
Abstract
Empirical evidence shows that Internet Gaming Disorder (IGD) with poor psychological well-being increases. IGD has become an emerging issue of significant public health concern and the World Health Organization has recently recognized it as a mental health condition. This study examined the efficacy of the Acceptance and Cognitive Restructuring Intervention Program (ACRIP) in reducing the symptoms of IGD and improving the psychological well-being of adolescent gamers from select Asian cultures after proving it effective in a prior study in the Indian setting. The development of the ACRIP employed a sequential exploratory research design and randomized controlled trial on thirty participants. Internet Gaming Disorder (IGDS9-SF) and Ryff’s Psychological well-being (PWB) scales were used to measure the severity of the gaming disorder and the state of psychological health of the experimental and control groups. Power analysis ascertained the study with a power of 0.90, indicating a strong probability of obtaining a statistically significant effect. Statistical analyses using paired t-test and MANOVA on post-test mean scores on IGD and PWB of the experimental group showed a significant difference which suggested that the ACRIP is efficacious and culture-free.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Since the proliferation of the internet in the 2000s and the prevalence of internet gaming among the adolescents, empirical evidence associating Internet Gaming Disorder (IGD) with poor psychological well-being has increased in number (Gentile et al., 2010; Gonzales-Bueso et al., 2018; Kuss & Griffiths, 2012a; Moudiab & Spada, 2019; Subramaniam et al., 2016). IGD has brought about other negative consequences such as impaired daily functioning (Hawi et al., 2018) and self-harming behaviors (Kuss & Griffiths, 2012b). The World Health Organization (WHO) incorporated "gaming disease," IGD official nomenclature, in the 11th International Classification of Diseases (ICD-11) in mid-2018 since the devastating implications of IGD continue to affect teenagers in an increasing number of nations. Medical practitioners and researchers utilize the ICD to diagnose and categorize illnesses (WHO, 2018). The WHO describes the symptoms of gaming disorder (Table 1), which can be continuous, episodic, or recurrent and must have occurred during the last 12 months to be considered significant for diagnosis. If the symptoms are severe and the diagnostic criteria are met, a shorter period may be considered.
The primary aspect of IGD, according to the American Psychiatric Association (APA), is long hours of gaming (8–10 h or more per day or 30 h per week), which leads to a decrease and abandonment of regular tasks. The preliminary diagnostic criteria leading to severe impairment or clinical distress (APA, 2013) used in the assessment of IGD are listed in Table 1 of the Diagnostic and Statistical Manual 5th edition, which was updated in 2013. (DSM-5). The IGD scale (IGDS9-SF) developed by Pontes and Griffiths (2015) used these criteria to assess the severity of gaming disorder.
To add to the harmful consequences of IGD, it has been linked to self-harming behaviors due to an obsessive fascination with gaming (Kuss & Griffiths, 2012b). Its psychological effects include compromising sleep, other leisure activities, socializing and relationships, and risking school and work performance (Hawi et al. 2018; Stavropoulos et al., 2017). It also causes health issues such as eye strain, carpal tunnel syndrome, back strain, and repetitive stress injury in some situations. IGD may require professional therapy due to the vast spectrum of actual and potentially adverse effects that allow its conduct to be recognized as abnormal under the APA's defined clinical standard (APA, 2000). (Kuss et al., 2017).
Children have been disproportionately affected by the COVID-19 pandemic because they have been forced to stay at home, away from their school, friends, and all of the activities they loved before the epidemic. As a result, spending long periods in front of the screens of tablets, smartphones, and computers playing electronic games was their only source of entertainment while at home, and there is no doubt that the sudden shift in children's lifestyle during the COVID-19 pandemic had severe consequences and risks threatening their stability at all levels (Walaa Elsayed, 2021).
Based on the existing literature, an effective intervention program to address IGD is yet to be produced. The review of treatments in 36 studies using Cognitive Therapy appears to lack cognition-based measures (King & Delfabbro, 2014). Due to flaws in diagnosis and post-treatment/follow-up procedures, there is no significant evidence of beneficial intervention, either short or long term. Furthermore, there is very little research on the effectiveness of various psychological therapies for adolescents (King et al., 2013; King & Delfabbro, 2014). Hence, to fill the gaps in the ongoing research for an efficacious intervention program to address IGD, the “Acceptance and Cognitive Restructuring Intervention Program” (ACRIP) was developed as an online intervention with the main objectives of reducing the symptoms of IGD and improving the psychological well-being of adolescent gamers of different Asian cultures during this pandemic (Fig. 1).

Flow chart of the Research process
Process of Program Development
The study procedure for developing the ACRIP as an intervention program used a mixed-method approach, namely a sequential exploratory design, and was thus divided into two phases: program creation and program validation. Selection of a problem, review of literature, exploration of relevant theories and conceptual frameworks, determination of research questions and hypotheses, data collection (assessment of methods including research instruments and procedures), analyses and drawing of conclusions, and developing the program draft, pilot study, expert validation, and finalizing the ACRIP modules before experimental validation were all part of the program development.
A topical, relevant, and important issue concerning public health was chosen. With IGD becoming more prevalent among adolescents when smartphone technology is rapidly evolving, internet game features are becoming more sophisticated, and high-speed internet access is becoming more accessible, particularly in Asia, there is a need to investigate and develop an intervention program that will effectively address IGD. Theoretical and conceptual frameworks were scrutinized and assessed. In structuring ACRIP, the concepts of two cognitive theoretical models have been integrated: the cognitive Behavioral model of Problematic Internet Use (PIU) and the Mindfulness theory.
According to the Cognitive Behavioral model of PIU, pathologic internet use is caused by "problematic cognitions linked with behaviors that either enhance or maintain the maladaptive response" (Davis, 2001, p.191). It was argued that dysfunctional self- and worldviews are sufficient proximal causes of IGD symptoms. A ruminative cognitive style is characterized by intense thought about oneself. Ruminating entails frequently thinking about difficulties related to one's internet use, which keeps the IGD cycle going rather than focusing on regular life activities. Self-doubt, negative self-appraisals, and low self-efficacy are examples of maladaptive self-perceptions.
"I am useless offline, but someone online," and "I am a failure when I am offline" are examples of distorted self-perceptions (Davis, 2001). In general, someone with low self-image uses the internet to get feedback and pleasant social contact. "The internet is the only place I am appreciated," "Nobody loves me offline," "People treat me nothing offline," and "The internet is my sole buddy," say people with cognitive biases about the world (Davis, 2001). These cognitive biases increase a person's reliance on internet gaming. As a result, whenever these cognitive distortions are activated in response to a stimulus connected with an internet game, IGD results (Davis, 2001). The essential structure of the mindfulness hypothesis, according to Langer (2000), is that mindlessness may be addressed with suitable interventions. Mindfulness can incline a person “to think and behave mindfully,” promoting sensitivity to the environment and supporting clearer thoughts and behaviors.
Data Gathering
Using the purposive sample method, 456 participants were picked from secondary schools in India. Adolescents were chosen at random and had to meet the following criteria to be included: (a) they had to be boys or girls, (b) between the ages of 13 and 18, (c) live with their biological parents or guardians, (d) actively play any of the online games that were available, (e) have five out of nine (9) IGD symptoms that have persisted for the past year, and (f) be able to understand English. With an age range of 13 to 18 years, there were more boys (n = 313, 69%) than females (n = 143, 31%) among the 456 adolescents tested (M,14.44 years; SD, 1.366). There were more adolescents captured in the 16–18 age range (n = 248, 54%) than in the13–15 age bracket (n = 208, 46%). The total hours spent gaming per week of participants showed 80% were playing more than30 h. Broken down, 20–29 h (n = 90, 20%); 30–35 h (n = 191,42%); 36–40 h (n = 103, 23%); and more than 40 h (n = 72,15%) (Kochuchakkalackal & Reyes, 2019). Ethical standards in gaining informed permission from the participants and license no. Before the study, MMERC 2018–11 from the Manila Medical Ethics Review Committee was followed. The pilot study was conducted to see the efficacy of the intervention program ACRIP. Wilcoxon signed-rank test evaluated the pre-test, and post-test scores of ten randomly selected adolescents from the 456-research pool for statistical analysis. Using the IGD and PWB measures, there was a significant difference in the adolescents' pre-test and post-test scores (IGD: Z = − 2.809, p = 0.005; PWB: Z = − 2.803, p = 0.005). The pilot study results revealed that the intervention program's modules are dependable, practicable, and effective. The ACRIP modules were content validated by 11 mental health specialists who were not part of the focus group discussions, using an adapted version of a standardized evaluation tool created and utilized by the US Agency for International Development (USAID). The inter-rater reliability coefficient was.78, indicating high consistency, dependability, and practicality.
An experimental study involving 40 teenagers who matched the inclusion requirements and were randomly selected from the remaining research pool was done to carry out the program validation (phase 2) of ACRIP. The experimental and control groups were assigned to twenty volunteers randomly. Surprisingly, mean post-test scores for the experimental group revealed a significant drop in IGD level at 17.25 (SD=79) and an increase in PWB level at 406.50. (SD=19.22). The post-test mean scores on IGD (SD=3.97) and PWB (122.90) for the control group were not significantly different (SD=48.42). The difference in the experimental group's pre-test and post-test mean scores in terms of IGD and PWB was shown using a paired t-test. PWB Mean score 126.10 (SD=18.96), post mean score is 406.50 (SD=19.22); p = 0.001. Mean 38.50 (SD=.40), Mean 17.25 (SD= .79); The MANOVA test revealed a statistically significant difference in the mean scores of the experimental group during the post-test (F (7, 32) = 3626.206, p = 0.001), indicating that the ACRIP relieved the teenagers' IGD symptoms and improved their psychological well-being. Cohen's d test revealed a significant effect on the ACRIP's efficacy (Cohen's d value IGD 7.27; PWB 7.23). In all phases of this research, the researcher obtained informed consent from the participants as well as from the parents/guardians of the participants.
Given the preceding empirical evidence and results of the previous research, the goal of this study was to test the following hypotheses: (a) IGD can lead to poor psychological well-being; (b) negative cognition can influence psychological well-being, and (c) the ACRIP intervention program is effective and culture-free in reducing the symptoms of internet gaming disorder and improving the psychological well-being of Asian adolescents.
Methods
Participants
A mixed-method, specifically sequential exploratory research design, was used in this study. thirty adolescent gamers who volunteered for this program were randomly chosen. Participants were studying medicine in Philippine colleges and nationalities of different Asian countries such as the Philippines, Nepal, Maldives, China, Taiwan, Vietnam, and Japan who met the following inclusion criteria: (1) adolescent males and females aged 16 to 19 years old, (2) engages actively in playing any of the available internet games, (3) have a high score in the IGD and low score in PWB scales, (4) plays more than 30 h per week, and (5) have at least five of nine symptoms of IGD in the last 12 months. Fifteen adolescents were randomly assigned to each experimental and control group to facilitate the study. The participants’ weekly gaming profiles showed 60% were playing at least 40 h, and 40% played 31–39 h.
A license to experiment in the Philippines was obtained from the Medical Center Manila Ethics Review Committee under MMERC 2018–11. Informed consent was obtained from the participants and their parents/legal guardians. They were assured of the confidentiality of information before being requested to fill out the questionnaires necessary to experiment and test in person.
Measures
Personal Data Sheet/Demographic Information Form (DIF)
The respondents' socio-demographic and gaming profiles were obtained using a researcher-created personal data sheet/demographic information form, which included age, gender, number of hours of internet gaming per week, length of gaming per session, frequently played game title and genre, years of experience in internet gaming, and family relations, among other things. This questionnaire also included an informed consent section.
Internet Gaming Disorder (IGD) Scale
The IGDS9-SF (Pontes & Griffiths, 2015) examined gaming behaviors over 12 months to determine the severity and negative impacts of IGD. The scale's nine items represented the nine IGD criteria established by DSM-5. They were rated on a 5-point Likert scale from 1 (never) to 5 (always) (very often). The scale exhibited excellent reliability, with a Cronbach's internal consistency coefficient of .96, which is comparable to other research coefficients (Fuster et al., 2016; Pontes & Griffiths, 2015, 2016). The overall score was calculated by summing all of the responses, ranging from 9 to 45 points, with higher scores indicating a higher degree of IGD. Gamers were distinguished from non-gamers as having satisfied at least five of the nine criteria. Each was answered as ‘5: Very Often’, which translated as an endorsement of the criterion.
Ryff’s Psychological Well-being (PWB) Scale
Ryff's long-form psychological well-being measure included 84 questions about how people view themselves and their lives. This self-report scale was created to measure an individual's happiness across six dimensions: autonomy, environmental mastery, personal growth, positive interpersonal relationships, life purpose, and self-acceptance. A 6-point Likert scale signifies responses: 1-strongly disagree, 2-moderately disagree, 3-slightly disagree, 4-slightly agree, 5-moderately agree, and 6-strongly agree. Before calculating the final score, answers to negatively scored questions were inverted so that high scores indicated high self-ratings and higher scores showed better well-being. According to Ryff and Keyes (1995), the reliability coefficients for each dimension are autonomy (0.83), environmental mastery (0.86), personal growth (0.85), positive relationships with others (0.88), and life purpose (0.88) and self-acceptance (α = 0.91).
Procedures
Prior to the experiment, the researcher performed an information drive at chosen medical schools in the Philippines regarding IGD and the importance of an intervention program. 100 medical students from different nationalities studying in Manila, Philippines were chosen who met the inclusion criteria and were evaluated using the purposive sampling technique. The research circumstances and demographic profiles of the youths were thoroughly studied to ensure participant homogeneity. Interviews and focus group discussions were performed to obtain helpful information. Participants were given an overview of the proceedings before the program began, and trained mental health specialists led the program. The experimental group completed all ACRIP courses in eight weeks, working on two three-hour modules per week. No one expressed a wish to withdraw from the program or leave early. The control group did not receive the intervention program during the experimental study. The IGD and PWB scales were used to assess both groups following the session.
The eight modules developed for the ACRIP, were summarized as AFFIRMED, and the objective of each module was briefly described as follows:
ACRIP Modules and Objectives
Module 1 Introductory Session: Accustomizing with Each Other– Present ACRIP and IGNITE Rapport (PAIR)
Introduce ACRIP to participants; build rapport with and among participants; promote enthusiasm and vigor among participants so that they can fully participate in the therapeutic process; educate participants about IGD and their potential to live a quality life, as well as the benefits of practicing mindfulness on a regular basis to improve their psychological well-being.
Module 2 Freeing Oneself from Dysfunctional Thoughts—Drop Resentments, Anger, Ill-feeling, and Negativity (DRAIN)
Identify dysfunctional thought patterns in yourself; educate participants about how thoughts affect mood; confront automatic negative ideas; minimize self-distorted thinking; enhance self-confidence; establish a positive self-concept, and consistently stick to a clear plan of action.
Module 3 Forging Oneself to Create Positive Vibes–Divert into Realistic and Optimistic Patterns (DROP)
To assist participants in recognizing negative thoughts and emotions and ventilating them from consciousness; accepting distorted thinking through practical reconstructive activities; increasing their motivation to be more active and dynamic in daily life; improving their self-esteem and self-efficacy, and instructing them on various strategies for creating positive vibes.
Module 4 Igniting and Re-Building Friendships and Relationships–Communicate, Reconnect, Encourage, Animate, Talk and Engage (CREATE)
To familiarize and educate participants on the various aspects of effective communication; identify positive mutual feelings between self and others; comprehend various problem-solving techniques; reconnect with lost relationships; encourage family and friends to provide more support to the participants, and re-animate self-talk.
Module 5 Re-Kindling Self-Love, Self-Respect, and Approval–Approval Care, and Concern to Enhance Positive Thinking (ACCEPT)
Encourage participants to have a better mental picture of themselves by encouraging them to accept their good and bad qualities, notice and acknowledge their positive aspects, and help them understand that a person's level of self-acceptance determines their well-being and affects all aspects of their life.
Module 6 Magnifying Self-Worth and Independence–Show Toughness, Autonomy, and Nobility in Decision Making (STAND)
To assist participants in developing a positive self-image, enhancing their self-worth, teaching them how to make decisions without relying on others, and assessing their standards. Consider their particular requirements.
Module 7 Enabling Control of Oneself Over the External World–Control Over Personality and the Environment (COPE)
To enable participants to identify positive coping skills and specific activities that improve environmental mastery; be aware of surrounding opportunities and develop a sense of control over the external world; teach participants to manage their body sensations and everyday affairs and improve surrounding context.
Module 8 Developing a Friendly Atmosphere Where Creativity is Enhanced—CHANGE (Cloistered in Hope and Acceptance, Nurtured and Goal-Enriched)
To assist participants to feel better about themselves, accepted and loved by their families and friends; to develop their creativity as a foundation for their future living; to inspire them to take the initiative to work and embrace future responsibilities, and to prepare them for program termination.
Results
After completing the Online ACRIP, the participants in the experimental group showed a significant shift in their behavior, as evidenced by their post-test ratings.
Table 1 shows that the mean score of participants in IGD was high at 37.80 (SD=4.71) and low at 122.44 in the pre-test (SD=20.57). Following the post-test, the mean score on the IGD measure was 18.47 (SD=1.96), indicating a decrease in IGD symptoms, but the mean score on the PWB measure was 405.81 (SD=12.57), showing an increase in their psychological well-being. The significant difference in mean scores demonstrated the ACRIP's effectiveness as an intervention program. After administering ACRIP, statistical analysis using paired t-tests revealed a significant difference in the experimental group's pre-test and post-test scores, resulting in reduced IGD symptoms and improved psychological well-being among adolescents of various cultural backgrounds (IGD t = 15.98, PWB t = − 42.56, p = 0.001).
On the other hand, Table 2 showed no notable change in pre-test and post-test mean scores in both IGD and PWB measures of the participants in the control group who were not administered the ACRIP, i.e., pre-test: IGD 38.40 (SD=5.02), PWB 124.50 (SD=51.45), post-test: IGD 38.10 (SD=3.95), PWB 123.75 (SD=48.40).
The two-way MANOVA of the experimental group's post-test scores in terms of IGD and PWB in Table 3 also revealed that the online ACRIP substantially lowered IGD symptoms and improved adolescents' psychological well-being during this pandemic (IGD: F = 493.42, PWB: F = 2210.54). According to the power analysis, the experimental investigation has a power of .90, indicating a high possibility of obtaining a statistically significant result.
In Table 4, the overall result of the MANOVA test on the post-test mean scores of the IGD and PWB in the experimental group implied a significant difference (F = 301.204) and an observed power of 0.90.
Discussion
This study aimed to see how effective and adaptable online ACRIP was in reducing internet gaming disorder symptoms and improving psychological well-being among Asian adolescents from various social backgrounds during this pandemic. As a result, the following hypotheses were established at the start of the study: (a) IGD may lead to poor psychological well-being; (b) negative cognition influences psychological well-being, and (c) the culture-free online intervention program ACRIP is effective in reducing the symptoms of internet gaming disorder and improving the psychological well-being of selected Asian adolescents.
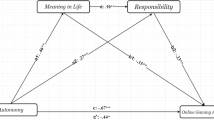
The experimental and control groups had higher mean IGD scores and lower mean PWB scores, confirming the predictions that (a) IGD may lead to poor psychological well-being and (b) adverse cognition affects psychological well-being. This supported Davis's idea that negative cognition (e.g., "I am nothing the offline") can lead to youth gaming more frequently and abandoning everyday activities, perhaps leading to IGD. It may be inferred that adolescent gamers' mental and emotional health declines in proportion to the depth of their negative cognition, which leads to poor psychological well-being, and that the intensity of their IGD symptoms primarily impacts their everyday functioning (Table 5).
The ACRIP regularly causes a noteworthy shift in behavior among adolescents with IGD, as evidenced by post-test findings demonstrating decreased IGD and higher PWB mean scores. The effectiveness of the online intervention program as a whole is not influenced by the participants’ culture. As a result of this trial, the ACRIP became more beneficial due to its increased adaptability benefit. The therapeutic program ACRIP effectively lowers internet gaming disorder symptoms and enhances the psychological well-being of chosen Asian teenagers, and it is culture-free. Overall, statistical analysis revealed that the program modules were practical and had a significant impact on achieving the program's goals.
The online ACRIP modules, which focus on cognitive restructuring and incorporate mindfulness and CBT theories, were successful. The gamers' behavior altered considerably after they understood cognitive distortion and its root causes. The concepts of self-awareness and self-acceptance, along with CBT techniques prevent these negative thought patterns. The theories used were judged to be applicable, and the program structure matches the experts' assessment that they are highly trustworthy in facilitating cognitive reorganization. This study looked at how mindfulness connected people to their underlying thoughts and emotions, which could be the source of their problems. Adolescents who accepted this concept were able to improve their psychological well-being and, as a result, make better life decisions by changing their behavior. As a result, we infer that positive cognition is essential for teenagers' psychological well-being.
Furthermore, during the diagnosis of adolescents with IGD, the program prioritized and investigated specific characteristics of psychological well-being. This helped identify the weak areas that needed to be improved or corrected. This study reveals that aspects of well-being that were determined to be problematic during diagnosis require probing and thorough consideration in designing and altering existing intervention programs to become effective.
Limitations of the Study and Recommendations
The ACRIP was developed as an intervention program that focused on the fundamental cause of the condition rather than the symptoms of IGD during this pandemic. Other risk factors that may have prompted teens to engage in online gaming should be investigated and identified during the diagnostic process. Although the grouping into experimental and control groups was done randomly, the results of the empirical study on the efficacy of the ACRIP utilizing a small sample size of 30 adolescents may not be generalized. Future research examining the long-term effectiveness of the ACRIP should include a larger sample size and, as a result, employ follow-up on participants' performance after they complete the program, as both were not included in this study.
The goal of this research was to add to the empirical evidence on outstanding problems in current research and cross-cultural analysis of IGD and investigate an effective intervention program that health professionals may use to interrupt the cycle of IGD among adolescents. This study supports the construction or restructuring of treatment policies and programs that will decrease the danger of IGD before it becomes a full-blown addiction with severe and detrimental implications for all adolescents at risk of developing it.
Availability of Data and Material
Not applicable.
Code Availability
Not applicable.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (DSM) (4th ed., Rev.) Washington, DC: Author.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM) (5th ed.). Arlington, VA: Author.
Davis, R. A. (2001). A cognitive behavioral model of pathological internet use. Computers in Human Behavior, 17, 187–195.
Elsayed, W. (2021). The negative effects of social media on the social identity of adolescents from the perspective of social work. Heliyon, 7(2), e06327. https://doi.org/10.1016/j.heliyon.2021.e06327
Fuster, H., Carbonell, X., Pontes, H. M., & Griffiths, M. D. (2016). Spanish validation of the Internet Gaming Disorder-20 (IGD-20) Test. Computers in Human Behavior, 56, 215–224. https://doi.org/10.1016/j.chb.2015.11.050
Gentile, D. A., Choo, H., Liau, A., Sim, T., Li, D., Fung, D., & Khoo, A. (2010). Pathological video game use among youths: A two-year longitudinal study. Pediatrics. https://doi.org/10.1542/peds.2010-1353
Gonzales-Bueso V., Santamaria J., Fernandez D., Merino L., Montero E., Jimenez-Murcia S., del Pino-Gutierrez A., & Ribas, J. (2018). Internet Gaming Disorder in Adolescents. Personality, psychopathology, and evaluation. Clinical and Health Psychology.
Hawi, N. S., Samaha, M., & Griffiths, M. D. (2018). Internet gaming disorder in Lebanon: Relationships with age, sleep habits, and academic achievement. J Behav Addict., 7(1), 70–78. https://doi.org/10.1556/2006.7.2018.16.
King, D., & Delfabbro, P. H. (2014). The cognitive psychology of internet gaming disorder. Clinical Psychology Review, 34(4), 298–308. https://doi.org/10.1016/j.cpr.2014.03.2006-16
King, D. L., Haagsma, M. C., Delfabbro, P. H., Gradisar, M., & Griffiths, M. D. (2013). Towards a consensus definition of pathological video-gaming: A systematic review of psychometric assessment tools. Clinical Psychology Review, 33, 331–342.
Kochuchakkalackal, G. K., & Reyes, M. E. S. (2019). Compulsive internet gaming and its relationship with poor psychological well-being among selected adolescents. Journal of Technology in Behavioral Science, 4, 303–308. https://doi.org/10.1007/s41347-019-00098-7
Kuss, D. J., & Griffiths, M. D. (2012a). Online gaming addiction in children and adolescents: A review of empirical research. Journal of Behavioral Addictions, 1(1), 3–22. https://doi.org/10.1556/JBA.1.2012.1.1
Kuss, D. J., & Griffiths, M. D. (2012b). Internet gaming addiction: A systematic review of empirical research. International Journal of Mental Health and Addiction, 10(2), 278–296.
Kuss, D. J., Griffiths, M. D., & Pontes, H. M. (2017). Chaos and confusion in DSM-5 diagnosis of IGD: Issues, concerns and recommendations for clarity in the field. Journal of Behavioral Addiction. https://doi.org/10.1556/2006.5.2016.062
Langer, E. J. (2000). Mindful learning. Current Directions in Psychological Sciences, 9(6), 220–223. https://doi.org/10.1111/1457-8721.00099
Moudiab, S., & Spada, M. M. (2019). The relative contribution of motives and maladaptive cognitions to levels of Internet Gaming Disorder. Addictive Behaviors Reports, 9, 100160.
Pontes, H. M., & Griffiths, M. D. (2015). Measuring DSM-5 internet gaming disorder: Development and validation of a short psychometric scale. Computers in Human Behavior, 45, 137–143. https://doi.org/10.1016/j.chb.2014.12.006
Pontes, H. M., & Griffiths, M. D. (2016). Portuguese validation of the internet gaming disorder scale-short-form. Cyberpsychology Behavior and Social Networking, 19(4), 288–293.
Ryff, C. D., & Keyes, C. L. M. (1995). The structure of psychological well-being revisited. Journal of Personality & Social Psychology, 69, 719–727. https://doi.org/10.1037/0022-3514.69.4.719
Stavropoulos, V., Kuss, D. J., Griffiths, M. D., Wilson, P., & Motti-Stefanidi, F. (2017). MMORPG gaming and hostility predict Internet addiction symptoms in adolescents: An empirical multilevel longitudinal study. Addictive Behaviors, 64, 294–300. https://doi.org/10.1016/j.addbeh.2015.09.001
Subramaniam, M., Abdin, E., Chua, B. Y., Pang, S., Satghare, P., Verma, S., Vaingankar, J., Ong, H. S., Chong, S. A., & Picco, L. (2016). Prevalence and correlates of internet gaming problem among internet users. Results from an Internet Survey. Annals of the Academy of Medicine, 45(5), 174–183.
World Health Organization. (2018). International classification of diseases. https://icd.who.int/browse11/l-m/en
Acknowledgements
Duly acknowledged.
Funding
The author declares that there is no funding.
Author information
Authors and Affiliations
Contributions
Not applicable.
Corresponding author
Ethics declarations
Conflict of interest
The author declares that there is no Conflict of interest.
Consent to Participate
Not applicable.
Consent for Publication
Authors have complete freedom.
Ethics Approval
Received from Manila Med Ethics Review Committee.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kochuchakkalackal Kuriala, G., Reyes, M.E.S. Cross-Cultural Efficacy of the Acceptance and Cognitive Restructuring Intervention Program (ACRIP) on the Internet Gaming Disorder Symptoms of Selected Asian Adolescents. Psychol Stud 68, 326–334 (2023). https://doi.org/10.1007/s12646-023-00721-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12646-023-00721-x