
Abstract
Background
The risk factors for ectopic pregnancy are on the rise. Despite the progress (availability of serum βhCG, USG and MRI), there are diagnostic and therapeutic challenges in the management. Up to 50% of ectopic pregnancies go undetected. Furthermore, cases seen as emergency with hemodynamic instability need urgent intervention with simultaneous arrangement of transport, blood transfusion and at times multidisciplinary team involvement. This is more challenging in a setting where resources are limited.
Objective
To evaluate the outcome of women presenting with uncommon ectopic pregnancies as life-threatening emergency. Challenges encountered in diagnosis, pre-operative evaluation, decision for surgery and the procedure are presented.
Patients and Methods
This is a series of twelve cases of uncommon ectopic pregnancies belonging to eight different types. These were managed under the first author during the period 2001 to 2019. Subjects were analyzed retrospectively.
Results
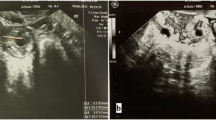
Diagnostic dilemma was faced in majority of the cases even with the use of ultrasonography. All the conceptions were spontaneous. Emergency surgical interventions were made on the basis of clinical evaluation. Five cases presented with massive hemoperitoneum. Blood transfusion was needed in nine cases. There was no mortality. One woman (case 4), with abdominal pregnancy, went home with a live baby, after the second laparotomy.
Conclusion
Uncommon ectopic pregnancies are life-threatening conditions. Clinical acumen and an alert mind are of superior value in diagnosis. Investigations are supportive. Early diagnosis and intervention are lifesaving.






Similar content being viewed by others


References
Tenore JL. Ectopic pregnancy. Am Fam Physician 2000; 61:1080–1088.1a.Chang J, Elam-Evans LD, Berg CJ, Herndon J, Flowers L, Seed KA et al. Pregnancy-related mortality surveillance – United States, 1991–1999. Morbidity and mortality weekly report Surveillance summaries (Washington, DC: 2002. 2003; 52(2):1–8.
ACOG Practise Bulletin No: 94: Medical management of ectopic pregnancy. Obstet Gynecol.2008; 111(6):1479-85.
Alkatout I, Honemeyer U, Strauss A, et al. Clinical diagnosis and treatment of ectopic pregnancy. Obstet Gynecol Surv. 2013;68:571–81.
Condous G, Okaro E, Khalid A, et al. The accuracy of transvaginal ultrasonography for the diagnosis of ectopic pregnancy prior to surgery. Hum Reprod. 2005;20:1404–9.
Worley KC, Hnat MD, Cunningham FG. Advanced extrauterine pregnancy: diagnostic and therapeutic challenges. Am J Obstet Gynecol. 2008;198:297–297.
Audain L, Brown WE, Smith DM, Clark JF. Cocaine use as a risk factor for abdominal pregnancy. J Natl Med Assoc. 1998;90:277–83.
Dutta DC (2000) Ectopic pregnancy; In: Emergencies in manipulative and operative obstetrics,(3rd edition) , New Central Book Agency, Kolkata, India.
Elizabeth H, Ana PL. Imaging unusual pregnancy implantations: rare Ectopic pregnancies and more. Am Roentgen Ray Soc. 2016;207:1380–92.
Ackerman TE, Levi CS, Dashefsky SM, et al. Interstitial line: sonographic finding in interstitial (cornual) ectopic pregnancy. Radiology. 1993;189:83–7.
Lau S, Tulandi T. Conservative medical and surgical management of interstitial ectopic pregnancy. Fertil Steril. 1999;72:207–15.
Downey GP, Tuck SM. Spontaneous uterine rupture during subsequent pregnancy following non excision of an interstitial ectopic gestation. Br J Obstet Gynaecol. 1994;101:162.
Vela G, Tulandi T. Cervical pregnancy : the importance of early diagnosis and treatment. J Minimum Invasive Gynecol. 2007;14:481.
Beddock R, Naepels P, Gondry C, et al. Diagnosis and current concepts of management of advanced abdominal pregnancy. Gynecol Obstet Fertil. 2004;32:55.
Verma R, Mascarenhas L, James D. Successful outcome of advanced abdominal pregnancy with exclusive omental insertion. Ultrasound Obstet Gynecol. 2003;21:192.
Cristalli B, Guichaoua H, Heid M, et al. Abdominal ectopic pregnancy: limits of laparoscopic treatment [in French]. J Gynecol Obstet Biol Reprod (Paris). 1991;21:751–3.
Raziel A, Schachter M, Mordechai E, et al. Ovarian pregnancy: a 12-year experience of 19 cases in one institution. Eur J Obstet Gynecol Reprod Biol. 2004;114:92–6.
Choi HJ, Im KS, Jung HJ, et al. Clinical analysis of ovarian pregnancy: a report of 49 cases. Eur J Obstet Gynecol Reprod Biol. 2011;158:87–9.
Spiegelberg O. Zur kasuistik der ovarialschwangerschaft. Arch Gynaekol. 1873;13:73–9.
Nahum GG. Rudimentary uterine horn pregnancy The 20th- century worldwide experience of 588 cases. J Reprod Med. 2002;47(2):151–63.
Hwang JH, Lee JK, Lee NW, Lee KW. Molar ectopic pregnancy in the uterine cornus. J Minimal Invas Gynecol. 2010;17(2):239–41.
Kagel T, Lemburg SP, Müller KM, et al. Mediastinal metastasis of a tubal choriocarcinoma following ectopic pregnancy as a rare cause of thoracic pain. Zentralbl Gynakol. 2006;128(2):90–4.
Osborn DA, Williams TR, Craig BM. Cesarean scar pregnancy: sonograph, magnetic resonance imaging findings, compilcations and management. J Ultrasound Med. 2012;31(9):1449.
Chou MM, Hwang JI, Tseng JJ, et al. Cesarean scar pregnancy: quantitive assessment of uterine neovascularisation with 3-dimentional color power Doppler imaging and successful treatment with uterine artery embolization. Am J Obstet Gynecol. 2004;190:866.
Ben Nagi J, Helmy S, Olifi-Ye bovi D et al. Reproductive outcomes of women with a previous history of Cesarean scar ectopic pregnancies, Hum Reprod 22: 2012, 2007.
Rolle CJ, Wai CY, Bawdon R, et al. Unilateral twin ectopic pregnancy in a patient with a history of multiple sexually transmitted infections. Infect Dis Obstet Gynecol. 2006;2006:10306.
Neuman WL, Ponto K, Farber RA, Shangold GA. DNA analysis of unilateral twin ectopic gestation. Obstet Gynecol. 1990;75:479–83.
Acknowledgments
The authors express their sincere gratitude to Sir, Sabaratnam Arulkumaran, Prof. Emeritus, St George’s University, London, Past President FIGO, BMA and RCOG, for his valuable guidance while writing this manuscript. We sincerely thank Prof. C.N. Purandare, Past President, FIGO, FOGSI and Dean ICOG for all his valuable guidance in writing the article. I thank Md Jakir Hossain for his assistance in manuscript and photographic presentation.
Funding
No funding was received.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare they have no conflict of interest.
Ethical approval
Ethical approval was taken from institutional ethics committee.
Ethical Standards
All procedures followed were in accordance with the ethical standards of the responsible committee on the human participants (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Informed Consent
Informed and written consent was obtained from all the eligible women. Additional informed consent was obtained from all individual participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Dr. Hiralal Konar, MBBS, MD, DNB, MNAMS, FACS (US), FRCOG (Lond), Prof and Head, Dept. OB-GYN: Agartala Govt. Medical College and GB Pant Hospital, Agartala,Tripura, India; Dr. Lisley Konar, MBBS, Resident (1st.Yr.M S), Dept OB-GYN, SDU, Academy of Higher Education and Medical Research, Karnataka, India; Dr. Chandrachur Konar, MS, DNB, Assistant Professor, Dept. OB-GYN. SDU Medical College, Karnataka, India; Dr Arindam Halder MBBS, MS, Associate Professor, Dept. OB-GYN, Dinajpur Medical College, West Bengal, India; Dr. Arindam Saha, MD, R.M.O cum Clinical Tutor, Dept. OB-GYN; N.R.S. Medical College, Calcutta, India; Dr. J. Khamaru, MD,Consultant Sonologist, Divine Nursingh Home, Calcutta, India.
Rights and permissions
About this article

Cite this article
Konar, H., Konar, L., Konar, C. et al. Uncommon Ectopic Pregnancies—Challenges in the Management. J Obstet Gynecol India 72 (Suppl 1), 224–234 (2022). https://doi.org/10.1007/s13224-021-01605-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13224-021-01605-8