
Abstract
Objectives
Mindfulness meditation has been claimed to decrease aspects of egoic functioning (EF). However, empirical evidence is largely lacking or is suggesting the reverse. Therefore, the aim was to examine the associations between mindfulness, mindfulness interventions, egoic functioning, and emotional well-being using different designs.
Method
We conducted three studies: (i) a cross-sectional study in the general population (n = 796), (ii) an experiment in a student population (n = 84) where we manipulated mindfulness meditation, and (iii) an intervention in self-enrolled individuals from the general population receiving a standard 8-week Mindfulness-Based Stress Reduction (MBSR) program (n = 165).
Results
In the cross-sectional study, most mindfulness facets showed positive (mainly with self-enhancement) or nonsignificant associations with facets of EF. In the experiment, participants in the mindfulness meditation (vs. control) condition exhibited lower self-enhancement of positive characteristics. In the intervention, some aspects of EF decreased (e.g. demanding control), whereas some increased (e.g. refusal to comply) after MBSR, and these changes correlated meaningfully with changes in self-reported mindfulness and well-being.
Conclusions
The results suggest that aspects of EF are differentially associated with aspects of self-reported mindfulness and differentially respond to a brief mindfulness manipulation and an 8-week MBSR intervention. We formulated two dimensions on which various relevant self-concept constructs may be positioned: competition-based versus compassion-based.
Preregistration
The studies are not preregistered.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Mindfulness meditation has become popular in Western societies, and the number of studies examining its effects, mechanisms, and moderators has risen dramatically over the past few decades (Goldberg et al., 2017). Mindfulness meditation programs enhance psychological well-being (e.g. decreases in symptoms of depression and anxiety, increases in quality of life) compared to waiting-list and treatment-as-usual control groups (Goldberg et al., 2017, 2018; Hoge et al., 2021; Khoury et al., 2013, 2015). We define mindfulness as “a process of regulating attention in order to bring a quality of nonelaborative awareness to current experience and a quality of relating to one’s experience within an orientation of curiosity, experiential openness, and acceptance” (Bishop et al., 2004, p. 234). It is derived from Buddhist psychology, in which decreases in self-centred psychological activity are considered central to the alleviation of human suffering (Ekman et al., 2005; Thera, 1972). This corresponds to modern psychological theory positing that “hypo-egoic functioning” facilitates healthy psychosocial functioning (Brown & Leary, 2016).
An alternative perspective has advocated that boosting one’s view of the self, even if illusory, is adaptive and associated with better psychosocial functioning (Taylor & Brown, 1988). Such self-enhancement processes can be defined as activity “to enhance positivity of self-conceptions or protect the self from negative information” (Sedikides, 1993, p. 318). A recent meta-analysis provided evidence for beneficial effects of self-enhancement for indices of psychological well-being, while effects were mixed for interpersonal adjustment (Dufner et al., 2019).
Seemingly in contrast to Buddhist theory claiming that meditation practice decreases self-centred psychological activity (Leary et al., 2006), recent literature has reported that meditation practice can be associated with increased, instead of decreased, self-enhancement (Gebauer et al., 2018; Vaughan-Johnston et al., 2021; Vonk & Visser, 2021). A subset of these studies (Gebauer et al., 2018; Vaughan-Johnston et al., 2021) is of particular relevance. Using a within-subject design involving samples with varying degrees of meditation experience, the studies found that, after having meditated (vs. not) for 15 min, participants scored higher on measures of self-enhancement. While intriguing, the studies and findings raise several questions.
The first question is related to the independent variable, meditation. These studies used metta, or loving-kindness, meditation as their manipulation. Meditation is a broad construct, even when confined to techniques with Buddhist origin, and attempts to classify them have not reached consensus to date (Cahn & Polich, 2006; A. Lutz et al., 2015; Travis & Shear, 2010). However, metta meditation differs from mindfulness meditation. The former focuses on producing positive feelings towards oneself and others, whereas mindfulness is focused on just being aware, nonjudgmentally, of what is happening in the present moment (Bishop et al., 2004). This distinction has been interpreted as reflecting fundamentally different cognitive processes: constructive (metta) versus deconstructive (mindfulness) (Dahl et al., 2015). Constructive meditation techniques involve cultivating wholesome psychological states or processes, while deconstructive meditation techniques aim at diminishing unwholesome psychological processes related to self-centredness. Although the originally hypothesised mechanism for self-enhancement (i.e. enhanced self-centrality, meaning the activity one invests time in becoming more important) is assumed to be true for any activity (Gebauer et al., 2018), it is conceivable that the more deconstructive mindfulness meditation may affect self-centred functioning quite differently from the more constructive metta meditation.
The second question is related to the outcome variable, self-enhancement. Self-enhancement was operationalised by a combination of three measures: so-called better-than-average, communal narcissism, and self-esteem (Gebauer et al., 2018; Vaughan-Johnston et al., 2021). Better-than-average is an often used measure of self-enhancement in which participants indicate to what extent they are better (or worse) than the average other participant of the study on usually favourable characteristics. Communal narcissism refers to strong self-enhancement tendencies in communal domains, which were assumed to be (metta) meditation relevant. However, it has been suggested that the items of the scale, such as “I am the most helpful person I know”, may not reflect a process of self-enhancement per se, but may reflect a genuine commitment to do good deeds, especially in socially sensitive meditators (Lumma et al., 2020). Finally, the authors also included self-esteem as a measure of self-enhancement based on previous empirical findings indicating that self-esteem is associated with aspects of self-enhancement (Sedikides & Gregg, 2008). Although it is argued that self-esteem and self-enhancement are not the same (Paulhus, 1998; Pelham & Swann, 1989), their three measures used did load on one second-order factor, suggesting one overarching concept. Results showed that effects of metta meditation (Experiment 2 in both studies) were somewhat different between the measures and between the two studies: while self-esteem was enhanced after meditation in both studies, communal narcissism was not, and the effect of better-than-average was dependent on the context: desirable characteristics in mainly the communal area (e.g. kind-hearted) were enhanced in the original study involving regular meditators versus non-communal (general; e.g. intelligent) desirable characteristics were enhanced in the replication study involving students (Gebauer et al., 2018; Vaughan-Johnston et al., 2021). It seems clear that the effects are depending on the construct assessed and the context in which they are studied.
In addition to the specific construct of self-enhancement, recently, it has been suggested to include a broader range of constructs related to egoic functioning besides self-enhancement as operationalised above to establish a more nuanced view on the matter (Lumma et al., 2020). Egoic functioning (EF) is defined as a broad construct involving various aspects of psychological functioning associated with self-interest with four, partly overlapping, general features: (i) self-preoccupation (cognition dominated by own life and outcomes), (ii) egocentrism (interpretation of events from own perspective), (iii) egoism (precedence on own outcomes over those of others), and (iv) heteronomy (behaviour controlled by own or others’ fixed images or expectations) (Brown & Leary, 2016). As the more deconstructive mindfulness (insight) forms of meditation have been posited to diminish EF (Dahl et al., 2015; Leary et al., 2006), it would be worthwhile to examine the associations of mindfulness and mindfulness meditation with different constructs that putatively tap into one or more of these four general features of EF.
Self-enhancement may be seen as primarily reflecting the facet of self-preoccupation, with probable influences by heteronomic motives (Paulhus & Reid, 1991). Narcissism includes an exaggerated form of self-enhancement (Foster et al., 2003; John & Robins, 1994). Narcissism often also includes egoistic and egocentric cognitions and behaviour (Back et al., 2013), although not necessarily as, for example, in the case of communal narcissism. Communal narcissism includes the same motives regarding grandiosity, self-esteem, entitlement, and power as the more prototypical agentic narcissism, but accomplished by communal means (Gebauer et al., 2012). The construct of social desirability (Crowne & Marlowe, 1964) may also be relevant as it taps more specifically into the heteronomic facet of EF. Finally, self-esteem has an unclear position within EF: it is associated with self-enhancement (and therefore self-preoccupation), but theoretically self-esteem is a construct distinct from EF, to which self-enhancement contributes as one of many factors (Gebauer et al., 2018; Paulhus, 1998; Pelham & Swann, 1989). As a result, the broader term of self-concept seems more appropriate when referring to all the above constructs together (i.e. EF constructs plus self-esteem).
Aspects of EF may be differentially adaptive or maladaptive in relation to emotional well-being (Baumeister et al., 2000, 2003; Dufner et al., 2019; Paulhus, 1998; Sedikides & Gregg, 2008). Because reduction of EF is claimed to be involved in the well-being enhancing effects of mindfulness (Ekman et al., 2005; Thera, 1972), it would be worthwhile to examine if any mindfulness-related changes in EF may be associated with changes in emotional well-being.
As a result of the above, the main purpose of the present series of studies was a first exploration of the associations between facets of EF, mindfulness, and well-being, generating directions for new hypotheses in this new research area. To this end, the following three explorative, not preregistered, studies are reported here:
-
(i)
A correlational study in the general population examining associations of aspects of EF (self-enhancement, narcissism, and egocentrism) and self-esteem, with aspects of self-reported mindfulness and emotional well-being,
-
(ii)
A pilot experimental study manipulating mindfulness by a brief intervention and examining its effects on aspects of EF (self-enhancement and narcissism), self-esteem, and emotional well-being, and
-
(iii)
A pre-post Mindfulness-Based Stress Reduction (MBSR) intervention study examining changes across time in aspects of EF (egocentrism and desirable responding), self-reported mindfulness facets, and emotional well-being.
Study 1
Method
Participants and Procedure
Dutch adults (n = 888) from a representative sample were participants in an online survey study in January and February 2022. Research assistants completed recruitment, as part of a second-year course in the Bachelor Psychology program of Tilburg University. Quota sampling was used to warrant an equal number of included men and women across various age ranges: 18–30, 31–40, 41–50, 51–60, 61–70, and 71 and above. Each research assistant recruited a total of 22 participants from the general population within these age ranges. Inclusion criteria were a sufficient comprehension of the Dutch language. The participants completed informed consent after being informed about the purpose of the study. Participants were asked to complete the questionnaire either digitally (www.qualtrics.com) or on paper.
Measures
Mindfulness
The Dutch short form (Bohlmeijer et al., 2011) of the Five Facet Mindfulness Questionnaire (Baer et al., 2006) (FFMQ-SF) was used to assess the widely studied five mindfulness skills using the following subscales: Observing (of sensory phenomena), Describing (one’s thoughts and feelings), Acting with Awareness, Nonjudging (one’s thoughts and feelings), and Nonreacting (to disturbing thoughts and images). The 24 items are scored on 5-point scales ranging from 1 (never or very rarely true) to 5 (very often or always true). The FFMQ-SF has shown adequate psychometric properties, such as Cronbach’s α ranging from 0.73 (Nonreacting) to 0.91 (Describing), construct validity, and sensitivity to change (Bohlmeijer et al., 2011).
Self-enhancement
EF was assessed using four instruments. First, we administered the often-used “better-than-average” operationalisation of self-enhancement, in which people rate themselves on favourable characteristics in comparison to most other people. Specifically, the current version was based on the 10-item Self-Attributes Questionnaire (Pelham & Swann, 1989), reflecting agentic characteristics such as intelligence, physical attractiveness, and sense of humour. Participants rated themselves to what extent they possessed each of these characteristics “compared to most other people of your age and sex you know” on 7-point scales going from 1 (much less than others) to 7 (much more than others). The original version was found to be reliable (Cronbach’s α of 0.76) and valid regarding substantial correlations with self-esteem (Pelham & Swann, 1989).
Narcissism
Next, two aspects of narcissism were assessed, a general classical form reflecting feelings of greatness, and communal narcissism. The general classical narcissism was assessed using the Admiration subscale from the Narcissistic Admiration and Rivalry Questionnaire (Back et al., 2013). The subscale consists of 9 items, such as “I am great” and “I show others how special I am”, which are scored on 6-point Likert scales ranging from 1 (does not apply at all) to 6 (applies completely). It has shown good reliability (Cronbach’s α of 0.87) and validity (Back et al., 2013). A 4-item version of the Communal Narcissism Inventory (Gebauer et al., 2012) was used, which has also been used in a previous study (Gebauer et al., 2018). Items, such as “I will be well known for the good deeds I will have done”, were scored on the same 6-point Likert scale and the 4-item version has shown adequate reliability (mean Cronbach’s α of 0.71 and 0.83) and validity regarding correlations with other measures of self-enhancement (Gebauer et al., 2018; Vaughan-Johnston et al., 2021).
Egocentrism
The Tilburg Index of Egocentrism (TIE) (Nyklíček, 2023) was used to assess other facets of EF, more related to egoism and egocentrism. Specifically, three facets are assessed: the strong need to be the one determining the course of things (Demanding Control; 6 items; Cronbach α = 0.86, example item “I can’t stand it when things don’t go my way”); the belief that the one’s views and opinions are superior (Superior Opinion; 5 items; Cronbach α = 0.82, example item “My views and opinions are great”); and the refusal to cooperate (Refusal; 4 items; Cronbach α = 0.74, example item “If I don’t like it, then it won’t happen”). The 15 items were scored on 5-point Likert scales ranging from (almost) never to (almost) always. Besides adequate reliability, the scale has shown acceptable construct validity as reflected by substantial correlations with related constructs such as desire for control and autonomy (Nyklíček, 2023).
Self-esteem
The Rosenberg Self-Esteem Scale (RSES) (Rosenberg, 1965) was used to assess global self-esteem. The 10-item version includes items such as “On the whole, I’m satisfied with myself”, which are scored on 4-point Likert scales ranging from completely disagree to completely agree. The scale has been widely used with adequate reliability and validity, also in Dutch samples (Franck et al., 2008; Rosenberg, 1965).
Anxiety
Symptoms of anxiety were assessed using the 7-item Generalized Anxiety Disorder scale (GAD-7) (Spitzer et al., 2006). Participants were asked to rate symptoms over the past 2 weeks on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day), with total scores ranging from 0 to 21. The Dutch version of the GAD-7 shows adequate reliability and validity (Donker et al., 2011).
Depression
Depressive symptoms over 2 weeks were assessed using the Dutch version of the 9-item Patient Health Questionnaire (Kroenke et al., 2001). Participants were asked to rate items on a 4-point Likert scale from 0 (not at all) to 3 (nearly every day), with higher scores reflecting more symptoms of depression. The PHQ-9 shows adequate psychometric properties (Kroenke et al., 2001; Löwe et al., 2004).
Data Analyses
Statistical analyses were conducted with SPSS version 26. Data were first screened for missing values, reliability of the (sub)scales, and assumptions underlying the analysis used. Pearson’s product-moment correlations were computed to examine associations between variables. Therefore, the distributions of the variables included in these analyses were first checked for normality.
Results
Out of the 888 participants who started the questionnaire, 796 (90%) completed the whole questionnaire set. Age ranged between 18 and 86 (mean 49 ± 17 years). Of the participants, 436 (55%) were female. Most people had a partner (605; 76%). A small majority was highly educated (high professional or university education; 412; 52%), while 561 (71%) had a paid job and 89 (11%) were students. The vast majority of the participants (96%) identified as European Dutch. A minority of 203 (26%) participants stated that they sometimes meditate (defined as a mental exercise mainly involving practicing attentiveness/mindfulness).
All scales showed a normal distribution (all skewness and kurtosis < 1.50), except symptoms of anxiety and depression, which were somewhat negatively skewed (2.10 and 2.15, respectively). Reliability of the scales was satisfactory (all Cronbach α > 0.70 with the lowest being for Nonreacting with an α of 0.71).
Pearson product-moment correlations among the self-concept measures showed that almost all were significantly correlated (p < 0.001), except self-esteem with two egocentrism subscales: Demanding Control and Refusal (r < 0.10). Self-esteem correlated most strongly with better-than-average, the two aspects of narcissism correlated most strongly with each other, and also the egocentrism subscales showed the strongest correlations among themselves (Table 1).
Most self-concept measures correlated positively with mindfulness facets, especially self-esteem, reaching r = 0.51 with the Acting with Awareness facet (Table 1). An exception was the Demanding Control scale, which correlated weakly negatively with Acting with Awareness and Nonjudging, and Refusal, which showed no associations with mindfulness facets (Table 1).
Regarding symptoms of anxiety and depression, they correlated negatively with self-esteem and better-than-average, while Demanding Control correlated weakly positively with anxiety and depression, and the other measures of self-concept did not (all r < 0.10) (Table 1).
Discussion
Various facets of self-concept (EF and self-esteem) seem to correlate differently with various facets of mindfulness. Most EF constructs correlate (modestly) positively with several mindfulness facets. However, the strongest association was found for self-esteem, which is not surprising in light of (i) theories and empirical evidence indicating that both self-esteem and mindfulness are psychologically favourable constructs generally positively associated with psychological well-being (Baumeister et al., 2003; Brown & Ryan, 2003; Brown et al., 2007; Pelham & Swann, 1989) and (ii) studies showing mindfulness interventions to increase self-esteem (Britton et al., 2021). At the same time, as some studies have suggested that self-esteem is substantially related to unrealistic self-enhancement (Gebauer et al., 2018), the positive associations with EF constructs may seem to oppose the notion that mindfulness should diminish EF (Brown et al., 2008; Thera, 1972). Indeed, the better-than-average measure of self-enhancement was positively associated with four out of five mindfulness facets in the current study.
However, it must be noted that the current correlational design does not allow for causal conclusions. Several alternative explanations are possible. For example, people overly positive in self-reports about themselves might also be inclined to overreport their mindfulness skills, which could be seen as a form of self-enhancement generalisation. If that were a valid explanation, it may explain the (small) association found between narcissistic tendencies and the nonreacting and describing facets of mindfulness. Also other, unmeasured, variables (e.g. genetics, attachment, life events) might be responsible for these associations found, making them spurious. To be able to draw clearer conclusions, other designs are needed, including mainly experimental studies. Experimental design was applied in Study 2 to address these considerations.
Study 2
This study involved a pilot experimental study comparing the effect of brief mindfulness instruction versus an active control condition on aspects of EF and momentary affect.
Method
Participants
Eighty-four undergraduate students at an American university volunteered to participate as partial fulfilment of a class requirement. Two participants did not complete the intervention (one did not have headphones on, and one consistently used their cell phone during the intervention) and were subsequently removed from analyses. The final sample of 82 had a mean age of 20 (SD = 3) and were primarily male (n = 47; female n = 35) and non-Hispanic White (n = 73; Asian/Pacific Islander n = 5; non-Hispanic Black n = 4). This sample resulted in a power of 0.61 to detect a group difference effect of medium effect size (f = 0.25).
Measures
Self-enhancement
A version of the “better-than-average” operationalisation was used. Participants were asked to evaluate themselves against the average student of their age and gender at their university on 23 positive traits (e.g. creativity, academic ability) and 19 negative traits (e.g. anxious, manipulative) using a 7-point scale ranging from Much less than the average college student of my age and gender to Much more than the average college student of my age and gender (Taylor et al., 2003). Both the positive (α = 0.86) and the negative (α = 0.78) scales demonstrated good internal consistency.
Narcissism
Narcissism was assessed with the Narcissism Personality Inventory-16 (Ames et al., 2006), which uses a forced choice scale (e.g. “I prefer to blend in with the crowd” vs. “I like to be the centre of attention”). The scale’s internal consistency was adequate (α = 0.72).
Self-esteem
The same Rosenberg Self-Esteem Scale (Rosenberg, 1965), which was used in Study 1, was also used in Study 2. The scale demonstrated good internal consistency (α = 0.90).
State positive affect
State positive affect was assessed with the Positive and Negative Affect Schedule-short version (Thompson, 2007), which consists of five items (e.g. “inspired”, “alert”) regarding how participants felt “right now”, and which were evaluated with a 5-point scale, ranging from Not at all to A lot. The scale demonstrated good internal consistency (α = 0.91).
Manipulation check
The validity of the mindfulness manipulation was assessed with two items (“How effective do you think the audios were for increasing attentional skills?” and “How much have your attentional skills improved as a result of the audio practice?”). These items were evaluated with a 5-point scale ranging from Not at all to Very much. The scale demonstrated good internal consistency (α = 0.87).
Interventions
The mindfulness and control interventions were adapted from previous research (Ostafin et al., 2012) by shortening the instructions. Both interventions were presented as practices designed to increase attention skills and delivered as audio recordings. The mindfulness intervention consisted of instructions to simply observe the sensations of breathing and whenever participants became distracted by thoughts, emotions, or body sensations, to return the attention to the breath without judgment of the distraction or the self as good or bad. The control audios consisted of passages from a research methodology textbook (Rosenthal & Rosnow, 1991), and in line with other attention training interventions (Wells, 1990), the control training audio instructed participants to return their attention back to the audio whenever they became distracted from it. Thus, the control intervention mainly controlled for a main practice of mindfulness: noticing distractions and redirecting the attention to a focus.
Procedure
Participants completed assessment procedures in groups consisting of one to four participants seated in cubicles that were partitioned on the front and sides and with a half-closed drape at the back, allowing the researcher to see if any problems occurred. After signing an informed consent form, participants completed basic demographic measures. Participants were then semi-randomly assigned to condition, with even-numbered participants assigned to one condition (control) and odd-numbered participants assigned to the other (mindfulness). In order to reduce potential fatigue, the interventions were spaced over three practice periods, with the first lasting 10 min and the second and third lasting 5 min each. Brief filler questionnaires (approximately 2 min) unrelated to this study followed the first two practice audios. After the second practice audio, the state positive affect measure was administered (before the filler questionnaire). After the third practice audio, participants completed the self-concept measures in the following order: self-enhancement, narcissism, self-esteem. After this, the participants completed the manipulation check items and were then debriefed.
Data Analyses
Statistical analyses were conducted with SPSS version 26. Data were first screened for missing values and assumptions underlying the analysis used. As there was no pre-assessment of the dependent measures, the hypothesis that mindfulness administration would be associated with enhanced self-enhancement (Gebauer et al., 2018) was assessed with independent samples t-tests on the outcome variables. Also group comparisons on the manipulation check and state positive affect were also examined with independent samples t-tests. Therefore, the distributions of the variables included in these analyses were first checked for normality. Six participants did not complete the manipulation check (four from the control condition and two from the mindfulness condition).
Results
There were no baseline differences between the groups regarding gender or age (p > 0.36). Analyses on the effects of the intervention on the manipulation check of perceived improvement in attentional skills and on state positive affect revealed that compared to the control group, the mindfulness group reported that the intervention had more effect on their attentional skills t(74) = 4.86, p < 0.001, Cohen’s d = 1.11, 95% confidence interval = 0.67–1.55. The mindfulness group also reported more state positive affect, t(80) = 2.89, p = 0.005, Cohen’s d = 0.65, 95% confidence interval = 0.21–1.09. Attention skills improvement and positive affect were positively correlated (r = 0.62, p < 0.001), while both variables were unrelated to the self-concept measures (Table 2).
Compared to the control group, the mindfulness group demonstrated a tendency towards less self-enhancement, which was significant for self-enhancement of positive traits (t(80) = 2.30, p = 0.02, Cohen’s d = 0.50, 95% confidence interval = 0.06–0.94). Effects were of small to medium sized (Table 3).
Discussion
The findings seem generally opposite to similar recent reports (Gebauer et al., 2018; Vaughan-Johnston et al., 2021). However, an important difference between the current study and the previous studies is the manipulation: while in previous studies metta (loving-kindness) meditation was used, in the present study the meditation was based on mindfulness. As discussed in the introduction, this may be a crucial difference as the practice of loving-kindness meditation is focused on producing positive feelings towards oneself and other beings, while mindfulness is focused on just being aware, nonjudgmentally, of what is happening in the present moment (Bishop et al., 2004; Thera, 1972). Because the outcome variables were highly similar to those utilised in the previous studies, the results seem to indicate that effects of meditation on self-enhancement are dependent on the contents of the meditation. Self-enhancement may be facilitated by meditation focused on enhancing kind and loving feelings towards oneself and others, while self-enhancement may indeed be diminished by the neutrally observing quality of mindfulness meditation. The latter effect is in line with both Buddhist (Thera, 1972) and psychological theories of mindfulness (Brown & Leary, 2016; Brown et al., 2007).
However, an important caution regarding this conclusion arises from two limitations of the current study, namely the lack of a baseline assessment of the outcome measures while the sample size is small. Although the sample was quasi-randomised and there were no differences between the groups in age or sex, we cannot exclude the possibility that due to chance the relatively small groups failed to be randomised on the baseline scores of the outcome variables, which may form an alternative explanation of the current results found. The findings regarding manipulation check and effects on state positive affect suggest that the mindfulness intervention was active, supporting the idea that the effects on self-enhancement were due to the mindfulness training, but we cannot rule out the alternative explanation just offered. In addition, the present somewhat underpowered between-subjects design may have facilitated the potential effects of this limitation, in addition to introducing a between-subjects error variance. Another limitation of the current study is the relatively homogenous sample, preventing generalisation to other populations.
The next step consisted of studying the associations between changes in EF, changes in mindfulness facets, and changes in psychological symptoms over the course of a full standard 8-week MBSR intervention.
Study 3
Method
Participants and Procedure
Self-selected participants of a standard 8-week MBSR training were asked for participation in one or two studies including a pre-post intervention survey study and an ecological monitoring study. An online screening was performed to examine potential exclusion criteria, if necessary supplemented by a telephone interview. According to G*Power 3.1.9.2, 171 participants would be needed to test pre-post changes using a paired samples t-test able to show a relatively small effect (Cohen’s d = 0.25) with a power of 0.90. For bivariate correlations between variables, able to also show a relatively small effect (r = 0.25) with the same power, a sample of 164 participants would suffice.
The exclusion criteria were assessed by the first author. Exclusion criteria were severe psychiatric disorders (e.g. current severe major depression episode, suicidal, or psychotic tendencies) and an inability to read and write in Dutch. Exclusion criteria were assessed by an online intake form and, if needed, followed up by a brief telephone interview by the first author. None of the individuals interested in the MBSR program was excluded due to presence of exclusion criteria. Participants provided written informed consent before the start of the study, after which they received the first set of questionnaires to be completed before the start of the MBSR program. After the end of the program, they were asked to complete the same questionnaires prior to intervention.
Measures
The questionnaire included questions on demographic and clinical variables, and scales assessing measures of EF, mindfulness, mood, perceived stress, and general well-being.
Egocentrism
The same TIE scale was applied as in Study 1.
Desirability
The 11-item Repressive Defensiveness subscale from the Weinberger Adjustment Inventory (Weinberger & Schwartz, 1990) was used to assess the tendency to deny own mild, but common, undesirable behaviour, so it may be seen as a measure of desirable responding. Examples of items are “Once in a while‚ I say bad things about people that I would not say in front of them” and “Once in a while‚ I say things that are not completely true” (both items reverse scored). The statements are answered on 5-point scales ranging from 1 (false) to 5 (true). The Dutch version showed adequate reliability (Cronbach’s α = 0.83) and validity (substantial correlation with the Marlowe-Crowne Social Desirability Scale) (Crowne & Marlowe, 1964) of r = 0.48 (Nyklíček et al., 1998).
Mindfulness
Mindfulness was assessed using the full FFMQ (Baer et al., 2006). The questionnaire consists of 39 items that address the same five facets of mindfulness as assessed in Study 1 by the following subscales: Observing (of sensory phenomena), Describing (one’s thoughts and feelings), Acting with Awareness, Nonjudging (one’s thoughts and feelings), and Nonreacting (to disturbing thoughts and images). Each item is rated on a 5-point Likert scale ranging from 1 (never or very rarely true) to 5 (very often or always true). The Dutch translation is used, which has shown adequate psychometric properties (Bohlmeijer et al., 2011), highly similar to the original (Baer et al., 2006, 2008).
Mood
Mood in the past period was assessed using the Dutch version (Wald & Mellenbergh, 1990) of the short form of the Profile of Mood States (POMS-SF; Shacham, 1983). The Dutch version consists of 32 self-report items asking participants how they feel “lately”, covering five subscales: Depression, Anxiety, Irritation, Fatigue, and Vitality. Each item is rated on a 5-point Likert scale ranging from 1 (not at all) to 5 (extremely). Studies have shown adequate convergent and discriminant validity of the POMS-SF (Baker et al., 2002; Wald & Mellenbergh, 1990).
Perceived Stress
The Perceived Stress Scale (PSS; Cohen et al., 1983) consists of 14 questions regarding the amount of stress the participants experienced in the past period. Items include items such as “How often have you been upset because of something that happened unexpectedly” and “how often have you felt that things were going your way” (reversed scoring). Participants answered the questions on a scale from 0 (never) to 4 (constantly/always). The PSS has good reliability (Cronbach’s α = 0.84–0.86), as well as discriminant and predictive validity (Cohen et al., 1983, 1993). The Dutch version used in the present study also showed good reliability (Cronbach’s α = 0.87) and concurrent and predictive validity (De Vries & Drent, 2004).
General Well-being
The World Health Organization index of Well-being (WHO-5; Bonsignore et al., 2001) consists of 5 items assessing general well-being with statements such as “I have felt cheerful and in good spirits” and “My daily life has been filled with things that interest me”. These items are scored on 6-point scales ranging from 0 (At no time) to 5 (All of the time). It has shown adequate reliability (e.g. Cronbach α of 0.82) and validity, also of the Dutch version (Bonsignore et al., 2001; de Wit et al., 2007).
Data Analyses
Statistical analyses were conducted with SPSS version 26. Data were first screened for missing values and assumptions underlying the analysis used. First, to test if changes from pre- to post-intervention were significant, paired samples t-tests were used. Pearson’s product-moment correlations were computed to examine associations between constructs, both at baseline and for associations between pre-post intervention changes. Therefore, the distributions of the variables included in these analyses were first checked for normality. Because classic pre-post intervention change scores showed reliability ranging from adequate to low (Gu et al., 2018), instead residuals were used of the regression of post-intervention scores on pre-intervention scores of the same variables.
Results
Participant Characteristics
Of the 193 individuals who participated in the MBSR program, 181 (94%) individuals agreed to complete the questionnaires for the study. Of those who agreed, 177 (98%) completed the pre-intervention questionnaires. This sample consisted of 129 (73%) women, 126 (71%) were highly educated (finished high vocational education or college/university), 134 (76%) had a paid job of at least 20 hr per week, 116 (66%) were married or were living together with a partner, age range was 20–63 years (mean of 43 years, SD of 10 years). A majority of the sample had some form of previous psychological treatment: 37 (21%) for depression, 24 (14%) for anxiety, 38 (22%) for stress-related complaints, and 33 (19%) for other symptoms. Current use of psychotropic medication was reported by 33 participants (19%), mainly antidepressants (15%).
Eleven (6%) MBSR participants dropped out of the program (attended less than 6 out of 8 sessions). Of the participants who completed the pre-intervention questionnaires, 165 (93%) also completed the post-intervention questionnaires. Cronbach’s alpha values of study variables were all α > 0.70 (lowest for Desirability at pre-intervention with an α of 0.73).
Baseline Correlations
In line with the correlations in Study 1, all egocentrism subscales intercorrelated significantly, but only Demanding Control correlated significantly with Desirability (r = − 0.26, p < 0.001; Table 4).
EF constructs showed differential associations with aspects of self-reported mindfulness. While Demanding Control correlated significantly negatively with all mindfulness facets, Desirability correlated positively with 3 out of 5 mindfulness facets, Refusal correlated positively with one, and Superior Opinion did not correlate with mindfulness at all (Table 4). A similar pattern of correlations was obtained with measures of psychological well-being, albeit reversed in sign for those measures reflecting complaints (Table 4).
Changes Between Pre- and Post-MBSR
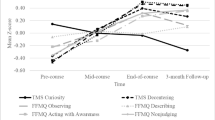
First, post-MBSR scores on all measures of psychological problems, well-being, and mindfulness facets were significantly different from pre-intervention scores in the expected directions showing medium-to-large effects (Table 5). Regarding changes in aspects of EF, changes from pre- to post-intervention were different between the various facets. While Demanding Control and Superior Opinion decreased, Refusal and Desirability increased, with only small effect sizes (Table 5 and Fig. 1).

Change in aspects of egoic functioning from pre-to-post Mindfulness-Based Stress Reduction program
Associations Between Changes
Pearson’s correlations between pre-post intervention changes in aspects of EF and changes in mindfulness facets revealed that while increases in two out of five mindfulness facets were significantly associated with a decrease in Demanding Control, increases in one or two out of five mostly other mindfulness facets were associated with increases in Superior Opinion, Refusal, and Desirability (Table 6). Regarding associations with changes in well-being, these largely inversely mirrored those with changes in mindfulness: while change in emotional complaints positively correlated with change in Demanding Control, the reverse is true for changes in mainly Refusal and Desirability (Table 6).
Discussion
The results of this study clearly show differential associations between mindfulness and facets of EF. However, the pattern of associations seems rather consistent across the following approaches: (i) one measurement time (pre-intervention) associations, (ii) changes from pre- to post-mindfulness intervention, and (iii) associations between changes in mindfulness, egoic functioning, and well-being from pre-to-post intervention.
For instance, one facet of EF, demanding control, showed consistent negative patterns of associations with mindfulness: negative correlations with all five mindfulness facets at pre-intervention, a decrease in scores on this facet from pre- to post-mindfulness intervention, and this decrease was associated with increases in two mindfulness facets over the course of the intervention. Associations in the opposite direction were found with well-being measures and emotional complaints. Among the four EF constructs, demanding control also showed the strongest associations with mindfulness (intervention) and well-being (negative). These findings fit well with the Buddhist theory of decreasing egoic functioning associated with less suffering after meditation practice, particularly involving ego-related desires, called taṇhā (Harvey, 2013). Although desire for control has also been theorised to be a universal and adaptive human desire (Burger & Cooper, 1979; Shapiro et al., 1996), it has also been found to be potentially maladaptive in contexts in which one does not have the possibility to exert much control (Shapiro et al., 1996), sometimes leading to psychopathology (Blackledge & Hayes, 2001; Hayes, 2004). The associations found in the present study were strongest in the context of a mindfulness-based stress reduction intervention, a context in which participants often experience a misfit between desire for control and actual control. The Demanding Control subscale used in the present studies may even tap into the more rigid form of desire for control with items such as “I can’t stand it when things don’t go my way”, which as a construct is rather opposite to adaptive constructs such as psychological flexibility (Kashdan & Rottenberg, 2010) and mindfulness, especially regarding the non-judgmental aspect of these constructs.
The reverse pattern was found for the facet of refusal (to comply), although the correlations with mindfulness facets and well-being at the pre-intervention moment were lower or absent. However, refusal increased from pre- to post-MBSR and this increase correlated with decreases in emotional complaints. In the context of MBSR, this may not be surprising as many participants joining this intervention express a tendency to usually put others’ needs in the forefront often at the expense of their own well-being (anecdotal reports from the current mindfulness trainer), which is also reflected in the relatively low scores on refusal at pre-intervention in the present study. Thus, in the present context, an increase in refusal to comply with wishes of others may actually be a favourable development for the participants.
Desirability correlated positively with various mindfulness facets at baseline and showed a small increase between pre- and post-intervention, and its increase correlated modestly with increase in the mindfulness facets of acting with awareness and nonreacting. These outcomes are in line with the few studies examining the association between social desirability and self-reported mindfulness (Baer et al., 2004; Brown & Ryan, 2003). The present results extend those findings by also showing a modest increase in desirable responding with participation in MBSR.
However, given the uncontrolled nature of this study, we cannot conclude that changes between pre- and post-intervention are due to the intervention. Nevertheless, because the changes were largely in line with correlations between aspects of EF and self-reported mindfulness at baseline and with correlations between changes in both classes of variables, this supports the possibility that the changes actually were related to participation in MBSR. An additional limitation of this study is that previous experience with mindfulness was not assessed, which may have influenced the results.
In conclusion, it seems that different aspects of EF show different associations with self-reported mindfulness and with participation in a mindfulness-based intervention. This will be discussed more extensively in the general discussion.
General Discussion
The present series of studies on the association between mindfulness, aspects of EF, and well-being involved (i) a correlational study in the general population, (ii) experimental study in student population, and (iii) intervention study in self-enrolled participants from the general population.
Across three studies, different aspects of self-concept were differentially associated with (i) aspects of self-reported mindfulness, (ii) administration of a brief mindfulness manipulation, and (iii) an 8-week MBSR intervention. Some aspects of EF and self-concept in general showed positive associations and some negative and some no associations with self-reported mindfulness and participation in mindfulness interventions.
Several aspects of self-concept were positively associated with self-reported mindfulness in a large sample of the general population (Study 1), mainly self-esteem and self-enhancement as assessed by the better-than-average operationalisation. However, these two measures exhibited lower scores after a brief mindfulness instruction, compared to a control condition, in a sample of students (Study 2). The decreased self-esteem scores after a mindfulness instruction were not anticipated as mindfulness-based interventions have been shown to generally increase self-esteem (Randal et al., 2015; Shonin et al., 2013). However, those effects are usually seen in samples with relatively low pre-intervention self-esteem, while in our experimental study, participants were students with normal-to-high levels of self-esteem (on average a 5 on a scale from 1 to 6). In addition, perhaps in a sample mostly inexperienced regarding meditation, a one-time brief mindfulness instruction might have been a relatively difficult task, with a (transient) negative consequence for self-esteem (although positive affect increased). However, the absence of a baseline assessment reduces the confidence in a conclusion along causal lines.
The lack of a control group in the MBSR intervention study (Study 3) also does not permit conclusions along causal lines, where a decrease in demanding control was shown between pre- and post-intervention. This facet of EF was also the one most consistently showing negative associations with mindfulness facets and the decrease in this facet over the course of the intervention was also associated with an increase in some mindfulness facets, prudently suggesting a consistency with the claimed hypo-egoic effect of mindfulness meditation (Brown & Leary, 2016; Thera, 1972).
However, two aspects of EF increased, slightly but significantly, over the course of the MBSR intervention: refusal and desirability. In the case of refusal, the relatively low baseline levels may point towards an explanation. Analogous to the often seen relatively low self-esteem at pre-intervention in psychological intervention groups, a low level of assertiveness may be expected. During the MBSR courses, participants learn to take better care of themselves, including standing up for themselves when needed (Kabat-Zinn, 1990). This effect may be reflected in post-intervention higher scores on items such as “If I don’t feel like it, I won’t do it”, probably reflecting not just an aspect of EF, but also assertiveness and taking care of oneself. Thus, this effect may be seen as adaptive in this context. Below we will attempt to enhance the conceptual and functional clarity among these various concepts.
The case of desirability is more complex as it is unclear what the extant measuring instruments, including ours, reflect exactly. In the literature, various constructs have been claimed to be involved, such as the more socially oriented impression management and defensiveness, and the more internally oriented self-deceptive self-enhancement (Paulhus, 1998; Weinberger & Davidson, 1994). In either case, the measure seems to reflect an aspect of EF, whether directed at impressing the other or (unconsciously) maintaining a favourable image of oneself. The enhancement of desirability across the course of a mindfulness-based intervention may then be seen as not in line with the claimed hypo-egoic effect of meditation, but rather in line with the self-enhancement hypothesis of meditation (Gebauer et al., 2018). However, again, because of the lack of a control group, the effects seen cannot be confidently ascribed to the intervention, although change in desirability correlated positively with change in two out of five self-reported mindfulness facets.
It may also be worthwhile to note that the hypo-egoic effects of meditation have been claimed not to take place in a short time frame (Thera, 1972), such as an 8-week MBSR intervention. Buddhist meditators practice intensely for many years in order to decrease EF, which the so-called three poisons (craving, hatred, and delusion of being an independent self) are a reflection of (Ekman et al., 2005). It is conceivable that a standard, relatively brief, 8-week MBSR aiming at stress reduction in usually meditation-naïve participants with stress-related problems might have effects on aspects of EF that are different from effects of long-term meditation practice, which usually also has a more ambitious aim (e.g. complete liberation from attachments and aversions causing suffering). While in an MBSR context, enhancement of aspects of one’s self-concept may be observed and even beneficial as discussed above, hypo-egoic effects may be more associated with long-term practice. Some evidence for the latter effect is found in a study in which experienced meditators showed altered cortical responses to self-relevant stimuli suggesting less self-focus (J. Lutz et al., 2016). In a qualitative study among experienced Buddhist meditators, meditation was even accompanied with a complete loss of a sense of self (Ekici et al., 2020).
In addition, several factors other than the sort of meditation practiced and meditation experience may be important in influencing possible effects of meditation on changes in self-concept. Besides baseline levels of the outcome variable, these factors may include attitude towards meditation (especially in meditation-naïve participants), and the purpose and expectations of practicing meditation.
In conclusion, the three studies reported here, together with the two previous experimental studies on effects of brief meditation (Gebauer et al., 2018; Vaughan-Johnston et al., 2021), have shown that effects of meditation on EF and self-concept in general are not clear-cut and seem to depend on (i) the kind of meditation practiced (e.g. metta or mindfulness) and (ii) the kind of self-concept used. Regarding the kind of mediation practiced, future studies should directly compare the effects of different meditation techniques in one study.
Here, we propose two dimensions of the EF and broader self-concept variables, which may be important to discern: (i) competitive self-interest and (ii) compassionate self-regard. Competitive self-interest involves the classic EF facets (Brown & Leary, 2016), which reflect some kind of competition in various life areas, including both material and immaterial areas (e.g. status, perceived spiritual level). This dimension is therefore strongly related to the concept of contingent self-esteem: self-esteem depending on the extent to which one lives to some interpersonal or intrapsychic expectations (Deci & Ryan, 1995). Regarding the constructs used in the present series of studies, putatively most are high on this dimension: self-enhancement, narcissism, desirability, demanding control, feelings of superiority of opinion, which all involve some kind of comparison or competition. This dimension has been shown to have both adaptive and less adaptive aspects, depending on the conceptualisation used and the context, e.g. intrapersonal versus interpersonal and safe versus threatening (Baumeister et al., 1996; Paulhus, 1998). This may have been reflected in our studies in which some of the concepts were positively (e.g. self-enhancement), some were negatively (e.g. demanding control), and some were largely unrelated (e.g. narcissism) to mindfulness and emotional well-being.
In contrast, the second dimension, compassionate self-regard, does not involve competitiveness, but involves a compassionate attitude towards oneself. One’s value does not depend on one’s accomplishments or even characteristics, but is derived from the simple fact of being a sentient being. Such an attitude is strongly related to concepts such as true, noncontingent self-esteem (Deci & Ryan, 1995; Kernis, 2003) and self-compassion (Neff, 2003; Neff & Vonk, 2009). In our studies, this dimension may have partly been reflected by the constructs of self-esteem and possibly also the construct of refusal insofar it reflects self-compassionate self-care. However, self-esteem and refusal are likely also affected by the first dimension, as both constructs are also boosted by aspects of EF, such as self-preoccupation and egocentrism, protection or enhancement of ones self-view being an important motive (Deci & Ryan, 1995; Neff, 2003). In our studies, both constructs were largely positively associated with mindfulness and emotional well-being. This is in line with previous research showing that self-compassion is enhanced by MBSR (Britton et al., 2021).
Limitations and Future Research
Not being able to draw conclusions in causal terms is a major limitation of the present series of studies, as a result of (i) the correlational design of Study 1, (ii) absence of a baseline assessment together with a small and homogenous sample in Study 2, and (iii) absence of a control group in Study 3, as discussed above in more detail. As the general approach of the current series of studies in this recently started new area of meditation-related research was explorative, broadening the scope of earlier studies to include mindfulness and a broader range of EF and self-concept constructs, the main purpose was to explore these associations and to facilitate new ways of thinking and hypothesis generation for the design of future studies examining the associations between mindfulness, aspects of self-concept, and well-being more rigorously.
Additional limitations include the still somewhat limited number of EF and related constructs and the samples used in the present studies reduce the generalisability to other EF constructs, other samples, and other contexts. Finally, all constructs have been assessed by self-report, which may have consequences for the validity. As has been suggested earlier, future research may aim at implementing multi-method approaches, including reports by significant others, implicit measures, or even more objective assessments using computerised tasks (Paulhus, 1998; Paulhus et al., 2003).
Future research may further examine the relevance of aspects of the two proposed self-concept dimensions of competitive self-interest and compassionate self-regard in the processes involved in mindfulness meditation. In such studies, it is important to take into account the influence of various personal and contextual factors, such as the motivation why participants meditate, the kind of meditation used, the length of the meditation program, and baseline characteristics of the participants. Needless to say that well-designed randomised intervention and other experimental studies are needed to be able to draw conclusions along causal lines.
Data Availability
Data and analysis scripts used for these studies can be accessed at Open Science Framework: https://osf.io/pfr4z/. Materials used in the present study can be accessed by the respective references provided in the Methods sections of Studies 1–3.
References
Ames, D. R., Rose, P., & Anderson, C. P. (2006). The NPI-16 as a short measure of narcissism. Journal of Research in Personality, 40(4), 440–450. https://doi.org/10.1016/j.jrp.2005.03.002
Back, M. D., Kufner, A. C. P., Dufner, M., Gerlach, T. M., Rauthmann, J. F., & Denissen, J. J. A. (2013). Narcissistic admiration and rivalry: Disentangling the bright and dark sides of narcissism. Journal of Personality and Social Psychology, 105(6), 1013–1037. https://doi.org/10.1037/a0034431
Baer, R. A., Smith, G. T., & Allen, K. B. (2004). Assessment of mindfulness by self-report: The Kentucky Inventory of Mindfulness Skills. Assessment, 11(3), 191–206. https://doi.org/10.1177/1073191104268029
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13(1), 27–45. https://doi.org/10.1177/1073191105283504
Baer, R. A., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., Walsh, E., Duggan, D., & Williams, J. M. (2008). Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment, 15(3), 329–342. https://doi.org/10.1177/1073191107313003
Baker, F., Denniston, M., Zabora, J., Polland, A., & Dudley, W. N. (2002). A POMS short form for cancer patients: Psychometric and structural evaluation. Psycho-Oncology, 11(4), 273–281. https://doi.org/10.1002/pon.564
Baumeister, R. F., Smart, L., & Boden, J. M. (1996). Relation of threatened egotism to violence and aggression: The dark side of high self-esteem. Psychological Review, 103(1), 5–33. https://doi.org/10.1037/0033-295X.103.1.5
Baumeister, R. F., Campbell, J. D., Krueger, J. I., & Vohs, K. D. (2003). Does high self-esteem cause better performance, interpersonal success, happiness, or healthier lifestyles? Psychological Science, 4(1), 1–44. https://doi.org/10.1111/1529-1006.01431
Baumeister, R. F., Bushman, B. J., & Campbell, W. K. (2000). Self-esteem, narcissism, and aggression Does violence result from low self-esteem. or from threatened egotism? Current Directions in Psychological Science, 9(1), 26–29 https://doi.org/10.1111/1467-8721.00053
Bishop, S. R., Lau, M. A., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., Segal, Z. V., Abbey, S., Speca, M., Velting, D., & Devins, G. (2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science and Practice, 11(3), 230–241. https://doi.org/10.1093/clipsy/bph077
Blackledge, J. T., & Hayes, S. C. (2001). Emotion regulation in acceptance and commitment therapy. Journal of Clinical Psychology, 57(2), 243–255. https://doi.org/10.1002/1097-4679
Bohlmeijer, E., ten Klooster, P. M., Fledderus, M., Veehof, M., & Baer, R. (2011). Psychometric properties of the Five Facet Mindfulness Questionnaire in depressed adults and development of a short form. Assessment, 18(3), 308–320. https://doi.org/10.1177/1073191111408231
Bonsignore, M., Barkow, K., Jessen, F., & Heun, R. (2001). Validity of the five-item WHO Well-Being Index (WHO-5) in an elderly population. European Archives of Psychiatry and Clinical Neuroscience, 251 Suppl 2, II27–31. https://doi.org/10.1007/BF03035123
Britton, W. B., Desbordes, G., Acabchuk, R., Peters, S., Lindahl, J. R., Canby, N. K., Vago, D. R., Dumais, T., Lipsky, J., Kimmel, H., Sager, L., Rahrig, H., Cheaito, A., Acero, P., Scharf, J., Lazar, S. W., Schuman-Olivier, Z., Ferrer, R., & Moitra, E. (2021). From self-esteem to selflessness: An evidence (gap) map of self-related processes as mechanisms of mindfulness-based interventions. Frontiers in Psychology, 12, 730972. https://doi.org/10.3389/fpsyg.2021.730972
Brown, K. W., & Leary, M. R. (2016). The emergence of scholarship and science on hypo-egoic phenomena. In K. W. Brown & M. R. Leary (Eds.), The Oxford Handbook of Hypo-Egoic Phenomena (pp. 3–14). Oxford University.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822–848. https://doi.org/10.1037/0022-3514.84.4.822
Brown, K. W., Ryan, R. M., & Creswell, J. D. (2007). Mindfulness: Theoretical foundations and evidence for its salutary effects. Psychological Inquiry, 18(4), 211–237. https://doi.org/10.1080/10478400701598298
Brown, K. W., Ryan, R. M., Creswell, J. D., & Niemiec, C. P. (2008). Beyond me: Mindful responses to social threat. In H. A. Wayment & J. J. Bauer (Eds.), Transcending self-interest: Psychological explorations of the quiet ego (pp. 75–84). APA.
Burger, J. M., & Cooper, H. M. (1979). The desirability of control. Motivation and Emotion, 3(4), 381–393. https://doi.org/10.1007/BF00994052
Cahn, B. R., & Polich, J. (2006). Meditation states and traits: EEG, ERP, and neuroimaging studies. Psychological Bulletin, 132(2), 180–211. https://doi.org/10.1037/0033-2909.132.2.180
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. https://doi.org/10.2307/2136404
Cohen, S., Tyrrell, D. A., & Smith, A. P. (1993). Negative life events, perceived stress, negative affect, and susceptibility to the common cold. Journal of Personality and Social Psychology, 64(1), 131–140. https://doi.org/10.1037//0022-3514.64.1.131
Crowne, D. P., & Marlowe, D. (1964). The approval motive. Wiley.
Dahl, C. J., Lutz, A., & Davidson, R. J. (2015). Reconstructing and deconstructing the self: Cognitive mechanisms in meditation practice. Trends in Cognitive Science, 19(9), 515–523. https://doi.org/10.1016/j.tics.2015.07.001
De Vries, J., & Drent, M. (2004). Relationship between perceived stress and sarcoidosis in a Dutch patient population. Sarcoidosis Vasculitis and Diffuse Lung Diseases, 21(1), 57–63.
de Wit, M., Pouwer, F., Gemke, R. J., Delemarre-van de Waal, H. A., & Snoek, F. J. (2007). Validation of the WHO-5 Well-Being Index in adolescents with type 1 diabetes. Diabetes Care, 30(8), 2003–2006. https://doi.org/10.2337/dc07-0447
Deci, E. L., & Ryan, R. M. (1995). Human autonomy: The basis for true self-esteem. In M. H. Kernis (Ed.), Efficacy, agency, and self-esteem (pp. 31–49). Plenum.
Donker, T., van Straten, A., Marks, I., & Cuijpers, P. (2011). Quick and easy self-rating of Generalized Anxiety Disorder: Validity of the Dutch web-based GAD-7, GAD-2 and GAD-SI. Psychiatry Research, 188(1), 58–64. https://doi.org/10.1016/j.psychres.2011.01.016
Dufner, M., Gebauer, J. E., Sedikides, C., & Denissen, J. J. A. (2019). Self-enhancement and psychological adjustment: A meta-analytic review. Personality and Social Psychology Review, 23(1), 48–72. https://doi.org/10.1177/1088868318756467
Ekici, C., Garip, G., & Van Gordon, W. (2020). The lived experiences of experienced vipassana Mahasi meditators: An interpretative phenomenological analysis. Mindfulness, 11(1), 140–152. https://doi.org/10.1007/s12671-018-1063-4
Ekman, P., Davidson, R. J., Ricard, M., & Wallace, B. A. (2005). Buddhist and psychological perspectives on emotions and well-being. Current Directions in Psychological Science, 14(2), 59–63. https://doi.org/10.1111/j.0963-7214.2005.00335.x
Foster, J. D., Campbell, W. K., & Twenge, J. M. (2003). Individual differences in narcissism: Inflated self-views across the lifespan and around the world. Journal of Research in Personality, 37(6), 469–486. https://doi.org/10.1016/S0092-6566(03)00026-6
Franck, E., De Raedt, R., Barbez, C., & Rosseel, Y. (2008). Psychometric properties of the Dutch Rosenberg Self-Esteem Scale. Psychologica Belgica, 48(1), 25–35. https://doi.org/10.5334/pb-48-1-25
Gebauer, J. E., Sedikides, C., Verplanken, B., & Maio, G. R. (2012). Communal narcissism. Journal of Personality and Social Psychology, 103(5), 854–878. https://doi.org/10.1037/a0029629
Gebauer, J. E., Nehrlich, A. D., Stahlberg, D., Sedikides, C., Hackenschmidt, A., Schick, D., Stegmaier, C. A., Windfelder, C. C., Bruk, A., & Mander, J. (2018). Mind-body practices and the self: Yoga and meditation do not quiet the ego but instead boost self-enhancement. Psychological Science, 29(8), 1299–1308. https://doi.org/10.1177/0956797618764621
Goldberg, S. B., Tucker, R. P., Greene, P. A., Simpson, T. L., Kearney, D. J., & Davidson, R. J. (2017). Is mindfulness research methodology improving over time? A Systematic Review. PLoS ONE, 12(10), e0187298. https://doi.org/10.1371/journal.pone.0187298
Goldberg, S. B., Tucker, R. P., Greene, P. A., Davidson, R. J., Wampold, B. E., Kearney, D. J., & Simpson, T. L. (2018). Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clinical Psychology Review, 59, 52–60. https://doi.org/10.1016/j.cpr.2017.10.011
Gu, Z., Emons, W. H. M., & Sijtsma, K. (2018). Review of issies about classical change scores: A multilevel modeling perspective on some enduring beliefs. Psychometrika, 83, 674–695. https://doi.org/10.1007/s11336-018-9611-3
Harvey, P. (2013). An introduction to Buddhism: Teachings, history and practices. Cambridge University.
Hayes, S. C. (2004). Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behavior Therapy, 35(4), 639–665. https://doi.org/10.1016/S0005-7894(04)80013-3
Hoge, E. A., Acabchuk, R. L., Kimmel, H., Moitra, E., Britton, W. B., Dumais, T., Ferrer, R. A., Lazar, S. W., Vago, D., Lipsky, J., Schuman-Olivier, Z., Cheaito, A., Sager, L., Peters, S., Rahrig, H., Acero, P., Scharf, J., Loucks, E. B., & Fulwiler, C. (2021). Emotion-related constructs engaged by mindfulness-based interventions: A systematic review and meta-analysis. Mindfulness, 12(5), 1041–1062. https://doi.org/10.1007/s12671-020-01561-w
John, O. P., & Robins, R. W. (1994). Accuracy and bias in self-perception - individual-differences in self-Enhancement and the role of narcissism. Journal of Personality and Social Psychology, 66(1), 206–219. https://doi.org/10.1037/0022-3514.66.1.206
Kabat-Zinn, J (1990) Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. Delacourt.
Kashdan, T. B., & Rottenberg, J. (2010). Psychological flexibility as a fundamental aspect of health. Clinical Psychology Review, 30(7), 865–878. https://doi.org/10.1016/j.cpr.2010.03.001
Kernis, M. H. (2003). Toward a conceptualization of optimal self-esteem. Psychological Inquiry, 14, 1–26. https://doi.org/10.1207/S15327965PLI1401_01
Khoury, B., Lecomte, T., Fortin, G., Masse, M., Therien, P., Bouchard, V., Chapleau, M. A., Paquin, K., & Hofmann, S. G. (2013). Mindfulness-based therapy: A comprehensive meta-analysis. Clinical Psychology Review, 33(6), 763–771. https://doi.org/10.1016/j.cpr.2013.05.005
Khoury, B., Sharma, M., Rush, S. E., & Fournier, C. (2015). Mindfulness-based stress reduction: A meta-analysis. Journal of Psychosomatic Research, 78(6), 519–528. https://doi.org/10.1016/j.jpsychores.2015.03.009
Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Leary, M. R., Adams, C. E., & Tate, E. B. (2006). Hypo-egoic self-regulation: Exercising self-control by diminishing the influence of the self. Journal of Personality, 74(6), 1803–1832. https://doi.org/10.1111/j.1467-6494.2006.00429.x
Löwe, B., Kroenke, K., Herzog, W., & Grafe, K. (2004). Measuring depression outcome with a brief self-report instrument: Sensitivity to change of the Patient Health Questionnaire (PHQ-9). Journal of Affective Disorders, 81(1), 61–66. https://doi.org/10.1016/S0165-0327(03)00198-8
Lumma, A. L., Heidenreich, T., & Michalak, J. (2020). How would the Buddha rate on Rosenberg’s self-esteem scale? Mindfulness, 11(2), 521–526. https://doi.org/10.1007/s12671-019-01281-w
Lutz, A., Jha, A. P., Dunne, J. D., & Saron, C. D. (2015). Investigating the phenomenological matrix of mindfulness-related practices from a neurocognitive perspective. American Psychologist, 70(7), 632–658. https://doi.org/10.1037/a0039585
Lutz, J., Bruhl, A. B., Doerig, N., Scheerer, H., Achermann, R., Weibel, A., Jancke, L., & Herwig, U. (2016). Altered processing of self-related emotional stimuli in mindfulness meditators. NeuroImage, 124(Pt A), 958–967. https://doi.org/10.1016/j.neuroimage.2015.09.057
Neff, K. D. (2003). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2(2), 85–101. https://doi.org/10.1080/15298860309032
Neff, K. D., & Vonk, R. (2009). Self-compassion versus global self-esteem: Two different ways of relating to oneself. Journal of Personality, 77(1), 23–50. https://doi.org/10.1111/j.1467-6494.2008.00537.x
Nyklíček, I., Vingerhoets, A. J. J. M., Van Heck, G. L., & Van Limpt, M. C. (1998). Defensive coping in relation to casual blood pressure and self-reported daily hassles and life events. Journal of Behavioral Medicine, 21(2), 145–161. https://doi.org/10.1023/A:1018775807593
Nyklíček, I. (2023). The tilburg index of egocentrism. https://osf.io/xh8aw/
Ostafin, B. D., Bauer, C., & Myxter, P. (2012). Mindfulness decouples the relation between automatic alcohol motivation and drinking behavior. Social and Clinical Psychology, 31(7), 729–745. https://doi.org/10.1521/jscp.2012.31.7.729
Paulhus, D. L. (1998). Interpersonal and intrapsychic adaptiveness of trait self-enhancement: A mixed blessing? Journal of Personality and Social Psychology, 74(5), 1197–1208. https://doi.org/10.1037/0022-3514.74.5.1197
Paulhus, D. L., & Reid, D. B. (1991). Enhancement and denial in socially desirable responding. Journal of Personality and Social Psychology, 60(2), 307–317. https://doi.org/10.1037/0022-3514.60.2.307
Paulhus, D. L., Harms, P. D., Bruce, M. N., & Lysy, D. C. (2003). The over-claiming technique: Measuring self-enhancement independent of ability. Journal of Personality and Social Psychology, 84(4), 890–904. https://doi.org/10.1037/0022-3514.84.4.890
Pelham, B. W., & Swann, W. B. (1989). From self-conceptions to self-worth: On the sources and structure of global self-esteem. Journal of Personality and Social Psychology, 57(4), 672–680. https://doi.org/10.1037/0022-3514.57.4.672
Randal, C., Pratt, D., & Bucci, S. (2015). Mindfulness and self-esteem: A systematic review. Mindfulness, 6(6), 1366–1378. https://doi.org/10.1007/s12671-015-0407-6
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton University.
Rosenthal, R., & Rosnow, R. L. (1991). Essentials of behavioral research: Methods and data analysis (2nd ed). McGraw Hill.
Sedikides, C. (1993). Assessment, enhancement, and verification determinants of the self-evaluation process. Journal of Personality and Social Psychology, 65(2), 317–338. https://doi.org/10.1037/0022-3514.65.2.317
Sedikides, C., & Gregg, A. P. (2008). Self-enhancement: Food for thought. Perspectives on Psychological Science, 3(2), 102–116. https://doi.org/10.1111/j.1745-6916.2008.00068.x
Shacham, S. (1983). A shortened version of the Profile of Mood States. Journal of Personality Assessment, 47, 305–306. https://doi.org/10.1207/s15327752jpa4703_14
Shapiro, D. H., Jr., Schwartz, C. E., & Astin, J. A. (1996). Controlling ourselves, controlling our world. Psychology’s role in understanding positive and negative consequences of seeking and gaining control. American Psychologist, 51(12), 1213–1230. https://doi.org/10.1037//0003-066x.51.12.1213
Shonin, E., Van Gordon, W., Slade, K., & Griffiths, M. D. (2013). Mindfulness and other Buddhist-derived interventions in correctional settings: A systematic review. Aggression and Violent Behavior, 18(3), 365–372. https://doi.org/10.1016/j.avb.2013.01.002
Spitzer, R. L., Kroenke, K., Williams, J. B., & Lowe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097. https://doi.org/10.1001/archinte.166.10.1092
Taylor, S. E., & Brown, J. D. (1988). Illusion and well-being: A social psychological perspective on mental health. Psychological Bulletin, 103(2), 193–210. https://doi.org/10.1037/0033-2909.103.2.193
Taylor, S. E., Lerner, J. S., Sherman, D. K., Sage, R. M., & McDowell, N. K. (2003). Portrait of the self-enhancer: Well adjusted and well liked or maladjusted and friendless? Journal of Personality and Social Psychology, 84(1), 165–176. https://doi.org/10.1037/0022-3514.84.1.165
Thera, N. (1972). The power of mindfulness. Unity Press.
Thompson, E. R. (2007). Development and validation of an internationally reliable short-form of the Positive and Negative Affect Schedule (PANAS). Journal of Cross-Cultural Psychology, 38(2), 227–241. https://doi.org/10.1177/0022022106297301
Travis, F., & Shear, J. (2010). Focused attention, open monitoring, and automatic self-transcending: Categories to organize meditations from Vedic, Buddhist, and Chinese traditions. Consciousness and Cognition, 19(4), 1110–1118. https://doi.org/10.1016/j.concog.2010.01.007
Vaughan-Johnston, T. I., Jacobson, J. A., Prosserman, A., & Sanders, E. (2021). Mind-body practices and self-enhancement: Direct replications of Gebauer et al.’s (2018) experiments 1 and 2. Psychological Science, 956797621997366. https://doi.org/10.1177/0956797621997366
Vonk, R., & Visser, A. (2021). An exploration of spiritual superiority: The paradox of self-enhancement. European Journal of Social Psychology, 51(1), 1–14. https://doi.org/10.1002/ejsp.2721
Wald, F. D. M., & Mellenbergh, G. J. (1990). De verkorte versie van de Nederlandse vertaling van de Profile of Mood States (POMS) [The shortened version of the Dutch translation of the Profile of Mood States (POMS)]. Nederlands Tijdschrift Voor De Psychologie, 45, 86–90.
Weinberger, D. A., & Davidson, M. N. (1994). Styles of inhibiting emotional expression: Distinguishing repressive coping from impression management. Journal of Personality, 62(4), 587–613. https://doi.org/10.1111/j.1467-6494.1994.tb00310.x
Weinberger, D. A., & Schwartz, G. E. (1990). Distress and restraint as superordinate dimensions of self-reported adjustment: A typological perspective. Journal of Personality, 58(2), 381–417. https://doi.org/10.1111/j.1467-6494.1990.tb00235.x
Wells, A. (1990). Panic disorder in association with relaxation induced anxiety: An attentional training approach to treatment. Behavior Therapy, 21(3), 273–280. https://doi.org/10.1016/S0005-7894(05)80330-2
Author information
Authors and Affiliations
Contributions
IN has initiated the manuscript, conducted Studies 1 and 3, performed analyses of Studies 1 and 3, and largely wrote the manuscript. BO has conducted Study 2, including the analyses, wrote parts of the manuscript, and edited other parts of the manuscript. MB has co-conducted Study 1 and has edited the manuscript.
Corresponding author
Ethics declarations
Ethics Approval
The studies have been approved by the ethics committees of Tilburg University (Studies 1 and 3) and North Dakota State University (Study 2) and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed Consent
All participants of the three studies provided written informed consent before the start of the study.
Use of Artificial Intelligence
The authors declare not to have used artificial intelligence for any purpose.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nyklíček, I., Ostafin, B.D. & Boekhorst, M.G.B.M. Does Mindfulness Decrease or Increase Egoic Functioning? Diverging Evidence From Different Study Designs. Mindfulness 15, 1044–1059 (2024). https://doi.org/10.1007/s12671-024-02351-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-024-02351-4