation is not possible on magnetic resonance imaging (MRI) [4] and its different sequences.
While volumetry involves measuring the whole area occupied by an object on each plane (usually axial) and then summing them, stereology employs statistical methods to arrive at an estimated area or volume [5–11]. Volumetry is a survey of all pixels, whereas stereology is a sample of pixels thought to represent the whole area or volume. The methods by which stereology can be used for sampling differ. One can use a systematic sampling method, usually employing a grid, in which the points on the grid are counted if they fall on the target. This is usually referred to Cavalier’s principle (for further information please see Appendix 1).
The aim of this study was to compare liver volume as measured by volumetry with that measured using stereology on several systematic grids and find which grid provides an accurate estimate of liver volume and its change over time, as well as to estimate the time required for a stereological study.
Materials and methods
Stereology
Based on a previous small pilot study with CT, we anticipated that a grid with a size somewhere between 3 and 5 cm would provide an accurate estimate of liver volume. In the pilot, we used several grids for measuring area.
The stereological measurements used in this study were performed using software developed in-house. The program was implemented in C++ as an offline private application using an open-source image processing platform for medical image analysis (http://code.google.com/p/platinum-image/), which can run on Windows, Mac OS, and Linux. The software allows use of stereology grids with the desired resolution in axial, sagittal, or coronal directions.
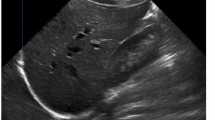
Each liver volume was measured on different occasions using 3-, 4-, 5-, and 6-cm grids. The measurements were made by a radiologist (with 11 years of experience in abdominal MRI and CT interpretation), blinded to the reference method and other stereological measurements (Fig. 1).

Screenshot of stereology software. The grid positioned on this slide is 40 x 40 mm (i.e., the grid resolution). The number of times the lines intersect within the boundaries of the liver is 13. Since each point of intersection represents 4 × 4 or 16 cm2, the total area occupied by the liver is estimated as 13 × 4 × 4 or 208 cm2. When an intersect falls on the border of the measured object, then a predefined corner is evaluated. Our radiologist opted for the upper right corner before the start of the study. If the right upper corner (or any corner chosen before the start of the study) is occupied by the object of interest, then the whole intersect is regarded as occupied by the liver. Otherwise, the intersection is considered to have fallen beyond the borders of the object of interest and is not included in the measurements
The liver volume for each subject was measured at three times: before and after low-calorie diet and after gastric bypass surgery. Differences between each of these states were calculated for each patient. These changes were measured by both stereological methods (3- to 6-cm grids) and volumetry. One subject had only two MRI examinations, and in this subject the change between these two available examinations was noted.
The subjects
The subjects were chosen from a previously published study [12], where the patients had undergone different treatments for obesity. All subjects were female. They had been imaged prior to and after treatments for weight reduction. The liver volumes were therefore expected to change due to these treatment regimens. The radiologist making stereological measurements did not have any information about the nature of that study. For details about the subjects, the reader is directed to the original study [12]. In summary, these patients were on average 34.7 years of age with an average weight of 121.3 kg at baseline dropping to 113.9 kg after 1 month of low-calorie diet and finally 105.8 kg 1 month after gastric bypass. The caloric intake comprised 30 % protein, 49 % carbohydrates, and 21 % fat. Total calorie intake was set to total energy expenditure (as calculated by Harris-Benedict) minus 1,000 kcal/day (minimum 860 kcal/day). The study had been approved by the local ethics committee.
MRI
The patients had been imaged before any treatment (first MRI), after treatment with low-calorie diet (second MRI), and after gastric bypass surgery (third MRI). MRI was performed on a 1.5T clinical scanner (Achieva; Philips Healthcare, Best, The Netherlands). Imaging parameters were as follows: T1 weighted images: TR 5.9 ms, TE 1.36/3.22/5.09 ms, flip angle 3°, elementary signal sampling field of view (FOV) (in motion direction) 112 mm, virtual FOV 530 × 377 × 2,000 mm3, and voxel size 2.07 × 2.07 × 8.00 mm3. Imaging was in supine position with the arms extended above the head.
Reference method
Volumetric measurements were made by two independent readers, and the average of their measurements was used as reference. The average time for measuring each liver volume was 17.2 ± 6.5 min.
Statistical methods
For statistical analysis, dedicated software (SPSS for Windows, version 20.0.0) and Microsoft Excel 2003 were used. The measured volumes were compared to the results of the reference method by using paired t-test. Correlation curves between different stereological measurements and the reference method were drawn based on calculation of correlation coefficient and coefficient of variation. The Pearson’s correlation coefficient (r) was calculated to assess the strength of linear dependency. Bland-Altman curves were drawn, and the percentage by which cases differed from the reference method was calculated.
Results
The average liver volume measured on volumetry was 1,998 mL with a standard deviation (SD) of 319 mL. The results of liver volume measured by the stereology method using different grids are shown in Table 1. The table also shows the average time needed for stereological measurements, the correlation coefficients and 95 % confidence intervals for difference in volume measurements. The 3- and 4-cm grids provided measurement results that differed from the volumetric measurements by less than 300 mL. The mean differences from volumetric measurements were 37 and 3 mL for 3- and 4-cm grids, respectively.
Scatterplots and Bland-Altman curves are shown for each grid (Figs. 2 and 3). When comparing the stereological method with volumetry, there was no statistically significant difference in measurements of liver volume or of changes in liver volume (p > 0.05).

Scatterplots demonstrate relations between measured liver volume by a 3-, b 4-, c 5-, and d 6-cm grid stereology. The linear regression lines are also drawn

Bland-Altman curves showing differences in liver volume measured with stereology and volumetry related to average liver volume on a 3-, b 4-, c 5-, d 6-cm grids
The changes in liver volume before and after treatment are shown in Table 2. Bland-Altman curves demonstrating differences in liver volume change for 3-, 4-, 5-, and 6-cm grids are shown in Fig. 4.

Bland-Altman curves demonstrating differences in liver volume changes as assessed by volumetry and by stereology on a 3-, b 4-, c 5-, and d 6-cm grids
Discussion
Our study shows that stereological methods employing 3- and 4-cm grids give accurate results for measuring both liver volume and changes in liver volume. Grids of 5 and 6 cm may still be useful in certain situations, e.g., when groups of patients are compared.
Stereology has the advantage of being done within a reasonable time. Although we used computer software to identify the points and to direct the process, this is not necessary as a simple overhead paper or any transparent paper placed on the monitor or hard copy image is sufficient. Stereology therefore entails small costs and can be used if there is no access to semi-automated or fully automated volumetry software.
Stereology also offers the advantage of being neither signal intensity-dependent nor density-dependent as several other available programs are. It can therefore be used in combination with ultrasound, CT, MRI with any sequence, etc. as long as there is no bias in cross-sectioning. One can choose to include or exclude lesions, vascular structures, or specific liver segments. Aydinli and colleagues have used stereology to evaluate response in hepatic alveolar echinococcosis and found that simple volumetric measurements were in some cases unable to replace stereology [13]. Mazonakis and colleagues used stereology for measurement of malignant liver lesions and compared their results to planimetry and found comparable values [14]. Stereology is particularly useful when the shape of an object is bizarre and unpredictable such as for the measurement of hepatic iron stores [15].
There are some drawbacks to our study. One could question our reference method. This method, however, is the basis of an already published study [12] and is a reliable and acceptable method [16]. In fact one study has found stereology better than volumetry when compared to intra-operative liver volume measurements [17]. In another study, Doherty and colleagues were able to show that stereology was superior to semi-automated volumetry for measurement of the temporal lobe [18].
To date there is only one study looking into stereology for measurement of liver volume [19]. These authors found stereology to be a more efficient approach than planimetry with an excellent agreement between the two. They, however, used 1.6-, 2.5-, and 3.3-cm grids and changed the number of sections studied. Interestingly, they found a larger difference (8.5 mL) between measurements when patients with hepatomegaly were studied compared to patients with normal liver volume (2.4 mL).
Our measurements were done on 8-mm-thick sections. Reiner and colleagues have found that the results of CT- and MR-based liver volumetry are dependent on slice thickness. Best volume measurements when time was factored in were 6- and 8-mm slices for CT and MRI, respectively [20].
Another aspect not studied to the best of our knowledge is measurement of liver volume in other imaging planes. We, like other authors before us, used axial sections. The liver has a special shape, with the lower segments of the right lobe tapering down vertically, much like the shape of a cone. Measuring cylinders or cones on planes perpendicular to their axes can cause bias. The sampling idea behind stereologic methods is that over- and underestimations cancel each other out.
Conclusion
Stereological methods can be used for accurate liver volume measurements with a 4 × 4 cm grid in less than 2 min.
References
Hori M, Suzuki K, Epstein ML, Baron RL (2011) Computed tomography liver volumetry using 3-dimensional image data in living donor liver transplantation: effects of the slice thickness on the volume calculation. Liver Transpl 17(12):1427–1436
Perkins JD (2009) Another formula to determine the prognosis of patients with acute liver failure. Liver Transpl 15(8):986–991
Nakayama Y, Li Q, Katsuragawa S, Ikeda R, Hiai Y, Awai K, Kusunoki S, Yamashita Y, Okajima H, Inomata Y, Doi K (2006) Automated hepatic volumetry for living related liver transplantation at multisection CT. Radiology 240(3):743–748
Karlo C, Reiner CS, Stolzmann P, Breitenstein S, Marincek B, Weishaupt D, Frauenfelder T (2010) CT- and MRI-based volumetry of resected liver specimen: comparison to intraoperative volume and weight measurements and calculation of conversion factors. Eur J Radiol 75(1):e107–e111
Boyce RW, Dorph-Petersen KA, Lyck L, Gundersen HJ (2010) Design-based stereology: introduction to basic concepts and practical approaches for estimation of cell number. Toxicol Pathol 38(7):1011–1025
Kamp S, Jemec GB, Kemp K, Kjeldsen CR, Stenderup K, Pakkenberg B, Dam TN (2009) Application of stereology to dermatological research. Exp Dermatol 18(12):1001–1009
Mühlfeld C, Nyengaard JR, Mayhew TM (2010) A review of state-of-the-art stereology for better quantitative 3D morphology in cardiac research. Cardiovasc Pathol 19(2):65–82
Dockery P, Fraher J (2007) The quantification of vascular beds: a stereological approach. Exp Mol Pathol 82(2):110–120
Weibel ER, Hsia CC, Ochs M (2007) How much is there really? Why stereology is essential in lung morphometry. J Appl Physiol 102(1):459–467
Nyengaard JR, Gundersen HJ (2006) Direct and efficient stereological estimation of total cell quantities using electron microscopy. J Microsc 222(Pt 3):182–187
Torkzad M, Lindholm J, Martling A, Blomqvist L (2003) Retrospective measurement of different size parameters of non-radiated rectal cancer on MR images and pathology slides and their comparison. Eur Radiol 13(10):2271–2277
Kullberg J, Sundbom M, Haenni A, Freden S, Johansson L, Börnert P, Ahlström A, Ahlström H, Karlsson A (2011) Gastric bypass promotes more lipid mobilization than a similar weight loss induced by low-calorie diet. J Obes 2011:959–601
Aydinli B, Kantarci M, Polat KY, Unal B, Atamanalp SS, Durur I, Unal D, Akgun M (2006) Stereological evaluation of treatment response in patients with non-resectable hepatic alveolar echinococcosis using computed tomography via the Cavalieri method. Liver Int 26(10):1234–1240
Mazonakis M, Damilakis J, Mantatzis M, Prassopoulos P, Maris T, Varveris H, Gourtsoyiannis N (2004) Stereology versus planimetry to estimate the volume of malignant liver lesions on MR imaging. Magn Reson Imaging 22(7):1011–1016
Ghugre NR, Gonzalez-Gomez I, Shimada H, Coates TD, Wood JC (2010) Quantitative analysis and modelling of hepatic iron stores using stereology and spatial statistics. J Microsc 238(3):265–274
Yoshizumi T, Taketomi A, Kayashima H, Yonemura Y, Harada N, Ijichi H, Soejima Y, Nishizaki T, Maehara Y (2008) Estimation of standard liver volume for Japanese adults. Transplant Proc 40(5):1456–1460
Duran C, Aydinli B, Tokat Y, Yuzer Y, Kantarci M, Akgun M, Polat KY, Unal B, Killi R, Atamanalp SS (2007) Stereological evaluation of liver volume in living donor liver transplantation using MDCT via the Cavalieri method. Liver Transpl 13(5):693–698
Doherty CP, Fitzsimons M, Holohan T, Mohamed HB, Farrell M, Meredith GE, Staunton H (2000) Accuracy and validity of stereology as a quantitative method for assessment of human temporal lobe volumes acquired by magnetic resonance imaging. Magn Reson Imaging 18(8):1017–1025
Mazonakis M, Damilakis J, Maris T, Prassopoulos P, Gourtsoyiannis N (2002) Comparison of two volumetric techniques for estimating liver volume using magnetic resonance imaging. J Magn Reson Imaging 15(5):557–563
Reiner CS, Karlo C, Petrowsky H, Marincek B, Weishaupt D, Frauenfelder T (2009) Preoperative liver volumetry: how does the slice thickness influence the multidetector computed tomography- and magnetic resonance-liver volume measurements? J Comput Assist Tomogr 33(3):390–397
Author information
Authors and Affiliations
Corresponding author
Appendix 1
Appendix 1
Basics of stereology
When radiologists are asked to measure the volume of an object by volumetry, they trace the object of interest on their cross-sectional images, and the software normally returns several values including the area confined within the marked trace. By adding the areas obtained and multiplying them by slice thickness the volume is estimated.
Basically the area is measured by using software to count all the pixels inside the marked trace. Stereology is based on sampling methods to estimate volume or area measurements. Instead of counting all the pixels, it utilizes statistical methods to estimate area or volume. This is very similar to the way an epidemiologist uses a sample of the population to know about the whole population. The interested reader is referred to the references mentioned below.
Take Fig. 5 as an example. There is a cloud-shaped object, and we are interested in measuring its area. We have drawn a set of thick parallel horizontal lines and a set of vertical parallel dashed lines. Each set of parallel lines is equally spaced. Each point created by intersection of a dashed and a solid line represents a certain area that is equal to the distance between nearby horizontal lines times the distance between nearby vertical lines. By simply counting the number of the points that fall within the object, we can estimate the area of the whole cloud-shaped object.

A cloud-shaped object to illustrate the methodology of stereology
The lines do not need to be vertical and horizontal. The approach we chose in our study was similar to that shown in Fig. 5 with the exception that the distance between vertical lines was equal to the distance between horizontal lines (not a requirement).
Occasionally, the intersection might fall on the border of an object. Looking at the lower left corner of the object in Fig. 5, we see such an issue, as shown in Fig. 6. The intersecting lines create four corners. The person making the measurements will have chosen a corner in advance (before starting measurements) to be the focus of attention in cases such as this, and only one corner may be chosen. The radiologist in this study always chooses the upper right corner. If the corner formed by the intersecting lines contains the object, then the object is counted as being represented by the intersection point. Otherwise it is considered outside the object. In our particular example the object is therefore inside and thus counted.

In stereology, sometimes the intersection of the grid lines falls on the border of the object
References for stereology in medicine
MBF Biosciences (2012) Stereology information for the biological sciences. www.stereology.info
Mattfeldt T. A brief introduction to computer-intensive methods, with a view towards applications in spatial statistics and stereology. J Microsc. 2011 Apr; 242 (1): 1–9.
Eriksen N, Rostrup E, Andersen K, Lauritzen MJ, Fabricius M, Larsen VA, Dreier JP, Strong AJ, Hartings JA, Pakkenberg B. Application of stereological estimates in patients with severe head injuries using CT and MR scanning images. Br J Radiol. 2010 Apr; 83 (988): 307–17.
Mühlfeld C, Nyengaard JR, Mayhew TM. A review of state-of-the-art stereology for better quantitative 3D morphology in cardiac research. Cardiovasc Pathol. 2010 Mar-Apr; 19 (2): 65–82.
Boyce RW, Dorph-Petersen KA, Lyck L, Gundersen HJ. Design-based stereology: introduction to basic concepts and practical approaches for estimation of cell number. Toxicol Pathol. 2010; 38 (7): 1011–25.
Mayhew TM, Mühlfeld C, Vanhecke D, Ochs M. A review of recent methods for efficiently quantifying immunogold and other nanoparticles using TEM sections through cells, tissues and organs. Ann Anat. 2009 Apr; 191 (2): 153–70.
Weibel ER, Hsia CC, Ochs M. How much is there really? Why stereology is essential in lung morphometry. J Appl Physiol. 2007 Jan; 102 (1): 459–67.
Okur A, Kantarci M, Akgun M, Alper F, Cayir K, Koc M, Onbas O. Unbiased estimation of tumor regression rates during chemoradiotherapy for esophageal carcinoma using CT and stereology. Dis Esophagus. 2005; 18 (2): 114–9.
Mayhew TM. A review of recent advances in stereology for quantifying neural structure. J Neurocytol. 1992 May; 21 (5): 313–28.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Torkzad, M.R., Norén, A. & Kullberg, J. Stereology: a novel technique for rapid assessment of liver volume. Insights Imaging 3, 387–393 (2012). https://doi.org/10.1007/s13244-012-0166-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13244-012-0166-z