
Abstract
Objectives
Maladaptive emotional processing of autobiographical memories is a key feature of depression that may persist during depressive remission. The primary objective of the present study was to assess the effects of an online mindfulness-based stress reduction (MBSR) intervention on emotion regulation upon everyday autobiographical memory retrieval in individuals with remitted depression.
Methods
We conducted a pilot randomized controlled trial in which students (76.4% female; mean age 22.26) with remitted depression were allocated to an 8-week online MBSR program (n = 28) or a waitlist-control condition (n = 27). The primary outcome was self-reported employment of five emotion regulation strategies and non-reactivity upon everyday retrieval of involuntary and voluntary autobiographical memories recorded in a memory diary and was measured at baseline and approximately 11 weeks postrandomization. Intention-to-treat (ITT) and per-protocol (PP) analyses were performed.
Results
Participants in the MBSR condition showed increases in non-reactivity irrespective of memory retrieval mode (ITT: d = 1.04, p = .010; PP: d = 1.58, p = .015), and increased use of cognitive reappraisal in response to involuntary memories (ITT: d = 0.41, p = .051; PP: d = − 0.62, p = .032) compared to the waitlist-control condition. Analyses of secondary outcomes showed additional effects for trait mindfulness and trait cognitive reappraisal, as well as depression symptoms and trait thought suppression.
Conclusion
These results provide preliminary evidence for the utility of using an online mindfulness program for improving emotion regulation upon autobiographical memory retrieval during depression remission.
Retrospective Trial Registration
ClinicalTrials.gov, NCT05121116.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Depression is a debilitating psychological disorder with a high risk of recurrence (for a review, see Richards, 2011). It often displays an early age onset (Richards, 2011), with prevalence rates being particularly high among university students (for a review, see Ibrahim et al., 2013). This high prevalence of depression among young individuals is concerning, as early-onset depression is associated with a heightened illness burden, including a greater number of depressive recurrences (Zisook et al., 2007). An important aim in depression research is therefore to understand the psychological factors implicated in depressive vulnerability, and how these factors can be targeted through interventions for young individuals with depression vulnerability.
One key psychological factor that is robustly linked to depression and has been suggested to play an important role in depressive recurrence is altered processing of autobiographical memories (for a review, see Dalgleish & Werner-Seidler, 2014). According to Dalgleish and Werner-Seidler (2014), individuals suffering from depression process their autobiographical memories in at least four distinct but interrelated ways, including biased retrieval of negative memories, impoverished retrieval of positive memories, overgeneral memory retrieval, and altered ways of relating to autobiographical memories. These processes, termed the four mnemonic horsemen of depression, interact in ways that maintain depression and increase the risk of depression recurrence (Dalgleish & Werner-Seidler, 2014). Alterations in the way individuals with depression relate to autobiographical memories have received increasing attention recently. For example, when individuals with depression have intrusive memories of negative past events, they experience higher levels of distress, negative emotions and appraisals, and interference with everyday activities compared to individuals without a depression history (Newby & Moulds, 2010, 2011a). Furthermore, intrusion-related distress, negative emotions and appraisals, and interference with everyday activities predict future levels of depression in individuals not receiving medication or psychological treatment (Newby & Moulds, 2011b, 2011c). However, it is not only intrusive memories of distressing events that lead to negative emotions and appraisals in individuals suffering from depression. Recent studies have demonstrated that individuals with depression experience more frequent negative moods and more intense negative emotions (i.e. sadness, anger, fear) and engage in more maladaptive emotion regulation and evaluations (i.e. memory suppression, brooding, and expressive suppression) in response to autobiographical memories retrieved in everyday life compared to individuals without depression (del Palacio-Gonzalez et al., 2017; Watson et al., 2012). Altered emotional responses are evident in response to positive as well as negative autobiographical memories (e.g. Kim &d Yoon, 2020) , and may persist during remission from depression, especially in response to memories that are retrieved spontaneously or involuntarily and in individuals with low mindfulness skills (Isham et al., 2020; Joormann et al., 2007).
The evidence outlined above suggests alterations in the ways individuals with depression emotionally relate and respond to both negative and positive autobiographical memories, and that some of these maladaptive processes may persist during remission from depression. Given that autobiographical memory retrieval occurs frequently in everyday life (Rasmussen et al., 2015), it constitutes a primary context in which negative emotions and evaluations may be maintained and reinforced in individuals with depression vulnerability. Therefore, emotion dysregulation upon autobiographical memory retrieval constitutes a potential depressogenic vulnerability that should be addressed in interventions aimed at reducing depressive vulnerability and recurrence.
One therapeutic approach that may address this vulnerability is mindfulness. On the one hand, mindfulness-based interventions (MBIs) are an evidence-based method to prevent depressive recurrence (e.g. Teasdale et al., 2000). It has been suggested that a potential mechanism by which MBIs may prevent depression recurrence in individuals with former depression is by promoting more adaptive emotion regulation, such as reducing the use of rumination and thought suppression (e.g. Hepburn et al., 2009; Michalak et al., 2011; Ramel et al., 2004). On the other hand, a key component of MBIs is to change an individual’s stance towards their inner experiences, such as thoughts, emotions, and memories (e.g. Hölzel et al., 2011), thus suggesting that MBIs may be particularly well suited for addressing the biases in emotional processing of autobiographical memories observed in depression. Indeed, emerging evidence suggests that MBIs change certain aspects of autobiographical processing, such as the retrieval of more specific autobiographical memories (as opposed to generalized event descriptions) in both community samples and samples with remitted depression (Heeren et al., 2009; Williams et al., 2000). These promising findings encourage the investigation of whether MBIs may also influence other aspects of autobiographical memory processing in depression, such as their emotional processing, which so far have received little attention.
In line with this possibility, a recent study found that higher levels of trait (i.e. habitual) mindfulness were associated with less memory suppression (i.e. attempts to avoid memories that might trigger unpleasant emotions; Wegner et al., 1987) for both involuntary and voluntary memories, and less brooding (i.e. facet of rumination; Treynor et al., 2003) and greater use of cognitive reappraisal (i.e. attempts to change how one views a situation in order to alter its emotional impact; Gross & Thompson, 2007) only upon retrieving involuntary autobiographical memories, in individuals with remitted depression (Isham et al., 2020). These findings suggest that the ability to be mindful may benefit the emotional processing of autobiographical memories, especially involuntary memories. A potential explanation for the differential relationships between mindfulness and involuntary and voluntary memories is the difference in how involuntary and voluntary memories come to mind. While involuntary memories are experienced as sudden and come to mind with little cognitive control, voluntary memories are retrieved in a more controlled and intentional manner (Berntsen, 2009). Therefore, involuntary memories may provide less opportunity to initiate sufficient cognitive control for implementing effective emotion regulation, compared to voluntary memories. Mindfulness, which involves present-moment-awareness (e.g. Baer et al., 2006) and has been found to enhance cognitive control functions (for a review, see Zainal & Newman, 2020), may enhance awareness and control over the involuntary retrieval process, and thus also the emotional processing of involuntary memories. Therefore, mindfulness may be especially well suited for influencing emotion regulation in response to memories that come to mind involuntarily. However, this does not deny the possibility that mindfulness may influence emotional processing of memories more broadly, including voluntary memories.
The primary aim of the present study was to investigate the effects of an online mindfulness-based stress reduction (MBSR) intervention on emotion regulation strategies employed upon everyday autobiographical memory retrieval in individuals with remitted depression. We hypothesized that online MBSR would decrease memory suppression, rumination, and expressive suppression, and increase cognitive reappraisal and non-reactivity upon memory retrieval, compared to a waitlist-control condition. We also predicted that these effects would be greater for involuntary memories than for voluntary memories. As a secondary study aim, we investigated whether the online MBSR employed in the present study performed similarly to MBIs in previous studies in terms of effects on trait measures of depression, mindfulness, and emotion regulation; and whether the effects of the online MBSR were similar for trait and state measures of emotion regulation.
Method
Participants
Participants were individuals who responded to study advertisements posted online, on campus, and in the local community of St Andrews, Scotland, and provided written informed consent prior to study participation. They were recruited as part of a larger research project involving both currently depressed, remitted depressed, and never-depressed participants, but only the remitted depressed participants were of interest for the present study. Since recruitment was done as part of a larger project, data from some of the participants in the present study have been reported previously (Isham et al., 2020). Specifically, 32 of the participants included in the present study took part in a previously published memory diary study (Isham et al., 2020) in which assessments were equivalent to the baseline phase of the present study. Following these assessments, the participants proceeded directly to the intervention phase of the present study, and finally to the postintervention assessment. Twenty-three additional participants took part in the present study, resulting in a final sample of 55 participants. Adequacy of sample size for intention-to-treat analyses was determined on the basis of previous simulations to estimate sufficient sample sizes for MLM (Maas & Hox, 2005), which suggest that a level two sample size (i.e. participants in the present study) above 50 should produce accurate regression coefficients, variance components, and standard errors.
The inclusion criteria for the present study were English fluency; being in the age range18–65; and being formerly depressed (i.e. at least one past major depressive episode) as assessed by the Mini-International Neuropsychiatric Interview Plus (MINI +) (Sheehan et al., 1998). The exclusion criterion was experiencing a current depressive episode, as assessed by the MINI + (Sheehan et al., 1998). We also assessed the presence of other psychiatric disorders in the sample, including (hypo)manic episode, dysthymia, posttraumatic stress disorder (PTSD), panic disorder, alcohol abuse and dependence, and generalized anxiety disorder (GAD). The two most common current psychiatric comorbidities were GAD (n = 24) and alcohol dependence (n = 13). All clinical interviews were conducted and rated by the first author. Inter-rater reliability for the psychiatric diagnoses was assessed by having an independent rater who assessed ten of the clinical interviews. The inter-rater agreement was 100% for depression diagnostics, and 99.29% for other diagnoses. Disagreements were discussed until reaching a consensus.
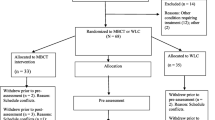
Fifty-five (42 female) participants with clinically remitted depression completed the baseline assessment. These participants constituted the ITT sample. Twenty out of 28 participants in the MBSR condition and 22 out of 27 in the waitlist-control condition took part in both the baseline and the FU assessments. Out of the 20 participants in the MBSR condition who took part in the FU assessment, 14 reported doing at least 4 weeks of the online MBSR program. An additional two participants reported doing at least 4 weeks of the intervention but did not complete any of the primary or secondary outcome measures at FU. Thus, the PP sample consisted of 14 participants in the MBSR condition and 22 participants in the waitlist-control condition. Figure 1 provides a complete overview of the study flow, including a breakdown of the completion of primary and secondary outcome measures, and numbers analysed in ITT and PP analyses.

Study flow diagram
Procedures
We randomized participants with remitted depression in a pilot controlled trial comparing the effects of an 8-week online MBSR program (n = 28) versus a waitlist-control condition (n = 27). Participants were enrolled in the trial on a continuous basis between January 2018 and March 2020, with the baseline assessment being conducted as soon as participants could make an appointment time. The baseline assessment consisted of a diagnostic interview, self-report measures of depression symptoms, trait mindfulness, and trait emotion regulation, and a structured memory diary. Because participant recruitment was done as part of a larger research project, participants also completed additional self-report measures on psychological symptoms and autobiographical memory which are not analysed in the present study.
Participants received an invitation to take part in the follow-up (FU) assessment approximately 8 weeks after allocation to either the MBSR condition or the waitlist-control condition, and took part in the assessment an average of 11.03 (SD = 2.20) weeks after completion of the baseline assessment. The time between baseline and FU assessment was not statistically different for the MBSR (M = 11.45 weeks, SD = 2.08) and the waitlist-control condition (M = 10.67 weeks, SD = 2.31), t(32) = 1.03, mean diff = 0.78, BCa 95% CI: − 0.82, 2.20. The FU assessment consisted of self-report measures of depression symptoms, trait mindfulness, and trait emotion regulation, and a structured memory diary. All participants were compensated for completing the baseline and FU assessments at a rate of approximately £5/hour. The study was granted ethical approval by the local ethics board at the University of St Andrews prior to commencement. The trial was retrospectively registered at ClinicalTrials.gov on October 21st, 2021.
Intervention
Participants in both conditions received information about mental health support organizations and student support options on campus following enrolment in the study. Participants assigned to the active intervention were asked to participate in the MBSR program delivered by Palouse Mindfulness (Palouse Mindfulness, n.d.) immediately after completing the baseline assessment. The MBSR program is freely available online (www.palousemindfulness.com). The program is based on Kabat-Zinn’s (1990) 8-week group program of mindfulness training which was initially developed for chronic pain patients but has also showed efficacy in improving emotion regulation, depression, and other mental health outcomes (e.g. Fjorback et al., 2011; Ramel et al., 2004). The 8-week program consists of the following formal mindfulness practices: introduction to body scan in week 1, guided sitting meditation in week 2, mindful yoga practices in weeks 3 and 4, meditation on difficult emotions in week 5, visualization meditation in week 6, loving-kindness meditation in week 7, and a silent meditation in week 8. Most mindfulness practices are planned to last approximately 30 min and participants are encouraged to engage in a mindfulness practice daily or as often as possible. In weeks 2–8, participants could choose to alternate the practice introduced each week with practices from previous weeks. In addition to the formal mindfulness practices described above, the MBSR program encourages participants to employ mindfulness in their daily lives, for example by bringing present-moment awareness to everyday activities. The website also gives access to educative readings and videos related to the weekly mindfulness practices. Participants in the active intervention had immediate access to all MBSR practices on the website but were asked to complete them sequentially and in the order described above over a period of 8 weeks after the baseline assessment.
Participants in the waitlist-control condition did not receive any intervention during the trial, but were given access to the mindfulness program after the FU assessment, which occurred on average 10.67 weeks after the baseline assessment. At this point, participants in the control condition were provided with the link to the MBSR website together with the study debrief sheet.
Adherence
We assessed adherence to the MBSR intervention via a weekly online self-report questionnaire, where participants in the MBSR condition were asked to report the frequency and length of formal mindfulness practices, and use of educative readings and videos. However, we only obtained reliable data from four participants on this questionnaire. We also asked participants to report on their overall engagement in the MBSR course during the FU assessment, which provided data from an additional ten participants. With the data available, we estimated that participants engaged in an average of 12.53 (SD = 8.09) hours of formal mindfulness practice over the course of the trial. An additional parameter of adherence was participating in at least half of the weekly modules of the intervention (i.e. 4 weeks). Participants who reported having practiced mindfulness in at least four of the weekly self-report questionnaires, or reported having completed at least four weeks of the MBSR program during the FU assessment, were considered as having participated in at least half of the weekly modules. This included a total of 16 participants in the MBSR condition (57.14%).
Measures
Primary Outcomes
The primary outcome was the employment of five emotion regulation strategies and non-reactivity upon retrieval of involuntary vs. voluntary autobiographical memories at FU as compared to baseline. This was assessed with a structured memory diary which has been described in detail in Isham et al. (2020) and can be found as supplemental materials to the present study. In short, participants were asked to record involuntary autobiographical memories immediately upon retrieval over a period of up to 5 days, or until they had recorded seven memories. Participants immediately rated their use of five emotion regulation strategies and a state mindfulness facet upon retrieval (cognitive reappraisal, reflection, brooding, memory suppression, expressive suppression, and non-reactivity; 1 = Not at all to 5 = A great deal) upon memory retrieval. The single items used to assess the five emotion regulation strategies have been used in previous studies (Palacio-Gonzalez et al., 2017; Isham et al., 2020) and were taken from validated questionnaires, including the Emotion Regulation Questionnaire (ERQ; Gross & John, 2003), the White Bear Suppression Inventory (WBSI; Wegner & Zanakos, 1994), and the Ruminative Response (RRS; Nolen-Hoeksema & Morrow, 1991). The item used to assess the mindfulness facet non-reactivity was taken from the Five-Facet Mindfulness Questionnaire to assess non-reactivity (FFMQ; Baer et al., 2006). Employing single items to assess emotion regulation in naturalistic studies has been found to result in reliable and valid assessments (Ong et al., 2006).
For each involuntary memory recorded in the memory diary, participants were instructed to complete additional questions for that memory and answer the same questions in relation to a word-cued (i.e. voluntary) memory when they had time later that day. Furthermore, for each involuntary memory, the participants had to generate a voluntary memory based on a word cue included in their research materials, and answer the same emotion regulation questions in relation to the voluntary memory. FU questions could be completed either on paper or online, as some students had graduated or left campus for holidays and were therefore unable to pick up a paper version of the questionnaires at FU. Participants who had left campus also received a reminder email containing the memory diary instructions and items.
Secondary Outcomes
Self-reported depression symptoms and trait measures of mindfulness and emotion regulation (thought suppression, expressive suppression, cognitive reappraisal, brooding, reflection, and overall rumination) were secondary outcomes.
We used the depression subscale of the Depression, Anxiety, Stress Scales (DASS; Lovibond & Lovibond, 1995) to assess symptoms of depression. This self-report measure consists of 42 items and consists of 3 subscales, depression, anxiety, and stress. Each item is rated on a 4-point rating scale (0 = Did not apply to me at all, 3 = Applied to me very much, or most of the time). In the current study, the baseline internal consistency for the depression subscale was good (Cronbach’s α = 0.94; McDonald’s ω = 0.94).
We measured trait mindfulness with the Five-Facet Mindfulness Questionnaire (FFMQ; Baer et al., 2006). This self-report measure consists of 39 statements to which subjects rate their agreement using a 5-point scale (1 = Never or very rarely true, 5 = Very often or always true). The FFMQ combines five mindfulness facets, including observing, describing, acting with awareness, non-judging of inner experience, and non-reactivity to inner experience. In the present study, the FFMQ exhibited good internal reliability at baseline (Cronbach’s α = 0.90; McDonald’s ω = 0.90).
The Ruminative Response Scale (RRS; Nolen-Hoeksema & Morrow, 1991) was employed to assess dispositional rumination. The total scale consists of 22 statements that describe ruminative responses to depressed mood. This can be divided into subscales of reflection and brooding, composed of five items each (Treynor et al., 2003). The scales use a 4-point rating scale (1 = Almost never, 4 = Almost always). In the current study, the scales exhibited adequate baseline internal consistency for both the full scale (Cronbach’s α = 0.89; McDonald’s ω = 0.90), the reflection subscale (Cronbach’s α = 0.69; McDonald’s ω = 0.68), and the brooding subscale (Cronbach’s α = 0.77; McDonald’s ω = 0.78) for the full scale, reflection subscale, and brooding subscale, respectively).
We employed the Emotion Regulation Questionnaire (ERQ; Gross & John, 2003) to measure dispositional cognitive reappraisal and expressive suppression. The cognitive reappraisal subscale consists of six items and the expressive suppression subscale consists of four items. Both scales use a 7-point rating scale (1 = Strongly disagree, 7 = Strongly agree). In the current study, the scales showed good baseline internal consistency for both cognitive reappraisal (Cronbach’s α = 0.86; McDonald’s ω = 0.86) and expressive suppression (Cronbach’s α = 0.73; McDonald’s ω = 0.76).
The White Bear Suppression Inventory (WBSI; Wegner & Zanakos, 1994) consists of 15 items assessing thought suppression responses. Subjects rate the degree to which they engage in each response, using a 5-point rating scale (1 = Strongly disagree, 5 = Strongly agree). The WBSI exhibited high baseline internal consistency (Cronbach’s α = 0.90; McDonald’s ω = 0.91) in the current study.
Data Analyses
Primary outcomes were analysed employing multilevel modelling (MLM). These analyses were based on intention-to-treat (ITT) using the baseline-observation carried forward method (BOCF) (e.g. Cavanagh et al., 2013; Danilewitz et al., 2016) to deal with missing FU data. The BOCF method follows the assumption that intervention participants who did not complete FU measures did not benefit from the intervention and is therefore a conservative method for dealing with missing data. ITT models held 1365 observations nested within 55 individuals.
Level 1 predictors in the MLM models were Time (baseline vs. FU) and Retrieval (involuntary vs. voluntary). Level 1 coefficients were modelled as randomly varying if their random error terms reached a significance level of 0.10, as recommended by Nezlek and Mroziński (2020). Time was modelled as randomly varying in the models assessing expressive suppression and non-reactivity, while Retrieval was modelled as randomly varying in the model assessing memory suppression. No other level 1 predictors were modelled as randomly varying. Level 2 consisted of the between-subjects predictor Treatment (MBSR vs. waitlist control), as well as 2- and 3-way interactions between predictors. For the primary outcomes, the main interactions of interest were Treatment × Time and Treatment × Time × Retrieval. Given the overall purpose of our analysis and a priori assumptions about the interactions of predictor variables, all predictor variables and interactions were entered into the multilevel models simultaneously (Anderson, 2012). We selected the autoregressive covariance structure (AR1) for the repeated measure (observations nested within participants), the unrestricted model covariance structure (UN) for parameters with randomly varying slopes, and the variance components (VC) covariance structure for remaining parameters. All models included random intercepts to account for variability in baseline levels of the outcome measures (Gallop & Tasca, 2009). In all models, we employed restricted maximum likelihood estimation (REML), which provides more accurate estimates and tests of fixed effects compared to maximum likelihood estimation (ML) (Nezlek and Mroziński, 2020). Effect sizes are reported as d = 2*√F/ddf.
Secondary outcomes were analysed employing repeated measures ANOVAs. These analyses were based on ITT using the BOCF method to deal with missing FU data. The between-subjects factor was treatment (MBSR vs. waitlist control) and the within-subjects factor was Time (baseline vs. FU).
Following analyses of primary and secondary outcomes based on ITT, we conducted per-protocol (PP) analyses in which we only included participants who completed both baseline and FU measures, and who reported completing at least 4 weeks of the MBSR program. The PP MLM models held 838 observations nested within 33 individuals. All analyses were conducted in SPSS Version 26 and 28. The model selections for the PP analyses were the same as for the ITT analyses, with the exception of the model assessing memory suppression, in which Retrieval was no longer modelled as randomly varying.
Results
Baseline Data
Baseline characteristics were not statistically different between the two conditions, with the exception of differing proportions of undergraduates and postgraduates, and a higher mean age in the waitlist-control condition (Table 1).
Memory Diary Completion
Participants who completed the memory diary recorded an average of 6.35 (SD = 1.35) involuntary memories and 6.29 (SD = 1.34) voluntary memories at baseline, and 6.13 (SD = 1.56) involuntary memories and 6.11 (SD = 1.64) voluntary memories at FU. The number of recorded memories was not significantly different for the MBSR and waitlist-control condition, neither at baseline nor at FU (see Table B.1 in the supplemental materials). Participants recorded the memories in their diaries over a mean period of 5.31 (SD = 2.34) days at baseline and 4.29 (SD = 1.78) days at FU. The number of days spent recording memories in the diary was not significantly different for the intervention conditions, neither at baseline nor at FU (see Table B.1 in the supplemental materials).
Intention-to-Treat Analyses: Primary Outcome
ITT means and standard deviations for the primary outcomes in the active intervention condition and control condition are reported in Table 2 and MLM results for the Time × Condition and Time × Condition × Retrieval interactions are reported in Table 3. A complete overview of the MLM unconditional and conditional models can be found in Table B.2 in the supplemental materials. In unconditional models, the intraclass correlations (ICC) were 0.227, 0.238, 0.173, 0.331, 0.188, and 0.284 for brooding, reflection, memory suppression, expressive suppression, cognitive reappraisal, and non-reactivity, respectively. These ICCs indicate that 66.9–82.7% of the variance in the primary outcomes was at the within-subjects level, while 17.3–33.1% of the variance was at the between-subjects level.
In ITT analyses, there was a marginally significant Time × Condition effect (p = 0.053) for non-reactivity (Table 3). Follow-up simple effect analyses of this interaction showed that there was a significant increase in self-reported non-reactivity from baseline to FU in the MBSR condition (b = 0.47, t(28.18) = 2.77, p = 0.010, d = 1.04) but not in the waitlist-control condition (b = 0.13, t(28.27) = 0.80, p = 0.433, d = 0.30). There was also a significant Time × Condition effect for cognitive reappraisal, which was further explained by a significant Time × Condition × Retrieval effect (Table 3). Follow-up simple effects analyses of the three-way interaction showed that there was a marginally significant increase in cognitive reappraisal from baseline to FU upon involuntary (b = 0.21, t(91.81) = 1.98, p = 0.051, d = 0.41) but not voluntary memory retrieval (b = − 0.03, t(123.15) = − 0.40, p = 0.689, d = 0.07) in the MBSR condition. Participants in the waitlist-control condition showed no significant changes in cognitive reappraisal from baseline to FU, neither for involuntary (b = − 0.06, t(72.00) = − 0.49, p = 0.623, d = 0.24) nor for voluntary memories (b = 0.08, t(91.30) = 0.83, p = 0.411, d = 0.17). There were no significant changes from baseline to FU for any of the remaining emotion regulation strategies.
Intention-to-Treat Analyses: Secondary Outcomes
Means, standard deviations, and ANOVAs for the secondary outcomes are reported in Table 4. In ITT analyses, there was a significant Time × Condition effect for trait mindfulness. Follow-up analyses showed that there was a significant increase in trait mindfulness from baseline to FU in the MBSR condition, t(26) = 3.06, mean diff = 11.81, BCa 95% CI: 5.04, 18.74, but not in the waitlist-control condition, t(26) = 1.37, mean diff = 2.52, BCa 95% CI: − 0.96, 6.01). There was also a significant Time × Condition effect for trait cognitive reappraisal. Follow-up analyses showed that there was a significant decrease in cognitive reappraisal from baseline to FU in the waitlist-control condition, t(26) = − 1.93, mean diff = − 2.26, BCa 95% CI: − 4.65, − 0.02, but no change in the MBSR condition, t(26) = 1.28, mean diff = 1.56, BCa 95% CI: − 0.67,3.78. There were no other significant Time × Condition interactions.
Per-protocol Analyses: Primary Outcome
PP means and standard deviations for the primary outcome in the active intervention condition and control condition are reported in Table 5. PP analyses replicated the ITT intervention effects on memory cognitive reappraisal and non-reactivity, while the results for brooding, reflection, memory suppression, and expressive suppression remained non-significant (see Table B.3 in the supplemental materials). Follow-up simple effect analyses of interactions showed that there was a significant increase in self-reported non-reactivity from baseline to FU in the MBSR condition (b = 0.78, t(12.67) = 2.81, p = 0.015, d = 1.58) but not in the waitlist-control condition (b = 0.19, t(20.07) = 0.87, p = 0.393, d = 0.39). There was also a significant increase in cognitive reappraisal from baseline to FU upon involuntary (b = 0.34, t(50.46) = 2.21, p = 0.032, d = 0.62) but not voluntary memory retrieval (b = − 0.08, t(49.80) = − 0.55, p = 0.585, d = 0.16) in the MBSR condition. Participants in the waitlist-control condition showed no significant changes in cognitive reappraisal from baseline to FU, neither for involuntary (b = − 0.10, t(41.72) = − 0.71, p = 0.482, d = 0.22) nor for voluntary memories (b = 0.11, t(58.56) = 0.88, p = 0.384, d = 0.23). There were no significant changes from baseline to FU for any of the remaining emotion regulation strategies.
Per-protocol Analyses: Secondary Outcome
PP means and standard deviations for the secondary outcomes in the intervention condition and control condition are reported in Table 6. PP analyses replicated the ITT intervention effects on trait mindfulness and trait cognitive reappraisal (see Table B.4 in the supplemental materials). In addition, there were significant Time × Condition effects for depression symptoms, and trait thought suppression (see Table B.4 in the supplemental materials). Follow-up analyses showed that there was a significant increase in trait mindfulness from baseline to FU in the MBSR condition, t(13) = 3.57, mean diff = 20.29, 95% CI: 9.85,31.80, but no change in the waitlist-control condition, t(21) = 1.37, mean diff = 3.09, 95% CI: − 1.97,7.19. For cognitive reappraisal, follow-up analyses suggested that the directions of change from baseline to FU were opposite in the MBSR condition and the waitlist-control condition; however, these changes were not statistically significant, t(13) = 1.10, mean diff = 2.21, 95% CI: − 2.60,6.28; t(21) = − 1.96, mean diff = − 2.77, 95% CI: − 5.68,0.08. For depression symptoms, there was a significant decrease in symptoms from baseline to FU in the MBSR condition, t(13) = − 2.43, mean diff = − 7.79, 95% CI: − 14.90, − 1.94, but no change in the waitlist-control condition, t(21) = 0.65, mean diff = 1.45, 95% CI: − 2.81, 5.24. Finally, there was a significant decrease in thought suppression from baseline to FU in the MBSR condition, t(13) = − 2.57, mean diff = − 9.36, 95% CI: − 16.17, − 2.49, but no change in the waitlist-control condition, t(19) = − 1.05, mean diff = − 1.41, 95% CI: − 4.04,1.27.
Discussion
The primary aim of the present study was to investigate the effects of an online MBSR program on emotion regulation upon involuntary and voluntary autobiographical memory retrieval in a sample of individuals with remitted depression. By doing so, the current work contributes with novel findings on how mindfulness training may influence the retrieval of autobiographical memories during depression remission. A secondary aim of the study was to assess whether the online MBSR employed in the present study performed similarly to MBIs in previous studies in terms of effects on depression symptoms, trait mindfulness, and trait emotion regulation more broadly. We found similar effects of this online MBSR intervention on depression symptoms, trait mindfulness, trait thought suppression, and to some extent cognitive reappraisal, as in previous studies (e.g. Chi et al., 2018; Goldin et al., 2017; Hepburn et al., 2009; Shapiro et al., 2011). These results are encouraging as they suggest that a free, online, and self-directed MBSR intervention can have measurable benefits among individuals in remission from depression.
Beyond aligning with existing findings concerning changes in depression symptoms, trait mindfulness, and trait emotion regulation, our more important findings concerned the increase in the employment of cognitive reappraisal and non-reactivity upon autobiographical memory retrieval in the MBSR intervention compared to the waitlist-control condition. Specifically, participants in the MBSR condition showed increased non-reactivity upon both involuntary and voluntary memory retrieval from baseline to FU compared to the waitlist-control condition. Furthermore, they showed increases in self-reported cognitive reappraisal upon involuntary but not voluntary memory retrieval compared to the waitlist-control condition. These findings shed light on the potential mechanisms of action of MBIs during depression remission that may influence the likelihood of depressive relapse or recurrence.
The increases in non-reactivity upon memory retrieval may suggest increased acceptance of experiencing autobiographical memories and related emotions in individuals with remitted depression, as suggested by previous research in which non-reactivity was associated with acceptance of experiences (Iani et al., 2019). A potential interpretation is that the online MBSR intervention helps individuals become more accepting of their experiences of remembering past events, whether these are retrieved spontaneously or not, by taking a more distanced stance to them and not letting them drive emotional or behavioural reactions. According to Garland et al., (2015a, 2015b), this ability to step back or disidentify from inner experiences leads to a broadening of awareness, which facilitates alternative appraisals of the experiences and may promote positive reappraisal. In line with this, previous research has shown that non-reactivity is associated with a greater habitual use of cognitive reappraisal (Iani et al., 2019), and as such may have supported the observed changes in cognitive reappraisal upon involuntary memory retrieval.
The observed increase in cognitive reappraisal for involuntary memories retrieved in everyday life may be associated with the effective down-regulation of negative emotions (e.g. Gross, 1998; Gross & John, 2003). As such, this increase in cognitive reappraisal may reduce negative emotions in everyday life, which in turn may protect against future depression. The finding that MBSR was associated with increased use of cognitive reappraisal in response to involuntary memories may be clinically relevant given the more frequent mood impact of involuntary relative to voluntary memories in everyday life, and the link between depression vulnerability and depressogenic responses to spontaneous cognitions (e.g. Berntsen & Hall, 2004; Marchetti et al., 2016).
The effect of the mindfulness intervention on cognitive reappraisal was unique for involuntary memories. For the remaining strategies, there were either similar effects for involuntary and voluntary memories or no significant effects. A possible explanation for the unique effect of mindfulness on cognitive reappraisal may be related to the antecedent-focused nature of this emotion regulation strategy (Gross, 1998). More specifically, as an emotion regulation strategy that takes place early in the emotion generation process (Gross, 1998), cognitive reappraisal may benefit from enhanced moment-to-moment awareness of inner experiences fostered by mindfulness practice (Crane et al., 2017). Enhanced moment-to-moment awareness of inner experiences may improve moment-to-moment awareness and control over the involuntary memory retrieval process, and that way provide a greater opportunity to identify, observe, and reappraise the experience of having memories of past events. This increased awareness of inner experiences may have less impact on voluntary memories, which by default are retrieved in with greater awareness than involuntary memories due to their intentional and generative nature. Therefore, detectable changes in cognitive reappraisal for voluntary memories may require either more pronounced increases in moment-to-moment awareness or may rely on greater or additional changes in mindfulness abilities.
The possible requirement of a greater change in mindfulness abilities may also explain the non-significant changes in other emotion regulation strategies. In particular, reductions in dysfunctional emotion regulation strategies such as brooding and memory suppression may rely on improvements in additional aspects of mindfulness, such as non-judging of inner experiences. More pronounced changes in mindfulness likely require a greater amount of mindfulness practice. In line with this, Baer et al. (2012) showed that significant changes in mindfulness did indeed occur at different time points for different mindfulness facets over the course of an 8-week MBSR intervention. The mindfulness facets observing, acting with awareness, and non-reactivity to inner experiences showed significant weekly increases already from week 1 to week 2 and subsequently at multiple points throughout the intervention. On the other hand, the mindfulness facet non-judging did not show a significant weekly change until week 3 and again in week 7, and weekly change in describing only occurred once, towards the end of the intervention. In addition, previous research has also demonstrated that the effects of MBIs on rumination may be dose-dependent (Hawley et al., 2014; Ramel et al., 2004). As such, it may be that the MBSR participants did not engage in sufficient mindfulness practice to show changes in some emotion regulation strategies.
Although we asked participants in the MBSR condition to track their weekly mindfulness practice in the present study, very few participants did so in a reliable manner. Therefore, we were unable to examine the dose-dependent effects of mindfulness practice in the present study. Future studies should consider using software to automatically record intervention adherence and allow for the investigation of dose-dependent effects of MBSR (e.g. Parsons et al., 2020; Wahbeh et al., 2014). They should also include multiple assessment points of state emotion regulation to detect potential fluctuation throughout the intervention period. Future studies could also consider investigating how changes in different mindfulness facets correspond to changes in different emotion regulation strategies.
In terms of our secondary study aim, our findings are consistent with previous studies showing that MBIs may lead to changes in trait mindfulness depression symptoms, thought suppression, and cognitive reappraisal (e.g. Goldin et al., 2017; Hepburn et al., 2009; Ramel et al., 2004; Shapiro et al., 2011). They also highlight the importance of intervention adherence for changes in depression symptoms and thought suppression, which were only found for participants who took part in at least 4 weeks of the MBSR intervention. Furthermore, the fact that participants in the MBSR condition showed changes in trait thought suppression but not memory suppression suggests that changes in trait emotion regulation may not always correspond to changes in state emotion regulation. This highlights the importance of investigating intervention effects on emotion regulation on both the state and trait levels.
Finally, the present study provides preliminary evidence that a free, online, and self-directed MBSR program may have beneficial effects on at-risk individuals in remission from depression. This is important for at least two reasons. First, there is evidence that people may prefer online formats of MBIs over individual or group formats due to reasons such as convenience, privacy, and flexibility (Wahbeh et al., 2014). Therefore, it is important to establish whether online formats show effects that are comparable to individual or group formats. Future studies could directly compare the effects of online and face-to-face MBSR. Second, online MBSR may help people with limited access to psychological health care, such as individuals waiting to get access to public health care or individuals who are unable to attend face-to-face therapy. However, challenges related to adherence to mindfulness practice remain for both online and in-person therapy formats. Therefore, future research and clinical practice could focus on enhancing adherence. Specifically, future studies could explore whether shorter programs may increase adherence while maintaining intervention effects compared to longer interventions such as the one employed in the present study, or whether programs may be adapted to suit particular individuals.
Limitations and Future Research
The present study had limitations that should be considered when interpreting its results. Although MLM sample size estimations by Maas and Hox (2005) indicate that our sample size was adequate for the ITT analyses, the sample size in our PP analyses was smaller than the recommended level two sample size of 50 to produce accurate regression coefficients, variance components, and standard errors. Therefore, our findings should be treated as preliminary and be replicated in a larger sample to ensure their robustness. Another limitation of our sample is the disproportionate percentage of females, which may limit generalizability. In addition, the sample was drawn primarily from a clinically diagnosed student population. This decreases the generalizability of our findings to clinical settings with a more diverse patient base. Nonetheless, this population was important to examine as the incidence of depression is very high in university student populations (Ibrahim et al., 2013). Not excluding participants on the basis of diagnostic comorbidity may be a limitation. On the one hand, comorbidities are very prevalent in depression (e.g. Otte, 2022) and thus our sample may be representative in this regard. On the other hand, not excluding participants with comorbidities means that we cannot rule out the possibility that diagnoses other than depression may have had an impact on our results.
A further limitation of the study concerns the measurement of multiple constructs with the same method (e.g. multiple constructs measured with self-report scales). This may produce spurious effects that are due to the common method used to measure multiple constructs rather than the constructs being measured. For example, when self-report scales are used to measure multiple constructs in the same study, this may produce inflated correlations among the items measuring these constructs due to factors such as response style, social desirability, and priming effects (Podsakoff et al., 2012).
In terms of study design, the use of a waitlist-control design rather than an active control condition raises the possibility that some of the effects observed in the present study may reflect placebo effects, as opposed to true intervention effects. Furthermore, while the present study provides preliminary evidence that online MBSR may enhance emotion regulation in response to autobiographical memories, it did not examine long-term effects. Future studies should replicate our findings in an active control design and include long-term follow-ups to examine whether effects remain over time. Finally, we did not examine whether the mindfulness intervention lead to changes in how individuals with remitted depression evaluated the valence of remembered events, or whether changes in emotion regulation were linked to specific emotions. Such changes may have important implications for the everyday mood of individuals in remission from depression. Future studies could investigate whether MBIs also change the self-reported valence of remembered events, as well as the valence of emotions experienced upon memory retrieval in everyday life.
Data Availability
The raw data underpinning this study cannot be made publicly available due to ethical regulations; however, data and materials will be made available on reasonable request, and in line with data protection regulations through contacting the primary author.
References
Anderson, D. (2012). Hierarchical linear modeling (HLM): An introduction to key concepts within cross-sectional and growth modeling frameworks (Technical Report No. 1308). Behavioral Research and Teaching, University of Oregon. https://files.eric.ed.gov/fulltext/ED545279.pdf
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13(1), 27–45. https://doi.org/10.1177/1073191105283504
Baer, R. A., Carmody, J., & Hunsinger, M. (2012). Weekly change in mindfulness and perceived stress in a mindfulness-based stress reduction program. Journal of Clinical Psychology, 68(7), 755–765. https://doi.org/10.1002/jclp.21865
Berntsen, D. (2009). Involuntary autobiographical memories: An introduction to the unbidden past. Cambridge University Press.
Berntsen, D., & Hall, N. M. (2004). The episodic nature of involuntary autobiographical memories. Memory & Cognition, 32(5), 789–803. https://doi.org/10.3758/BF03195869
Cavanagh, K., Strauss, C., Cicconi, F., Griffiths, N., Wyper, A., & Jones, F. (2013). A randomised controlled trial of a brief online mindfulness-based intervention. Behaviour Research and Therapy, 51(9), 573–578. https://doi.org/10.1016/j.brat.2013.06.003
Chi, X., Bo, A., Liu, T., Zhang, P., & Chi, I. (2018). Effects of mindfulness-based stress reduction on depression in adolescents and young adults: A systematic review and meta-analysis. Frontiers in Psychology, 9, 1034.
Crane, R. S., Brewer, J., Feldman, C., Kabat-Zinn, J., Santorelli, S., Williams, J. M. G., & Kuyken, W. (2017). What defines mindfulness-based programs? The warp and the weft. Psychological Medicine, 47(6), 990–999.
Dalgleish, T., & Werner-Seidler, A. (2014). Disruptions in autobiographical memory processing in depression and the emergence of memory therapeutics. Trends in Cognitive Sciences, 18(11), 596–604. https://doi.org/10.1016/j.tics.2014.06.010
Danilewitz, M., Bradwejn, J., & Koszycki, D. (2016). A pilot feasibility study of a peer-led mindfulness program for medical students. Canadian Medical Education Journal, 7(1), e31.
del Palacio-Gonzalez, I., & Dritschel. (2020). Trait mindfulness and emotion regulation upon autobiographical memory retrieval during depression remission. Mindfulness, 11(12), 2828–2840. https://doi.org/10.1007/s12671-020-01494-4
del Palacio-Gonzalez, A., Berntsen, D., & Watson, L. A. (2017). Emotional intensity and emotion regulation in response to autobiographical memories during dysphoria. Cognitive Therapy and Research, 41(4), 530–542. https://doi.org/10.1007/s10608-017-9841-1
Fjorback, L. O., Arendt, M., Ørnbøl, E., Fink, P., & Walach, H. (2011). Mindfulness-based stress reduction and mindfulness-based cognitive therapy–a systematic review of randomized controlled trials. Acta Psychiatrica Scandinavica, 124(2), 102–119. https://doi.org/10.1111/j.1600-0447.2011.01704.x
Gallop, R., & Tasca, G. A. (2009). Multilevel modeling of longitudinal data for psychotherapy researchers: II The Complexities. Psychotherapy Research, 19(4–5), 438–452. https://doi.org/10.1080/10503300902849475
Garland, E. L., Farb, N. A., Goldin, P. R., & Fredrickson, B. L. (2015a). The mindfulness-to-meaning theory: Extensions, applications, and challenges at the attention–appraisal–emotion interface. Psychological Inquiry, 26(4), 377–387. https://doi.org/10.1080/1047840X.2015.1092493
Garland, E. L., Farb, N. A., Goldin, R. P., & Fredrickson, B. L. (2015b). Mindfulness broadens awareness and builds eudaimonic meaning: A process model of mindful positive emotion regulation. Psychological Inquiry, 26(4), 293–314. https://doi.org/10.1080/1047840X.2015.1064294
Goldin, P. R., Morrison, A. S., Jazaieri, H., Heimberg, R. G., & Gross, J. J. (2017). Trajectories of social anxiety, cognitive reappraisal, and mindfulness during an RCT of CBGT versus MBSR for social anxiety disorder. Behaviour Research and Therapy, 97, 1–13. https://doi.org/10.1016/j.brat.2017.06.001
Gross, J. J. (1998). Antecedent-and response-focused emotion regulation: Divergent consequences for experience, expression, and physiology. Journal of Personality and Social Psychology, 74(1), 224–237. https://doi.org/10.1037/0022-3514.74.1.224
Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348–362. https://doi.org/10.1037/0022-3514.85.2.348
Gross, J. J., & Thompson, R. A. (2007). Emotion regulation: Conceptual foundations. In J. J. Gross (Ed.), Handbook of emotion regulation (pp. 3–24). The Guilford Press.
Hawley, L. L., Schwartz, D., Bieling, P. J., Irving, J., Corcoran, K., Farb, N. A., Anderson, A. K., & Segal, Z. V. (2014). Mindfulness practice, rumination and clinical outcome in mindfulness-based treatment. Cognitive Therapy and Research, 38(1), 1–9. https://doi.org/10.1007/s10608-013-9586-4
Heeren, A., Van Broeck, N., & Philippot, P. (2009). The effects of mindfulness on executive processes and autobiographical memory specificity. Behaviour Research and Therapy, 47(5), 403–409. https://doi.org/10.1016/j.brat.2009.01.017
Hepburn, S. R., Crane, C., Barnhofer, T., Duggan, D. S., Fennell, M. J., & Williams, J. M. G. (2009). Mindfulness-based cognitive therapy may reduce thought suppression in previously suicidal participants: Findings from a preliminary study. British Journal of Clinical Psychology, 48(2), 209–215. https://doi.org/10.1348/014466509X414970
Hölzel, B. K., Lazar, S. W., Gard, T., Schuman-Olivier, Z., Vago, D. R., & Ott, U. (2011). How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspectives on Psychological Science, 6(6), 537–559.
Iani, L., Lauriola, M., Chiesa, A., & Cafaro, V. (2019). Associations between mindfulness and emotion regulation: The key role of describing and nonreactivity. Mindfulness, 10(2), 366–375. https://doi.org/10.1007/s12671-018-0981-5
Ibrahim, A. K., Kelly, S. J., Adams, C. E., & Glazebrook, C. (2013). A systematic review of studies of depression prevalence in university students. Journal of Psychiatric Research, 47(3), 391–400. https://doi.org/10.1016/j.jpsychires.2012.11.015
Joormann, J., Siemer, M., & Gotlib, I. H. (2007). Mood regulation in depression: Differential effects of distraction and recall of happy memories on sad mood. Journal of Abnormal Psychology, 116(3), 484. https://psycnet.apa.org/doi/10.1037/0021-843X.116.3.484
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. Delta.
Kim, D., & Yoon, K. L. (2020). Emotional response to autobiographical memories in depression: Less happiness to positive and more sadness to negative memories. Cognitive Behaviour Therapy, 49(6), 475–485. https://doi.org/10.1080/16506073.2020.1765859
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33(3), 335–343. https://doi.org/10.1016/0005-7967(94)00075-u
Maas, C. J., & Hox, J. J. (2005). Sufficient sample sizes for multilevel modeling. Methodology: European Journal of Research Methods for the Behavioral and Social Sciences, 1(3), 86. https://psycnet.apa.org/doi/10.1027/1614-2241.1.3.86
Marchetti, I., Koster, E. H., Klinger, E., & Alloy, L. B. (2016). Spontaneous thought and vulnerability to mood disorders: The dark side of the wandering mind. Clinical Psychological Science, 4(5), 835–857. https://doi.org/10.1177/2F2167702615622383
Michalak, J., Hölz, A., & Teismann, T. (2011). Rumination as a predictor of relapse in mindfulness-based cognitive therapy for depression. Psychology and Psychotherapy: Theory, Research and Practice, 84(2), 230–236. https://doi.org/10.1348/147608310X520166
Newby, J. M., & Moulds, M. L. (2010). Negative intrusive memories in depression: The role of maladaptive appraisals and safety behaviours. Journal of Affective Disorders, 126(1–2), 147–154. https://doi.org/10.1016/j.jad.2010.03.012
Newby, J. M., & Moulds, M. L. (2011a). Characteristics of intrusive memories in a community sample of depressed, recovered depressed and never-depressed individuals. Behaviour Research and Therapy, 49(4), 234–243. https://doi.org/10.1016/j.brat.2011.01.003
Newby, J. M., & Moulds, M. L. (2011b). Do intrusive memory characteristics predict depression at 6 months? Memory, 19(5), 538–546. https://doi.org/10.1080/09658211.2011.590505
Newby, J. M., & Moulds, M. L. (2011c). Do negative appraisals and avoidance of intrusive memories predict depression at six months? International Journal of Cognitive Therapy, 4(2), 178–186. https://doi.org/10.1521/ijct.2011.4.2.178
Nezlek, J. B., & Mroziński, B. (2020). Applications of multilevel modeling in psychological science: Intensive repeated measures designs. L’annee Psychologique, 120(1), 39–72.
Nolen-Hoeksema, S., & Morrow, J. (1991). A prospective study of depression and posttraumatic stress symptoms after a natural disaster: The 1989 Loma Prieta Earthquake. Journal of Personality and Social Psychology, 61(1), 115–121. https://doi.org/10.1037/0022-3514.61.1.115
Ong, A. D., Bergeman, C. S., Bisconti, T. L., & Wallace, K. A. (2006). Psychological resilience, positive emotions, and successful adaptation to stress in later life. Journal of Personality and Social Psychology, 91(4), 730–749. https://doi.org/10.1037/0022-3514.91.4.730
Otte, C. (2022). Incomplete remission in depression Role of psychiatric and somatic comorbidity. Dialogues in Clinical Neuroscience, 10(4), 453–460. https://doi.org/10.31887/DCNS.2008.10.4/cotte
Parsons, C. E., Madsen, M. A., Jensen, K. L., Kæseler, S., Fjorback, L. O., Piet, J., Roepstorff, A., & Linehan, C. (2020). Smartphone monitoring of participants’ engagement with home practice during mindfulness-based stress reduction: Observational study. JMIR Mental Health, 7(1), e14467.
Podsakoff, P. M., MacKenzie, S. B., & Podsakoff, N. P. (2012). Sources of method bias in social science research and recommendations on how to control it. Annual Review of Psychology, 63, 539–569.
Ramel, W., Goldin, P. R., Carmona, P. E., & McQuaid, J. R. (2004). The effects of mindfulness meditation on cognitive processes and affect in patients with past depression. Cognitive Therapy and Research, 28(4), 433–455. https://doi.org/10.1023/B:COTR.0000045557.15923.96
Rasmussen, A. S., Ramsgaard, S. B., & Berntsen, D. (2015). Frequency and functions of involuntary and voluntary autobiographical memories across the day. Psychology of Consciousness: Theory, Research, and Practice, 2(2), 185–205. https://doi.org/10.1037/cns0000042
Richards, D. (2011). Prevalence and clinical course of depression: A review. Clinical Psychology Review, 31(7), 1117–1125. https://doi.org/10.1016/j.cpr.2011.07.004
Shapiro, S. L., Brown, K. W., Thoresen, C., & Plante, T. G. (2011). The moderation of mindfulness-based stress reduction effects by trait mindfulness: Results from a randomized controlled trial. Journal of Clinical Psychology, 67(3), 267–277. https://doi.org/10.1002/jclp.20761
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., Hergueta, T., Baker, R., & Dunbar, G. C. (1998). The Mini-International Neuropsychiatric Interview (M.I.N.I): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. The Journal of Clinical Psychiatry, 59(20), 22–33. ISBN/ISSN: 0160–6689
Teasdale, J. D., Segal, Z. V., Williams, J. M. G., Ridgeway, V. A., Soulsby, J. M., & Lau, M. A. (2000). Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. Journal of Consulting and Clinical Psychology, 68(4), 615. https://psycnet.apa.org/doi/10.1037/0022-006X.68.4.615
Treynor, W., Gonzalez, R., & Nolen-Hoeksema, S. (2003). Rumination reconsidered: A psychometric analysis. Cognitive Therapy and Research, 27(3), 247–259. https://doi.org/10.1023/A:1023910315561
Wahbeh, H., Svalina, M. N., & Oken, B. S. (2014). Group, one-on-one, or internet? Preferences for mindfulness meditation delivery format and their predictors. Open Medicine Journal, 1, 66–74. https://doi.org/10.2174/2F1874220301401010066
Watson, L. A., Berntsen, D., Kuyken, W., & Watkins, E. R. (2012). The characteristics of involuntary and voluntary autobiographical memories in depressed and never depressed individuals. Consciousness and Cognition, 21(3), 1382–1392. https://doi.org/10.1016/j.concog.2012.06.016
Wegner, D. M., & Zanakos, S. (1994). Chronic thought suppression. Journal of Personality, 62(4), 615–640. https://doi.org/10.1111/j.1467-6494.1994.tb00311.x
Wegner, D. M., Schneider, D. J., Carter, S. R., & White, T. L. (1987). Paradoxical effects of thought suppression. Journal of Personality and Social Psychology, 53(1), 5–13. https://doi.org/10.1037//0022-3514.53.1.5
Williams, J. M. G., Teasdale, J. D., Segal, Z. V., & Soulsby, J. (2000). Mindfulness-based cognitive therapy reduces overgeneral autobiographical memory in formerly depressed patients. Journal of Abnormal Psychology, 109(1), 150–155. https://doi.org/10.1037/0021-843X.109.1.150
Zainal, N. H., & Newman, M. G. (2020). Mindfulness enhances cognitive functioning: A meta-analysis of 100 randomized controlled trials. PsyArXiv. https://doi.org/10.31234/osf.io/vzxw7
Zisook, S., Lesser, I., Stewart, J. W., Wisniewski, S. R., Balasubramani, G. K., Fava, M., Gilmer, W. S., Dresselhaus, T. R., Thase, M. E., Nierenberg, A. A., Trivedi, M. H., & Rush, A. J. (2007). Effect of age at onset on the course of major depressive disorder. American Journal of Psychiatry, 164(10), 1539–1546.
Author information
Authors and Affiliations
Contributions
AEI: designed and executed the study, analysed the data, and wrote the first full draft of the paper. APG: collaborated with the design and writing of the study, and provided feedback on data analyses. BD: collaborated with the design and writing of the study, and provided feedback on data analyses. All authors approved the final version of the manuscript for submission.
Corresponding author
Ethics declarations
Ethics Approval
The local board for research ethics at the University of St Andrews approved the study prior to commencement. Informed consent was obtained from all individual participants.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Isham, A.E., del Palacio-Gonzalez, A. & Dritschel, B. The Effects of an Online Mindfulness Intervention on Emotion Regulation upon Autobiographical Memory Retrieval in Depression Remission: a Pilot Randomized Controlled Trial. Mindfulness 13, 2613–2627 (2022). https://doi.org/10.1007/s12671-022-01983-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-022-01983-8