
Abstract
Objectives
The primary objective of this study was to investigate the feasibility assessed by reach and dose of an organizational-level workplace-adapted mindfulness-based intervention (MBI). Secondarily, potential changes in mental health and organizational outcomes were evaluated.
Method
Using a quasi-experimental design without a control group, the study included four small- and medium-sized private companies. A three-step MBI was delivered live online via Zoom. Feasibility was assessed using data on reach (number of participants) and dose (number of sessions attended). Data on mental health and organizational outcomes were collected at baseline and 3- and 12-month follow-up and analyzed using mixed-effects linear regression for continuous variables, and mixed-effects logistic regression for dichotomous variables.
Results
In total, 278 (75.54%) employees and managers participated in an introductory session, and 169 (45.92%) signed up for a workplace-adapted 10-week MBSR course, while 3 (75.00%) companies participated in an implementation workshop. Among MBSR-participants, the median dosage was 9/10 sessions in three companies, and 8/10 in one company. Only small statistically non-significant changes were seen in mental health outcomes, such as tendencies to decreased perceived stress and increased well-being at 3-month follow-up. However, these tendencies were not sustained at 12-month follow-up. Yet, a positive impact was seen on respondents’ ability to decenter, and thus observe one’s thoughts and feelings, at both 3- and 12-month follow-up. Organizational impact at 3-month follow-up varied across outcome measures, with a statistically significant reduced likelihood of occasionally experiencing negative acts. However, at 12-month follow-up, this reduction was no longer statistically significant, and measures of social capital and psychological safety had generally decreased.
Conclusions
This workplace MBI is deemed feasible. However, the potential impacts on mental health and organizational outcomes remain unclear.
Preregistration
This study is registered at ISRCTN Registry (ISRCTN93567471).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The declining mental health of the world’s population is concerning, and actions to ameliorate this decline are of immense importance (WHO, 2018). Mental health may be defined as “a state of well-being that enables people to cope with the stresses of life, to realize their abilities, to learn well and work well, and to contribute to their communities” (WHO, 2022b). Thus, good mental health is not limited to the absence of mental disorders, but entails skills, such as coping with stress and working productively, which may positively affect an individual’s mental health. Practicing mindfulness has been found to positively affect such individual skills by, for example, improving awareness and connection to others (Bonde et al., 2022; Dahl et al., 2020), as well as enhancing distal mental health outcomes, such as reduced perceived stress, and improved well-being (De Vibe et al., 2017; Khoury et al., 2015; van Agteren et al., 2021). Moreover, mindfulness practices are intended to improve emotion regulation, potentially leading to enhanced ability to modulate emotional responses (Vago & David, 2012). Mindfulness may be defined as “… the awareness arising through paying attention on purpose in the present moment, non-judgmentally, in the service of self-understanding, wisdom, and compassion” (Kabat-Zinn, 2018, p. xxxiv). Mindfulness practice may enable individuals to experience the present moment with curiosity and kindness, and by being aware in the moment, one has the possibility of noticing thoughts, feelings, and bodily sensations. Moreover, practicing mindfulness may result in changes in how one relates to these thoughts, feelings, and perceptions, which could affect social situations (Crane et al., 2017). Hence, being aware of one’s own internal state may impact the way individuals engage in social interactions, e.g., by listening actively and responding in a more reflected manner as opposed to reacting automatically in, for example, stressful situations (Dahl et al., 2020; Kabat-Zinn, 2013, 2018). In a study from 2010, the authors found that humans are not mentally present in what we are doing approximately 47% of our waking hours (Killingsworth & Gilbert, 2010). Being aware in the present moment allows for the possibility of noticing when the mind is on a mental time travel, which enables individuals to bring the attention back to the present. In their study, the authors also found that people are most happy when mentally present in what they are doing independently of what activity they are engaged in (Killingsworth & Gilbert, 2010). Therefore, being aware in the present moment may enhance individual skills that protect the mental health (mental health skills), such as emotion regulation and connection to others (WHO, 2022b), as well as independently positively affect well-being (Killingsworth & Gilbert, 2010).
Mindfulness-Based Stress Reduction (MBSR) is a curriculum-based 8-week program designed to support participants in developing the ability to be aware in the present moment with kindness to one self and others. The program is delivered by a trained MBSR teacher in a group format over the course of 8 weeks with weekly 2.5-hr sessions and one 7-hr silent retreat day (Santorelli, 2014). Each session focuses on a specific topic, such as perception, pleasant experiences, and communication. MBSR has been evaluated in both clinical and non-clinical study populations as well as in various settings, including, e.g., hospitals and workplaces (De Vibe et al., 2017). Across these study populations and settings, MBSR has been found effective in reducing perceived stress, and symptoms of depression and anxiety, as well as enhancing overall well-being (De Vibe et al., 2017). Thus, it may be argued that MBSR can be utilized as a mental health–promoting intervention that can be delivered effectively to broad populations in everyday life settings, such as workplaces.
Since the release of the Perth Charter in 2012, it has been recommended that mental health–promoting interventions should be implemented in everyday life settings, such as schools, universities, and workplaces (McHenry & Donovan, 2012; WHO, 2021, 2022a). In 2022, international guidelines on mental health at work, including recommendations of implementing interventions to improve and protect the mental health among the working population, were released (WHO, 2022a). In these guidelines, it is stated that “When people have good mental health, they are better able to cope with the stresses of life, realize their own abilities, learn and work well and contribute actively to their communities. And when people have good working conditions, their mental health is protected” (WHO, 2022a). Thus, mental health and working conditions exist in a mutually enhancing relationship where improved mental health may positively affect (work) communities and good working conditions may positively affect individuals’ mental health. Furthermore, in these guidelines, mindfulness-based interventions (MBIs) are explicitly recommended as individual universal interventions to enhance workers’ stress-management skills (WHO, 2022a).
The research field of mindfulness in the workplace has continuously grown during the past decades, and positive effects on both individual and organizational outcomes have been uncovered (Good et al., 2015; Michaelsen et al., 2023; Muñoz Bohorquez et al., 2023). Still, most research has been conducted in public workplace contexts (Janssen et al., 2018), with the majority carried out in health care settings (Lomas et al., 2017). Thus, there is a call for investigating MBIs in private workplace settings. Based on previous and emergent research, a framework for both individual and organizational effects of implementing mindfulness in workplace contexts has been proposed (Good et al., 2015). While the evidence of individual effects of practicing mindfulness in workplace contexts is more substantial, less is known about mindfulness’ potential impact on organizational outcomes, such as communication and workplace climate (Good et al., 2015). Similarly, in a systematic review and meta-analysis from 2020, the authors found that MBIs offered in a workplace context were effective in enhancing employee mental health across occupational settings, but the evidence of effects on organizational outcomes, such as work engagement and job satisfaction, was still scarce (Vonderlin et al., 2020). Similar results were found in the most recent systematic review and meta-analysis of MBIs in workplace settings (Michaelsen et al., 2023). In this review from 2023, workplace outcomes such as job satisfaction and productivity were found to be positively affected by mindfulness interventions offered in workplace settings (Michaelsen et al., 2023). Moreover, recent research has demonstrated that mindfulness may contribute to organizational impacts, such as prosocial behavior, reduced incivility at work, and a more conflict positive work environment (Hülsheger et al., 2021; Kay & Skarlicki, 2020; Panditharathne & Chen, 2021). Furthermore, in a recent study, the authors found that mindfulness training may foster greater levels of altruism and support for non-group members, such as ethnic minority groups, which may positively influence interpersonal relations (Zheng et al., 2023). Hence, current evidence indicates that mindfulness delivered in workplace contexts may positively affect individual mental health and the psychosocial working environment. Thereby, mindfulness may contribute to the mutually enhancing relationship between mental health and working conditions (WHO, 2022a). However, more research is needed to build the evidence base of potential organizational outcomes of mindfulness in workplace contexts. To affect such organizational outcomes, e.g., workplace relationships, interventions may effectively be delivered at an organizational level to entire workplace populations. In their framework for developing and evaluating complex interventions, the Medical Research Council (MRC) encourages interventions to be delivered using such whole system approaches to evoke system change (Skivington et al., 2021). In a workplace context, this may be translated into targeting the whole workplace and not merely selected individuals within the workplace. Thus, by using a population-based approach (Rose et al., 2008), an MBI may be offered to all employees and managers within a given workplace and not solely a selected group such as those at high risk of future sick leave. Moreover, by integrating mindfulness in the organization, changes in social interactions may influence relations positively, and thus perhaps contribute to healthier psychosocial work environments. Regarding public health, in recent decades much emphasis has been placed on the inadequacy of intervention effectiveness alone, emphasizing the importance of careful implementation considerations (Skivington et al., 2021). The intervention must be accessible to and accepted by the target population to achieve public health impact (Moore et al., 2015). Therefore, it is imperative to evaluate how accessible such interventions are when implemented in workplace settings, and to what extent employees and managers accept them and choose to participate. This understanding is essential to evaluating the feasibility of an intervention, as key uncertainties regarding acceptability are an integral part of feasibility and pilot evaluations of complex interventions (Skivington et al., 2021). To ensure accessibility and that a workplace MBI reaches as many employees and managers as possible, we wanted to evaluate the feasibility of delivering such an intervention to entire company populations, thus using a population-based approach to potentially evoke system change within the participating companies (Rose et al., 2008; Skivington et al., 2021).
The primary aim of this study was therefore to investigate the feasibility of an organizational-level MBI including a workplace-adapted MBSR program in private workplace settings. To determine feasibility, we wanted to evaluate how many employees and managers the intervention reached (reach), and how much of the intervention participants received (dose). We hypothesized that if the intervention had an acceptable reach and dose, and thus found feasible, this may contribute to enhanced mental health skills and mental health among employees and managers. Furthermore, we hypothesized that if the intervention was found feasible, this could also positively affect the psychosocial work environment through improved workplace relations.
Method
Participants
The study was designed as a quasi-experimental no-control group feasibility study. To enroll in the research project, companies were required to meet certain criteria; companies had (i) to be privately owned and (ii) to have a total staff count of 10–249. Companies were recruited from January 2020 to October 2020. Multiple channels were utilized for company recruitment. These included direct contact to seemingly interesting companies, and online advertisement on both social media (LinkedIn, Twitter, and Facebook) and the Danish Center for Mindfulness’ webpage. Moreover, the possibility to enroll was announced in digital newsletters from business organizations within, e.g., production businesses. In total, four companies enrolled in the study representing a total of 368 employees and managers at baseline. The included companies comprised a media company, a chain of restaurants, a production company, and an IT-company.
Procedure
Once a company expressed interest in participating in the research project, a preliminary meeting was held between the principal investigator, an MBSR teacher, and representatives from the company management. At this meeting, company representatives were informed that the intervention was an organizational-level intervention. Thus, the intervention was to be offered to all employees and managers and not solely for selected groups within the company. Furthermore, company representatives were informed that by enrolling in the research project, management was required to allow all employees to participate in a 2-hr obligatory introductory session during working hours. Moreover, managers had to agree to enable all employees to sign up for a 10-week workplace-adapted MBSR course during working hours, or alternatively, provide monetary payment for time spend participating during leisure time. Upon commitment to these terms, a formal contract of participation was signed by a company representative and the principal investigator. A project team member collaborated with a company representative on the practical organization of the intervention in the company. Thus, company wishes for commencement date, and weekday and time for the 10-week workplace-adapted MBSR course(s) were accommodated as good as possible. Data were collected at baseline, 3-month, and 12-month follow-up using the electronic data capture tool REDCap, a secure web-based system hosted by Aarhus University (Harris et al., 2009).
Up until now, several MBIs have been delivered and evaluated in workplace settings. For example, the 8-week program “Finding Peace in a Frantic World” was developed by Mark Williams as an adaptation of the 8-week curriculum-based Mindfulness-Based Cognitive Therapy (MBCT) program. This program has been found effective in reducing stress and the risk of leaving one’s job (de Bruin et al., 2020). Moreover, in a study by Kersemaekers et al. (2018), the authors developed a workplace-adapted MBI called “WorkingMind” (Kersemaekers et al., 2018). This program was built on the basis of traditional mindfulness programs such as MBSR and MBCT, but in addition to the eight weekly 2.5-hr sessions, the intervention included a full 2-day training (Kersemaekers et al., 2018), thus making it a higher-dose intervention than the original MBSR or MBCT program. In Denmark, only a small number of professionals have received the MBCT teacher training, whereas a larger number are capable of teaching the MBSR course. Therefore, we wished to develop and evaluate the feasibility of a lower-dose mindfulness program closely adapted from the original MBSR program to enable Danish MBSR teachers to potentially deliver the program at workplaces in the future.
Therefore, we developed a three-step intervention including a workplace-adapted MBSR program. The three steps consisted firstly of an obligatory 2-hr introductory session on mental health and research on mindfulness held for employees and managers in the respective companies. Secondly, all employees and managers were offered the possibility to participate in a 10-week live online workplace-adapted MBSR course. Lastly, all companies were offered a workshop on further implementation of mindfulness in the company following the 10-week workplace-adapted MBSR course.
The introductory session consisted of knowledge dissemination of the following: what mental health is, the bodily stress response, the possibility to train one’s mental health, and mindfulness as a way of doing this. Moreover, previous research on the effects of MBSR was presented, participants were invited to engage in two brief guided mindfulness practices, and information on the 10-week live online workplace-adapted MBSR course was presented. The workplace-adapted MBSR program was systematically adapted from the original MBSR program to ensure the validity of the proposed program theory (Online Resource 1). The adaptation was conducted with due caution of core elements and flexible elements of the original MBSR program. Thus, to ensure context fit while retaining the active elements of the intervention, adaptation was conducted in accordance with recommendations proposed by Crane et al. (2017). Accordingly, the workplace-adapted MBSR program was delivered by a trained MBSR teacher, followed the original MBSR curriculum, including the same weekly themes, and applied an experience-based approach using mindfulness exercises, horizontal inquiry of direct experiences, and a group-based format (Crane et al., 2017). The program was delivered live online via Zoom over the course of 10 weeks with weekly 1.5-hr sessions. During the 10-week workplace-adapted MBSR courses, all MBSR teachers delivering an MBSR course received weekly 1.5-hr supervision sessions from the third author. The supervisions followed the Mindfulness-Based Interventions: Teaching Assessment Criteria (MBI-TAC) (Crane et al., 2021). The implementation workshop was a 2-hr workshop for selected managers and employee representatives, hosted by the second author, an MBSR teacher, and the first author. The workshop included in-group and plenary discussions on whether mindfulness should be implemented in the company, and if so how this would be possible. Moreover, facilitators and barriers to further implementation were identified upon discussions, and finally, an action plan for further implementation was agreed upon.
The intervention was delivered in the four respective companies from March 2020 to April 2021. Hence, this study was conducted during the COVID-19 pandemic. Figure 1 depicts a timeline of the intervention period in the four included companies with timestamps of influential events across the study period. During the research project, the COVID-19 pandemic resulted in several local, regional, and national lockdowns. During these lockdowns, the majority of employees and managers were either required to work from home when possible or sent home from work when remote work was not feasible, for example, when working as a chef in a restaurant. Moreover, lockdowns resulted in schools being closed. Therefore, some employees and managers in this study were working from home while home schooling their children, or supporting the online teaching provided by school teachers. Additionally, Company 3 underwent an extensive re-organization during the study period resulting in some employees and managers being reassigned or dismissed. Figure 1 was built on knowledge obtained from national guidelines and recommendations as well as through dialogue with the included companies.

Timeline of the intervention including timestamps of influential events during the study period
Measures
The primary outcome was data on the feasibility of implementing this workplace MBI in small- and medium-sized private companies. Feasibility data consisted of data on reach and dose (Moore et al., 2015). Reach related to the proportions of employees and managers participating in the three intervention components, while dose related to medians of the number of sessions, employees and managers participated in when signed up for a 10-week workplace-adapted MBSR course.
Secondary outcomes were self-reported mental health outcomes, including measures of stress, symptoms of depression and anxiety, well-being, resilience, decentering, disturbed sleep, and awakening problems. Furthermore, secondary outcome measures also included organizational factors containing measures of social capital, negative acts, and team psychological safety. Data on secondary self-reported outcomes were collected at baseline, 3-month, and 12-month follow-up.
Perceived Stress Scale
The 10-item version of PSS was utilized to gather information on subjective stress (Cohen et al., 1983). The 10-item scale provides insights into how often during the past month the respondent has experienced his or her life as uncontrollable, unpredictable, or overloaded. A 5-point Likert scale is used to score items with sum score ranges of 0–40. Higher values indicate higher levels of perceived stress. Previous research has found the scale to be valid and reliable (Cohen et al., 1983; Eskildsen et al., 2015; Lee, 2012). For reliability test, McDonald’s omega was calculated. McDonald’s omega was deemed acceptable, indicating good internal consistency if the estimate was 0.70 or higher (McNeish, 2018). McDonald’s omega for PSS in the present study was estimated at 0.85.
The Hopkins Symptom Checklist-5
The Hopkins Symptom Checklist-5 (SCL-5) is a 5-item scale developed for measuring self-reported symptoms of depression and anxiety (Tambs & Moum, 1993). All items are scored on a 4-point scale, and an average score is calculated across the 5 items (score range 1–4) with higher scores indicating more self-reported symptoms of depressions and anxiety. This 5-item version correlates with the 25-item version at r = 0.92 (Strand et al., 2003), with McDonald’s omega = 0.84.
Brief Resilience Scale
The Brief Resilience Scale (BRS) is a 6-item self-reported measure of an individual’s resilience. Items are scored on a 5-point scale, and subsequently, an average score across items is calculated (score range 1–5). Higher values indicate higher levels of resilience (Smith et al., 2008). Suggested cut-points for low, normal, and high resilience are as follows: low 1.00–2.99, normal 3.00–4.30, and high 4.31–5.00 (Smith et al., 2008). To our knowledge, no construct validation of BRS has been conducted in a Danish context yet. However, BRS has been suggested by international researchers to be among the most valid resilience measures (Windle et al., 2011). McDonald’s omega for the present study was estimated at 0.88.
Short Warwick-Edinburgh Mental Well-Being Scale
The Short Warwick-Edinburgh Mental Well-Being Scale (SWEMWBS) is a shortened version of the original 14-item Warwick-Edinburgh Mental Well-Being Scale (WEMWBS) (Stewart-Brown et al., 2009). SWEMWBS is a 7-item measure of self-reported well-being over the past 2 weeks. All items are positively worded and are scored on a 5-point Likert scale. Whereas the score on the original WEMWBS is a simple sum score (14–70), Stewart-Brown et al. (2009) recommend that SWEMWBS raw scores are converted to metric scores using a conversion table (Stewart-Brown et al., 2009). Total SWEMWBS score ranges from 7 to 35 with higher scores indicating greater well-being. The SWEMWBS has been found to correlate with the original WEMWBS at r = 0.92 in a Danish sample (Koushede et al., 2019). McDonald’s omega in the present study was estimated at 0.79. Based on the Danish Health and Wellbeing Survey (Rosendahl Jensen et al., 2022), the following cut-points on the metric SWEMWBS have been suggested: low mental well-being, 7.00–19.98; moderate mental well-being, 19.99–29.30; high mental well-being, 29.31–35.00 (Santini et al., 2022).
Experiences Questionnaire–Decentering
In this study, the 11-item decentering factor from the 2-factorial Experiences Questionnaire (EQ) (Fresco et al., 2007) was included. EQ–decentering is a self-reported measure of respondents’ ability to observe one’s own thoughts and feelings objectively, knowing that these are indeed thoughts and feelings, and not reality (Fresco et al., 2007). Items are scored on a 5-point Likert scale with total score ranges from 11 to 55, with higher values indicating greater ability to decenter. To our knowledge, no validation study of EQ–decentering has been conducted in a Danish setting. However, previous international research has found the measure to be valid and reliable (Fresco et al., 2007). McDonald’s omega estimate in the present study was 0.86.
Sleep Problems
Problems relating to sleep in the past 4 weeks were measured using a 6-item modified version of the Karolinska Sleep Questionnaire (KSQ) (Hansen et al., 2014). Items represent two indexes: disturbed sleep (DSI) and awakening problems (AWI) (Rugulies et al., 2012). Items are scored on a 5-point Likert scale. Scores are calculated as mean scores within each index with ranges on both indexes from 1 to 5 (Hansen et al., 2014). This modified version of the KSQ has previously been utilized in Danish research, and has been found valid and reliable (Hansen et al., 2014). In the present study, McDonald’s omega was estimated at 0.79.
Social Capital
In this study, workplace social capital was measured using the 25-item Danish social capital questionnaire (Borg et al., 2014). The questionnaire aims at measuring social capital as experienced from a group level (Meng et al., 2018). Items are divided into four subscales: bonding social capital (within teams), bridging social capital (between teams), and social capital between employees and managers (linking social capital—immediate manager, and linking social capital—top management). Items are scored on a 5-point scale. To calculate a total score for each subscale, responses are rescaled from 0 to 100. Thus, total sum scores range from 0 to 100 with higher values indicating higher levels of social capital. The questionnaire is widely used in Danish workplace contexts. McDonald’s omegas for the four subscales were estimated at 0.89, 0.89, 0.75, and 0.90 for bonding, bridging, linking—immediate management, and linking—management overall social capital, respectively.
Short Negative Acts Questionnaire
The Danish version of the 9-item Short Negative Acts Questionnaire (S-NAQ), a shortened version of the 22-item Negative Acts Questionnaire – Revised (NAQ-R) (Conway et al., 2018), was utilized to measure negative acts in the workplace. The S-NAQ is a self-reported measure of how often the respondents have experienced nine different negative acts, such as feeling ignored or being ridiculed. Items are scored on a 5-point scale. Total scores are calculated as sum scores, resulting in total score ranges from 9 to 45 (Conway et al., 2018), with higher scores indicating higher levels of negative acts. In previous research, a cut-off score of > 12 has been used to estimate occasional experience of negative acts, indicating experiencing negative acts sometimes or monthly (Conway et al., 2018). S-NAQ has been found valid and to correlate with the NAQ-R at r = 0.85 (Conway et al., 2018). McDonald’s omega for the present study was 0.73.
Team Psychological Safety
To measure team psychological safety, the 7-item measure developed by Edmondson (1999) was utilized (Edmondson, 1999). Items are scored on a 7-point Likert scale. Total scores are calculated as sum scores with score ranges from 7 to 49, with higher values indicating greater team psychological safety. The measure has been found valid in previous research (Hastings et al., 2018). In the present study, McDonald’s omega was estimated at 0.74.
Data Analyses
Data on reach and received dose of the intervention were obtained from the records of participation, which was systematically gathered throughout the intervention. Subsequently, reach was calculated as the percentage of eligible employees and managers who participated in each of the three intervention components. Moreover, to assess the received dose of the 10-week workplace-adapted MBSR course, the median number of sessions attended was calculated.
Analyses of tendencies of change in continuous variables of self-reported mental health outcomes and organizational factors were performed using a mixed-effect linear regression model with systematic effects of time, sex, age, cohabitation status (living with or without a partner), education, job type, company, and random effect of course/group. Analyses of tendencies of change in the dichotomized S-NAQ-scores (more or less than 12) were conducted using a mixed-effects logistic regression model with systematic effects of time, sex, age, education, job type, cohabitation status, and company.
Loss to follow-up analyses at 3 months’ follow-up among all employees and managers were carried out using t-tests and χ2 tests. Two-tailed p-values were estimated, and p = 0.05 was assumed statistically significant. Similarly, a loss to follow-up analysis at 3 months was performed for employees and managers who did not sign up for or complete a 10-week workplace-adapted MBSR course (participated in < 4 sessions). In all loss to follow-up analyses, baseline data from those who contributed with follow-up data at 3 months were compared to baseline data from those who did not contribute with follow-up data at 3 months. Sensitivity analyses were conducted for all employees and managers at both 3- and 12-month follow-up. In the sensitivity analyses of continuous outcomes, missing outcomes were substituted with the model-based prediction adding or subtracting 0.2*SD. In the sensitivity analyses of the dichotomized outcome of occasionally experiencing negative acts, model-based predictions of the proposed impact of missing data were conducted by simulating log odds by adding or subtracting nothing (missing at random), 10%, and 20% variance in the log odds of occasionally experiencing negative acts.
Results
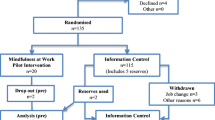
Figure 2 illustrates the flow of participants from baseline to 12-month follow-up.

Flow of participants
In total, 368 employees and managers were employed in one of the four companies at baseline. Thus, 368 persons were eligible for participation in the intervention.
In Table 1, baseline characteristics of employees and managers who completed a baseline questionnaire are displayed. Respondents consisted equally of women and men with a mean age of 41.74 years at baseline. Approximately half of the employees and managers contributing with baseline data had more than 3 years of education following high school level and were working as skilled workers/specialists at baseline.
In total, 213 (57.88%) completed the baseline questionnaire. To receive a follow-up questionnaire, employees and managers had to have contributed with baseline data. Thus, of the 213 who contributed with baseline data, 139 (65.26%) completed a 3-month follow-up questionnaire, while 86 (40.38%) completed a 12-month questionnaire.
Intervention Reach and Dose
Table 2 displays the reach of each of the three intervention components. Firstly, a total of 278 (75.54%) employees and managers participated in an obligatory introductory session on mental health and mindfulness. Secondly, 169 (45.92%) of the 368 eligible employees and managers signed up for a 10-week workplace-adapted MBSR course. Lastly, three (75.00%) companies participated in a workshop on further implementation of mindfulness in the company. In Table 3, the received dosage of the 10-week workplace-adapted MBSR course is presented. Across companies, employees, and managers who completed a 10-week workplace-adapted MBSR course, the medians for participation out of 10 sessions were 9 in three of the companies and 8 in one company. Of those employees and managers who discontinued a 10-week workplace-adapted MBSR course, the median dosage was no higher than 2.50 out of 10 sessions before leaving the course.
Tendencies of Change
In Table 4, tendencies of changes in self-reported mental health outcomes from baseline to 3-month and 12-month follow-up are shown. Overall, changes in distal measures of mental health, such as perceived stress, symptoms of depression and anxiety, and well-being, were small to none at both 3-month and 12-month follow-up. However, a positive tendency was seen in the EQ–decentering score at 3 months (1.15 [95% CI − 0.03 to 2.33]), and at 12-month follow-up, this change was statistically significant (1.46 [95% CI 0.02 to 2.89]).
Similarly, Table 5 presents the tendencies of changes from baseline in the organizational outcomes social capital and psychological safety. At 3 months’ follow-up, bonding social capital, linking social capital (overall management), and psychological safety were largely unchanged, while bridging social capital (1.16 [95% CI − 2.17 to 4.50]) and linking social capital (immediate management) (− 1.92 [95% CI − 5.23 to 1.39]) were affected in opposite directions. At 12 months’ follow-up, all social capital subscales showed varying degrees of decrease, including a statistically significant decline in linking social capital (immediate management) (− 8.78 (95% CI − 12.88 to − 4.69)), and a statistically non-significant decline in psychological safety (− 1.54 [95% CI − 3.17 to 0.05]).
The median S-NAQ scores for the three data collection times were as follows: baseline, 11.00 (q25; q75, 9.00; 13.00), 3-month follow-up, 10.00 (q25; q75, 9.00; 12.00), and 12 months, 10.50 (q25; q75, 10.00; 12.00). Table 6 displays odds ratios for occasionally experiencing negative acts (an S-NAQ score of > 12) at 3 and 12 months compared to baseline.
Loss to Follow-Up and Sensitivity Analyses
According to the loss to follow-up analysis for all employees and managers, the baseline characteristics of those who contributed with questionnaire data at 3-month follow-up largely resembled the baseline characteristics of those who did not complete a 3-month follow-up questionnaire (Online Resource 2), as was the case for loss to follow-up at 12-month follow-up. However, a loss to follow-up analysis of employees and managers who did not complete a 10-week workplace-adapted MBSR course (did not sign up or participated in < 4 sessions) revealed that MBSR non-completers who answered a 3-month follow-up questionnaire had a generally better mental health at baseline compared to those MBSR non-completers, who did not answer a 3-month follow-up questionnaire (Online Resource 3). Thus, the MBSR non-completers contributing with 3-month questionnaire data were not representable of the entire sub-population of MBSR non-completers. Moreover, a total of 109 (86.51%) employees and managers who participated in 4–10 sessions of a 10-week workplace-adapted MBSR course completed the 3-month follow-up questionnaire, while 63 (50.00%) completed the 12-month follow-up questionnaire (Online Resource 4). These proportions are in contrast to those of employees and managers who participated in < 4 sessions, where only 30 (34.48%) completed the 3-month questionnaire, and 22 (25.29%) completed the 12-month follow-up questionnaire (Online Resource 4), resulting in a differentiated loss to follow-up between completers and non-completers.
In the sensitivity analyses of continuous outcomes, both mental health and organizational outcome estimates were affected depending on the scenarios (Online Resource 5 and 6). Hence, for several of the estimates, both the direction of the association and the certainty of the estimate were impacted. However, the mental health outcome demonstrating the largest tendency of change in the main analysis, EQ–decentering, showed positive changes in both scenarios. Hence, even if the missing outcomes were set to be 0.2*SD lower than predicted, the change in EQ–decentering still showed a favorable development from baseline to follow-up. However, the association was no longer statistically significant at 12-month follow-up (Online Resource 5). The sensitivity analyses of the dichotomous outcome of occasionally experiencing negative acts showed that the estimated odds ratio at 12-month follow-up may be biased due to the low response rate. Hence, even if data were assumed to be missing at random, non-responders may have had a lower log odds of occasionally experiencing negative acts in the workplace (Online Resource 7).
Discussion
Implementation of mental health–promoting and preventive interventions is crucial in order to ameliorate the global decline of the populations’ mental health. Workplaces have been highlighted as potential mental health–promoting arenas, and MBIs have demonstrated positive effects on mental health outcomes. However, less is known of the feasibility and potential impact of organizational-level workplace MBIs in private workplace settings. The results of this study demonstrate that it is indeed feasible to implement an organizational-level MBI including a 10-week live online workplace-adapted MBSR course in small- and medium-sized private companies, when evaluated using measures for reach and received dose of the intervention. Yet, little to no change was observed in distal mental health outcome measures of perceived stress, symptoms of depression and anxiety, resilience, well-being, and sleep, while mixed tendencies were observed in organizational outcomes.
The feasibility of the intervention was assessed using data on reach of the three intervention components and received dose of the 10-week workplace-adapted MBSR program. A benchmark for an acceptable level of reach when using a population-based strategy to deliver a mental health–promoting and preventive intervention was not found. Overall, 75.54% participated in an introductory session, while 45.92% signed up for a 10-week workplace-adapted MBSR course. In a study by Montero-Marin et al. (2020), in which the authors offered a 6-session workplace-adapted MBSR course in a logistic company, 110 employees out of a total 300 eligible employees (36.66%) chose to decline to participate in the intervention (Montero-Marin et al., 2020). However, the employees contributing with data only amounted to 68 individuals. Based on the baseline characteristics of these individuals, the included employees in the study by Montero-Marin et al. (2020) experienced a higher perceived stress level at baseline compared to the participants in the present study (Montero-Marin et al., 2020). This might indicate that the employees in the study by Montero-Marin et al. may have had a greater incentive to participate than the employees in the present study, which may contribute to a higher participation rate. Thus, based on baseline characteristics of employees and managers in the present study, indicating a moderate mental health across study participants, the reach of the intervention is deemed acceptable.
Dosage cut-points for MBI participation have previously been utilized to evaluate the feasibility of MBIs. Hence, a mean value of half of the sessions attended may indicate that the intervention is appropriate, yet in need of further improvement, whereas participation in 66.67% or more may be deemed feasible (Kuyken et al., 2008; Montero-Marin et al., 2020). The median received dose in the present study was well-above these cut-points, and thus, the received dose is deemed acceptable, supporting the feasibility of this workplace MBI. Moreover, the dose received in this study is comparable to that found in a similar study (Kersemaekers et al., 2018).
This workplace MBI yielded little to no changes in mental health outcomes. Interestingly, this is not in line with results of most previously published research on MBIs in workplace settings (Lomas et al., 2017; Michaelsen et al., 2023; Vonderlin et al., 2020). In a systematic review including 153 studies of MBIs in workplace contexts, the authors found that the vast majority of the included studies demonstrated positive effects on mental health outcomes, such as stress, anxiety, depression, and well-being (Lomas et al., 2017). The reasons why the same tendencies are not present in this study may be explained by several contextual factors as well as methodological considerations. Firstly, employees and managers who contributed with questionnaire data in this study had only a small room for mental health improvement at baseline. Therefore, large changes in mental health outcomes would not be expected (Rose et al., 2008). Secondly, the intervention in the present study was an organizational-level intervention delivered using a population-based strategy. Thus, the intervention was not targeted at selected high-risk group but instead delivered to employees and managers representing individuals across the mental health continuum (Rose et al., 2008). The potential changes in mental health outcomes among employees and managers with poorer mental health—and hence a greater room for improvement—might therefore have been diluted by those individuals with good mental health (Rose et al., 2008). However, this is merely a theoretical proposition. Still, previous research of MBIs in the workplace, with interventions deploying a high-risk strategy, have yielded larger impacts than the tendencies presented in the present study (Huang et al., 2015). Thus, the first and second potential explanation are closely related. Thirdly, the present study was carried out amid the COVID-19 pandemic, resulting in dramatically altered everyday life circumstances both at work and during leisure time. Across countries and population groups, the COVID-19 pandemic negatively impacted the mental health (Chandola et al., 2022; Chiesa et al., 2021; Guo et al., 2020). In Denmark, well-being measured using SWEMWBS decreased statistically significantly among the general population from pre-pandemic 2019 to autumn 2020 (mid-pandemic) (Thygesen et al., 2021). Thus, a sustained level of mental health outcomes, as found in this study, might represent a positive outcome. However, due to the lack of a control group, we do not know what would have happened had we not provided the intervention. Hence, this conclusion must be made with due caution.
However, the results of the present study indicated a tendency of a positive change in the EQ–decentering score, representing skills in detaching oneself from thoughts and feelings. This positive change in decentering is in accordance with mindfulness theory (Shapiro et al., 2006). Thus, by engaging in mindfulness as a practice or a state, individuals may experience a “fundamental shift in perspective” of how they relate to thoughts and feelings (Shapiro et al., 2006), that is, a greater ability to observe one’s experiences without being consumed by them. This shift may proposedly have a positive influence on well-being (Shapiro et al., 2006). Moreover, decentering has been found to aid in maintaining well-being during adversity (Bernstein et al., 2015; Wang et al., 2023). Thus, decentering may act as an intermediate outcome that could potentially influence more distal mental health outcomes. As such, the ability to decenter may be a protective mental health skill. This is in line with previously published qualitative results from this multi-method quasi-experimental research project. The qualitative results indicate that this organizational-level workplace MBI has the potential to positively impact mental health skills, such as enhanced self-care, and present-moment awareness enabling altered behavioral patterns during stressful situations (Bonde et al., 2022). Moreover, similar findings were uncovered in a recent qualitative study conducted among politicians in the UK Parliament (Simonsson et al., 2023). Hence, the mental health–promoting and preventive MBI evaluated in this study may bear greater impact on intermediate outcomes, such as mental health skills, than on more distal mental health outcomes, such as perceived stress and symptoms of depression and anxiety. However, these enhanced mental health skills may protect the participating employees’ and managers’ future mental health.
In this study, we also investigated tendencies of change in organizational outcomes relating to interpersonal relations. At 3-month follow-up, observed changes in these outcomes varied. As such, the social capital between departments/teams (bridging) increased, whereas the social capital between employees and immediate management decreased, while social capital within teams/departments (bonding) and that between employees and overall management were largely unchanged. Additionally, psychological safety also remained largely unchanged at 3-month follow-up. However, at 12-month follow-up, outcomes of social capital and psychological safety all decreased. Yet, the odds of occasionally experiencing negative acts in the workplace reduced statistically significantly from baseline to 3-month follow-up. However, this protective impact diminished from 3-month to 12-month follow-up. Where previous research has contributed to somewhat consistent evidence of the positive mental health effects of MBIs in workplace settings, less is known of the potential organizational impacts of such interventions (Michaelsen et al., 2023; Vonderlin et al., 2020). Still, the majority of research have indicated positive organizational impacts of MBIs (Good et al., 2015; Panditharathne & Chen, 2021; Sajjad & Shahbaz, 2020). The included organizational outcome measures in this study are by definition relational. Hence, workplace social capital, negative acts, and psychological safety are all relational constructs that are affected by human interaction. In the above-mentioned systematic review by Lomas et al. (2017), the authors found no studies reporting either no changes in or worsening of relationships following an MBI delivered in workplace settings (Lomas et al., 2017). Thus, the results from the present study indicating negative tendencies of change in some organizational outcomes are not in line with the majority of the established evidence base. However, the apparent protective impact on negative acts from baseline to 3-month follow-up may potentially be due to improved interpersonal relationships in the workplace. This is in accordance with a recent study of the regulating role of mindfulness in uncivil behavior at work (Hülsheger et al., 2021). In their study, the authors found that high levels of trait mindfulness were associated with low levels of enacted incivility at work (Hülsheger et al., 2021). Moreover, in a study among UK politicians, the authors found that practicing mindfulness in a group may facilitate greater empathy for others and viewing each other as entire human beings as opposed to merely professionals (Simonsson et al., 2023). Thus, delivering MBIs in a group format may play a key role in potential relational effects of such interventions in workplace settings.
However, the present study was conducted as a quasi-experimental study with no control group. Hence, the results regarding tendencies of changes from baseline to the two follow-up points may have been influenced by outside circumstances during the study period and, thus, not solely by the intervention itself. As a result of the COVID-19 pandemic, the intervention period was characterized by national, regional, and local lockdowns, resulting in social distancing and remote work (Fig. 1). Previous research has found that forced remote work during the COVID-19 pandemic may have generated several challenges for the psychosocial work environment (Reznik et al., 2022; Sjöblom et al., 2022; Smith et al., 2022). For example, working from home has been found to negatively affect the social connectedness within the workplace as personal interactions are either conducted virtually or not at all (Reznik et al., 2022). In the present study, the majority of employees and managers were forced to work from home for shorter or longer periods of time during the project due to either national, regional, or local COVID-19-related lockdowns (Fig. 1). Thus, the COVID-19-related forced remote work during the project period may have contributed to the decline in social capital and psychological safety seen in this study. However, regarding the experience of negative acts in the workplace, remote work might be proposed to act as a protective factor (Bollestad et al., 2022). In the current study, baseline data were collected from three out of four companies right before either a national lockdown or implementation of COVID-19 restrictions, such as encouragement to work from home or forced remote work. On the other hand, 3-month follow-up data were collected during a national lockdown in two out of four companies, while it was collected during a time with fewer restrictions in the remaining two companies. Hence, at baseline the majority of employees and managers were physically present at their respective workplace, while at 3-month follow-up, about half was working remotely. Thus, changes in the frequency of negative acts might be due to fewer social interactions in the workplace at 3-month follow-up compared to baseline. However, previous research indicates that negative acts, such as workplace bullying, may persist even during remote work (Kompella, 2022). Additionally, the results are in line with previous research that has demonstrated positive impacts of mindfulness on interpersonal relations, such as reduced incivility at work (Hülsheger et al., 2021; Kay & Skarlicki, 2020; Panditharathne & Chen, 2021). Therefore, the tendency of change in reduced odds of occasionally experiencing negative acts at 3-month follow-up may not be written off as caused entirely by the lack of interactions within the physical workplace. Moreover, sensitivity analyses indicated that the estimated odds ratio of occasionally experiencing negative acts at 12-month follow-up may be biased towards a potential underestimation of the impact at 12-month follow-up. Hence, according to sensitivity analyses, even if data were assumed to be missing at random, non-responders may have had a lower log odds of occasionally experiencing negative acts compared to responders (Online Resource 7). Therefore, the results of the analysis of 12-month follow-up must be interpreted with due caution.
In the present study, tendencies indicated that especially the social capital between employees and the immediate management worsened both at 3- and 12-month follow-up. A study of the impact of remote work on workplace social capital in Nordic companies concluded that remote work may impact negatively on workplace social capital (Bühring et al., 2021). Additionally, a qualitative study found that leading psychologically safe work environments when working remotely requires extensive and deliberate managerial actions compared to non-remote work (Sjöblom et al., 2022). Thus, if managers fail to, e.g., spend extra time interacting virtually with their employees, this may negatively influence the psychosocial work environment between employees and management. Moreover, in a Portuguese case study, the authors found that a decline in the psychosocial work environment during the COVID-19 pandemic persisted even after 2 years of living with the pandemic (Gaspar et al., 2023). Hence, damage done to the psychosocial work environment during the pandemic may have long-term consequences. Thus, the tendencies of change in the psychosocial work environment until 12-month follow-up may possibly be explained by the natural progression of time. Yet, the tendencies of change regarding especially the social capital between employees and management indicated that this workplace MBI probably did not ameliorate such potential negative impacts on the psychosocial work environment. However, at 3-month follow-up, a tendency to improvements was identified in the bridging social capital, that is, the social capital between departments/teams. This is in accordance with mindfulness theory that practicing mindfulness may improve relations (Dahl et al., 2020; Kabat-Zinn, 2013, 2018; Lomas et al., 2017), as well as previous research (Good et al., 2015; Panditharathne & Chen, 2021). Moreover, a recent qualitative study from this multi-method research project also demonstrated positive impacts on bridging social capital (Bonde et al., 2023). Furthermore, only a small decrease was seen on the bridging social capital at 12-month follow-up, this being the smallest decrease in the organizational outcome measures at 12-month follow-up. As such, this workplace MBI may have ameliorated potential negative impacts of the COVID-19 pandemic on the social capital between departments/teams.
This study entails a number of strengths. Firstly, the workplace MBI was delivered as an organizational-level intervention using a population-based approach not only to improve the mental health of employees and managers, but also to contribute to creating healthier psychosocial work environments. Hence, the participating companies committed to implementing mindfulness as part of their organization, and to ensure that all employees and managers had the opportunity to receive the intervention. Therefore, this intervention was a multi-level intervention, including both individuals and organizations. As previously noted, mental health and the quality of (work) communities exist in a mutually enhancing relationship (WHO, 2022a). Thus, implementing interventions that promote both mental health and the psychosocial work environment may yield even stronger mental health–promoting results as opposed to interventions only targeting one of the two. Secondly, this research project was conducted in private workplace settings, whereas previous research has predominantly been carried out in public workplace settings (Janssen et al., 2018; Lomas et al., 2017). Thirdly, the included companies represented workplaces within media, restaurants, production, and IT. Additionally, one of the companies was an international company with divisions across the globe. Thus, the feasibility and tendencies of change are not limited to one business area or one country. Moreover, the included companies represented businesses, such as restaurants, that were heavily impacted by restrictions during the COVID-19 pandemic, as well as a company undergoing an extensive re-organization resulting in uncertainty among employees and managers during the study period. Thus, the findings of this study indicate that the intervention may be feasible even under strained organizational conditions. Lastly, the workplace-adapted MBSR program was systematically developed using best practice guidelines for adapting MBIs (Crane et al., 2017), and closely followed the curriculum of the original 8-week MBSR program. Finally, the intervention was delivered live online via Zoom. Even though face-to-face delivery historically has been the most common mode of delivery, online formats have gained way during the past decade. In a time of an increasing amount of remote work, investigating such live online formats is in line with developments in everyday work life. Moreover, such online formats have previously been found as effective as in-person delivered MBIs measured on mental health outcomes (Aikens et al., 2014; Michaelsen et al., 2023). However, less is known of the organizational impacts of online MBIs. Therefore, this study may add to the growing evidence of online delivery modes of MBIs in workplace settings.
Limitations and Future Research
This study is also characterized by some limitations. Most notably, the quasi-experimental study design without a control group prohibits the conclusion of intervention effects. However, the main purpose of this study was to evaluate the feasibility of the intervention in a private workplace setting. Thus, the study design fulfilled the purpose for which it was intended. Yet, the evaluation of the secondary purpose, that is, the tendencies of change in mental health and organizational outcome measures, was complicated by the study’s susceptibility to changes in time.
Moreover, it was not possible to construct a control group using employees and managers who did not complete a 10-week workplace-adapted MBSR course, as the group of MBSR non-completers who contributed with follow-up data were not representative of the entire group of MBSR non-completers. Thus, the responding MBSR non-completers constituted a highly selected group with pre-existing good mental health (Online Resource 3).
Strongly linked to the study design being susceptible to changes during the project period, the intervention was carried out during the COVID-19 pandemic, resulting in dramatic variations in time. Thus, as described in the “Method” section, differences in contextual factors, such as remote work, at the three measuring points may have impacted the tendencies of change. Hence, especially at baseline where few study participants worked remotely, the opposite was the case at 3-month follow-up. Thus, if factors such as remote work affect the psychosocial work environment or mental health negatively, this difference from baseline to 3-month follow-up may cause a natural decline in these outcomes at 3-month follow-up, independently of the intervention. At 12-month follow-up, however, restrictions had been lifted. Yet, as described above, the psychosocial work environment may have been negatively affected by the COVID-19 pandemic even after restrictions were lifted (Gaspar et al., 2023).
Furthermore, there was a large amount of missing data at both the 3-month questionnaire (34.74%) and the 12-month questionnaire (59.62%), thus resulting in response rates of respectively 65.26% and 40.38% within the group of employees and managers who contributed with baseline data. Low response rate was also the case in previous research of mindfulness in workplace contexts (49.80%) (Hülsheger et al., 2013), as well as the average response rate in organizational surveys (52.30%) (Anseel et al., 2010). The response rate at 12-month follow-up must be considered low when compared to response rates of the above-mentioned previous research. Missing data will always pose a problem for interpretation of the results, as we do not know what those employees and managers that did not contribute with questionnaire data would have answered if they had responded. However, according to the loss to follow-up analyses at 3-month follow-up, baseline characteristics of responders resembled those of non-responders (Online Resource 2). This might indicate that if those who dropped out had contributed with data, the results might have been similar to those observed in the present study. Thus, missing data might mostly have affected the certainty of the estimates. However, this argument must be made with due caution. Sensitivity analyses of the odds of occasionally experiencing negative acts in the workplace revealed that the estimate at 12-month follow-up may be biased due to non-responders (Online Resource 7). Hence, the likelihood of occasionally experiencing negative acts at 12 months must be interpreted cautiously.
Relating to mental health outcomes, these were mostly unchanged from baseline to 3- and 12-month follow-up. However, positive tendencies to improvements in the mental health skill, decentering, were identified. These findings could indicate that this workplace MBI may facilitate improvements in intermediate outcomes, such as skills that protect the mental health, while generating only small to no changes in more distal measures of mental health. Thus, this study would have benefitted from including more measures of such skills. Still, the lack of changes in the distal mental health outcomes might—as previously described—bear witness of an underlying positive tendency, as the general well-being of the Danish population decreased during the intervention period (Thygesen et al., 2021).
This study indicates that it is feasible to implement an organizational-level workplace-adapted MBI in private workplace settings measured on reach and received dose of the intervention. However, the impact of the intervention on mental health outcomes and organizational outcomes is uncertain. Future research would benefit from including one or more control groups, potentially in a randomized controlled design or alternatively utilizing a non-equivalent dependent variable design including one or more variables that would not be expected to change due to the intervention, such as amount of work or demands (Häfner et al., 2015). To evaluate the effectiveness of this organizational-level workplace MBI using a randomized controlled design, effects would have to be evaluated at company-level, and thus, cluster-randomization should be conducted with companies representing clusters. This design, however, will require a large amount of companies enrolling in such trial. Moreover, when using MBIs as interventions to promote mental health and prevent mental health problems, as well as delivering these using a population-based approach, impacts on distal outcome measures, such as perceived stress, and symptoms of depression and anxiety, might be limited (Rose et al., 2008). Hence, future research may benefit from including more measures of intermediate outcomes, such as decentering, to capture potential changes in protective mental health skills. Such skills may contribute to improved mental health beyond the intervention period. Therefore, by not including measures of mental health skills, such as decentering, interventions may wrongfully be deemed ineffective. Moreover, future research should include data on facilitators and barriers to implementation, such as management commitment.
Data Availability
Data will be provided without reservations upon request to the corresponding author.
References
Aikens, K. A., Astin, J., Pelletier, K. R., Levanovich, K., Baase, C. M., Park, Y. Y., & Bodnar, C. M. (2014). Mindfulness goes to work: Impact of an online workplace intervention. Journal of Occupational and Environmental Medicine, 56(7), 721–731. https://doi.org/10.1097/jom.0000000000000209
Anseel, F., Lievens, F., Schollaert, E., & Choragwicka, B. (2010). Response rates in organizational science, 1995–2008: A meta-analytic review and guidelines for survey researchers. Journal of Business and Psychology, 25(3), 335–349. https://doi.org/10.1007/s10869-010-9157-6
Bernstein, A., Hadash, Y., Lichtash, Y., Tanay, G., Shepherd, K., & Fresco, D. M. (2015). Decentering and related constructs: A critical review and metacognitive processes model. Perspectives on Psychological Science, 10(5), 599–617. https://doi.org/10.1177/1745691615594577
Bollestad, V., Amland, J., & Olsen, E. (2022). The pros and cons of remote work in relation to bullying, loneliness and work engagement: A representative study among Norwegian workers during COVID-19. Frontiers in Psychology, 13, 1016368. https://doi.org/10.3389/fpsyg.2022.1016368
Bonde, E. H., Mikkelsen, E. G., Fjorback, L. O., & Juul, L. (2022). Impacting employees’ and managers’ mental health skills using a workplace-adapted mindfulness-based intervention. Frontiers in Psychology, 13, 1020454. https://doi.org/10.3389/fpsyg.2022.1020454
Bonde, E. H., Mikkelsen, E. G., Fjorback, L. O., & Juul, L. (2023). The impact of an organizational-level mindfulness-based intervention on workplace social capital and psychological safety: A qualitative content analysis. Frontiers in Psychology, 14, 1112907. https://doi.org/10.3389/fpsyg.2023.1112907
Borg, V., Mateu, N. C., & Clausen, T. (2014). Udvikling af en ny metode til undersøgelse af social kapital på arbejdspladsen [Development of a new method for studying social capital in the workplace]. NFA. https://nfa.dk/da/Forskning/Udgivelse?journalId=8addb238-1424-4241-8a51-2247c0d9d643.
Bühring, T., Randrup, A. G., & Jørgensen, C. (2021). Fjernarbejdets betydning for arbejdmiljøet i Norden: Rapport om reguleringen og betydningen af fjernarbejde for arbejdsmiljøet i de nordiske lande [The impact of remote work on the work environment in the Nordic countries: Report on the regulation and impact of remote work on the work environment in the Nordic countries]. Oxford Research. https://oxfordresearch.dk/publications/fjernarbejdets-betydning-for-arbejdsmiljoet-i-norden/.
Chandola, T., Kumari, M., Booker, C. L., & Benzeval, M. (2022). The mental health impact of COVID-19 and lockdown-related stressors among adults in the UK. Psychological Medicine, 52(14), 2997–3006. https://doi.org/10.1017/S0033291720005048
Chiesa, V., Antony, G., Wismar, M., & Rechel, B. (2021). COVID-19 pandemic: Health impact of staying at home, social distancing and ‘lockdown’ measures—A systematic review of systematic reviews. Journal of Public Health, 43(3), e462–e481. https://doi.org/10.1093/pubmed/fdab102
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. https://doi.org/10.2307/2136404
Conway, P. M., Høgh, A., Nabe-Nielsen, K., Grynderup, M. B., Mikkelsen, E. G., Persson, R., Rugulies, R., Bonde, J. P. E., Francioli, L., & Hansen, Å. M. (2018). Optimal cut-off points for the Short-Negative Act Questionnaire and their association with depressive symptoms and diagnosis of depression. Annals of Work Exposures and Health, 62(3), 281–294. https://doi.org/10.1093/annweh/wxx105
Crane, R. S., Brewer, J., Feldman, C., Kabat-Zinn, J., Santorelli, S., Williams, J. M., & Kuyken, W. (2017). What defines mindfulness-based programs? The warp and the weft. Psychological Medicine, 47(6), 990–999. https://doi.org/10.1017/s0033291716003317
Crane, R., Bartley, T., Evans, A., Karunavira, Sansom, S., Silverton, S., Soulsby, J., Williams, V., Kuyken, W., Williams, M., Yiangou, A., Fennell, M., Surawy, C., Eames, C., Fletcher, M., Hastings, R., Koerbel, L., & Octigan, K. (2021). Mindfulness-based interventions: Teaching assessment criteria. Bangor University. https://mbitac.bangor.ac.uk/documents/MBITACmanual0517.pdf.
Dahl, C. J., Wilson-Mendenhall, C. D., & Davidson, R. J. (2020). The plasticity of well-being: A training-based framework for the cultivation of human flourishing. PNAS, 117(51), 32197–32206. https://doi.org/10.1073/pnas.2014859117
De Bruin, E. I., van der Meulen, R. T., de Wandeler, J., Zijlstra, B. J. H., Formsma, A. R., & Bögels, S. M. (2020). The Unilever study: Positive effects on stress and risk for dropout from work after the finding peace in a frantic world training. Mindfulness, 11, 350–361. https://doi.org/10.1007/s12671-018-1029-6
De Vibe, M., Bjørndal, A., Fattah, S., Dyrdal, G. M., Halland, E., & Tanner-Smith, E. E. (2017). Mindfulness-based stress reduction (MBSR) for improving health, quality of life and social functioning in adults: A systematic review and meta-analysis. Campell Systematic Reviews, 13(1), 1–264. https://doi.org/10.4073/csr.2017.11
Edmondson, A. (1999). Psychological safety and learning behavior in work teams. Administrative Science Quarterly, 44(2), 350–383. https://doi.org/10.2307/2666999
Eskildsen, A., Dalgaard, V. L., Nielsen, K. J., Andersen, J. H., Zachariae, R., Olsen, L. R., Jorgensen, A., & Christiansen, D. H. (2015). Cross-cultural adaptation and validation of the Danish consensus version of the 10-item Perceived Stress Scale. Scandinavian Journal of Work, Environment & Health, 41(5), 486–490. https://doi.org/10.5271/sjweh.3510
Fresco, D. M., Moore, M. T., van Dulmen, M. H. M., Segal, Z. V., Ma, S. H., Teasdale, J. D., & Williams, J. M. G. (2007). Initial psychometric properties of the experiences questionnaire: Validation of a self-report measure of decentering. Behavior Therapy, 38(3), 234–246. https://doi.org/10.1016/j.beth.2006.08.003
Gaspar, T., Salado, V., do CéuMachado, M., Guedes, F. B., Faia-Correia, M., & Coelho, A. (2023). Impact of COVID-19 on management, quality and satisfaction of health organizations: A case study in a Portuguese hospital. International Journal of Environmental Research, 17(1), 21. https://doi.org/10.1007/s41742-022-00505-7
Good, D., Lyddy, C., Glomb, T., Bono, J., Brown, K., Duffy, M., Bear, R., Brewer, J., & Lazar, S. (2015). Contemplating mindfulness at work: An integrative review. Journal of Management, 42(1), 114–142. https://doi.org/10.1177/0149206315617003
Guo, J., Feng, X. L., Wang, X. H., & van IJzendoorn, M. H. (2020). Coping with COVID-19: Exposure to COVID-19 and negative impact on livelihood predict elevated mental health problems in Chinese adults. International Journal of Environmental Research and Public Health, 17(11), 3857. https://doi.org/10.3390/ijerph17113857
Häfner, A., Stock, A., & Oberst, V. (2015). Decreasing students’ stress through time management training: An intervention study. European Journal of Psychology of Education, 30(1), 81–94. https://doi.org/10.1007/s10212-014-0229-2
Hansen, A. M., Hogh, A., Garde, A. H., & Persson, R. (2014). Workplace bullying and sleep difficulties: A 2-year follow-up study. International Archives of Occupational and Environmental Health, 87(3), 285–294. https://doi.org/10.1007/s00420-013-0860-2
Harris, P. A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J. G. (2009). Research electronic data capture (REDCap)–A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42(2), 377–381. https://doi.org/10.1016/j.jbi.2008.08.010
Hastings, E., Jahanbakhsh, F., Karahalios, K., Marinov, D., & Bailey, B. (2018). Structure or nurture?: The effects of team-building activities and team composition on team outcomes. Proceedings of the ACM on Human-Computer Interaction, 2, 1–21. https://doi.org/10.1145/3274337
Huang, S. L., Li, R. H., Huang, F. Y., & Tang, F. C. (2015). The potential for Mindfulness-based intervention in workplace mental health promotion: Results of a randomized controlled trial. PLoS One, 10(9), e0138089. https://doi.org/10.1371/journal.pone.0138089
Hülsheger, U. R., Alberts, H. J., Feinholdt, A., & Lang, J. W. (2013). Benefits of mindfulness at work: The role of mindfulness in emotion regulation, emotional exhaustion, and job satisfaction. Journal of Applied Psychology, 98(2), 310–325. https://doi.org/10.1037/a0031313
Hülsheger, U. R., van Gils, S., & Walkowiak, A. (2021). The regulating role of mindfulness in enacted workplace incivility: An experience sampling study. Journal of Applied Psychology, 106(8), 1250–1265. https://doi.org/10.1037/apl0000824
Janssen, M., Heerkens, Y., Kuijer, W., van der Heijden, B., & Engels, J. (2018). Effects of mindfulness-based stress reduction on employees’ mental health: A systematic review. PLoS One, 13(1), e0191332. https://doi.org/10.1371/journal.pone.0191332
Kabat-Zinn, J. (2013). Full catastrophe living: How to cope with stress, pain and illness using mindfulness meditation. Bantum Books.
Kabat-Zinn, J (2018) Meditation is not what you think. Hachette Book Group
Kay, A. A., & Skarlicki, D. P. (2020). Cultivating a conflict-positive workplace: How mindfulness facilitates constructive conflict management. Organizational Behavior and Human Decision Processes, 159, 8–20. https://doi.org/10.1016/j.obhdp.2020.02.005
Kersemaekers, W., Rupprecht, S., Wittmann, M., Tamdjidi, C., Falke, P., Donders, R., Speckens, A., & Kohls, N. (2018). A workplace mindfulness intervention may be associated with improved psychological well-being and productivity. A preliminary field study in a company setting Frontiers in Psychology, 9, 195. https://doi.org/10.3389/fpsyg.2018.00195
Khoury, B., Sharma, M., Rush, S. E., & Fournier, C. (2015). Mindfulness-based stress reduction for healthy individuals: A meta-analysis. Journal of Psychosomatic Research, 78(6), 519–528. https://doi.org/10.1016/j.jpsychores.2015.03.009
Killingsworth, M. A., & Gilbert, D. T. (2010). A wandering mind is an unhappy mind. Science, 330(6006), 932. https://doi.org/10.1126/science.1192439
Kompella, S. (2022). Persisting menace: A case-based study of remote workplace bullying in India. International Journal of Bullying Prevention. https://doi.org/10.1007/s42380-022-00152-8
Koushede, V., Lasgaard, M., Hinrichsen, C., Meilstrup, C., Nielsen, L., Rayce, S. B., Torres-Sahli, M., Gudmundsdottir, D. G., Stewart-Brown, S., & Santini, Z. I. (2019). Measuring mental well-being in Denmark: Validation of the original and short version of the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS and SWEMWBS) and cross-cultural comparison across four European settings. Psychiatry Research, 271, 502–509. https://doi.org/10.1016/j.psychres.2018.12.003
Kuyken, W., Byford, S., Taylor, R. S., Watkins, E., Holden, E., White, K., Barrett, B., Byng, R., Evans, A., Mullan, E., & Teasdale, J. D. (2008). Mindfulness-based cognitive therapy to prevent relapse in recurrent depression. Journal of Consulting and Clinical Psychology, 76(6), 966–978. https://doi.org/10.1037/a0013786
Lee, E. H. (2012). Review of the psychometric evidence of the perceived stress scale. Asian Nursing Research, 6(4), 121–127. https://doi.org/10.1016/j.anr.2012.08.004
Lomas, T., Medina, J. C., Ivtzan, I., Rupprecht, S., Hart, R., & Eiroa-Orosa, F. J. (2017). The impact of mindfulness on well-being and performance in the workplace: An inclusive systematic review of the empirical literature. European Journal of Work and Organizational Psychology, 26(4), 492–513. https://doi.org/10.1080/1359432X.2017.1308924
McHenry, J. A., & Donovan, R. J. (2012). Perth Charter for the Promotion of Mental Health and Wellbeing. Seventh World Conference on the Promotion of Mental Health and the Prevention of Mental and Behavioural Disorders, Perth, Western Australia
McNeish, D. (2018). Thanks coefficient alpha, we’ll take it from here. Psychological Methods, 23(3), 412–433. https://doi.org/10.1037/met0000144
Meng, A., Clausen, T., & Borg, V. (2018). The association between team-level social capital and individual-level work engagement: Differences between subtypes of social capital and the impact of intra-team agreement. Scandinavian Journal of Psychology, 59(2), 198–205. https://doi.org/10.1111/sjop.12435
Michaelsen, M. M., Graser, J., Onescheit, M., Tuma, M. P., Werdecker, L., Pieper, D., & Esch, T. (2023). Mindfulness-based and mindfulness-informed interventions at the workplace: A systematic review and meta-regression analysis of RCTs. Mindfulness, 14(6), 1271–1304. https://doi.org/10.1007/s12671-023-02130-7
Montero-Marin, J., Kuyken, W., Gasión, V., Barceló-Soler, A., Rojas, L., Manrique, A., Esteban, R., & Campayo, J. G. (2020). Feasibility and effectiveness of a workplace-adapted mindfulness-based programme to reduce stress in workers at a private sector logistics company: An exploratory mixed methods study. International Journal of Environmental Research and Public Health, 17(5), 1643–1645. https://doi.org/10.3390/ijerph17051643
Moore, G. F., Audrey, S., Audrey, M., Bond, L., Bonell, C., Hardeman, W., Moore, L., O’Cathain, A., Tinati, T., Wight, D., & Baird, J. (2015). Process evaluation of complex interventions: Medical Research Council guidance. British Medical Journal, 350, h1258. https://doi.org/10.1136/bmj.h1258
Muñoz Bohorquez, J., Parra, D. C., Saperstein, S. L., Aparicio, E. M., Lewin, A. B., & Green, K. M. (2023). Feasibility of implementing a mindfulness-based online program for Latina immigrants and the staff that work with them. Mindfulness, 14, 1148–1161. https://doi.org/10.1007/s12671-023-02123-6
Panditharathne, P. N. K. W., & Chen, Z. (2021). An integrative review on the research progress of mindfulness and its implications at the workplace. Sustainability, 13(24), 13852. https://doi.org/10.3390/su132413852
Reznik, J., Hungerford, C., Kornhaber, R., & Cleary, M. (2022). Home-based work and ergonomics: Physical and psychosocial considerations. Issues in Mental Health Nursing, 43(10), 975–979. https://doi.org/10.1080/01612840.2021.1875276
Rose, G., Khaw, K., & Marmot, M. (2008). Rose’s strategy on preventive medicine. Oxford University Press.
Rosendahl Jensen, H. A., Thygesen, L. C., Møller, S. P., Dahl Nielsen, M. B., Ersbøll, A. K., & Ekholm, O. (2022). The Danish Health and Wellbeing Survey: Study design, response proportion and respondent characteristics. Scandinavian Journal of Public Health, 50(7), 959–967. https://doi.org/10.1177/14034948211022429
Rugulies, R., Martin, M. H., Garde, A. H., Persson, R., & Albertsen, K. (2012). Deadlines at work and sleep quality. Cross-sectional and longitudinal findings among Danish knowledge workers. American Journal of Industrial Medicine, 55, 260–269. https://doi.org/10.1002/ajim.21022
Sajjad, A., & Shahbaz, W. (2020). Mindfulness and social sustainability: An integrative review. Social Indicators Research, 150, 73–94. https://doi.org/10.1007/s11205-020-02297-9
Santini, Z. I., Ekholm, O., Koyanagi, A., Stewart-Brown, S., Meilstrup, C., Nielsen, L., Fusar-Poli, P., Fusar-Poli, V., & Thygesen, L. C. (2022). Higher levels of mental wellbeing predict lower risk of common mental disorders in the Danish general population. Mental Health & Prevention, 26, 200233. https://doi.org/10.1016/j.mhp.2022.200233
Santorelli, S. (2014). Mindfulness-based stress reduction (MBSR): Standards of practice. University of Massachusetts Medical School. Retrieved April 26, 2024 from https://mindfulness.au.dk/fileadmin/mindfulness.au.dk/Artikler/Santorelli_mbsr_standards_of_practice_2014.pdf
Shapiro, S. L., Carlson, L. E., Astin, J. A., & Freedman, B. (2006). Mechanisms of mindfulness. Journal of Clinical Psychology, 62(3), 373–386. https://doi.org/10.1002/jclp.20237
Simonsson, O., Bergljottsdotter, C., Narayanan, J., Fisher, S., Bristow, J., Ormston, R., & Chambers, R. (2023). Mindfulness in politics: A qualitative study on mindfulness training in the UK Parliament. Mindfulness, 14, 1362–1370. https://doi.org/10.1007/s12671-023-02156-x
Sjöblom, K., Mäkiniemi, J. P., & Mäkikangas, A. (2022). “I was given three marks and told to buy a Porsche” - Supervisors’ experiences of leading psychosocial safety climate and team psychological safety in a remote academic setting. International Journal of Environmental Research and Public Health, 19(19), 12016. https://doi.org/10.3390/ijerph191912016
Skivington, K., Matthews, L., Simpson, S. A., Craig, P., Baird, J., Blazeby, J. M., Boyd, K. A., Craig, N., French, D. P., McIntosh, E., Petticrew, M., Rycroft-Malone, J., White, M., & Moore, L. (2021). A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. British Medical Journal, 374, n2061. https://doi.org/10.1136/bmj.n2061
Smith, B. W., Dalen, J., Wiggins, K., Tooley, E., Christopher, P., & Bernard, J. (2008). The brief resilience scale: Assessing the ability to bounce back. International Journal of Behavioral Medicine, 15, 194–200. https://doi.org/10.1080/10705500802222972
Smith, P., Oudyk, J., Cedillo, L., Inouye, K., Potter, G., & Mustard, C. (2022). The psychosocial work environment among educators during the COVID-19 pandemic. Occupational Medicine, 72(7), 439–445. https://doi.org/10.1093/occmed/kqac050
Stewart-Brown, S., Tennant, A., Tennant, R., Platt, S., Parkinson, J., & Weich, S. (2009). Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS): A Rasch analysis using data from the Scottish Health Education Population Survey. Health and Quality of Life Outcomes, 7, 15. https://doi.org/10.1186/1477-7525-7-15
Strand, B. H., Dalgard, O. S., Tambs, K., & Rognerud, M. (2003). Measuring the mental health status of the Norwegian population: A comparison of the instruments SCL-25, SCL-10, SCL-5 and MHI-5 (SF-36). Nordic Journal of Psychiatry, 57(2), 113–118. https://doi.org/10.1080/08039480310000932
Tambs, K., & Moum, T. (1993). How well can a few questionnaire items indicate anxiety and depression? Acta Psychiatrica Scandinavica, 87(5), 364–367. https://doi.org/10.1111/j.1600-0447.1993.tb03388.x
Thygesen, L. C., Møller, S. P., Ersbøll, A. K., Santini, Z. I., Nielsen, M. B. D., Grønbæk, M. K., & Ekholm, O. (2021). Decreasing mental well-being during the COVID-19 pandemic: A longitudinal study among Danes before and during the pandemic. Journal of Psychiatric Research, 144, 151–157. https://doi.org/10.1016/j.jpsychires.2021.09.035
Vago, D., & David, S. (2012). Self-awareness, self-regulation, and self-transcendence (S-ART): A framework for understanding the neurobiological mechanisms of mindfulness. Frontiers in Human Neuroscience, 6, 296. https://doi.org/10.3389/fnhum.2012.00296
van Agteren, J., Iasiello, M., Lo, L., Bartholomaeus, J., Kopsaftis, Z., Carey, M., & Kyrios, M. (2021). A systematic review and meta-analysis of psychological interventions to improve mental wellbeing. Nature Human Behaviour, 5, 631–652. https://doi.org/10.1038/s41562-021-01093-w
Vonderlin, R., Biermann, M., Bohus, M., & Lyssenko, L. (2020). Mindfulness-based programs in the workplace: A meta-analysis of randomized controlled trials. Mindfulness, 11(7), 1579–1598. https://doi.org/10.1007/s12671-020-01328-3
Wang, Y., Garland, E. L., & Farb, N. A. S. (2023). An experimental test of the mindfulness-to-meaning theory: Casual pathways between decentering, reappraisal, and well-being. Emotion, 23(8), 2243–2258. https://doi.org/10.1037/emo0001252
WHO. (2018). Fact sheet on sustainable development goals: Health targets - Mental health. https://www.who.int/europe/publications/i/item/WHO-EURO-2018-2364-42119-58012
WHO. (2021). Comprehensive mental health action plan 2013–2030. https://www.who.int/publications/i/item/9789240031029
WHO. (2022a). WHO guidelines on mental health at work. https://www.who.int/publications/i/item/9789240053052
WHO. (2022b). World mental health report: Transforming mental health for all. https://www.who.int/publications/i/item/9789240049338
Windle, G., Bennett, K. M., & Noyes, J. (2011). A methodological review of resilience measurement scales. Health and Quality of Life Outcomes, 9, 8. https://doi.org/10.1186/1477-7525-9-8
Zheng, D., Berry, D. R., & Brown, K. W. (2023). Effects of brief mindfulness meditation and compassion meditation on parochial empathy and prosocial behavior toward ethnic out-group members. Mindfulness, 14(10), 2454–2470. https://doi.org/10.1007/s12671-023-02100-z
Acknowledgements
The authors would like to thank all employees and managers who participated in this study. Moreover, we would like to thank the company representatives who took the opportunity to engage their company in this research project. Furthermore, a heartfelt thank you to the MBSR teachers Bente Pedersen, Mie Glud Pedersen, and Camilla Marcinkowski for invaluable contributions to the development and delivery of the 10-week workplace-adapted MBSR program.
Funding
Open access funding provided by Aarhus Universitet This study was funded by The Velliv Association (Grant Number: 19-0506). The Velliv Association did not influence the study design, data collection and analysis, interpretation of the results, manuscript draft, or the decision to publish the results.
Author information
Authors and Affiliations
Contributions
Emilie Hasager Bonde: methodology, formal analysis and investigation, writing—original draft preparation, writing—review and editing. Eva Gemzøe Mikkelsen: conceptualization, writing—review and editing. Lone Overby Fjorback: writing—review and editing. Lise Juul: conceptualization, methodology, formal analysis and investigation, writing—review and editing, funding acquisition, supervision
Corresponding author
Ethics declarations
Ethics Approval
This study was performed in accordance with the principles of the Declaration of Helsinki. Approval was provided by the Danish Data Protection Agency (February 13 2020/2016–051-000001/1715).
Consent to Participate
Before providing consent, all eligible subjects received written information on the research project, and intention to publish results thereof. In accordance with national legislation, consent was obtained from all subjects involved in the study upon contribution with questionnaire data.
Competing Interests
The Danish Center for Mindfulness, Department of Clinical Medicine, Aarhus University offers revenue-funded MBSR courses and MBSR teacher training. The authors declare that they have no financial interests.
Disclaimer
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Artificial Intelligence
No artificial intelligence services were used during the preparation of this paper.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bonde, E.H., Mikkelsen, E.G., Fjorback, L.O. et al. Exploring an Organizational-Level Mindfulness-Based Intervention in Private Workplace Settings. Mindfulness 15, 1453–1471 (2024). https://doi.org/10.1007/s12671-024-02375-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-024-02375-w