
Abstract
Current non-invasive prenatal diagnosis for fetal aneuploidies is based on biochemical and ultrasound markers and needs to be improved in order to reduce the number of pregnant women subjected to invasive diagnostic procedures. Proteomic technologies allow for new strategies for discovering biomarkers in complex biological fluids in a high-throughput and sensitive manner. Application of advance proteomic tools to profile pathology-specific proteins in maternal plasma obtained from pregnancies with aneuploid fetuses revealed biomarker-candidates that can potentially revolutionize the diagnostic and treatment procedure in favor of better prediction and improved individual outcomes. The current review focuses on studies of maternal peripheral blood using proteomic technologies, describes alterations noted in the presence of fetal aneuploidies and discuss their potential use as biomarkers for non-invasive prenatal diagnosis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chromosome aneuploidies and structural abnormalities are a leading cause of developmental disabilities and congenital malformations in man with an incidence of about one in 200 newborns [1].
The current approach for testing for fetal chromosome abnormalities is cytogenetic analysis of fetal cells following amniocentesis or chorionic villus sampling (CVS). These diagnostic tests, which have an accuracy of approximately 99%, are most often used as a second line of study, due to their invasiveness and relative risk for fetal loss. As various studies have demonstrated, all women undergoing invasive tests, only 1%–5% actually have an affected fetus [2, 3].
In order to reduce, or even eliminate, unnecessary invasive procedures screening tests for fetal chromosome abnormalities have been developed. Prenatal screening aims to estimate a woman’s risk of having an affected fetus based on a combination of ultrasound markers and the concentration of certain biomarkers [4]. Second-trimester screening biomarkers for fetal aneuploidies, known as «quad screening», involve maternal serum α-fetoprotein (AFP), unconjugated estriol (uE3), human chorionic gonadotropin (hCG) and inhibin A [5]. Screening in the first trimester of gestation involves nuchal translucency measurement combined with maternal serum hCG and PAPP-A. Despite intense efforts, the highest detection rate obtained using prenatal screening techniques is 95% at a false positive rate of 5% and may be even lower if certain screening techniques (e.g., nuchal translucency) are not offered [5, 6]. Additionally, available screening tests for fetal aneuploidies lack specificity. Patients who screen positive are generally offered genetic counseling and definitive diagnosis is recommended through invasive procedures [7].
With regards to the early non-invasive prenatal detection of fetal aneuploidies the need for and the development of reliable serum biomarkers, which are both sensitive and specific, remains a long awaited priority.
Recent advances in mass spectrometry based proteomic technologies are transforming medical research [8, 9]. Proteomics involve the analysis and illumination of all proteins encoded by the genome. It is these proteins that can be pursued as biomarkers for non-invasive prenatal diagnosis and possibly elucidate the molecular mechanisms involved in fetal aneuploidies. Biomarkers represent specific biological conditions, including disease states and may have potential roles at every step of disease management. In contrast to genetic biomarkers, in the form of disease genes, that are able to define the risk of developing a disease, alterations of the proteome can be used for prediction, early detection and diagnosis as well as disease prognosis, progress monitoring and evaluation of response to therapy. In addition to their direct use in tracking disease, proteomic biomarkers can provide targets for therapeutic intervention and advance knowledge about signaling pathways involved in disease.
This review will explore the possibility of applying proteomic technologies for the identification of novel biomarkers that aim to improve prenatal screening tests for fetal aneuploidies.
Source of biomarkers for non-invasive prenatal diagnosis
Efforts for improvement of current screening include several related biological fluids, such as maternal peripheral blood, maternal urine or cervical-vaginal fluid (CVF) that can be easily obtained using minimally invasive procedures.
Urine has the advantage of being frequently and non-invasively available, abundant and as a result of being a filtrate of serum, relatively simple in its composition. Although the protein complement of urine has been characterized using various proteomics technologies, its low protein content and high concentration in salts and other contaminants represent a major challenge for the routine quantitative studies required for biomarker discovery [10–12]. Consequently, detection of proteins in urine has received relatively little attention as a source of potential biomarkers for fetal aneuploidies CVF is a complex biological fluid that contains proteins predominantly synthesized by the endocervix and vaginal cells [13]. Shaw et al. characterized the protein repertoire of human CVF using two different fractionation approaches, SDS-PAGE and strong cation exchange chromatography, followed by LCMS/MS [14]. They identified 685 proteins with extracellular or membrane proteins making up to 30% of the proteins identified. Dasari et al. compared the CVF proteome with that of the AF and showed 77 proteins unique to CVF, while 56 were also present in AF, due to leakage of AF into CVF caused by disruption and secretion of the chorionic-decidual interface [15]. Further investigation, however, will be necessary in order to explore the possibility of using CVF for diagnosis or screening of aneuploidies.
Maternal peripheral blood has been frequently analyzed in order to identify differentially expressed proteins for pregnancy-related conditions [16–19]. This idea is mainly based on the observation that the placenta from fetuses with chromosomal aneuploidies is morphologically distinct from that of euploid fetuses, a feature attributed to altered aberrant protein expression. As the placenta is in direct contact with maternal circulation, proteins released by it can be detected in maternal plasma, and consequently serve as promising markers for fetal aneuploidies.
For protein studies plasma is often preferred over serum because it is obtained by bypassing the process of clotting which activates proteases and degrades proteins into fragments. It represents however the most complex of human proteomes, due to the large dynamic range (10 orders of magnitude) of individual protein concentrations [8]. The most abundant protein present in human plasma is albumin at 35–50 mg/ml. The top 10 most abundant proteins make up 90% of plasma proteins and mask the presence of lower-abundance proteins. For this reason depletion of the most abundant proteins and/or prefractionation are recommended in order to observe the less abundant ones [20]. Depletion can be performed using various commercial kits mainly based on affinity columns [7, 20, 21]. This approach, however, carries certain disadvantages, as some of the high-abundance proteins, albumin in particular, are known to act as carrier molecules for other proteins and by removing them, potentially interesting molecules may be lost as well [22, 23].
Prefractionation is usually performed using either two-dimensional electrophoresis (2D-E) or liquid chromatography (LC). 2D-E is the most commonly used proteomic approach for biomarker discovery, due to its power to separate proteins in a gel matrix based on two independent physicochemical properties of each protein: the isoelectric point (pI) and the molecular weight (MW) [24–26]. 2D-E has the advantage of easy visualization of large numbers of proteins. When gels from different samples are compared, it is possible to identify gel spots that differ between samples. The main drawbacks of 2D-E include reproducibility, time and labor intensiveness of the process and imperfect separation of hydrophobic proteins in both Pi and MW extremities.
Liquid chromatography (LC) is gaining in popularity due its resolving power. Proteins are often first digested and the resulting peptides are separated by chromatography, based on a different characteristic, such as charge, followed by another chromatographic separation based on another property, such as hydrophobicity [27]. 2D-LC coupled to tandem mass spectrometry (MS/MS) is now commonly known as multi-dimensional protein identification technique (MudPIT) [28].
Application of proteomics for prenatal biomarker discovery
To date, several studies have analyzed maternal blood in search for biomarkers for fetal aneuplodies using «top-down» and «bottom-up» MS based proteomic technologies. Most studies focused on DS, since it is the most common congenital anomaly, with a prevalence of 1 in 732 births [29].
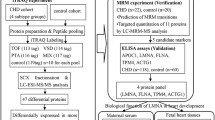
The first attempt to identify biomarkers for DS was performed using a combination of top-down and bottom-up approaches such as DIGE, 2-dimensional liquid chromatography chromatofocusing, MudPIT, LC/LC-MS/MS and MALDI-TOF-MS peptide profiling (Table 1) [16]. First and 2nd trimester maternal serum from women carrying DS fetuses and gestational age-matched controls, were analyzed. A list of 25 proteins differentially abundant in DS serum was reported with an average recognition capability that approached 96%.
Kolialexi et al. analyzed plasma from 8 women carrying a DS fetus and from 12 women carrying chromosomally normal ones, matched for gestational age, maternal age and ethnicity, in the 2nd trimester of pregnancy, using 2-DE coupled with MALDI-TOF-MS [17]. Gel comparison revealed nine proteins differentially expressed in maternal plasma in women with DS fetuses (Fig. 1). Eight proteins, Transthyretin (TTHY), Ceruloplasmin (CERU), Afamin (AFAM), Alpha-1-microglobulin (AMBP), Apolipoprotein E (APOE), Serum amyloid P-component (SAMP), Histidine-rich glycoprotein (HRG) and Alpha-1-antitrypsin (A1AT) were up-regulated and one, Clusterin (CLUS), down- regulated. All nine proteins detected in this study are known to be involved in fetal growth and development, while APOE, SAMP, AFAM and CLUS are associated with the DS phenotype. All differentially expressed proteins are candidate biomarkers for DS, providing opportunities for the development of non-invasive prenatal diagnosis. In another study, the same group compared the protein composition of maternal plasma samples from pregnant women with normal and Turner syndrome fetuses, using a similar methodology [18]. The study showed nine proteins (C1S, CO3, CLUS, AFAM, HABP2, IGHA1, HPT, SHBG, and CD5L) significantly increased in the plasma of women carrying TS fetuses, whereas KNG1, IGJ, and TTHY were decreased.

2D-E regions including spots with different intensity in maternal plasma samples from women known to carry normal and DS fetuses. Differentially expressed spots correspond to Apo E and SAMP (From [17] copyright Willey. reproduced with permission)
Busch et al., using Surface-Enhanced Laser Desorption/Ionization time of- flight mass spectrometry (SELDI-TOF) technology, compared the proteomic profiles of first-trimester serum samples from women carrying a normal fetus with samples from cases carrying a fetus with DS [30]. Following bio-informatic analysis, a combined pattern of six peaks was found to predict discrimination between the two groups of mothers with 91% sensitivity and 97% specificity. Lack of precise protein identification in SELDI-TOF, however, limits the information about these biomarkers to their m/z value.
Recently, Kolla et al. used four-plex iTRAQ labeling to compare six 1st trimester maternal plasma samples from women known to carry DS fetuses [19]. Analysis revealed 50 proteins, with a variety of functions and expression levels, differentially expressed in DS fetuses. Further verification of these proteins may reveal potential biomarkers which could improve current screening.
Concluding remarks and outlook
Proteomic studies that explore proteins released by the fetus into the maternal circulation offer new opportunities for the identification of either one protein marker or a panel of markers for non-invasive prenatal diagnosis that could be usefully employed for diagnostic purposes or improvement of the current screening methods.
It is important to note that experimental design using standard protocols, followed by appropriate analytical techniques and statistical analysis, are critical to proteomic experiments. In complex samples, such as peripheral blood, use of analytical techniques that allow rapid screening and require small quantity of sample for accurate protein identification are of great importance. Of equal importance is the use of protocols that guarantee identical sample collection and proper storage conditions to ensure reproducibility. Emphasis should be placed on sample purification, protein digestion plus affinity capture and sample fractionation to reduce the complexity of the target biological fluid. It must also be noted that, when identifying biomarkers for prenatal diagnosis, gestational age-matched controls must be used, since proteins content depend on the developmental stage of the fetus.
Regardless of the method used as the first step of biomarker discovery process, the resulting candidate markers need to be further proved and tested if they are to become clinically used biomarkers. Candidates need to be further qualified, in order to confirm their differential abundance in the tested samples, in a targeted manner, in a statistically significant number of samples. Unfortunately, antibodies against these newly discovered candidates are frequently unavailable, and alternatives to immunoassays should be used [31].
Finally, before any meaningful application of these proteomic biomarkers, a clinical assay should be developed and extensive validation in the form of well-designed, statistically significant human clinical trials must be performed. Validation should also involve large scale multicenter clinical trials to ensure the sensitivity and specificity required for prenatal diagnosis. It is important to compare the sensitivity and specificity of the new biomarkers for population screening with those of the currently available tests for the detection of pregnancies at risk for fetal anuploidies. Thus the collection of biological samples, along with clinical, ultrasonographic and biochemical data in large biobanks is necessary.
References
Faas BH, Cirigliano V, Bui TH. Rapid methods for targeted prenatal diagnosis of common chromosome aneuploidies. Semin Fetal Neonatal Med. 2011;16:81–7.
Haddow JE, Palomaki GE, Knight GJ, Williams J, Pulkkinen A, Canick JA, et al. Prenatal screening for Down’s syndrome with use of maternal serum markers. N Engl J Med. 1992;327:588–93.
Verp MS, Bombard AT, Simpson JL, Elias S. Parental decision following prenatal diagnosis of fetal chromosome abnormality. Am J Med Genet. 1988;29:613–22.
D’Alton M, Cleary-Goldman J. First and second trimester evaluation of risk for fetal aneuploidy: the secondary outcomes of the FASTER Trial. Semin Perinatol. 2005;29:240–6.
Malone FD, Canick JA, Ball RH, Nyberg DA, Comstock CH, Bukowski R, et al. First-trimester or second-trimester screening, or both, for Down’s syndrome. N Engl J Med. 2005;353:2001–11.
Knight GJ, Palomaki GE, Neveux LM, Smith DE, Kloza EM, Pulkkinen AJ, et al. Integrated serum screening for Down syndrome in primary obstetric practice. Prenat Diagn. 2005;25:1162–7.
Avent ND, Plummer ZE, Madgett TE, Maddocks DG, Soothill PW. Post-genomics studies and their application to non-invasive prenatal diagnosis. Semin Fetal Neonatal Med. 2008;13:91–8.
Anderson NL, Anderson NG. The human plasma proteome: history, character, and diagnostic prospects. Mol Cell Proteomics. 2002;1:845–67.
Bahtiyar MO, Copel JA, Mahoney MJ, Buhimschi IA, Buhimschi CS. Proteomics: a novel methodology to complement prenatal diagnosis of chromosomal abnormalities and inherited human diseases. Am J Perinatol. 2007;24:167–81.
Adachi J, Kumar C, Zhang Y, Olsen JV, Mann M. The human urinary proteome contains more than 1500 proteins, including a large proportion of membrane proteins. Genome Biol. 2006;7:R80.
Kentsis A, Lin YY, Kurek K, Calicchio M, Wang YY, Monigatti F, et al. Discovery and validation of urine markers of acute pediatric appendicitis using high-accuracy mass spectrometry. Ann Emerg Med. 2010;55:62–70.e4.
Candiano G, Santucci L, Petretto A, Bruschi M, Dimuccio V, Urbani A, et al. 2D-electrophoresis and the urine proteome map: where do we stand? J Proteomics. 2010;73:829–44.
Huggins GR, Preti G. Vaginal odors and secretions. Clin Obstet Gynecol. 1981;24:355–77.
Shaw JL, Smith CR, Diamandis EP. Proteomic analysis of human cervico-vaginal fluid. J Proteome Res. 2007;6:2859–65.
Dasari S, Pereira L, Reddy AP, Michaels JE, Lu X, Jacob T, et al. Comprehensive proteomic analysis of human cervical-vaginal fluid. J Proteome Res. 2007;6:1258–68.
Nagalla SR, Canick JA, Jacob T, Schneider KA, Reddy AP, Thomas A, et al. Proteomic analysis of maternal serum in Down syndrome: identification of novel protein biomarkers. J Proteome Res. 2007;6:1245–57.
Kolialexi A, Tsangaris GT, Papantoniou N, Anagnostopoulos AK, Vougas K, Bagiokos V, et al. Application of proteomics for the identification of differentially expressed protein markers for Down syndrome in maternal plasma. Prenat Diagn. 2008;28:691–8.
Kolialexi A, Anagnostopoulos AK, Papantoniou N, Vougas K, Antsaklis A, Fountoulakis M, et al. Potential biomarkers for Turner in maternal plasma: possibility for noninvasive prenatal diagnosis. J Proteome Res. 2010;9:5164–70.
Kolla V, Jeno P, Moes S, Tercanli S, Lapaire O, Choolani M, et al. Quantitative proteomics analysis of maternal plasma in Down syndrome pregnancies using isobaric tagging reagent (iTRAQ). J Biomed Biotechnol. 2010;2010:952047.
Hannan NJ, Stoikos CJ, Stephens AN, Salamonsen LA. Depletion of high-abundance serum proteins from human uterine lavages enhances detection of lower-abundance proteins. J Proteome Res. 2009;8:1099–103.
Imre T, Kremmer T, Heberger K, Molnar-Szollosi E, Ludanyi K, Pocsfalvi G, et al. Mass spectrometric and linear discriminant analysis of N-glycans of human serum alpha-1-acid glycoprotein in cancer patients and healthy individuals. J Proteomics. 2008;71:186–97.
Huang HL, Stasyk T, Morandell S, Mogg M, Schreiber M, Feuerstein I, et al. Enrichment of low-abundant serum proteins by albumin/immunoglobulin G immunoaffinity depletion under partly denaturing conditions. Electrophoresis. 2005;26:2843–9.
Liu T, Qian WJ, Mottaz HM, Gritsenko MA, Norbeck AD, Moore RJ, et al. Evaluation of multiprotein immunoaffinity subtraction for plasma proteomics and candidate biomarker discovery using mass spectrometry. Mol Cell Proteomics. 2006;5:2167–74.
O’Farrell PH. High resolution two-dimensional electrophoresis of proteins. J Biol Chem. 1975;250:4007–21.
Gorg A, Weiss W, Dunn MJ. Current two-dimensional electrophoresis technology for proteomics. Proteomics. 2004;4:3665–85.
Carrette O, Burkhard PR, Sanchez JC, Hochstrasser DF. State-of-the-art two-dimensional gel electrophoresis: a key tool of proteomics research. Nat Protoc. 2006;1:812–23.
Tambor V, Fucikova A, Lenco J, Kacerovsky M, Rehacek V, Stulik J, et al. Application of proteomics in biomarker discovery: a primer for the clinician. Physiol Res. 2010;59:471–97.
Wolters DA, Washburn MP, Yates 3rd JR. An automated multidimensional protein identification technology for shotgun proteomics. Anal Chem. 2001;73:5683–90.
Canfield MA, Ramadhani TA, Langlois PH, Waller DK. Residential mobility patterns and exposure misclassification in epidemiologic studies of birth defects. J Expo Sci Environ Epidemiol. 2006;16:538–43.
Busch A, Michel S, Hoppe C, Driesch D, Claussen U, von Eggeling F. Proteome analysis of maternal serum samples for trisomy 21 pregnancies using ProteinChip arrays and bioinformatics. J Histochem Cytochem. 2005;53:341–3.
Anderson L, Hunter CL. Quantitative mass spectrometric multiple reaction monitoring assays for major plasma proteins. Mol Cell Proteomics. 2006;5:573–88.
Author information
Authors and Affiliations
Corresponding author
Additional information
G. T. Tsangaris is a National Representative of EPMA in Greece.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Kolialexi, A., Anagnostopoulos, A.K., Tounta, G. et al. Biomarker development for non-invasive prenatal diagnosis of fetal aneuploidies: predictive reliability and potential clinical application. EPMA Journal 2, 157–161 (2011). https://doi.org/10.1007/s13167-011-0084-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13167-011-0084-z