
Abstract
Background and aim
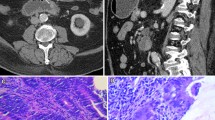
Small bowel follow through (SBFT) and enteroclysis have low sensitivity in picking up lesions in obscure gastrointestinal bleed (OGIB). Computed tomographic enterography (CT-EG), performed with 64-slice multiphase CT system by using large volumes of ingested neutral enteric contrast material, has high spatial and temporal resolution in visualization of the small bowel wall and lumen. The role of 64-slice multiphase CT-EG in the evaluation of OGIB is still evolving, and data on this role are scarce. We evaluated the efficacy of 64-slice multiphase CT-EG using polyethylene glycol (PEG) electrolyte solution as neutral contrast in patients of OGIB.
Methods
CT-EG was performed with 64-slice multiphase CT system using large volume (2,000 mL) of PEG electrolyte solution as oral contrast in patients of OGIB.
Results
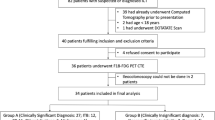
Thirty-five patients (21 men, age 41.4 [13.5] y, range 19–70 year) with OGIB underwent CT-EG; 20 patients had overt OGIB whereas 15 patients had occult OGIB. Among 15 patients with occult OGIB, 10 patients had iron deficiency anemia (IDA) with fecal occult blood test (FOBT) positive and 5 had IDA with FOBT negative. Thirty-two patients (92 %) completed the procedure successfully. The total time taken for the ingestion of 2,000 mL of PEG electrolyte solution was median 64 (range 60–78) minutes. Adequate luminal distension of small bowel was seen in 29 (90.6 %) patients for successful interpretation of radiological images. Fifteen of 32 (46.9 %) patients had positive findings on CT-EG; 12 of them underwent exploratory laparotomy. The surgical findings were in conformity with CT-EG findings in all patients, which included gastrointestinal stromal tumors (GIST; n = 6), carcinoid (1), Meckel’s diverticulum (1), small bowel adenocarcinoma (2) and jejunal vascular malformation (2).
Conclusion
64-slice multiphase CT-EG is a useful investigation in the evaluation of both occult and overt OGIB.




Similar content being viewed by others
References
Zuckerman GR, Prakash C, Askin MP, Lewis BS. AGA technical review on the evaluation and management of occult and obscure gastrointestinal bleeding. Gastroenterology. 2000;118:201–21.
Lin S, Rockey DC. Obscure gastrointestinal bleeding. Gastroenterol Clin North Am. 2005;34:679–98.
Mata A, Bordas JM, Feu F, et al. Wireless capsule endoscopy in patients with obscure gastrointestinal bleeding: a comparative study with push enteroscopy. Aliment Pharmacol Ther. 2004;20:189–94.
Ge ZZ, Hu YB, Xiao SD. Capsule endoscopy and push enteroscopy in the diagnosis of obscure gastrointestinal bleeding. Chin Med J (Engl). 2004;117:1045–9.
Scapa E, Jacob H, Lewkowicz S, et al. Initial experience of wireless-capsule endoscopy for evaluating occult gastrointestinal bleeding and suspected small bowel pathology. Am J Gastroenterol. 2002;97:2776–9.
Lo S, Ross A, Leighton J, et al. Double balloon enteroscopy: an initial multicenter U.S experience. Am J Gastroenterol. 2005;100:A-243.
Rockey DC, Cello JP. Evaluation of the gastrointestinal tract in patients with iron deficiency anemia. N Engl J Med. 1993;329:1691–5.
Rabe FE, Becker GJ, Besozzi MJ, Miller RE. Efficacy study of the small bowel examination. Radiology. 1981;140:47–50.
Willis JR, Chokshi HR, Zuckerman GR, Aliperti G. Enteroscopy-enteroclysis: experience with a combined endoscopic radiographic technique. Gastrointest Endosc. 1997;45:163–7.
Scott R, Paulsen BS, James E, et al. CT enterography as a diagnostic tool in evaluating small bowel disorders: review of clinical experience with over 700 cases. Radiographics. 2006;26:641–57.
Tochetto S, Yaghmai V. CT enterography: concept, technique and interpretation. Radiol Clin N Am. 2009;47:117–32.
Arslan H, Etlik O, Kayan M, Harman M, Tuncer Y, Temizöz O. Per oral CT enterography with lactulose solution: preliminary observations. AJR. 2005;185:1173–9.
Huprich JE, Fletcher JG, Alexander JA, Fidler JL, Burton SS, McCullough CH. Obscure gastrointestinal bleeding: evaluation with 64-section multiphase CT enterography-initial experience. Radiology. 2008;246:562–71.
Megibow AJ, Babb JS, Hecht EM, et al. Evaluation of bowel distension and bowel wall appearance by using neutral oral contrast agent for multi detector row CT. Radiology. 2006;238:87–95.
Young BM, Fletecher JG, Booya F, et al. Head to head comparison of oral contrast agents for cross sectional enterography: small bowel distension, timing, and side effects. J Comput Assist Tomogr. 2008;32:32–8.
Gore RM, Balthazar EJ, Ghahremani GG, Miller FH. CT features of ulcerative colitis and Crohn’s disease. AJR. 1996;167:3–15.
Booya F, Fletcher JG, Johnson CD, et al. CT enterography: detection of active Crohn’s disease during optimal bowel wall enhancement (abstr.). In: Radiological Society of North America Scientific assembly and annual meeting program. Oak Brook, III: Radiological Society of North America; 2004. 611.
Mazzeo S, Caramella D, Battolla L, et al. Crohn’s disease of the small bowel: spiral CT evaluation after oral hyper hydration with isotonic solution. J Comput Assist Tomogr. 2001;25:612–6.
Wold PB, Fletcher JG, Johnson CD, Sandborn WJ. Assessment of small bowel Crohn’s disease: noninvasive per oral CT enterography compared with other imaging methods and endoscopy-feasibility study. Radiology. 2003;229:275–81.
Foutch PG. Angiodysplasia of gastrointestinal tract. Am J Gastroenterol. 1993;88:807–18.
Lewis BS, Kornbluth A, Waye JD. Small bowel tumors: yield of enteroscopy. Gut. 1991;32:763–5.
Pillenl F, Penigaud M, Milot L, Saurin JC, Chayvialle JA, Valette PJ. Possible small bowel neoplasm: contrast enhanced and water enhanced multidetector CT enteroclysis. Radiology. 2006;241:796–801.
Lewis BS. Small intestinal bleeding. Gastroenterol Clin North Am. 2000;29:67–95.
Horton KM, Juluru K, Montogomery E, Fishman EK. Computed tomography imaging of gastro intestinal stromal tumors with pathology correction. J Comput Assist Tomogr. 2004;28:811–7.
Mag Linte DD. Capsule imaging and the role of radiology in the investigation of diseases of the small bowel. Radiology. 2005;236:763–7.
Elsayes KM, Menias CO, Harvin HJ, Francis IR. Imaging manifestations of Meckel’s diverticulum. AJR. 2007;189:81–8.
Pennazio M, Santucci R, Rondonotti E, et al. Outcome of patients with obscure gastrointestinal bleeding after capsule endoscopy: report of 100 consecutive cases. Gastroenterology. 2004;126:643–53.
Triezter SI, Leighton JA, Leontiadis GI, et al. A meta analysis of the yield of capsule endoscopy compared to other diagnostic modalities in patients of OGIB. Am J Gastroenterol. 2005;100:2407–18.
Estevez I, Gonzale CB, Vazquez z-IL, Alonso PA, Vázquez-Millán Mde L, Pardeiro R. Incidence of tumor pathology according to study using capsule endosopy for patients with obscure gastro-intestinal bleeding. Surg Endosc. 2007;21:1776–80.
Lewis BS, Eisen GM, Friedman S. Pooled analyses to evaluate results of capsule endoscopy trials. Endoscopy. 2005;37:960–5.
Andrew R, Shahab M, Jeffrey T, et al. Double balloon enteroscopy detects small bowel mass lesions missed by capsule endoscopy. Dig Dis Sci. 2008;53:2140–3.
Jaffee TA, Moria Gaca A, Deloney S, et al. Radiation dose from small bowel follow through and abdominopelvic MDCT in Crohn’s disease. AJR. 2007;189:1015–22.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sodhi, J.S., Zargar, S.A., Rashid, W. et al. 64-section multiphase CT enterography as a diagnostic tool in the evaluation of obscure gastrointestinal bleeding. Indian J Gastroenterol 31, 61–68 (2012). https://doi.org/10.1007/s12664-012-0176-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12664-012-0176-2