
Abstract
Prevalence of fluorosis is mainly due to the consumption of more fluoride through drinking water. It is necessary to identify the fluoride endemic areas to adopt remedial measures for the people under the risk of fluorosis. The objectives of this study were to identify the exact location of fluoride endemic areas in Manur block of Tirunelveli District and to estimate fluoride exposure level through drinking water for different age groups. Identification of fluoride endemic areas was performed through Isopleth and Google earth mapping techniques. Fluoride level in drinking water samples was estimated by fluoride ion selective electrode method. A systematic clinical survey conducted in 19 villages of Manur block revealed the rate of prevalence of fluorosis. From this study, it has been found that Alavanthankulam, Melapilliyarkulam, Keezhapilliyarkulam, Nadupilliyarkulam, Keezhathenkalam and Papankulam are the fluoride endemic villages, where the fluoride level in drinking water is above 1 mg/l. Consumption of maximum fluoride exposure levels of 0.30 mg/kg/day for infants, 0.27 mg/kg/day for children and 0.15 mg/kg/day for adults were found among the respective age group people residing in high fluoride endemic area. As compared with adequate intake level of fluoride of 0.01 mg/kg/day for infants and 0.05 mg/kg/day for other age groups, the health risk due to excess fluoride intake to the people of Alavanthankulam and nearby areas has become evident. Hence the people of these areas are advised to consume drinking water with optimal fluoride to avoid further fluorosis risks.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fluoride is an essential oligo-element, beneficial for the development of bone and teeth (McDonagh et al. 2000; Boulétreau et al. 2006; Messaitfa 2008). World Health Organization and Indian Council of Medical Research described the drinking water quality guideline value for fluoride is 1.5 mg/l (World Health Organization (WHO) 1963; Indian Council of Medical Research (ICMR) 1975). Intake of large quantities of fluoride through drinking water than the optimal safe level is the primary reason for the prevalence of dental and skeletal fluorosis in various parts of world (Chowdhury and Shepherd 1990; Gopalakrishnan et al. 1991; Infante 1975; Gopalakrishnan and Mebrahtom 2006; 2011; Zhu et al. 2006; Karro et al. 2006). Fluorosis is a slow, progressive, crippling malady, which affects every organ, tissue and cell in the body and results in health complaints along overlapping manifestations with several other diseases. Dental fluorosis is characterized by lusterless, opaque white patches in the enamel, which may become stained yellow to dark brown, and in severe forms cause marked pitting and brittleness of teeth. Dental fluorosis is sensitive to even small changes in fluoride exposure from drinking water, and this sensitivity is greater at 1–3 years of age than at 4 or 5 years (Burt et al. 2000). Fluoride is present in water as almost completely dissociated fluoride ion from the parent compounds occurring either naturally or in the form of added salts (Jackson et al. 2002; Harrison 2005). Bioavailability of soluble fluoride is largely controlled by acidity in the stomach. Thus, the systemic fluoride absorption from water through the gastrointestinal tract into bloodstream is nearly 100 % by the process of simple diffusion without any intervention of overall water quality (Ekstrand et al. 1978; Rao 1984; Whitford 1994; Whitford 1996; Cerklewski 1997; Maguire et al. 2005; Doull et al. 2006). Hence, water fluoride level is the primary reason for the cause of fluorosis. Fluoride intake from water depends on the amount of water ingested by itself and the quantity of water ingested through food by means of water used for cooking and their fluoride content (Kahama et al. 1997; Karro and Rosentau 2005; Martin 1951; Onyango et al. 2004; Levy 1994; Viswanathan et al. 2009a, 2010). However, studies indicate that while total fluid intake increases with age and the intake of drinking water decreases after increase of age (Galagan et al., 1957). Fluoride intake level through drinking water itself decreases with increase of age; moreover, 50 % of the total fluoride intake per day is derived from food and beverages (Viswanathan et al. 2009a, b). Many of the previous studies, from various parts of the world, reported the development of dental fluorosis even if the people consume drinking water with fluoride less than 1.0 mg/l, (Riordan 1993; Clark 1994; Ibrahim et al. 1995; Heller 1997) which implies that the optimal fluoride dose level in drinking water may vary with various features like local climatic conditions, methods of food processing and cooking, (Galagan and Vermillion 1957; Galagan et al. 1957; Khan et al. 2004), amount of food and water intake and its fluoride and other nutrients’ level and dietary habits of the community (Danielsen and Gaarder 1955; Cao et al. 2000; Kaseva 2006). About 80 % of the diseases in world are due to poor quality of drinking water, and the fluoride contamination in drinking water is responsible for 65 % of endemic fluorosis around global (Felsenfeld and Robert 1991; World Health Organization (WHO) 2002). Furthermore, 50 % of the ground water sources in India have been contaminated by fluoride and more than 90 % of rural drinking water supply programmes are based on ground water. A variety of standards and guidelines for exposure to fluoride have been recommended to aid in the protection against dental caries and/or the development of adverse health effects. The National Research Council has estimated “adequate and safe” daily fluoride intakes to be 0.1–0.5 mg for infants less than 6 months of age, 0.2–1.0 mg for infants between 6 and 12 months, 0.5–1.0 mg for children between the ages of 1 and 3 years, 1.0–2.5 mg for 4- to 6-year-old children, 1.5–2.5 mg for children from 7 years to adulthood and 1.5–4.0 mg for adults (National Research Council, NRC 2001). The prevalence of fluorosis in man is reported from 22 states of India, affecting more than 40 million people (Teotia and Teotia 1991; Chinoy 1991; Srikanth et al. 1994; Susheela 2000). The global prevalence of fluorosis is reported to be about 32 % (Mella et al. 1994). The number of people getting affected, the number of villages, blocks, districts and states endemic for fluorosis have been steadily increasing ever since the disease was discovered in India during 1930s. Many of the people in Manur block of Tirunelveli District, Tamil Nadu, are affected by dental fluorosis. In order to find out the quantitative rate of prevalence of fluorosis and to determine the magnitude of fluoride exposure dose through drinking water among different age groups of people in Manur block, an extensive investigation was performed by estimating fluoride level in drinking water and through clinical survey. Identification of exact geographical location of high fluoride exposed area is much useful to perform remedial measures and is helpful to give awareness about fluorosis to the villagers residing in the particular area. Mapping of fluoride endemic areas is facilitated using Google Earth, because it displays satellite images of most inhabited regions of Earth, allowing users to visually see the exact location with geographical information.
Methods and materials
In order to identify the fluoride endemic areas, a total of 65 drinking water samples were randomly collected from 19 villages in Manur block of Tirunelveli District, Tamil Nadu, for fluoride analysis. Each sample collected from a particular village is identified by a different symbol. The collected samples were stored in polyethylene bottles and stored at ≤10°C in a refrigerator before the analysis. Villages in Manur block were classified into three categories such as normal area, medium fluoride endemic area and high fluoride endemic area where the drinking water fluoride level lower than 1.0, 1–2 and above 2.0 mg/l, respectively.
Clinical survey was conducted among the people and school children of different age groups and gender residing in the villages of Manur block. The percentage incidence of fluorosis was calculated from the number of people affected by fluorosis from the respective area with total number of people surveyed. A total of 2,879 school children aged between 5 and 14 years and 3,272 villagers within the age group of 25–70 were randomly selected and examined for this study. This clinical survey including 19 schools and 19 villages located in Manur block of Tirunelveli District. According to Dean’s classification, persons with dental fluorosis on permanent teeth were identified and characterized with the help of two practicing dentists under day light in regular chair (Viswanathan et al. 2009b).
Fluoride levels in drinking water samples were measured by using Orion fluoride ion selective electrode using total ionic strength adjustment buffer (TISAB II). The instrument was calibrated with standard fluoride solutions so chosen that the concentration of one was ten times the concentration of the other and also that the concentration of the unknown falls between those standards. Then the concentration of the unknown was directly read from the digital display of the meter (Fluoride Electrode Instruction Manual 1991).
The fluoride exposure dose was calculated by the following generic equation:
where C is the fluoride concentration (mg/l), WI is the amount water intake per day (l/day) and BW is the body weight (kg). The water intake level of different age groups was accounted through household survey. Infants in their budding life drank 250 ml of boiled water per day. In boiled water, fluoride level increases proportionally to the loss of volume, so the concentration of fluoride in tap water is doubled (Grimaldo et al. 1995; Viswanathan et al. 2009b). The estimated water intake for children and adult was 1.5 and 3.0 l/day, respectively. For the calculation, body weight of infants in the age group of 0–6 months was kept as 6 kg and of children aged between 7 years to adulthood as 20 kg and that of adults above 19 years as 70 kg. The mean of minimum and maximum range of water fluoride level in each block was used for minimum and maximum exposure dose calculation.
Based on the results of fluoride level in drinking water samples, Google earth satellite images of exact location of fluoride endemic areas were prepared using Google Earth 6.1 Beta. The exact location of normal and fluoride endemic areas with scale is displayed in Table 1. Isopleths mapping also performed to locate the high fluoride endemic areas with information about the water fluoride level. Fluoride zones containing high fluoride levels in their drinking water were identified and distinguished by different symbols (Fig. 1).

Location of normal and fluoride endemic areas in Manur block of Tirunelveli district, Tamil Nadu, India
Results
Prevalence of fluorosis and water fluoride level
Fluoride levels in drinking water samples collected from 19 villages in Manur block of Tirunelveli are presented in Table 2. As per the fluoride level, villages of Alavanthankulam and Pappankulam are categorized as high fluoride endemic areas (F2). Melapilliyarkulam, Keezhapilliyarkulam, Nadupilliyarkulam, Keezhathenkalam are categorized as medium fluoride endemic areas (F1) and the other villages (Table 2) with optimum fluoride level are considered as normal areas (N). The rate of prevalence of fluorosis among school children and villagers in Manur block of Tirunelveli District are illustrated in Tables 3 and 4, respectively. The percentage of prevalence of fluorosis among the surveyed school children and villagers in Manur block is 28 and 33 %, respectively.
Nearly 26 % of children and 58 % of villagers residing in high fluoride endemic areas are severely affected by dental fluorosis. Almost 41 % of children and 33 % of villagers in medium fluoride endemic areas are affected by dental fluorosis. About 29 % of school children and 31 % of villagers in normal areas are having mild dental fluorosis symptoms. Among the school children 16 % of boys and 13 % of girls are affected by fluorosis. In villagers of Manur block 19 % of men and 14 % of women are affected by dental fluorosis. The range of drinking water fluoride level in normal area is from 0.1 to 1.00 mg/l. The maximum fluoride level in drinking water in medium fluoride endemic area is 2.00 mg/l, and 3.6 mg/l in Alavanthankulam where totally 281 people are affected by dental fluorosis out of the 818 surveyed. Hence, this region is considered as the high fluoride endemic area.
Fluoride endemic areas and fluoride exposure
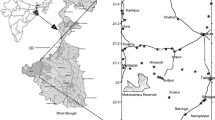
The exact location of Manur block of Tirunelveli District in South India is shown in Fig. 2. Normal and fluoride endemic areas situated in Manur block of Tirunelveli District are located in Fig. 3. The high fluoride endemic area is displayed in Fig. 4. The maximum range of fluoride exposure dose through drinking water for infants from normal to high fluoride endemic areas is from 0.18 to 1.80 mg per day, respectively. Children residing in normal areas are exposed to almost 0.05 mg/kg/day of fluoride and adults were exposed to 0.03 mg/kg/day of fluoride. The mean fluoride exposure levels for infants, children and adults in medium fluoride endemic areas are 0.07, 1.2 and 2.4 mg/day, respectively. In high fluoride endemic area, infants, children and adults are exposed to daily fluoride intake as high as 1.4, 4.2 and 8.4 mg, respectively. Ranges of fluoride exposure dose levels based on the average body weight of the various age groups of people are illustrated in Table 5. The maximum range of fluoride exposure dose level is recorded in infants in high fluoride endemic area ranges from 0.11 to 0.30 mg/kg/day. Daily fluoride exposure dose levels of various age groups of people in areas with different water fluoride level are shown in Fig. 5.

Location of Manur Block of Tirunelveli District, Tamil Nadu, South India

Location of normal and fluoride endemic areas in Manur block of Tirunelveli

Location of high fluoride endemic areas in Manur block of Tirunelveli district, Tamil Nadu, India

Mean fluoride intake level through drinking water for various age groups
Discussion
The rate and extent of fluorosis in Manur block of Tirunelveli District increases with increase of fluoride level in drinking water and age. Ground water is the main drinking water source of these selected study areas. Abnormal level of fluoride in ground water is common in fractured hard rock zone with pegmatite veins (Ramesam and Rajagopalan 1985). Fluoride ion from these minerals that leached into the ground water may contribute to high fluoride concentrations in the drinking water sources (Schultheiss and Godley 1995). The results indicate that the school children in the age group of 514 years and village people in the age group of 25–70 years are equally affected by dental fluorosis. The extent of prevalence of fluorosis among school children is higher in boys than in girls; correspondingly, men in fluoride endemic areas are highly affected by fluorosis than women. Previous study also reported that boys are more susceptible to fluorosis (Mann et al. 1990). It has not been proved that fluorosis is sex-dependent but nutritional habits, especially breast feeding, climatic conditions, play a major role in the prevalence and severity of fluorosis. As regards the study area, the weather condition of Tirunelveli district is warmest than the nearby areas. Normally the people residing in warm areas consume more drinking water. Moreover, boys and men consume more water than girls and women, which enhances the daily fluoride intake level among boys and men in the study area. Children residing in fluoride endemic areas are exposed to more fluoride. Many of the previous studies reported a significant inverse-concentration–response relationship between the fluoride level in drinking water and the intelligence quotient (IQ) of children. As the fluoride level in drinking water increases the IQ falls and the rates of mental retardation and borderline intelligence increase (Li et al. 1995; Zhao et al. 1996; Xiang et al. 2003). Prevalence of fluorosis due to the consumption of more fluoride through drinking water among children may also adversely affect the foetal cerebral function and neurotransmitters (Yu et al. 1996; Zhang and Zhu 1998; Shi and Dai 1990; Chen et al. 1990). The present study reveals that two remote villages of Manur block of Tirunelveli District, namely Alavanthankulam and Pappankulam are the high fluoride endemic areas. The drinking water fluoride levels in these villages are as high as 3.6 and 2.00 mg/l, respectively. Identification and prediction of exact location of fluoride endemic villages through mapping of fluoride endemic areas are highly useful to government agencies for supplying water with optimal fluoride level, installing defluoridation plants and for conducting awareness creation programmes. Illustration of fluoride endemic areas with information about the fluoride level in Manur block of Tirunelveli District is presented in Fig. 1. Infants in Manur block of Tirunelveli District are highly exposed to fluoride than children and adults. Especially, infants in high fluoride endemic areas are exposed to fluoride through drinking water by nearly 30 times more (Table 5) than the recommended level of 0.01 mg/kg/day (Agency for Toxic Substances and Disease Registry (ATSDR) 1993; Food and Nutrition Board 1997; National Research Council, NRC 2001). Drinking water is an important path way for fluoride exposure, since the presence of nearly 100 % bioavailable soluble fluoride (Jackson et al. 2002; Maguire et al. 2005). Apart from drinking water, infants commonly consume milk and powder-based milk formulae; Milk is known to interfere with the rate of fluoride absorption. Milk and milk products diminish the fluoride availability through gastrointestinal tract by 20–50 % in human, due to the presence of high calcium concentrations (Spak et al. 1982; Trautner and Sibert 1986; Whitford 1996). Milk is also rich in fats, which increase the lag time of the food or beverage in the stomach (Trautner and Sibert 1986; Whitford 1996). Moreover, the rate of prevalence of fluorosis among the milk-consuming children is lower than that of non-milk-consuming children (Chen et al. 1997). Even though the people in normal areas consume less fluoride through drinking water, they are showing dental fluorosis symptoms mainly because of using tea, coffee, infant formulae and fluoridated tooth paste. The fluoride exposure dose level decreases with increase of age group from infants to adults. The results of the present study are highly associated with the previous report (Viswanathan et al. 2009a). In villages of Manur block, people consume sorghum (Sorghum bicolor) and Pearl millet (Pennisetum typhoides) as the chief staple foods. It has been already found that intake of diets based on sorghum and Pearl millet resulted in significant increase in retention of fluoride; mean increase in retention being 12.2 % as compared with diets based on rice at identical intake of fluoride (Lakshmaiah and Srikantia 1977). This fact has been attributed to the presence of higher amount of molybdenum in sorghum than rice. Sorghum contains high levels of molybdenum as compared with other cereals (Deosthale et al. 1977). High molybdenum intake is known to cause secondary deficiency of copper, an essential element for bone development (Arthur 1965). It is also observed that copper deficiency along with high fluoride intake is associated with high prevalence of genu valgum (Krishnamachari and Krishnaswamy 1973; Krishnamachari 1976, 1986). Absorption of fluoride from food is more complicated and a variety of dietary factors can either increase or decrease the amount of fluoride absorption (Ericsson 1968; Cremer and Buttner 1970; Whitford 1994; Cerklewski 1997; Ozsvath 2009). In humans, the bioavailability of fluoride from various food items was reported to vary from 2 to 79 %. Parameters like pH and mineral content of the food are the important factors on the bioavailability of fluoride through food (Ekstrand et al. 1978; Spak et al. 1982, Shulman and Vallejo 1990; Goyal et al. 1998). Children and adults in high fluoride endemic areas are highly exposed to fluoride through drinking water, as much as 50 and 30 times more than the recommended level of 0.05 mg/kg/day.
Conclusions
This present study identified two fluoride endemic villages in Manur block of Tirunelveli District, where the drinking water fluoride level is higher than the recommended safe level. Hence, it is recommended that the government authorities take serious steps to supply drinking water with low fluoride to the identified fluoride endemic villages in Manur block of Tirunelveli, Tamilnadu, South India. The exact locations of fluoride endemic areas are identified using Google Earth and Isopleths techniques to help the Government adopt remedial measures to the people under the risk of fluorosis in that particular area. Commonly all the age groups of people in the identified areas are highly exposed to fluoride beyond the recommended safety levels. The fluoride exposure dose level through drinking water decreases with increase in age from infants to adults. Based on the study, the people in fluoride endemic areas are advised to use water with safe level of fluoride content for drinking and cooking and to use rice-based diet with rich calcium instead of using sorghum-based diet to avoid further risks of fluorosis.
References
Agency for Toxic Substances and Disease Registry (ATSDR) (1993) A toxicological profile for fluorides, hydrogen fluoride, and fluorine. US Department of Health and Human Services, Atlanta, p 112
Arthur D (1965) Inter-relationships of molybdenum and copper in the diet of guinea pigs. J Nutr 87:69–76
Boulétreau PH, Bost M, Fontanges E, Lauverjat M, Gutknecht C, Ecochard R, Delmas PD, Chambrier C (2006) Fluoride exposure and bone status in patients with chronic intestinal failure who are receiving home parenteral nutrition. Am J Clin Nutr 83:1429–1437
Burt BA, Keels MA, Heller KE (2000) The effects of a break in water fluoridation on the development of dental caries and fluorosis. J Dental Res 79:761–769
Cao J, Yan Z, Jianwei L (2000) Fluoride in the environment and brick-tea-type fluorosis in Tibet. J Fluor Chem 160:93–97
Cerklewski FL (1997) Fluoride bioavailability—nutritional and clinical aspects. Nutr Res 17(5):907–929
Chen Z, Liu W, Su GA (1990) study of the effect of fluoride on foetus tissue. Chin J Endemiol 9:345–346
Chen YX, Lin MQ, Xiao YD, Gan WM, Min D, Chen C (1997) Nutrition survey in dental fluorosis affected areas. Fluoride 30(2):77–80
Chinoy NJ (1991) Effect of fluoride on physiology of animals and human beings. Ind J Environ Toxicol 1(1):17–32
Chowdhury NG, Shepherd MG (1990) Fluoride intake of infants in New Zealand. J Dent Res 69(12):1828–1833
Clark DC (1994) Influence of exposure to various fluoride technologies on the prevalence of fluorosis. Commun Dent Oral Epidemiol 22:61–464
Cremer HD, Buttner W (1970) Absorption of fluorides. In: Fluorides and human health. WHO monograph no. 59. World Health Organization, Geneva, pp 75–91
Danielsen ME, Gaarder T (1955) Fluorine content of drinking-water and food in western Norway, the Bergen district. Arbok Nat Recke 5:1
Deosthale YG, Krishnamachari KAVR, Belavady B (1977) Copper, molybdenum, and zinc in rice, sorghum, and Pearl-millet grains from fluorosis and non-fluorosis areas of Andhra Pradesh. Ind J Agric Sci 47:333–335
Doull J, Boekelheide K, Farishian BG, Isaacson RL, Klotz JB, Kumar JV (2006) Fluoride in drinking water: a scientific review of EPA’s standards. In: Committee on fluoride in drinking water. Board on Environmental Studies and Toxicology, Division on Earth and Life Sciences, National Research Council of the National Academies. National Academies Press, Washington, DC, p 530
Ekstrand J, Ehrnebo M, Boreus LO (1978) Fluoride bioavailability after intravenous and oral administration: importance of renal clearance and urine flow. Clin Pharmacol Therap 23:329–337
Ericsson Y (1968) Influence of sodium chloride and certain other food components on fluoride absorption in the rat. J Nutr 96:60–68
Felsenfeld AJ, Robert MA (1991) A report of fluorosis in the United States secondary to drinking well water. J Am Med Assoc 265(4):486–488
Fluoride Electrode Instruction Manual (1991) Orion Res Inc, USA, pp 4–9
Food and Nutrition Board (1997) Institute of medicine. National Academic Press, Washington, DC, pp 190–249
Galagan DJ, Vermillion JR (1957) Determining optimum fluoride concentrations. Public Health Rep 72:491–493
Galagan DJ, Vermillion JR, Nevitt GA, Stadt ZM, Dart RE (1957) Climate and fluoride intake. Public Health Rep 72:484–490
Gopalakrishnan S, Mebrahtom K (2006) Prevalence of fluorosis in certain villages of Ghindae area of Eritrea, North East Africa-suggestions for prevention and control. Ind J Environ Protect 26:202–207
Gopalakrishnan S, Viswanathan G (2011) Assessment of fluoride-induced changes on physicochemical and structural properties of bone and the impact of calcium on its control in rabbits. J Bone Miner Metab. doi:10.1007/s00774-011-0312-6
Gopalakrishnan S, Narasimhan S, Seenipandian C (1991) Incidence of fluorosis in 10 villages near Tuticorin—suggestions for prevention and control. Ind J Environ Protect 11(2):118–123
Goyal A, Gaupa K, Tewari A (1998) Bioavailability of fluoride in human from commonly consumed diets in India. J Ind Soc Pedod Prev Dent Dis 16:1–6
Grimaldo M, Borja V, Ramirez AL, Ponce M, Rosas M, Diaz-Barriga F (1995) Endamic fluorosis in San Luis Potosi, Mexico.I. Identification of risk factors associated with human exposure to fluoride. Environ Res 68:25–30
Harrison PTC (2005) Fluoride in water: a UK perspective. J Fluor Chem 126:1448–1456
Heller KE (1997) Dental caries and dental fluorosis at varying water fluoride concentrations. J Publ Health Dent 57:136–143
Ibrahim YE, Affan AA, Bjorvatn K (1995) Prevalence of dental fluorosis in Sudanese children from two villages with 0.25 and 2.5 ppm fluoride in the drinking water. Int J Paediatr Dent 5:223–229
Indian Council of Medical Research (ICMR) (1975) Manual of standards of quality for drinking water supplies. In: Special report series, 2nd edn, New Delhi, India, p 44
Infante PF (1975) Dietary fluoride intake from supplements and communal water supplies. Am J Dis Child 129:835–837
Jackson PJ, Harvey PW, Young WF (2002) Chemistry and bioavailability aspects of fluoride in drinking water. Report No.05037, 27. Henley Road, Medenham, Marlow, Bucks, SL7 2HD: WRC-NSF Ltd 5-9
Kahama RW, Kariuki DN, Kariuki HN, Njenga LW (1997) Fluorosis in children and sources of fluoride around Lake Elementaita region of Kenya. Fluoride 30(1):19–25
Karro E, Rosentau A (2005) Fluoride levels in the Silurian-Ordovician aquifer system of western Estonia. Fluoride 38:307–311
Karro E, Indermitte E, Saava A, Haamer K, Marandi A (2006) Fluoride occurrence in publicly supplied drinking water in Estonia. Environ Geol 50:389–396
Kaseva ME (2006) Contribution of trona (madadi) into excessive fluorosis—a case study in Maji ya Chai ward, Northern Tanzania. Sci Tot Environ 366:92–100
Khan AA, Whelton H, O’Mullane D (2004) Determining the optimal concentration of fluoride in drinking water in Pakistan. Commun Dent Oral Epidemiol 32:166–172
Krishnamachari KAVR (1976) Further observations on the syndrome of endemic genu valgum of South India. Ind J Med Res 64:284–292
Krishnamachari KAVR (1986) Skeletal fluorosis in humans: a review of recent progress in the understanding of the disease. Prog Food Nutr Sci 10:279–314
Krishnamachari KAVR, Krishnaswamy K (1973) Genu valgum and osteoporosis in an area of endemic fluorosis. Lancet 2:877–879
Lakshmaiah N, Srikantia SG (1977) Fluoride retention in humans on sorghum and rice based diets. Ind J Med Res 65:543–548
Levy SM (1994) Review of fluoride exposures and ingestion. Commun Dent Oral Epidemiol 22(3):173–180
Li XS, Zhi JL, Gao RO (1995) Effect of fluoride exposure on intelligence in children. Fluoride 28(4):189–192
Maguire A, Zohouri FV, Mathers JC, Steen IN, Hind march PN, Moynihan PJ (2005) Bioavailability of fluoride in drinking water: a human experimental study. J Dental Res 84(11):989–993
Mann J, Mahmoud W, Ernest M, Sgan-cohen H, Shoshan N, Gedalia I (1990) Fluorosis and dental caries in 6–8 year-old children in a 5 ppm area. Commun Dent Oral Epidemiol 18:77–79
Martin DJ (1951) The Evanston dental caries study VIII. Fluorine content of vegetables cooked in fluorine containing waters. J Den Res 30:676–681
McDonagh MS, Whiting PF, Wilson PM, Sutton AJ, Chestnutt I, Cooper J, Misso K, Bradley M, Treasure E, Kleijnen J (2000) Systematic review of water fluoridation. Br Med J 321:855–859
Mella S, Molina X, Atalah E (1994) Prevalence of dental fluorosis and its relation with fluoride content of public drinking water. Rev Méd Chile 122(11):1263–1270
Messaitfa A (2008) Fluoride contents in ground waters and the main consumed foods (dates and tea) in Southern Algeria region. Environ Geol 55:377–383
National Research Council (NRC) (2001) National Academics Press. Washington, DC, USA
Onyango MS, Kojima Y, Aoyi O, Bernardo EC, Matsuda H (2004) Adsorption equilibrium modelling and solution chemistry dependence of fluoride removal from water by trivalent-cation exchanged zeolite F-9. J Colloid Interface Sci 279:341–350
Ozsvath DL (2009) Fluoride and environmental health: a review. Rev Environ Sci Biotechnol 8(1):59–79
Ramesam V, Rajagopalan KJ (1985) Fluoride ingestion into the natural waters of hard-rock areas, peninsular India. J Geol Soc 26:125–132
Rao GS (1984) Dietary intake and bioavailability of fluoride. In: Darby WJ (ed) Annual review of nutrition, vol. 4. Annual Review, Inc, Palo Alto, pp 115–136
Riordan PJ (1993) Dental fluorosis, dental caries and fluoride exposure among 7 year olds. Caries Res 27:71–77
Schultheiss WA, Godley GA (1995) Chronic fluorosis in cattle due to the ingestion of a commercial lick. J South Afr Veterinary Assoc 66(2):83–84
Shi J, Dai G (1990) A study of the effects of fluoride on the human foetus in an endemic fluorosis area. Chung Hua Liu Hsing Ping Hsueh Tsa Chih 9:10–12
Shulman ER, Vallejo M (1990) Effect of gastric contents on the bioavailability of fluoride in humans. Pediatr Dent 12:237–240
Spak CJ, Ekstrand J, Zylberstein D (1982) Bioavailability of fluoride added to baby formula and milk. Caries Res 16:249–256
Srikanth R, Khanam A, Rao AMM (1994) Fluoride in borehole water in selected villages of Medak district, Andra Pradesh, India. Fluoride 27:93–96
Susheela AK (2000) A treatise on fluorosis. Fluorosis Research and Rural Development Foundation. New Delhi, pp 1–119
Teotia SPS, Teotia M (1991) Endemic fluoride: bones and teeth—update. Ind J Environ Toxicol 1(1):1–16
Trautner K, Sibert G (1986) An experimental study of bioavailability of fluoride from dietary sources in man. Arch Oral Biol 31(4):223–228
Viswanathan G, Jaswanth A, Gopalakrishnan S, Siva ilango S (2009a) Mapping of fluoride endemic areas and assessment of fluoride exposure. Sci Tot Environ 407(5):1579–1587
Viswanathan G, Jaswanth A, Gopalakrishnan S, Siva ilango S, Aditya G (2009b) Determining the optimal fluoride concentration in drinking water for fluoride endemic regions in South India. Sci Total Environ 407(20):5298–5307
Viswanathan G, Gopalakrishnan S, Siva ilango S (2010) Assessment of water contribution on total fluoride intake of various age groups of people in fluoride endemic and non-endemic areas of Dindigul District, Tamil Nadu, South India. Water Res 44:6186–6200
Whitford GM (1994) Intake and metabolism of fluoride. Adv Dental Res 8(1):5–14
Whitford GM (1996) The metabolism and toxicity of fluoride. In: Monographs in oral science, vol 12–15. Karger, Basel, pp 46–58
World Health Organization (WHO) (1963) International standards for drinking water, 2nd edn, Geneva
World Health Organization (WHO) (2002) Environmental health criteria, vol 227. Fluorides. Geneva, pp 1–251
Xiang Q, Liang Y, Chen L, Wang C, Chen B, Chen X, Zhou M, Shanghai PR (2003) Effect of fluoride in drinking water on children’s intelligence. Fluoride 36(2):84–94
Yu Y, Yang W, Dong Z (1996) Changes in neurotransmitters and their receptors in human foetal brain from an endemic fluorosis area. Chung Hua Liu Hsing Ping Hsueh Tsa Chih 15:257–259
Zhang A, Zhu D (1998) Effect of fluoride on the human foetus. Chin J Endem Prev Treat 13:156–158
Zhao LB, Liang GH, Zhang DH, Wu XR (1996) Effect of a high fluoride water supply on children’s intelligence. Fluoride 29(4):190–192
Zhu C, Bai G, Liu X, Li Y (2006) Screening high fluoride and high arsenic drinking water and surveying endemic fluorosis and arsenism in Shaanxi province in western China. Water Res 40:3015–3022
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Gopalakrishnan, S.B., Viswanathan, G. & Siva Ilango, S. Prevalence of fluorosis and identification of fluoride endemic areas in Manur block of Tirunelveli District, Tamil Nadu, South India. Appl Water Sci 2, 235–243 (2012). https://doi.org/10.1007/s13201-012-0043-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13201-012-0043-4