
Abstract
Purpose of Review
This review will highlight advances in pregnancy of unknown location (PUL) management and advocate for incorporating desiredness and triaging of low-risk patients to less intensive follow-up when possible.
Recent Findings
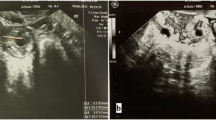
After the initial diagnosis of a PUL, fluid is sometimes seen inside the uterine cavity on transvaginal ultrasound. A retrospective study looked at the incidence of ectopic pregnancy in patients who have intrauterine fluid collections and found that the risk of ectopic pregnancy in this population is very low. For patients with PUL and an intrauterine fluid collection, a follow-up ultrasound in 1 week can be offered. For patients with undesired PULs, mifepristone and misoprostol can be given and has been shown to lead to shorter time to diagnosis and pregnancy resolution compared to establishing a final diagnosis prior to initiating medication abortion. However, abortion efficacy is lower in patients with undesired PULs. Therefore, medication abortion can be initiated in this population in the carefully selected patient and with close interval follow-up. Multiple algorithms exist and are available for clinicians to use to risk stratify patients with PUL; the M4 model was found in a systematic review to outperform other models. For patients with persistent PULs, active management is more successful at pregnancy resolution than expectant management.
Summary
Clinicians should provide active management to patients with undesired pregnancy of unknown location. Selected patients at low risk of ectopic pregnancy can be triaged to less intensive follow-up in order to reduce unnecessary blood-draws and visits.

Similar content being viewed by others

References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
ACOG Practice Bulletin No. 191: Tubal Ectopic Pregnancy. Obstet Gynecol. 2018;131(2):e65–77.
Barnhart K, van Mello NM, Bourne T, Kirk E, Van Calster B, Bottomley C, et al. Pregnancy of unknown location: a consensus statement of nomenclature, definitions, and outcome. Fertil Steril. 2011;95(3):857–66.
Brown DL, Doubilet PM. Transvaginal sonography for diagnosing ectopic pregnancy: positivity criteria and performance characteristics. J Ultrasound Med. 1994;13(4):259–66.
ACOG Practice Bulletin No. 193: Tubal Ectopic Pregnancy. Obstet Gynecol. 2018;131(3):e91–103.
• Lee IT, Rubin ES, Wu J, Koelper N, Barnhart KT. The incidence and importance of the pseudogestational sac revisited. Am J Obstet Gynecol. 2022;226(4):537.e1–e7. This retrospective cohort study sought to calculate the incidence of intrauterine fluid collections among patients presenting with pregnancy of unknown location who were ultimately diagnosed with ectopic versus intrauterine pregnancies. They found that the presence of an intrauterine fluid collection rarely was associated with an ectopic pregnancy.
• Volovsky M, Duarte Ayala MG, Narayanamoorthy S, Chiware TM, Kotlyar AM, Taylor HS, et al. A bedside test to detect the presence of embryonic or fetal tissue in vaginal blood. Obstet Gynecol. 2022;140(6):983–8. This prospective study aimed to validate a POC test (ROM plus) to detect fetal blood in patients presenting in early pregnancy with vaginal bleeding. The test strip had a sensitivity of 95.7% and a specificity of 97.7%. Showing potential that in patients with a positive result intensive serial follow up to rule out ectopic pregnancy is likely not necessary.
Santelli JS, Lindberg LD, Orr MG, Finer LB, Speizer I. Toward a multidimensional measure of pregnancy intentions: evidence from the United States. Stud Fam Plann. 2009;40(2):87–100.
Flynn AN, Schreiber CA, Roe A, Shorter JM, Frarey A, Barnhart K, et al. Prioritizing Desiredness in Pregnancy of Unknown Location: An Algorithm for Patient-Centered Care. Obstet Gynecol. 2020;136(5):1001–5.
Wu JK, Sadecki EN, Kyweluk MA, Senapati S, Flynn AN, Steider E, et al. Patient attitudes and preferences for the management of pregnancy of unknown location. F&S Reports. 2022;3(3):246–52.
• Goldberg AB, Fulcher IR, Fortin J, Hofer RK, Cottrill A, Dethier D, et al. Mifepristone and misoprostol for undesired pregnancy of unknown location. Obstet Gynecol. 2022;139(5):771–80. This retrospective cohort study set to compare immediate initiation of medication abortion versus delayed initiation among patients who had undesired pregnancies of unknown location. In the immediate start group there was quicker time to final diagnosis but lower abortion efficacy.
Shannon C, Brothers LP, Philip NM, Winikoff B. Ectopic pregnancy and medical abortion. Obstet Gynecol. 2004;104(1):161–7.
Barnhart K, Sammel MD, Chung K, Zhou L, Hummel AC, Guo W. Decline of serum human chorionic gonadotropin and spontaneous complete abortion: defining the normal curve. Obstet Gynecol. 2004;104(5 Pt 1):975–81.
Bobdiwala S, Kyriacou C, Christodoulou E, Farren J, Mitchell-Jones N, Al-Memar M, et al. Evaluating cut-off levels for progesterone, β human chorionic gonadotropin and β human chorionic gonadotropin ratio to exclude pregnancy viability in women with a pregnancy of unknown location: a prospective multicenter cohort study. Acta Obstet Gynecol Scand. 2022;101(1):46–55.
Seeber BE, Sammel MD, Guo W, Zhou L, Hummel A, Barnhart KT. Application of redefined human chorionic gonadotropin curves for the diagnosis of women at risk for ectopic pregnancy. Fertil Steril. 2006;86(2):454–9.
Cameron KE, Senapati S, Sammel MD, Chung K, Takacs P, Molinaro T, et al. Following declining human chorionic gonadotropin values in pregnancies of unknown location: when is it safe to stop? Fertil Steril. 2016;105(4):953–7.
Silva C, Sammel MD, Zhou L, Gracia C, Hummel AC, Barnhart K. Human chorionic gonadotropin profile for women with ectopic pregnancy. Obstet Gynecol. 2006;107(3):605–10.
Morse CB, Sammel MD, Shaunik A, Allen-Taylor L, Oberfoell NL, Takacs P, et al. Performance of human chorionic gonadotropin curves in women at risk for ectopic pregnancy: exceptions to the rules. Fertil Steril. 2012;97(1):101-6.e2.
• Bobdiwala S, Saso S, Verbakel J, Al-Memar M, Van Calster B, Timmerman D, et al. Diagnostic protocols for the management of pregnancy of unknown location: a systematic review and meta-analysis. BJOG: an International Journal of Obstetrics & Gynaecology. 2019;126(2):190–8. This prospective multicenter study investigated patients presenting with PUL and sought to validate a two-step protocol that included the M6 risk-prediction model. The majority of patients were appropriately triaged as low-risk of ectopic and thus shortened their intensive follow up period. Of the 320 patients ultimately diagnosed with an ectopic pregnancy, 15 were misclassified as low risk.
Van Calster B, Bobdiwala S, Guha S, Van Hoorde K, Al-Memar M, Harvey R, et al. Managing pregnancy of unknown location based on initial serum progesterone and serial serum hCG levels: development and validation of a two-step triage protocol. Ultrasound Obstet Gynecol. 2016;48(5):642–9.
Bobdiwala S, Christodoulou E, Farren J, Mitchell-Jones N, Kyriacou C, Al-Memar M, et al. Triaging women with pregnancy of unknown location using two-step protocol including M6 model: clinical implementation study. Ultrasound Obstet Gynecol. 2020;55(1):105–14.
Link CA, Maissiat J, Mol BW, Barnhart KT, Savaris RF. Diagnosing ectopic pregnancy using Bayes theorem: a retrospective cohort study. Fertility and Sterility. 2022.
•• Barnhart KT, Hansen KR, Stephenson MD, Usadi R, Steiner AZ, Cedars MI, et al. Effect of an active vs expectant management strategy on successful resolution of pregnancy among patients with a persisting pregnancy of unknown location: the ACT or NOT randomized clinical trial. JAMA. 2021;326(5):390–400. This multicenter randomized clinical trial sought to determine if active management is more effective in achieving pregnancy resolution than expectant management for persistent pregnancy of unknown location and if empirical methotrexate is non-inferior to uterine evacuation followed by methotrexate if needed for persistent pregnancy of unknown location. Patients who were randomized to active management were more likely to experience successful pregnancy resolution than those randomized to expectant management. This study also found that empiric methotrexate was non-inferior to diagnostic uterine evacuation followed by methotrexate for patients with persistent pregnancy of unknown location.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Flynn has nothing to disclose.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Flynn, A.N. Updates in the Management of Pregnancy of Unknown Location: A Focus on Expediting and Streamlining Care. Curr Obstet Gynecol Rep 12, 64–69 (2023). https://doi.org/10.1007/s13669-023-00355-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13669-023-00355-w