
Abstract
Purpose
There is a paucity of literature on anesthetic drug shortages and their impact on patient safety in lower-middle-income countries. We sought to determine the magnitude of the problem, the effect on patient care and safety, and the adverse patient outcomes witnessed by anesthesiologists in Pakistan
Methods
We conducted a nationwide, multicentre, cross-sectional survey of a representative sample of anesthesiologists in Pakistan (January 2021 to June 2021). The survey questionnaire was adapted from the American Society of Anesthesiologists (ASA) survey on drug shortages and was modified based on the national essential medication list 2018 of Pakistan. It was distributed through Google Forms to anesthesiologists practicing in both the private and government sector. The names of hospitals or the identity of anesthesiologists was not required. The questionnaire consisted of 20 items and focused on the anesthesiologists’ experience of drug shortages, the availability of drugs, and the impact of drug shortages on their individual practice.
Results
Two hundred and forty-six responses were received. Approximately 50% (122/246) of anesthesia practitioners in Pakistan reported anesthetic drug shortages. Fifty-seven percent of respondents mentioned using an inferior drug that may have significantly affected the delivery of anesthetic care. Four participants mentioned severe morbidity and another four mentioned observing a mortality associated with drug shortage.
Conclusion
Anesthetic drug shortages are common in anesthetic practice in Pakistan and they appear to affect patient care and outcomes.
Résumé
Objectif
Il existe peu de littérature sur les pénuries de médicaments anesthésiques et leur impact sur la sécurité des patients dans les pays à revenu intermédiaire ou faible. Nous avons cherché à déterminer l’ampleur du problème, l’effet sur les soins et la sécurité des patients ainsi que les issues indésirables observées par les anesthésiologistes au Pakistan.
Méthode
Nous avons mené une enquête transversale multicentrique à l’échelle nationale auprès d’un échantillon représentatif d’anesthésiologistes au Pakistan (janvier 2021 à juin 2021). Le questionnaire de l’enquête a été adapté de l’enquête de l’American Society of Anesthesiologists (ASA) sur les pénuries de médicaments et a été modifié en fonction de la liste nationale des médicaments essentiels 2018 du Pakistan. Il a été distribué via Google Forms aux anesthésiologistes exerçant dans les secteurs privé et gouvernemental. Les noms des hôpitaux et l’identité des anesthésiologistes n’étaient pas demandés. Le questionnaire comprenait 20 éléments et portait sur l’expérience des anesthésiologistes en matière de pénuries de médicaments, la disponibilité des médicaments et l’impact des pénuries de médicaments sur leur pratique individuelle.
Résultats
Deux cent quarante-six réponses ont été reçues. Environ 50 % (122/246) des praticiens anesthésistes au Pakistan ont signalé des pénuries de médicaments anesthésiques. Cinquante-sept pour cent des répondants ont mentionné avoir utilisé un médicament de qualité inférieure qui pourrait avoir eu une incidence significative sur la prestation des soins anesthésiques. Quatre participants ont mentionné une morbidité grave et quatre autres ont mentionné avoir observé une mortalité associée à une pénurie de médicaments.
Conclusion
Les pénuries de médicaments anesthésiques sont courantes dans la pratique anesthésique au Pakistan et semblent affecter les soins aux patients et les devenirs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Medication shortages are presently a global issue in both high-income countries (HIC) and low–middle-income countries (LMICs) and have both quality and financial ramifications.1 These can be compounded further in some countries by additional issues of import, licensing, government policies, and problems in local manufacturing.2 Anesthesia as a specialty is particularly affected by shortages because they can have a significant effect on patient safety.3,4 In spite of this, there is a paucity of data in anesthetic literature, particularly from LMICs.
Pakistan is a LMIC located in South Asia with a population of approximately 208 million.5 A few studies by local pharmacists have discussed medication shortages with a focus on the production and distribution of medication,6,7 but there are little evidence-based data highlighting the actual shortages faced by the anesthesiologists. An editorial published in the only anesthetic journal in Pakistan in 2009 had focused on the unavailability of essential anesthetic drugs in the country. Another editorial published in the same journal in 2019 pointed out that data need to be available on the magnitude of the problem to tackle drug shortages and for strategies to be recognized.8,9
As there was no prior information available from the end-users on anesthetic drug availability, we sought to undertake a nationwide survey of anesthesiologists in the country to determine the magnitude of the problem, its effect on patient care and safety, and adverse patient outcomes witnessed in their practice.
Methods
We conducted a multicentred cross-sectional survey between January 2021 and June 2021 among anesthesiologists practicing in different secondary and tertiary public or private sector hospitals in Pakistan.
The questionnaire was adapted from the American Society of Anesthesiologists (ASA) drug shortages survey10 and was modified based on the 2018 national essential medication list of Pakistan11 and the 2019 World Health Organization (WHO) essential drug list.12 Other locally used medications were added to the list. The modifications were done with the help of two other consultant anesthesiologists who reviewed the tool and gave their recommendations. After this, we pretested the survey in our own institution (sample size, 10). The questionnaire consisted of three different sections. The first section included a brief explanation of the study and informed consent. The second section covered the major demographic variables related to the institution of practice, province, working hours, and years of anesthesia experience. The names of hospitals or the identity of anesthesiologists was not required. A coded list of anesthesiologists’ e-mails was kept by the principal investigator. The third section focused on the anesthesiologists’ experience of drug shortages, drug unavailability, and the impact of drug shortages on their individual practice at the time of filling in the survey. More than one answer was possible to questions in the third section. An option for open-ended suggestions for other drugs they felt should be available for anesthetic use in Pakistan was also included. The questionnaire was in English since the language is widely spoken and understood in the scientific community in Pakistan. It consisted of 20 items (Electronic Supplementary Material, eAppendix).
A waiver was requested and obtained from the ethical review committee of The Aga Khan University to administer this noninterventional survey. A list of hospitals was obtained from the Pakistan Bureau of Statistics.13 Purposive sampling was used to select hospitals from each province, i.e., Sindh, Punjab, Baluchistan, and Khyber Pakhtunkhwa. The criteria of the sampling were to select a mix of both government-owned and private hospitals from different administrative divisions of the four provinces, so as to represent anesthesiologists from all over the country. E-mail addresses of anesthesiologists were obtained from the Pakistan Society of Anesthesiologists’ resources. The questionnaire was distributed via Google Forms to anesthesiologists working in these hospitals in all four provinces. An electronic survey link to the Google form was sent by e-mail. Each questionnaire was accompanied by a cover letter in English, explaining the purpose of the survey and a separate consent form to be signed by the individual anesthesiologists. In case of no response to the initial e-mail, two reminders were sent after 30 and 45 days. Only participants who had more than two years of training in anesthesia were included in the study. Not more than two anesthesiologists from one hospital were included. No incentives were offered to complete the survey.
Data analysis
All data were entered and analyzed through IBM SPSS Statistics for Windows version 23.0 (IBM Corp., Armonk, NY, USA). We used descriptive statistics to evaluate the data.
Results
We received 246/350 responses, representing a return rate of 70%. In total, the sample represented 196 hospitals in Pakistan.
Table 1 shows the provincial distribution, type of hospitals, and anesthetic work experience of the surveyed population. Sixty-five percent of the anesthesiologists were from Punjab. Eighty-seven percent were working more than five days per week in the operating rooms. The majority (96%) were also administering anesthesia for emergency surgeries in their practice.
Report on drug shortages
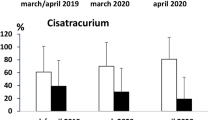
All responders described a current shortage of one or more anesthesia drugs. Drugs that were reported short by more than 50% of anesthesiologists are shown in the Figure. These shortages reflect a period of six months from January 2021 to June 2021. Table 2 shows the percentage of anesthesiologists who reported the shortage of each medication.

Drug shortages reported by more than 50% of anesthesiologists (January 2021–June 2021)
Effect of COVID-19 on drug shortages
Approximately half of the respondents (122/246, 50%) reported that, since the onset of the COVID-19 pandemic, they had experienced further shortage of anesthetic drugs in their workplace.
Impact of drug shortages
The impact of drug shortages as reported by the anesthesiologists is shown in Table 3. This question had more than one possible answer. Fifty-seven percent of anesthesiologists reported using an inferior anesthetic drug because a better agent was not available. Table 3 summarizes the different ramifications due to drug shortages. Forty-four percent of participants noted that drug shortages had increased the cost of anesthesiology in their hospital. As regards patient care, the unavailability of drugs led to mortality in four reports (2%).
Discussion
The World Health Organization has stated that medication shortages are a less-investigated issue in LMIC. They further state that access to essential medications is an indicator of the right to health.14 In our survey, approximately one out of two anesthesia practitioners in Pakistan reported anesthetic drug shortages of some kind in their workplace during the first six months of 2021. Fifty-seven percent of respondents mentioned using an inferior drug that may have affected the delivery of anesthetic care. There were four reports of severe morbidity and another four of having observed a mortality associated with drug shortages. We explain the anesthesia setup in Pakistan at the end of the Discussion.
Anesthetic drug shortages often have adverse outcomes because not all therapeutic substitutes are equivalent.15 A marker of quality in anesthetic care is the prevention of adverse postoperative outcomes such as postoperative nausea and vomiting.16 Forty-four percent of anesthesiologists in our survey reported a shortage in antiemetic drugs like ondansetron, and 23% reported an increase in postoperative nausea and vomiting. As noted, in four cases of drug shortage, the outcome was patient mortality. We do not have details of these reports because of the nature of the survey, but the statements reflect the negative effect of drug shortages perceived by our participants.
Regarding the economic cost of drug shortages, nearly half of participants reported that drug shortages increased the cost of anesthesiology in their department. This has been pointed out in other surveys from HIC.17 The cost of care in these cases may be increased for various reasons, such as the difference in cost between the original drug and the substituted drug, increased labor costs, increased time investments by the pharmacy, delays in getting the substitutes, and cancelations due to drug unavailability.
Seventeen percent of participants in our study reported using less familiar agents. This could explain the drug errors reported by 8% of respondents, but we cannot confirm this because of our survey design. Drug shortages can increase medication errors as pointed by other authors.18 In our survey, 36% of participants said that drug shortages increased the operating time and postoperative recovery time and delayed discharge from the hospital. These results are consistent with those of other studies that drug shortages are associated with an extended stay in the hospital.18,19 Other reasons for a longer operating time are delays getting substitute drugs from the pharmacy, complications caused by incorrect drug administration, and prolonged effects of the substituted drug.
Even before the COVID-19 pandemic, Pakistan was struggling with a drug shortage due to a lack of regulatory policies and financial constraints.6,7 The burden of the pandemic has exacerbated the crisis further, with panic buying and hoarding of drugs like methylprednisolone, chloroquine, ivermectin, and azithromycin—drugs that were needed to manage COVID-19 cases in critical care.20
Similar surveys have been reported from Canada and the USA;3,4 however, we were unable to find a similar survey from our region. In the USA survey, medications that were unavailable to more than 50% of anesthesiologists were neostigmine and thiopental. The Canadian survey (2013) used a different methodology and looked at trends over four time intervals. Drug shortages reported in the previous 12 months were ephedrine (27.5%), propofol (17.9%), and succinylcholine (13.5%). In our survey, the availability of relatively newer drugs like rocuronium, sevoflurane, and ropivacaine was more of an issue. Halothane shortages are understandable as its production decreased after the introduction of isoflurane and sevoflurane; however, it is still used by some because it is cheaper. Availability of opioids is a chronic issue in our country.8,9 Fentanyl is imported but it is only available in a few teaching hospitals. Alfentanil and remifentanil are not yet approved in Pakistan. Lack of availability of short-acting opioid analgesics results in substitution for long-acting drugs like nalbuphine or tramadol for both intraoperative and postoperative analgesia. This increases the recovery time and postanesthesia recovery room stay. Morphine is locally manufactured and cheap, but morphine and fentanyl are tightly controlled by the national drug regulatory authority, which issues only a set quota to individual hospitals for the whole year. No further quota are issued if the yearly quota is used up. Nickerson et al.21 reviewed the access of controlled medications in LMIC and commented on restrictive national laws and policies present in many of the countries. They emphasized the role of the anesthesia community in collaborating with policy makers to improve access to controlled medications.21
Shortage of oxygen and nitrous oxide probably reflects a local procurement issue in government institutions as the purchase mechanism there is more bureaucratic than that in private hospitals. This is not due to production or cost. Lack of oxygen, as reported by 35% of our respondents, leads to cancelation of cases. Nitrous oxide shortages are particularly important in the absence of potent opioids. In such circumstances, most hospitals use 100% oxygen as the carrier gas as medical air is not freely available. Unavailability of nitrous oxide and potent opioids results in more hemodynamic variations than when air is used with less potent analgesics. Long-term use of high-percentage oxygen also leads to generation of free radicals and lung injury.22
Some respondents specifically commented on the unavailability of drugs in secondary care government-owned hospitals, while they were available in teaching hospitals.
Regarding requests for other drugs, the majority requested short-acting synthetic opioids such as remifentanil. It is surprising to note that a very small number requested dantrolene, which is not on the formulary and is not available in Pakistan. Dexmedetomidine was added to the formulary in 2021 and is currently freely available.
A recent qualitative study explored the regulatory and supply hurdles for drug shortages in Pakistan and identified shortages of raw materials, nontraditional distribution, and sudden fluctuations in demand as the main hurdles.23 They did not include physicians in their survey. Drug-related policies are implemented by the Drug Regularity Authority of Pakistan.24 Which of these issues applies to anesthetic drugs needs to be explored further. Our survey did not explore the reasons for these drug shortages because this is not under the control of anesthesiologists; we focused on the extent of the problem and the type of drugs that are in short supply.
Strengths and limitations
A strength of our study is its national scope. Although not all anesthesiologists or hospitals in Pakistan were included, a representative sample was taken from each province. The differences in sample size reflect the differences in population size of the provinces.
This study has some limitations. First, the results were likely affected by recall bias, which is common in such surveys. Second, we did not examine the duration of or reasons for drug shortages. Third, we did not ask about the details of severe morbidity and mortality. Finally, we did not differentiate between secondary and tertiary hospitals.
Anesthesia services in Pakistan
The College of Physicians and Surgeons of Pakistan is responsible for training anesthesia specialists in Pakistan. It offers two types of structured, competency-based training: a four-year fellowship (FCPS) and a two-year membership basic training diploma (MCPS). Both cadres can practice as consultants in hospitals, FCPS holders in teaching hospitals and MCPS holders in peripheral hospitals. The licensing body is the Pakistan Medical Council.
Healthcare in Pakistan is provided by both public and private sector hospitals. The two systems run in parallel. Either of these hospitals could be teaching or non-teaching. Public hospitals are three-tiered, primary, secondary, and tertiary, with anesthesia services required in the secondary and tertiary hospitals. Public sector is financed by the government and the public healthcare structure is organized according to 37 administrative divisions. The distribution of anesthesiologists between these hospitals is not known.
Conclusion
In conclusion, drug shortages are common in anesthetic practice in Pakistan and appear to affect patient care and outcomes. There is a need to explore underlying factors further to frame a strategy for prevention.
References
Gray A, Manasse HR Jr. Shortages of medicines: a complex global challenge. Bull World Health Organ 2012; 90: 158–A. https://doi.org/10.2471/blt.11.101303
Atif M, Malik I, Mushtaq I, Asghar S. Medicines shortages in Pakistan: a qualitative study to explore current situation, reasons and possible solutions to overcome the barriers. BMJ Open 2019; 9: e027028. https://doi.org/10.1136/bmjopen-2018-027028
Hall R, Bryson GL, Flowerdew G, et al. Drug shortages in Canadian anesthesia: a national survey. Can J Anesth 2013; 60: 539–51. https://doi.org/10.1007/s12630-013-9920-z
De Oliveira GS Jr, Theilken LS, McCarthy RJ. Shortage of perioperative drugs: implications for anesthesia practice and patient safety. Anesth Analg 2011; 113: 1429–35. https://doi.org/10.1213/ane.0b013e31821f23ef
Pakistan Bureau of Statistics. Population census. Available from URL: http://www.pbs.gov.pk/content/population-census (accessed October 2022).
Fatima SA, Khaliq A. A survey regarding drug shortage in tertiary care hospitals of Karachi, Pakistan. J Pharm Pract Commun Med 2017; 3: 262–6. http://dx.doi.org/https://doi.org/10.5530/jppcm.2017.4.69
Zaidi S, Bigdeli M, Aleem N, Rashidian A. Access to essential medicines in Pakistan: policy and health systems research concerns. PLoS One 2013; 8: e63515. https://doi.org/10.1371/journal.pone.0063515
Khan TH. Availability of essential drugs in Pakistan. Anaesth Pain Intensive Care 2009; 13: 1–3. Available from URL: https://www.apicareonline.com/index.php/APIC/issue/view/33 (accessed October 2022).
Khan FA. Anesthetic drugs shortage in lower and middle income countries: a safety and quality issue. Anaesth Pain Intensive Care 2019: 24: 337–9. https://doi.org/10.35975/apic.v23i4.1164
ECRI. ASA drug shortage survey: effects on anesthesia practice, patients 2012. Available from URL: https://www.ecri.org/search-results/member-preview/physicianpracticeenews/pages/phys050412_asa (accessed October 2022).
Drug Regulatory Authority of Pakistan. National essential medicines list 2018. Available from URL: https://www.dra.gov.pk/wp-content/uploads/2022/07/NEML-OCTOBER-2018.pdf (accessed October 2022).
World Health Organization. World Health Organization model list of essential medicines, 2019. Available from URL: https://apps.who.int/iris/bitstream/handle/10665/325771/WHO-MVP-EMP-IAU-2019.06-eng.pdf?ua=1 (accessed October 2022).
Pakistan Bureau of Statistics. Hospitals/dispensaries and beds by province. Available from URL: https://www.pbs.gov.pk/sites/default/files/tables/social_statistics/Hospital_Dispanceries.pdf (accessed October 2020).
Perehudoff K. Universal access to essential medicines as part of the right to health: a cross-national comparison of national laws, medicines policies, and health system indicators. Glob Health Action 2020; 13: 1699342. https://doi.org/10.1080/16549716.2019.1699342
Dutton RP, Cohen JA. Medication shortages: are we the iron chefs or our own worst enemies? Anesth Analg 2011; 113: 1298–9. https://doi.org/10.1213/ane.0b013e3182282968
Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg 1999; 89: 652–8. https://doi.org/10.1097/00000539-199909000-00022
Kaakeh R, Sweet BV, Reilly C, et al. Impact of drug shortages on U.S. health systems. Am J Health Syst Pharm 2011; 68: 1811–19. https://doi.org/10.2146/ajhp110210
McLaughlin M, Kotis D, Thomson K, et al. Effects on patient care caused by drug shortages: a survey. J Manag Care Pharm 2013; 19: 783–8. https://doi.org/10.18553/jmcp.2013.19.9.783
Shukar S, Zahoor F, Hayat K, et al. Drug shortage: causes, impact, and mitigation strategies. Front Pharmacol 2021; 12: 693426. https://doi.org/10.3389/fphar.2021.693426
Hashmi FK, Atif N, Malik UR, et al. Misinformation in wake of the COVID-19 outbreak: fueling shortage and misuse of lifesaving drugs in Pakistan. Disaster Med Public Health Prep 2021; 15: e32–3. https://doi.org/10.1017/dmp.2020.400
Nickerson JW, Pettus K, Wheeler KE, et al. Access to controlled medicines for anesthesia and surgical care in low-income countries: a narrative review of international drug control systems and policies. Can J Anesth 2017; 64: 296–307 https://doi.org/10.1007/s12630-016-0805-9
Amarelle L, Quintela L, Hurtado J, Malacrida L. Hyperoxia and lungs: what we have learned from animal models. Front Med (Lausanne) 2021; 8: 606678. https://doi.org/10.3389/fmed.2021.606678
Kumar S, Bano S. Comparison and analysis of health care delivery systems: Pakistan versus Bangladesh. J Hosp Med Manage 2017; 3: 21–2. https://doi.org/10.4172/2471-9781.100020
Drug Regularity Authority of Pakistan. Homepage. Available from URL: https://www.dra.gov.pk (accessed October 2021).
Author contributions
Mehreen Malik helped design and conduct the study, analyzed the data, and wrote the first draft of the manuscript. Fauzia A. Khan generated the idea, helped design and conduct the study, analyzed the data, and went through the various drafts of the manuscript.
Acknowledgements
We would like to acknowledge the help of Dr. Liaqat Ali, Associate Professor of Anaesthesia, Allama Iqbal Medical College, Lahore, Pakistan, for his help in the distribution of survey forms in the Punjab province.
Disclosures
None.
Funding statement
None.
Editorial responsibility
This submission was handled by Dr. Stephan K. W. Schwarz, Editor-in-Chief, Canadian Journal of Anesthesia/Journal canadien d’anesthésie.
Author information
Authors and Affiliations
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Malik, M., Khan, F.A. Anesthetic drug shortages in Pakistan: a multicentre nationwide survey. Can J Anesth/J Can Anesth 70, 335–342 (2023). https://doi.org/10.1007/s12630-022-02381-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-022-02381-3