
Abstract
Introduction
Bisexual individuals experience discrimination both from heterosexual individuals and from the Lesbian and Gay (LG) community. This double discrimination affects their mental health. This study aimed to explore the relationship between binegativity (from heterosexual and LB individuals) and internalized binegativity and symptoms of depression and anxiety, as well as the mediating role of social support. The second purpose was to explore whether these variables could predict the symptoms of depression and anxiety.
Methods
A sample of 110 bisexual individuals (77.3% cisgender women, Mage = 25.2) completed self-report measures.
Results
Most participants reported being discriminated against by heterosexual (93.2%) and LG (81.8%) individuals. However, they perceived and experienced higher discrimination from heterosexual people. The majority experienced internalized binegativity. As hypothesized, heterosexual discrimination predicted depressive and anxiety symptoms. Contrary to expectations, discrimination from the LG community and internalized binegativity did not predict symptoms, although bivariate correlations showed a positive relationship. Social support was a moderator of symptoms of depression, but not of anxiety.
Conclusions
These findings highlight the impact of binegativity on the mental health of bisexual individuals and the importance of social support.
Policy implications
Our results provide practitioners and policymakers with evidence of the effects of discrimination experienced by bisexual individuals. Educational campaigns and public awareness programs are needed to foster a more inclusive and accepting society.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Bisexual individuals are likely to encounter stigma and discrimination based on their sexual orientation throughout their lives. Between 18.8% of bisexual men and 9.1% of bisexual women report episodes of verbal violence (Nebot-García et al., 2019); 17.5% of bisexual women have experienced sexual violence (Sanz-Barbero et al., 2021) and are more likely to experience intimate partner violence (59.8%) than lesbians (46.3%) (Chen et al., 2020). This chronic experience of discrimination can increase the risk of developing mental health problems such as depression, anxiety, isolation, and suicide attempts (Arnett et al., 2019; McDermott et al., 2018; Newcomb & Mustanski, 2010).
This higher incidence of psychological issues in bisexual individuals has been explained through the Minority Stress Model (Brooks, 1981; Meyer, 2003). This model states that sexual minorities experience additional stress compared to the general population, which stems from their increased exposure to discrimination, social stigma, and hostility. Concretely, bisexual individuals are exposed to two types of stressors linked to their sexual orientation: distal or objective stressors (e.g., harassment, discrimination, violence, marriage inequality) and proximal or subjective stressors (e.g., internalization of negative attitudes toward one's orientation, expectations of rejection). Hatzenbuehler (2009) created a psychological framework that merged a Minority Stress Model with common psychological processes. According to the author, distal and proximal stressors amplify maladaptive coping strategies and emotional regulation mechanisms (e.g., rumination, social isolation, hopelessness, and negative schemas), thereby increasing the risk of psychopathology. Therefore, proximal stressors, along with maladaptive psychological processes, mediate between distal stressors and mental health outcomes.
In this context, bisexual individuals may be more vulnerable to mental health issues because they face discrimination and social stigma (binegativity or anti-bisexual discrimination) from heterosexual and LG individuals (Doan Van et al., 2019; Nemtay & Hines, 2020). In other words, they experience binegativity from both within and outside the community, which has been denominated double discrimination (Ochs, 1996). Binegativity is associated with social prejudice due to the dichotomous conception of sexual orientation (Eliason, 2000; Zivony & Lobel, 2014). Stereotypical views surrounding bisexuality are associated with microaggressions, including dismissal of identity (i.e., bisexuals as promiscuous and confused; bisexuality is an illegitimate sexual orientation), mistrust (i.e., "bisexual individuals as untrustworthy partners," "bisexuals are sexually irresponsible"), and hypersexualization (Grove, 2022; Schulz et al., 2023). Consequently, bisexual people report a higher number of adverse psychosocial experiences, including daily microaggressions (Flanders, 2015) and interpersonal violence, such as childhood abuse, violence, and rejection by family and friends (Feinstein & Dyar, 2017; Johnson & Grove, 2017; Jorm et al., 2002). Previous studies indicate gender differences in binegativity, suggesting that bisexual men experience more binegativity than bisexual women, particularly by heterosexual men (Manalastas et al., 2023; Yost & Thomas, 2012). This can be attributed to two reasons. First, because of the sexual objectification and fetishization of the identity of bisexual women by heterosexual men (Serpe et al., 2020). Research on binegativity has shown that heterosexual men tend to perceive bisexual men and women differently, holding negative attitudes toward men but positive, albeit sexist, attitudes toward women (Dyar et al., 2014). For example, Yost and Thomas (2012) found that heterosexual men labeled bisexual men as "really gay," whereas they described bisexual women as "sexy." Second, the binegative attitudes of heterosexual men may stem from their perceived deviation of bisexual men from traditional masculinity (Hertlein et al., 2016). Conversely, heterosexual women show less binegativity toward both bisexual men and women (Eliason, 2000). Although LG individuals have fewer negative attitudes toward bisexual people, they are not exempt from them, especially toward bisexual men (Dyar et al., 2014; Friedman et al., 2014). These experiences of binegativity make bisexual individuals less likely to disclose their sexual orientation to others (Schrimshaw et al., 2018).
In addition to distal stressors, bisexual individuals face unique proximal stressors, one of which is internalized binegativity. Internalized binegativity is defined as "negative perceptions and biases about both one's bisexual identity and the concept of bisexuality in general" (Pollitt & Roberts, 2021, p. 2). It has been associated with worse mental health outcomes, including depression, anxiety, self-harm, lower self-esteem, and reduced social support (Meyer, 2003). Social support has been described as a protective factor against mental health problems (Mei et al., 2022) and stigma (Friedman et al., 2014). It has been associated with better adaptation to stressful factors (Schmitt et al., 2014) and with resilience (Salim et al., 2019), as it improves self-efficacy (Wang et al., 2020), self-esteem (Shi, 2022), and life satisfaction (Alshammari et al., 2021). In fact, lack of social support appears to be associated with more severe psychiatric symptoms (Morina et al., 2021). In the case of LGB youth, Ryan et al. (2009) found that those who reported family rejection were 5.9 times more likely to experience depression and 8.4 times more likely to attempt suicide. Similarly, Hegna and Wichstrøm (2007) found that a lack of parental support was associated with suicide attempts among LGB youth. In this scenario, bisexual individuals tend to report less social support than LG and their heterosexual peers (Friedman et al., 2014), which could, in turn, lead to a higher risk of developing psychological problems (Brewster & Moradi, 2010; Feinstein & Dyar, 2017). While previous research has explored the role of social support, there is limited information on the impact of different types of social support (i.e., parental or friend support) on mental health.
All the factors mentioned above underscore the impact of distal and proximal stressors on the mental health of sexual minorities (Hatzenbuehler, 2009; Meyer, 2003). Despite the singularity of these stressors and their effects on mental health, research concerning their impact among bisexual people is scarce compared to LG individuals (Brewster & Moradi, 2010). In addition, while the double discrimination faced by bisexual people is frequently described in informal contexts, studies exploring this issue empirically are limited.
Therefore, the present study aimed to investigate the impact of anti-bisexual discrimination on mental health and the effects of proximal and distal stressors by addressing the following questions:
-
(a)
Is there an association between internalized binegativity and social support (parents and friends’ support) and depression and anxiety?
-
(b)
Is bisexual discrimination (from heterosexual people and the LG community) associated with internalized binegativity and social support?
-
(c)
To what extent do these variables (internalized binegativity and social support) predict the symptoms of anxiety and depression?; and
-
(d)
Is social support (parents and friends) a protective factor against the impact of distal and proximal stressors?
Methods
Participants
The initial sample was composed of 128 participants, but 18 were excluded because they did not satisfy the inclusion criteria (a) by not disclosing their sexual orientation (n = 13) and (b) by not identifying as bisexuals (n = 5). The final sample consisted of 110 participants, ranging in age from 18 to 63 years (M = 25.2, SD = 8.3). Participants identified themselves as follows: 75.5% (n = 83) cisgender women, 20% (n = 25) cisgender men, 1.8% (n = 2) transgender men, and 2.7% (n = 3) were non-binary. The entire sample self-identified as bisexual. Most of the participants were white (97.3%) and university students (60.9%). Sociodemographic characteristics are detailed in Table 1.
Procedure
The sample was recruited using different sampling methods in December 2022 and May 2023, including: (a) social media posts (i.e., Twitter); (b) the collaboration of students from the University of Córdoba (Spain); and (c) the collaboration of Spanish LGBTQ (Lesbian, Gay, Bisexual, Transgender, and Queer) organizations contacted via email. The estimated response rate was 20.8%. Participants completed an informed consent form in which the aims of the study were explained. This study was approved by the Ethics Committee of the University of Córdoba, Spain (CEIH-23–11).
Measures
Anti-Bisexual Experiences Scale (ABES;Brewster & Moradi, 2010)
The Anti-Bisexual Experiences Scale (ABES) is a self-report tool used to assess the perception of prejudice experienced by individuals who identify as bisexual. It is composed of two subscales: (a) the ABES-H for prejudice by heterosexual individuals (e.g., "Heterosexual people have excluded me from social networks because I am bisexual"), and (b) the ABES-LG for prejudice by gay/lesbian individuals (e.g., "Gay/lesbian people have treated me negatively because I am bisexual"). Each subscale has 17 items that explore three types of adverse experiences: sexual orientation instability (SOI), sexual irresponsibility (SI), and interpersonal hostility (IH) on a 6-point Likert scale (1 = "never" to 6 = "almost all the time"). No specific cutoff score has been established; therefore, higher scores on the scale indicate a greater perception of experienced prejudice (scores range from 17 to 102). In the current sample, Cronbach's alpha ranged from good to excellent for all subscales, ranging from 0.86 to 0.96.
Internalized Binegativity
Internalized binegativity was measured using items from various instruments. Five items were selected from the Internalized Homonegativity subscale of the Lesbian, Gay, and Bisexual Identity Scale (Mohr & Fassinger, 2000). These items were adapted for bisexual individuals by Sheets and Mohr (2009) (e.g., "Bisexual lifestyles are not as satisfying as heterosexual/LG ones"). The estimated internal consistency of this subscale was 0.77. Five items from the internalized binegativity subscale of the Bisexual Identity Inventory (Paul et al., 2014) were used (e.g., "Being bisexual prevents me from having meaningful intimate relationships"). The internal consistency of this subscale ranged from 0.73 to 0.93. Finally, two items were explicitly created because of the lack of available items from validated scales (i.e., "I feel guilty for being bisexual" and "Sometimes I wish I were not bisexual"). These items were designed to explore guilt and the desire to change sexual orientation, two themes commonly described in the literature on internalized binegativity. To this end, the items were initially proposed and discussed by the authors (i.e., appropriate wording, validity) until a consensus was reached.
The 12 items were rated on a 7-point Likert scale (1 = "Strongly disagree" to 7 = "Strongly agree"). There is no specific cut-off score; therefore, higher scores indicate higher levels of internalized binegativity (ranging between 12 and 84).
Social Support from Parents and Friends Scale (AFA-R; González-Ramírez & Landero-Hernández, 2014)
This self-report is composed of 14 items that evaluate two subscales: (a) parental support (e.g., "You have someone in your family to talk to when you need it") and (b) friend support (e.g., "You trust a friend to talk about things that worry you"). Each item is rated on a 5-point Likert scale (1 = "Never" to 5 = "Almost always"). The scale does not have a defined cutoff point; thus, total scores range from 14 to 70 with higher scores indicating greater perception of social support. Cronbach's alpha for the scale was 0.92.
Beck Depression Inventory (BDI-II; Beck et al., 1996)
Beck Depression Inventory (BDI) is a self-report measure of depressive symptoms. The scale comprises 21 items that assess several aspects of depression, including mood, pessimism, sense of failure, self-dissatisfaction, guilt, punishment, suicidal thoughts, and sadness. The items are rated on a scale of 0 to 3 based on symptom intensity. Beck et al. (1996) suggested the following cut-off scores for depression: 0–13 = minimal depression; 14–19 = mild depression; 20–28 = moderate depression; 29–63 = severe depression). The BDI has been validated in different populations, including psychiatric outpatients, college students, clinical and non-clinical adults, battered women, and veterans, and has excellent consistency (α = 0.93).
Beck Anxiety Inventory (BAI; Beck et al., 1988)
The Beck Anxiety Inventory (BAI) assesses the symptoms of anxiety. It consists of 21-items rated on a 4-point Likert scale (0 = "Not at all" to 3 = "Severely, I could hardly bear it") that measures two factors corresponding to cognitive and somatic symptoms. According to Beck et al. (1988), the cut-off scores for this scale are: 0–7 = minimal anxiety, 8–15 = mild anxiety, 16–25 = moderate anxiety, and 26–63 = severe anxiety. The BAI showed good internal consistency (α = 0.92).
Statistical Analyses
All analyses were performed using SPSS 28. First, descriptive statistics were performed for sociodemographic data. Descriptive statistics and the Wilcoxon W-test were conducted to characterize binegative experiences. The homogeneity and normality tests revealed that only one variable (social support) was normally distributed. However, this variable was marginally nonsignificant (p = 0.053). Therefore, nonparametric tests were performed. The distribution of all variables (i.e., ABES-H, ABES-LG, internalized binegativity, AFA-R, BDI, BAI) was positively skewed. Concerning kurtosis, ABES-H, AFA-R, and BDI showed a platykurtic distribution (i.e., kurtosis < 0), and the ABES-LG, internalized binegativity, and the BAI showed a leptokurtic distribution (i.e., kurtosis > 0). The association between the variables was explored through bivariate correlations (Spearman's Rho), while the predictive model was performed using multiple linear regressions (MLR) with "enter" method test. The independent variables in the MLR were (a) discrimination by heterosexuals and LG; (b) internalized binegativity; and (c) social support. The dependent variables were depression and anxiety. All models were tested for multicollinearity using the variance inflation factor (< 5), eigenvalue (> 0.05), and condition index (< 15). No multicollinearity was observed among the variables.
Results
Experiences of Binegativity and Symptoms of Depression and Anxiety
Most of the participants reported having been discriminated against by heterosexuals (n = 108, 93.2%) and LG (n = 90, 81.8%), according to their answers to the ABES. Participants perceived more discrimination committed by heterosexual people (W = -6.657, p < 0.001). Moreover, according to the means obtained in each subscale, bisexual people endured greater discrimination from heterosexual individuals (M = 45.5) than from LG individuals (M = 33.3). Concerning the different types of bisexual discrimination, participants reported more experiences of prejudice from heterosexual individuals than from LG individuals in “sexual orientation instability” (Mheterosexual = 26.0 vs. MLG = 19.1), “sexual irresponsibility” (Mheterosexual = 9.9 vs. MLG = 6.8), and “interpersonal hostility” (Mheterosexual = 9.5 vs. MLG = 7.3). A total of 75.5% (n = 83) of the participants experienced internalized binegativity.
Depression was generally mild (M = 17.46, SD = 13.08). Among the participants, 34% (n = 34) obtained scores that indicated moderate depression and 18% (n = 20) had severe depression. Similarly, the mean values for anxiety were mild (M = 14.41, SD = 11.47). Participants with moderate anxiety scores represented 34.26% (n = 37) and 14.81% (n = 16) with severe anxiety.
Correlation Analyses
Social support was the only variable that showed a normal distribution. The results were marginally nonsignificant (p = 0.053); therefore, nonparametric tests were performed. A positive correlation was found between heterosexual and LG discrimination, internalized binegativity, and symptoms of anxiety and depression. A negative correlation was found between social support and depression, but not with anxiety (Table 2).
Subscale analyses were performed to explore potential differences in the type of anti-bisexual sentiments and the role of different types of social support on depression and anxiety (Table 3).
Concerning the specific prejudices that comprise the bisexual discrimination scale (ABES), significant positive correlations were found between prejudices from heterosexual individuals (sexual orientation instability, sexual irresponsibility, and interpersonal hostility), depression, and anxiety. However, discrimination from lesbian and gay individuals was only correlated with depression in the case of prejudices concerning sexual irresponsibility and interpersonal hostility. Anxiety only correlated negatively with interpersonal hostility, but not with the rest of the variables.
Regarding social support (AFA-R), significant negative correlations were found between social support from friends and depression; however, no relationship with anxiety was found. Nevertheless, social support from parents was negatively correlated with both depression and anxiety.
Analysis of the Relationship of the Predictor Variables
It was hypothesized that discrimination, internalized binegativity, and social support could predict the symptoms of depression and anxiety. Multiple linear regression (MLR) was used to test this model.
Relationship Between the Predictor Variables and Depression.
The results showed that discrimination by heterosexuals (ABES-H) and by LG individuals (ABES-LG), internalized binegativity, and social support (AFA-R) accounted for 27.9% (R2) of the symptoms of depression (BDI-II). Since the ANOVA was significant [F(4, 105) = 10.16, p < 0.001], a MLR analysis was conducted. ABES-H and AFA-R were significant predictors (β = 0.23, p = 0.004 and β = -0.50, p < 0.001, respectively), and the intercept (constant) of BDI-II in the MLR was 35. Symptoms of depression were positively predicted by ABES-H but negatively predicted by AFA-R. Nonsignificant variables (ABES-LG and internalized binegativity) were removed from the model, and the model was recalculated to improve its precision and predictive value. In the recalculated model, the independent variables ABES-H and AFA-R accounted for 27.4% (R2) of the dependent variables. As the ANOVA was significant [F(2, 107) = 20.19, p < 0.001], a MLR analysis was conducted. ABES-H and AFA-R were significant predictors (β = 0.19, p = 0.003 and β = -0.50, p < 0.001, respectively), and the intercept (constant) of BDI-II in the MLR was 35 in the MLR. ABES-H positively predicted depression, while AFA-R negatively predicted it.
To explore whether different types of anti-bisexual discrimination predicted depression symptoms, a model with these variables (i.e., sexual orientation instability, sexual irresponsibility, and interpersonal hostility) was tested. The ANOVA result was significant [F(6, 103) = 3.425, p = 0.004]. The only variable that predicted depression was the prejudice “sexual orientation instability” by heterosexual individuals (β = 0.47, p = 0.005). Similarly, different types of social support (i.e., parents vs. friends) were examined. The ANOVA was significant [F(2, 107) = 24.87, p < 0.001]. Parental support negatively predicted symptoms of depression (β = -1.06, p < 0.001).
Relationship Between Predictor Variables and Anxiety
The independent variables (ABES-H, ABES-LG, social support, and internalized binegativity) accounted for 19.6% (R2) of anxiety symptoms (BAI). Since the ANOVA was significant [F(4, 105) = 6.39, p < 0.001], a MLR analysis was conducted. The ABES-H was significant (β = 0.27, p < 0.001), whereas the intercept (constant) of the BAI in the MLR was 6.38. ABES-H positively predicted anxiety. Variables that did not show significance (ABES-LG, social support, and internalized binegativity) were removed from the model and the model was recalculated to improve its precision and enhance its predictive value. Following this modification, the independent variable ABES-H accounted for 16.8% (R2) of the dependent variable. As the ANOVA was significant [F(1, 108) = 21.81, p < 0.001], a MLR analysis was conducted. The ABES-H was significant (β = 0.27, p < 0.001), and the intercept (constant) of the BAI in the MLR was 2.35. Finally, the ABES-H score positively predicted anxiety.
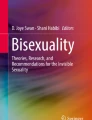
To explore whether different types of bisexual discrimination predicted symptoms of anxiety, a model with these variables (i.e., sexual orientation instability, sexual irresponsibility, and interpersonal hostility) was tested. The ANOVA was significant [F(6, 103) = 4.420, p < 0.001]. The only variable that predicted depression was “sexual orientation instability” from heterosexual individuals (β = 0.36, p = 0.012). Different types of social support (i.e., parents vs. friends) were examined. The ANOVA result was significant [F(2, 107) = 6.90, p = 0.002]. Parents’ support negatively predicted anxiety symptoms of anxiety (β = -0.61, p < 0.001). A final predictive model was established (Fig. 1).

Predictive model of the influence of proximal and distal stressors on mental health
Discussion
This study examined the impact of several distal and proximal stressors (anti-bisexual discrimination, IB, and social support) on the severity of anxiety and depressive symptoms. As hypothesized, participants reported discrimination from heterosexual and LG people, but was higher from heterosexuals (Arnett et al., 2019; Friedman et al., 2014). The results showed that binegativity stemming from heterosexual and LG individuals was associated with symptoms of anxiety and depression, which is consistent with previous studies (Dyar & London, 2018; Keating & Muller, 2020). When different types of discrimination were examined, the results showed that all prejudice from heterosexual individuals were positively associated with depression and anxiety. However, in relation to LG discrimination, only “sexual irresponsibility” and “interpersonal hostility” were associated with depression and interpersonal hostility with anxiety. Internalized binegativity was positively associated with symptoms of depression and anxiety, which is consistent with the concept of proximal stressors described by Hatzenbuehler (2009). As expected, social support was negatively correlated with depression, which may reflect its role as a protective factor. Regarding different types of social support, friends' support was negatively correlated with depression but not with anxiety. However, parental support was negatively correlated with both depression and anxiety. Thus, interventions should focus on providing social support, especially encouraging parental support due to its protective role that seem to reduce the impact of discrimination and improve mental health among members of the bisexual community.
These results partly support the hypothesis that distal stressors (i.e., anti-bisexual discrimination, internalized binegativity, and social support) predict depressive and anxiety symptoms. In this vein, the only variable that predicted the symptoms of depression and anxiety was antibisexual discrimination from heterosexual individuals. Concerning specific prejudices, “sexual orientation instability” was the only variable that predicted anxiety and depression but only when it stemmed from heterosexual individuals. While the role of anti-bisexual discrimination is aligned with previous studies (Arnett et al., 2019; Friedman et al., 2014), our results concerning the role of binegativity from LG individuals on internalized binegativity differ from previous literature (Pond & Farvid, 2017; Sarno et al., 2020). Internalized binegativity has been associated with negative psychological outcomes, including depressive symptoms, anxiety (Gibbs & Goldbach, 2015), higher rates of substance use disorders and other mental health problems (Hatzenbuehler et al., 2008), and suicidal ideation (Pachankis et al., 2018). Although these findings suggest that internalized binegativity may contribute to poor mental health outcomes for bisexual individuals, our results do not support its role as a predictive factor for worse mental health outcomes, contrary to previous research (Hatzenbuehler, 2009). It is important to note that our participants reported limited discrimination experiences from LG individuals (the scores obtained by the participants on the internalized binegativity scale were mild). Therefore, the scarcity of such experiences may diminish their predictive power. Nevertheless, the lack of experiences of binegativity from LG individuals could be due to several reasons. The first possible explanation lies in the demographic characteristics of our sample: college students with high social support, educated, and referring to low levels of general binegativity. Second, the participants were not asked about their engagement or connection with a broader LG community; thus, they may have had limited experience with LG individuals, which could explain their lack of opportunities to experience binegativity. Finally, a third possible explanation is the lack of a validated scale to measure internalized binegativity, which may have influenced the results. Internalized binegativity was evaluated using items from different scales and two items specifically elaborated upon for the aims of the study. Consequently, the items utilized may not be exhaustive enough to explore internalized binegativity.
Social support was a moderating variable for depression, which is consistent with the findings of previous studies. Research has highlighted the role of social support in the well-being of bisexual individuals, especially when facing societal negativity and biphobia (Mohr et al., 2009), as it can help bisexual individuals develop a stronger and more positive bisexual identity, improve their coping skills, and enhance their well-being (Gupta & Thyloth, 2021; Mohr et al., 2009). Social support was not associated with anxiety. Although this may be counterintuitive, previous studies have reported similar results (Kim, 2014), in which "social support assists with symptoms of depression, but not necessarily with anxiety (Sharpley et al., 2015, p. 883). A possible explanation for this may be the characteristics of the measures used to explore anxiety symptoms. Although the BAI is one of the most widely used scales worldwide to assess anxiety (Sanz, 2014), it is not exempt from limitations, including (a) the type of symptoms it assesses (predominantly somatic) and (b) it measures the severity of an individual's anxiety during the previous week. Consequently, individuals presenting with more cognitive symptoms or long-term symptoms may be overlooked. When different types of social support were examined, the results showed that parental support negatively predicted both depression and anxiety, while support from friends did not. Our findings suggest the importance of considering different types of social support when examining this variable in relation to mental health outcomes. Additionally, the positive impact of parental support demonstrates the importance of promoting interventions focused on family support and accompaniment. According to previous studies, parental support is associated with positive mental health outcomes among bisexual individuals, including affirmed identity (Taylor & Neppl, 2023) and increased resilience (Salim et al., 2019).
Limitations
Despite the importance of the findings, this study has certain limitations that may affect the generalization of the results. First, convenience sampling may have increased the homogeneity of the sample in terms of age, gender, and race (i.e., most of the sample was composed of cisgender women, white, and young). Future studies should explore binegativity in more heterogeneous samples, particularly with regard to race and ethnicity. Second, the measure used to explore Internalized Binegativity was not validated; thus, it may have contributed to our findings. In addition, the authors created two items without prior validation. Future research should advocate the development and validation of instruments to assess Internalized Binegativity. Third, the participants were not asked about their engagement or connection with LG individuals. Thus, the low level of discrimination reported by our participants could be explained by their limited interactions with LG individuals. Future studies should explore participants' connections with LB individuals. Fourth, cross-sectional and correlational studies are not exempt from limitations because they do not allow causal relationships. While the predictive design facilitates the establishment of possible cause–effect relationships, longitudinal designs should be used in future studies. Fifth, the sample size of this study was small. However, due to the specificity of the sample and the difficulty in accessing it, it may be sufficient to meet the objectives of the study. Additionally, our sample included a small percentage of bisexual men (22%). Future research should explore this issue using larger samples, including endeavors to recruit more bisexual men.
Policy Implications
These findings have significant implications for practitioners and policy makers. Psychological research has shown the detrimental effects of discrimination on sexual minorities. However, it is important to note that bisexual discrimination can arise from both heterosexual and LG individuals. Although our results indicate that only discrimination from heterosexual people predicted depression and anxiety, discrimination from LG individuals positively correlated with anxiety and depression. Thus, comprehensive anti-discrimination policies, educational campaigns, and public awareness programs should be present across settings -not just LGBTQ focused ones- so as to reach heterosexual individuals who may not be as informed about sexual identities relative to someone who belongs to the LGBTQ community. Efforts should focus on challenging prejudiced attitudes and promoting empathy, respect, and understanding among individuals with diverse sexual orientations.
Although we did not find a significant influence of LG discrimination on bisexual individuals, more research is needed in light of perceived experiences reported in informal contexts. This study highlights the importance of providing social support to bisexual individuals. Social support is negatively correlated with depression, indicating its potential as a protective factor against mental health problems. Policies should encourage the development and implementation of support networks, community organizations, and counseling services tailored to the needs of the bisexual community because of the specific forms of violence they experience and unique societal aggressions such as "double discrimination" (Mulick & Wright, 2002). An example of a successful experience in promoting social support can be found in Genders and Sexualities Alliances (GSAs). GSAs are "student-run organizations that unite LGBTQ and allied youth to build community and organize around issues impacting them in their schools and communities" (GSA Network, 2023). Previous studies have reported the benefits associated with implementing GSAs in schools, including a safe space to discuss relevant topics for LGBTQ youth, such as mental and sexual health issues, access to resources and information (Poteat et al., 2017), and a reduction in discrimination and violence (Steck & Perry, 2016). These initiatives should not only advocate the creation of safe and inclusive spaces (Porta et al., 2017) but also provide resources for individuals to access social support from friends, family and peers who understand their unique experiences. Research has shown that promoting contact between heterosexual, LG, and bisexual individuals reduces binegativity by improving intergroup attitudes (Lytle et al., 2017). While these initiatives have proven to be effective for LGBTQ youth, there is no evidence of their effect on lesbian-gay youth, bisexual youth, and transgender youth. This lack of evidence may be attributed to the fact that the LGBTQ community has been conceptualized as a homogenous group, neglecting the unique needs and experiences of its members. Consequently, more research that keep the identities distinct is needed.
It is also crucial to address internalized binegativity among bisexuals because our study suggests that it is positively associated with symptoms of depression and anxiety. Policies should prioritize the provision of mental health services that target internalized binegativity and promote positive bisexual identity development. This can be achieved through psychoeducation, therapy, and support groups that promote self-acceptance, challenge negative beliefs, and build resilience among bisexual individuals. However, it is essential to consider that internalized binegativity stems from recurrent experiences of anti-bisexual discrimination. Thus, it is essential to promote positive social attitudes towards the bisexual community due to their experience of double discrimination. In this vein, in addition to strategies such as GSAs, it is necessary to implement national regulations aimed at protecting sexual minorities and normalizing diversity. An example of how national politics can change the social reality of the bisexual community can be found in Spain. According to the LGBT + Pride 2021 Global Survey (IPSOS, 2021), 80% of the population identify as heterosexual, 3% as LGB, and 4% as bisexual. In Spain, the rates are slightly higher, with 5% of people identifying as gay (compared to 3% in the United States) and 6% as bisexual (the same for the US). Spain has been recognized as one of the most advanced countries regarding LGBTQ legislation (e.g., being the third country in the world to formally legalize same-sex marriages nationwide in 2005, approving the law for the equality of transgender people, and guaranteeing LGBTI rights in 2023). This legislation has placed Spain as the fourth European country on the ILGA Rainbow Map (2023) and is ranked 3 on the IGLYO Inclusive Education Index (2022). However, despite the advancements in LGBTQI policies, bisexual individuals continue to experience high levels of discrimination, from both heterosexual and LG individuals. This demonstrates that discrimination is an issue that needs to be continually addressed, even in places that are objectively progressive.
Furthermore, policy initiatives should consider an intersectional approach to effectively address the mental health needs of sexual minorities. It is essential to recognize and understand the intersecting identities and experiences of individuals, such as those based on race, ethnicity, socioeconomic status and gender identity, as these factors can compound the effects of discrimination and influence access to support systems. Policies must be inclusive, culturally sensitive, and tailored to the diverse needs of sexual minorities. Despite significant advances in the study of LGBTQ-specific needs that have promoted the development of research, prevention, and intervention programs, bisexual-specific policies and strategies are scarce. It is also important to continue investigating bisexuality to raise awareness of their unique stressors and needs, which differ from the needs of the broader Lesbian, Gay, Transgender, and Queer community. Diverse sexual orientations and gender identities have traditionally been studied as a whole, but research has shown that bisexuals have specific needs due to the unique stressors they face (i.e., stereotypes and discrimination from within and outside the LGBTQ community). It is essential to develop more research on bisexual-specific needs to open the "dialogue about how to develop best practices to advance bisexual health equity" with programs such as Bi Us, For Us (Beach & Hall, 2020, p. 251) or educational resources such as the "Roadmap to Bisexual Inclusion" (Rankin & Hiwatari, 2018).
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Alshammari, A., Piko, B., & Fitzpatrick, K. (2021). Social support and adolescent mental health and well-being among Jordanian students. International Journal of Adolescence and Youth, 26, 211–223. https://doi.org/10.1080/02673843.2021.1908375
Arnett, J. E., Frantell, K. A., Miles, J. R., & Fry, K. M. (2019). Anti-bisexual discrimination as insidious trauma and impacts on mental and physical health. Psychology of Sexual Orientation and Gender Diversity, 6(4), 475–485. https://doi.org/10.1037/sgd0000344
Beach, L. B., & Xavier Hall, C. D. (2020). Bi Us, For Us: Articulating foundational principles for research in partnership with bisexual communities. Journal of Bisexuality, 20(3), 251–272. https://doi.org/10.1080/15299716.2020.1841478
Beck, A. T., Epstein, N., Brown, G., & Steer, R. A. (1988). An inventory for measuring clinical anxiety: Psychometric properties. Journal of Consulting and Clinical Psychology, 56(6), 893–897. https://doi.org/10.1037/0022-006X.56.6.89
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck Depression Inventory–II (BDI-II). APA PsycTests.
Brewster, M. E., & Moradi, B. (2010). Perceived experiences of anti-bisexual prejudice: Instrument development and evaluation. Journal of Counseling Psychology, 57(4), 451–468. https://doi.org/10.1037/a0021116
Brooks, V. R. (1981). Minority stress and lesbian women. Lexington Books.
Chen, J., Walters, M. L., Gilbert, L. K., & Patel, N. (2020). Sexual violence, stalking, and intimate partner violence by sexual orientation. United States. Psychology of Violence, 10(1), 110–119. https://doi.org/10.1037/vio0000252
Doan Van, E. E., Mereish, E. H., Woulfe, J. M., & Katz-Wise, S. L. (2019). Perceived discrimination, coping mechanisms, and effects on health in bisexual and other non-monosexual adults. Archives of Sexual Behavior, 48(1), 159–174. https://doi.org/10.1007/s10508-018-1254-z
Dyar, C., & London, B. (2018). Longitudinal Examination of a bisexual-specific minority stress process among bisexual cisgender women. Psychology of Women Quarterly, 42(3), 342–360. https://doi.org/10.1177/0361684318768233
Dyar, C., Feinstein, B. A., & London, B. (2014). Dimensions of sexual identity and minority stress among bisexual women: The role of partner gender. Psychology of Sexual Orientation and Gender Diversity, 1(4), 441–451. https://doi.org/10.1037/sgd0000063
Eliason, M. (2000). Bi-negativity: The stigma facing bisexual men. Journal of Bisexuality, 1(2–3), 137–154. https://doi.org/10.1300/J159v01n02_05
Feinstein, B. A., & Dyar, C. (2017). Bisexuality, minority stress, and health. Current Sexual Health Reports, 9(1), 42–49. https://doi.org/10.1007/s11930-017-0096-3
Flanders, C. E. (2015). Bisexual health: A daily diary analysis of stress and anxiety. Basic and Applied Social Psychology, 37(6), 319–335. https://doi.org/10.1080/01973533.2015.1079202
Friedman, M. R., Dodge, B., Schick, V., Herbenick, D., Hubach, R. D., Bowling, J., Goncalves, G., Krier, S., & Reece, M. (2014). From bias to bisexual health disparities: Attitudes toward bisexual men and women in the United States. LGBT Health, 1(4), 309–318. https://doi.org/10.1089/lgbt.2014.0005
Gibbs, J. J., & Goldbach, J. (2015). Religious conflict, sexual identity, and suicidal behaviors among LGBT young adults. Archives of Suicide Research, 19(4), 472–488. https://doi.org/10.1080/13811118.2015.1004476
González-Ramírez, M. T., & Landero-Hernández, R. (2014). Propiedades psicométricas de la escala de Apoyo Social Familiar y de Amigos (AFA-R) en una muestra de estudiantes [Psychometric properties of the Social Support from Parents and Friends Scale (AFA-R) in a sample of students]. Acta De Investigación Psicológica, 4(2), 1469–1480. https://doi.org/10.1016/S2007-4719(14)70387-4
Grove, M. E. (2022). Development and Initial Validation of the Hypersexualization of Bisexual Women Measure (HBWM) (Doctoral dissertation, Lehigh University). ProQuest Dissertations & Theses Global.
GSA Network. (2023). What is a GSA club? https://gsanetwork.org/what-is-a-gsa/
Gupta, B., & Thyloth, M. (2021). Role of multimodal psychotherapeutic approaches in bisexual adult man: A case study. Journal of Psychosexual Health, 1(3), 81–87. https://doi.org/10.1177/2631831821994253
Hatzenbuehler, M. L. (2009). How does sexual minority stigma “get under the skin”? A Psychological Mediation Framework. Psychological Bulletin, 135(5), 707–730. https://doi.org/10.1037/a0016441
Hatzenbuehler, M. L., McLaughlin, K. A., & Nolen-Hoeksema, S. (2008). Emotion regulation and internalizing symptoms in a longitudinal study of sexual minority and heterosexual adolescents. Journal of Child Psychology and Psychiatry, 49(12), 1270–1278. https://doi.org/10.1111/j.1469-7610.2008.01924.x
Hegna, K., & Wichstrøm, L. (2007). Suicide Attempts among Norwegian Gay, Lesbian and Bisexual Youths: General and specific risk factors. Acta Sociologica, 50(1), 21–37. https://doi.org/10.1177/0001699307074880
Hertlein, K. M., Hartwell, E. E., & Munns, M. E. (2016). Attitudes toward bisexuality according to sexual orientation and gender. Journal of Bisexuality, 16(3), 339–360. https://doi.org/10.1080/15299716.2016.1200510
IGLYO. (2022). LGBTQI European education index 2022. https://www.education-index.org/2022/
IPSOS. (2021). LGBT+ Pride 2021 Global Survey. https://www.ipsos.com/en/lgbt-pride-2021-global-survey-points-generation-gap-around-gender-identity-and-sexual-attraction
Johnson, N. L., & Grove, M. (2017). Why us? Toward an understanding of bisexual women’s vulnerability for and negative consequences of sexual violence. Journal of Bisexuality, 17(4), 435–450. https://doi.org/10.1080/15299716.2017.1364201
Jorm, A. F., Korten, A. E., Rodgers, B., Jacomb, P. A., & Christensen, H. (2002). Sexual orientation and mental health: Results from a community survey of young and middle-aged adults. British Journal of Psychiatry, 180(5), 423–427. https://doi.org/10.1192/bjp.180.5.423
Keating, L., & Muller, R. T. (2020). LGBTQ+ based discrimination is associated with PTSD symptoms, dissociation, emotion dysregulation, and attachment insecurity among LGBTQ+ adults who have experienced trauma. Journal of Trauma & Dissociation, 21(1), 124–141. https://doi.org/10.1080/15299732.2019.1675222
Kim, I. (2014). The role of critical ethnic awareness and social support in the discrimination–depression relationship among Asian Americans: Path analysis. Cultural Diversity and Ethnic Minority Psychology, 20(1), 52–60. https://doi.org/10.1037/a0034529
Lytle, A., Dyar, C., Levy, S. R., & London, B. (2017). Contact with bisexual individuals reduces binegativity among heterosexuals and lesbian women and gay men. European Journal of Social Psychology, 47(5), 580–599.
Manalastas, E. J., Blumenau, H. S., & Feinstein, B. A. (2023). Gender differences in attitudes toward bisexual people and bisexuality: A systematic review and meta-analysis. Psychology of Sexual Orientation and Gender Diversity. https://doi.org/10.1037/sgd0000624. Advance online publication.
McDermott, E., Hughes, E., & Rawlings, V. (2018). The social determinants of Lesbian, Gay, Bisexual and transgender youth suicidality in England: A mixed methods study. Journal of Public Health, 40(3), e244–e251. https://doi.org/10.1093/pubmed/fdx135
Mei, S., Meng, C., Hu, Y., Guo, X., Lv, J., Qin, Z., Liang, L., Li, C., Fei, J., Cao, R., & Hu, Y. (2022). Relationships between depressive symptoms, interpersonal sensitivity and social support of employees before and during the COVID-19 epidemic: A cross-lag study. Frontiers in Psychology. https://doi.org/10.3389/fpsyg.2022.742381
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697. https://doi.org/10.1037/0033-2909.129.5.674
Mohr, J. J., & Fassinger, R. E. (2000). Measuring dimensions of lesbian and gay male experience. Measurement and Evaluation in Counseling & Development, 33(2), 66–90. https://doi.org/10.1080/07481756.2000.12068999
Mohr, J. J., Weiner, J. L., Chopp, R. M., & Wong, S. J. (2009). Effects of client bisexuality on clinical judgment: When is bias most likely to occur? Journal of Counseling Psychology, 56(1), 164–175. https://doi.org/10.1037/a0012816
Morina, N., Kip, A., Hoppen, T., Priebe, S., & Meyer, T. (2021). Potential impact of physical distancing on physical and mental health: A rapid narrative umbrella review of meta-analyses on the link between social connection and health. BMJ Open. https://doi.org/10.1136/bmjopen-2020-042335
Mulick, P. S., & Wright, L. W., Jr. (2002). Examining the existence of biphobia in the heterosexual and homosexual populations. Journal of Bisexuality, 2(4), 45–64. https://doi.org/10.1300/j159v02n04_03
Nebot-García, J. E., Martínez-Gómez, N., Castro-Calvo, J., Gil-Juliá, B., & Ballester-Arnal, R. (2019). Violencia derivada de la orientación sexual en adultos mayores. International Journal of Developmental and Educational Psychology, 1(3), 377–386.
Nemtay, A., & Hines, S. (2020). Lived experience of Iranian bisexual women: A thematic analysis. Journal of Gay & Lesbian Social Services, 32(2), 164–190. https://doi.org/10.1080/10538720.2019.1690610
Newcomb, M. E., & Mustanski, B. (2010). Internalized homophobia and internalizing mental health problems: A meta-analytic review. Clinical Psychology Review, 30(8), 1019–1029. https://doi.org/10.1016/j.cpr.2010.07.003
Ochs, R. (1996). Biphobia: It goes more than two ways. In B. A. Firestein (Ed.), Bisexuality: The psychology and politics of an invisible minority (pp. 217–239). Sage Publications Inc.
Pachankis, J. E., Sullivan, T. J., Feinstein, B. A., & Newcomb, M. E. (2018). Young adult gay and bisexual men’s stigma experiences and mental health: An 8-year longitudinal study. Developmental Psychology, 54(7), 1381–1393. https://doi.org/10.1037/dev0000518
Paul, R., Smith, N. G., Mohr, J. J., & Ross, L. E. (2014). Measuring dimensions of bisexual identity: Initial development of the Bisexual Identity Inventory. Psychology of Sexual Orientation and Gender Diversity, 1(4), 452–460. https://doi.org/10.1037/sgd0000069
Pollitt, A. M., & Roberts, T. S. (2021). Internalized binegativity, LGBQ+ Community involvement, and definitions of bisexuality. Journal of Bisexuality, 21(3), 357–379. https://doi.org/10.1080/15299716.2021.1984363
Pond, T., & Farvid, P. (2017). “I do like girls. I promise”: Young bisexual women’s experiences of using Tinder. Psychology of Sexualities Review, 8(2), 6–24. https://doi.org/10.53841/bpssex.2017.8.2.6
Porta, C., Singer, E., Mehus, C., Gower, A., Saewyc, E., Fredkove, W., & Eisenberg, M. (2017). LGBTQ Youth’s views on Gay-Straight Alliances: Building community, providing gateways, and representing safety and support. The Journal of School Health, 87(7), 489–497. https://doi.org/10.1111/josh.12517
Poteat, V., Heck, N., Yoshikawa, H., & Calzo, J. (2017). Gay-Straight Alliances as settings to discuss health topics: Individual and group factors associated with substance use, mental health, and sexual health discussions. Health Education Research, 32, 258–268. https://doi.org/10.1093/her/cyx044
Rankin, S., & Hiwatari, J. (2018). Roadmap to bisexual inclusion: A guide for Scottish services. Equality Network. https://www.equality-network.org/resources/roadmap-to-bisexual-inclusion/
Ryan, C., Huebner, D., Diaz, R. M., & Sanchez, J. (2009). Family rejection as a predictor of negative health outcomes in White and Latino lesbian, gay, and bisexual young adults. Pediatrics, 123(1), 346–352. https://doi.org/10.1542/peds.2007-3524
Salim, S., Robinson, M., & Flanders, C. (2019). Bisexual women’s experiences of microaggressions and microaffirmations and their relation to mental health. Psychology of Sexual Orientation and Gender Diversity, 6(3), 336–346. https://doi.org/10.1037/sgd0000329
Sanz, J. (2014). Recommendations for the use of the Spanish adaptation of the Beck Anxiety Inventory (BAI) in clinical practice [Recomendaciones para la utilización de la adaptación española del Inventario de Ansiedad de Beck (BAI) en la práctica clínica]. Clínica y Salud, 25(1), 39–48. https://doi.org/10.5093/cl2014a3
Sanz-Barbero, B., Saurina, C., Serra, L., Renart Vicens, G., Vall-Llosera Casanovas, L., Otero-García, L., López, M. J., Perez, G., & Vives-Cases, C. (2021). Prevalence and associated factors with sexual violence victimisation youth before, during and after the COVID-19 lockdown: A cross-sectional study in Spain. BMJ open, 11(11), e055227. https://doi.org/10.1136/bmjopen-2021-055227
Sarno, E. L., Newcomb, M. E., Feinstein, B. A., & Mustanski, B. (2020). Bisexual men’s experiences with discrimination, internalized binegativity, and identity affirmation: Differences by partner gender. Archives of Sexual Behavior, 49(5), 1783–1798. https://doi.org/10.1007/s10508-020-01712-z
Schmitt, M. T., Branscombe, N. R., Postmes, T., & Garcia, A. (2014). The consequences of perceived discrimination for psychological well-being: A meta-analytic review. Psychological Bulletin, 140(4), 921–948. https://doi.org/10.1037/a0035754
Schrimshaw, E., Downing, M., & Cohn, D. (2018). Reasons for non-disclosure of sexual orientation among behaviorally bisexual men: Non-disclosure as stigma management. Archives of Sexual Behavior, 47, 219–233. https://doi.org/10.1007/s10508-016-0762-y
Schulz, C. T., Stamates, A. L., Ehlke, S. J., & Kelley, M. L. (2023). Dimensions of binegativity differentially predict drinking to cope motivations and alcohol use severity among bisexual women. Experimental and Clinical Psychopharmacology, 31(2), 305–311. https://doi.org/10.1037/pha0000590
Serpe, C., Brown, C., Criss, S., Lamkins, K., & Watson, L. (2020). Bisexual women: Experiencing and coping with objectification, prejudice, and erasure. Journal of Bisexuality, 20, 456–492. https://doi.org/10.1080/15299716.2020.1820421
Sharpley, C., Hussain, R., Wark, S., Mcevoy, M., & Attia, J. (2015). The influence of social support on psychological distress in older persons: An examination of interaction processes in Australia. Psychological Reports, 117(3), 883–896. https://doi.org/10.2466/21.10.PR0.117c27z5
Sheets, R. L., & Mohr, J. J. (2009). Perceived social support from friends and family and psychosocial functioning in bisexual young adult college students. Journal of Counseling Psychology, 56(1), 152–163. https://doi.org/10.1037/0022-0167.56.1.152
Shi, Y. (2022). Assessment of effect of perceived social support on school readiness, mental well-being, and self-esteem: Mediating role of psychological resilience. Frontiers in Psychology. https://doi.org/10.3389/fpsyg.2022.911841
Steck, A., & Perry, D. (2016). Fostering safe and inclusive spaces for LGBTQ students: Phenomenographic exploration of high school administrators’ perceptions about GSAs. Journal of LGBT Youth, 13, 352–377. https://doi.org/10.1080/19361653.2016.1185759
Taylor, A. B., & Neppl, T. K. (2023). Sexual identity in Lesbian, Gay, Bisexual, Transgender, and Queer or Questioning emerging adults: the role of parental rejection, and sexuality specific family support. Journal of Family Issues, 44(2), 409–428. https://doi.org/10.1177/0192513X211050063
The International Lesbian, Gay, Bisexual, Trans and Intersex Association [ILGA]. (2023). Rainbow Map. https://rainbow-europe.org/
Wang, S., Feng, K., Zhang, Y., Liu, J., Wang, W., & Li, Y. (2020). Antecedents of public mental health during the COVID-19 pandemic: Mediation of pandemic-related knowledge and self-efficacy and moderation of risk level. Frontiers in Psychiatry. https://doi.org/10.3389/fpsyt.2020.567119
Yost, M. R., & Thomas, G. D. (2012). Gender and binegativity: Men’s and women’s attitudes toward male and female bisexuals. Archives of Sexual Behavior, 41(3), 691–702. https://doi.org/10.1007/s10508-011-9767-8
Zivony, A., & Lobel, T. (2014). The invisible stereotypes of bisexual men. Archives of Sexual Behavior, 43(6), 1165–1176. https://doi.org/10.1007/s10508-014-0263-9
Funding
Funding for open access publishing: Universidad de Córdoba/CBUA
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. The study was approved by the Ethics Committee of the Universidad de Córdoba.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Velasco, J., Miranda-Tena, A. & Sanmartín, F.J. Bisexual Discrimination, Internalized Binegativity and their Impact on Mental Health. Sex Res Soc Policy (2024). https://doi.org/10.1007/s13178-024-00990-9
Accepted:
Published:
DOI: https://doi.org/10.1007/s13178-024-00990-9