
Abstract
Purpose
The aim of this study was to evaluate the safety of drinking carbohydrate-containing fluids two hours prior to surgery in older adults using ultrasonography.
Methods
We conducted a nonrandomized and noninferiority comparative study in 60 patients aged over 65 yr who were scheduled for total knee arthroplasty. Patients who were fasted from midnight (fasting group) or who drank 400 mL of a carbohydrate-containing fluid (carbohydrate ingestion group) two hours prior to surgery were matched for age, sex, and body mass index. We measured the cross-sectional area (CSA) of gastric antrum using ultrasound and estimated the gastric fluid volume as the study’s primary outcome measure. The noninferiority margin (δ) for the mean difference was predefined as 50 mL. The secondary outcome measures included CSA of the antrum and qualitative gastric volume.
Results
The mean (standard deviation) gastric volume was not significantly different between the fasting group and the carbohydrate ingestion group (30.2 [25.4] mL vs 28.4 [35.8] mL; each group, n = 30; P = 0.81). The mean difference in gastric volume was −1.9 mL (95% confidence interval [CI], −17.9 to 14.2), and the upper limit of the 95% CI was lower than the prespecified noninferiority limit (δ = 50 mL). Secondary outcomes were not significantly different between the two groups.
Conclusion
Drinking of carbohydrate-containing fluid two hours prior to surgery was noninferior to overnight fasting with respect to residual gastric volume at induction of anesthesia in healthy older adults who undergoing total knee arthroplasty.
Study registration
ClinicalTrials.gov (NCT04514380); registered 14 August 2020.
Résumé
Objectif
L’objectif de cette étude était d’évaluer l’innocuité de la consommation d’une préparation glucidique deux heures avant une chirurgie chez les personnes âgées à l’aide de l’échographie.
Méthode
Nous avons mené une étude comparative non randomisée et de non-infériorité chez 60 patients âgés de plus de 65 ans qui devaient bénéficier d’une arthroplastie totale du genou. Les patients étaient à jeun depuis minuit (groupe à jeun) ou avaient bu 400 mL d’une préparation glucidique (groupe d’ingestion de glucides) deux heures avant la chirurgie et ont été appariés pour l’âge, le sexe et l’indice de masse corporelle. Nous avons mesuré la section transversale de l’antre gastrique à l’aide de l’échographie et estimé le volume de liquide gastrique en tant que mesure du critère d’évaluation principal de l’étude. La marge de non-infériorité (δ) pour la différence moyenne a été prédéfinie à 50 mL. Les mesures de critères d’évaluation secondaires comprenaient la section transversale de l’antre et le volume gastrique qualitatif.
Résultats
Le volume gastrique moyen (écart type) n’était pas significativement différent entre le groupe à jeun et le groupe d’ingestion de glucides (30,2 [25,4] mL vs 28,4 [35,8] mL; chaque groupe, n = 30; P = 0,81). La différence moyenne de volume gastrique était de -1,9 mL (intervalle de confiance [IC] à 95 %, -17,9 à 14,2), et la limite supérieure de l’IC 95 % était inférieure à la limite de non-infériorité prédéfinie (δ = 50 mL). Aucune différence intergroupe significative n’a été observée dans les critères d’évaluation secondaires.
Conclusion
La consommation d'une préparation glucidique deux heures avant la chirurgie n'était pas inférieure au jeûne nocturne en ce qui concerne le volume gastrique résiduel à l'induction de l'anesthésie chez les personnes âgées en bonne santé qui bénéficient d'une arthroplastie totale du genou.
Enregistrement de l'étude
www.ClinicalTrials.gov (NCT04514380); enregistrée le 14 août 2020.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The risk of pulmonary aspiration and the idea that a longer fast improves the safety of surgical patients have led to excessive preoperative food and fluid restriction. Nevertheless, guidelines for preoperative fasting have changed over the last decade, and recent practice guidelines recommend the ingestion of carbohydrate-containing fluid two hours prior to surgery. This is based on the concept that excessive fasting is not only unnecessary but also detrimental.1,2 Furthermore, modern protocols such as “enhanced recovery after surgery” encourage oral carbohydrate drinks before surgery.3 Nevertheless, various factors known to contribute to delayed gastric emptying, such as advanced age,4 diabetes mellitus,5 and chronic kidney disease,6 warrant consideration when managing preoperative fasting because patients with these factors may not have an empty stomach even after the generally recommended fasting times.7
Gastric function is generally well preserved during healthy aging.8 Nevertheless, there are conflicting results on the effects of aging on gastric emptying time, which have been reported to be accelerated,9 slowed,10 or unchanged.11 To date, evidence supports that a modest slowing of gastric emptying occurs with healthy aging.8 Gastric volume (GV) can be influenced by slowing of gastric emptying in older adults. Nevertheless, studies regarding the safety profile of carbohydrate drinking two hours prior to surgery among older adults are still lacking.
The present study aimed to assess the safety of drinking carbohydrate-containing fluids two hours prior to surgery in older adults. Toward this goal, we sought to compare the residual GV between patients who fasted and patients who ingested carbohydrate-containing fluids two hours preoperatively.
Methods
Study design and patients
We conducted a prospective nonrandomized and noninferiority comparative study at Seoul National University Bundang Hospital between September 2020 and March 2021 according to institutional and Good Clinical Practice guidelines. The participants were older adults (age, 65–85 yr) scheduled for total knee arthroplasty (TKA). Patients older than 86 yr and those with diabetes mellitus, chronic kidney disease, and an American Society of Anesthesiologists (ASA) Physical Status score ≥ III were excluded.
Ethics
This study complied with the 1964 Helsinki Declaration and its later amendments. After approval by Institutional Review Board on 31 August 2020 (B-2008/633-301; Chairperson, Hak Chul Jang; Seoul National University Bundang Hospital), the protocol was registered at ClinicalTrials.gov (NCT04514380, registered on 14 August 2020). The first patient was recruited on 16 September 2020 and the last patient on 19 March 2021. All patients gave their written informed consents before participation.
Trial protocol
Two surgeons performed the TKAs following similar clinical procedures, except for the preoperative fasting protocol. One protocol was overnight fasting, and the other was ingestion of 400 mL of a carbohydrate-containing fluid two hours prior to surgery (Nucare NoNPO® [12.8% maltodextrin, 50 kcal·100 mL−1, 0.52 mg⋅mL−1 sodium, 0.48 mg⋅mL−1 potassium]; Daesang Wellife, Seoul, Republic of Korea). We matched patients in the carbohydrate ingestion group and the fasting group for age (difference, ± 2 yr), sex, and body mass index (BMI; difference, ± 2 kg⋅m−2).
Pre-emptive oral analgesia comprised pregabalin 75 mg, celecoxib 200 mg, and acetaminophen 650 mg with < 20 mL water and was administered 30–60 min before surgery.
Ultrasound examination
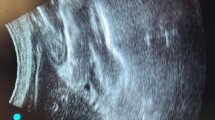
In the preoperative holding area, ultrasound scanning was conducted twice, with patients in a semirecumbent and right lateral decubitus (RLD) position for greatest sensitivity.12 The anesthesiologist who performed the ultrasound scanning was blinded to the patient grouping. A cross-sectional image of the gastric antrum was acquired using a low-frequency convex array transducer (probe rC60xi, 2–5 Hz) connected to a Sonosite EDGE II ultrasound machine (Fujifilm Sonosite, Inc., Bothell, WA, USA). The gastric antrum was evaluated according to a standard protocol.13 We identified the gastric antrum along the edge of the left lobe of the liver anteriorly, and anterior to the aorta in the sagittal or sagittal oblique sonographic view at the epigastric level (Fig. 1). Gastric content was assessed both quantitatively and qualitatively.

Ultrasound image of the gastric antrum in the epigastric area obtained in a sagittal or parasagittal plane. The arrows indicate the gastric antrum; P = pancreas.
Quantitative analysis
We used three images of gastric antrum, which were taken between peristaltic contraction in both semirecumbent and RLD positions, to calculate the cross-sectional area (CSA). To determine the CSA of the antrum in the RLD, we used a formula to calculate the area of an ellipse, using two perpendicular diameters of the antrum: the anteroposterior (AP) and craniocaudal (CC) diameters:
We applied the average value of the three measurements to the following previously validated formula14 to calculate the residual GV:
In the formula, RLD-CSA refers to the antral CSA measured at the RLD position. A calculated GV < 0 was considered 0 mL.
Qualitative assessment
We used the simple three-point grading system defined by Perlas et al.15 as follows: grade 0 was a completely empty antrum in both semirecumbent and RLD positions; grade 1 was an empty antrum in the semirecumbent position, but visible fluid in the RLD position, and grade 2 was visible fluid in the antrum in both positions, implying a high-volume state.
Outcome measurements
The primary outcome measure was the calculated GV. The secondary outcomes were the qualitative GV (grades 0, 1, and 2) and the CSA of the antrum.
Sample size
We calculated the sample size using the TrialSize Package for R (TwoSampleMean.NIS; R Foundation for Statistical Computing, Vienna, Austria), based on alpha = 0.025, beta = 0.9, sigma = 25, k = 1, delta = 50, and margin = 27 (where alpha, beta, sigma, k, and margin denote significance level, power, pooled standard deviation [SD] of two groups, allocation ratio, noninferiority margin, and true mean difference between two groups, respectively). It was calculated that 28 patients were needed per group to estimate a pooled SD of 25 mL for the primary outcome. This should detect a difference in means of 27 mL with a noninferiority margin of 50 mL, for an alpha level of 0.025 and a power of 90%. On the assumption of an overall rate of loss to follow-up of 20%, this generated a sample size of 32 participants per group.
Statistical analysis
Continuous variables are presented as mean (SD) and categorical variables are presented as numbers and proportion (n/total N [%]). After normality check using the Shapiro–Wilk test, Student’s t test or Fisher’s exact test was used for the former and the Chi square test was used for the latter. We used IBM SSPS for Windows version 25 software (IBM Corp., Armonk, NY, USA) for the calculations and considered all P values significant at the < 0.05 level.
Results
A total of 68 patients scheduled for TKA were evaluated for eligibility. After matching for age, sex, and BMI, the carbohydrate and fasting groups included 32 patients each. Among them, two patients in each group (total four patients) were excluded because of poor ultrasound images, leaving 30 participants in each group for analysis (Fig. 2). Table 1 shows the patients’ baseline characteristics.

Patient inclusion flow chart
Gastric volume
The mean (SD) GVs were 28.4 (35.8) mL and 30.2 (25.4) mL in the carbohydrate and the fasting group, respectively (Table 2). The mean difference of GV was −1.9 (95% confidence interval [CI], −17.9 to 14.2). Noninferiority was identified because the upper limit of the 95% CI was lower than the predetermined noninferiority margin (δ = 50) (Fig. 3). The GV/kg was comparable between the two groups (Table 2).

Noninferiority diagram of gastric volume differences in the carbohydrate group and the fasting group. The dotted line indicates a noninferiority margin (δ) of 50 mL. Squares indicate mean gastric volume differences (carbohydrate group – fasting group), and error bars indicate the 95% confidence interval of the difference between the two groups.
Cross-sectional area and grade
The CSA measured in either semirecumbent or RLD position did not differ significantly between the two groups (Table 2). In the qualitative assessment (Table 2), only one patient showed grade 2 gastric content in the carbohydrate group, whose calculated residual GV was 80.1 mL.
Discussion
Despite the probability of slower gastric emptying in older adults, few studies have evaluated the safety of carbohydrate drinking two hours prior to surgery among this population. This study showed that ingestion of carbohydrate-containing fluid two hours prior to surgery was noninferior to overnight fasting with respect to residual GV in older adults. This finding supports the hypothesis that normal gastric emptying is maintained in older adults without risk factors of delayed gastric emptying.
Gastric emptying following carbohydrate solution intake has been evaluated in several studies.16,17 Nevertheless, most studies have been conducted in healthy volunteers or adults aged under 65 yr. Jian et al.18 evaluated the gastric CSA after the ingestion of a carbohydrate solution in healthy volunteers and showed that carbohydrate intake two hours preoperatively was safe prior to anesthesia. Furthermore, in term parturients who ingested 400 mL of a carbohydrate fluid two hours prior to elective Cesarean delivery, the residual GV returned to the baseline levels within 100 min after the ingestion and did not increase the risk of pulmonary aspiration.19
Gastric emptying time in older adults remains controversial.9,10,11 One study compared the liquid emptying time between young (24–51 yr) and older (71–81 yr) males and reported that the absorption speed of a liquid (but not solid) meal was slower in older men than in younger men, showing retention of 40% in the older men and 25% in the younger men at 120 min.4 In contrast, Hellström et al.20 observed no evidence of delayed gastric emptying and reported that oral intake of a carbohydrate drink prior to surgery did not increase the pulmonary aspiration risk in older women undergoing hip fracture surgery. Despite the coexistence of additional risk factors, such as stress caused by injury, pain, or diabetes, which are known to influence gastric motility, the gastric emptying rate was similar between the old group and the sex-matched control group.
Our results support the notion that there is no difference in residual GV between carbohydrate ingestion and overnight fasting. After administration of 400 mL of carbohydrate fluid, the mean residual GV was about 28 mL. Although one patient had grade 2 GV, the calculated volume was 81 mL (1.3 mL⋅kg−1), and this did not exceed the volume considered as high risk for pulmonary aspiration (1.5 mL⋅kg−1).
Several studies have reported that preoperative carbohydrate intake did not affect the gastric emptying time or residual GV and had no adverse events.21,22 In addition, there were several benefits of drinking carbohydrate fluid prior to surgery, including reducing thirst, hunger, feelings of weakness, or postoperative insulin resistance.23,24
Enhanced recovery after TKA has also shown that carbohydrate drinking may improve insulin resistance and glucose metabolism.25 Nevertheless, the routine ingestion of carbohydrate-containing fluid is not recommended because evidence remains limited and more research is needed in older and frail patients. Although the advantages listed above were not investigated in this study, preoperative carbohydrate intake can be considered in the healthy older adult group according to our results. Further studies are required to confirm that this practice is independent of regurgitation and pulmonary aspiration in older adult patients.
As described in the Methods section, two different preoperative fasting protocols (overnight fasting and carbohydrate drinking) were followed in our TKA patients according to the surgeons’ preference. Although evidence may suggest improvements to fasting guidelines, it is hard to change an old habit. One observational study reported that in a cohort scheduled for elective surgery between 2018 and 2019, the median duration of fasting from clear liquid was 5 hr 23 min and from solid foods was 14 hr 51 min, which is about 2.5 times the recommended two and six hours.26 Continuous efforts should be made to implement the recent fasting guidelines, and excessive preoperative fasting should be avoided in clinical practice.
This study has some limitations that need to be considered when interpreting the findings. First, we did not enroll patients with comorbidities such as diabetes mellitus and chronic kidney disease. These conditions are known to influence gastric emptying time, and these patients are not given carbohydrate-containing fluids in our institution. Further research is required to investigate the effects of these conditions on residual GV after drinking carbohydrate-containing fluid. Second, this was not a randomized study. Nevertheless, all preoperative care plans were similar between the two groups except for the fasting protocol. In addition, age, sex, and BMI were matched to minimize their effects on the GV. Third, we cannot rule out a volume effect of water consumed preoperatively for the pre-emptive oral analgesics. Nevertheless, the allowed volume was less than 20 mL. Furthermore, in some studies, the mean GV was approximately 28 mL to 30 mL even after eight hours of fasting before surgery,27,28 which is similar to ours in the fasting group (30.2 mL). Therefore, the small volume of water taken for pre-emptive oral analgesic medication is unlikely to have had a significant effect on the residual GV measured in this study. Finally, since our study was performed in ASA Physical Status I and II older adults, the generalizability of the results may be limited.
In conclusion, the residual GV after the ingestion of a carbohydrate-containing fluid two hours prior to surgery was noninferior to overnight fasting with respect to residual GV. Hence, routine overnight fasting to minimize the risk of gastric aspiration during the perioperative period in older adults warrants reconsideration. Nevertheless, several older adults have underlying disease (i.e., diabetes mellitus and renal insufficiency), which are known to delay gastric emptying. Further research is needed in these patients to evaluate the residual GV after drinking of a carbohydrate-containing fluid.
References
American Society of Anesthesiologists. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists task force on preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration. Anesthesiology 2017; 126: 376–93.
Smith I, Kranke P, Murat I, et al. Perioperative fasting in adults and children: guidelines from the European Society of Anaesthesiology. Eur J Anaesthesiol 2011; 28: 556–69.
Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg 2017; 152: 292–8.
Moore JG, Tweedy C, Christian PE, Datz FL. Effect of age on gastric emptying of liquid--solid meals in man. Dig Dis Sci 1983; 28: 340–4.
Garg H, Podder S, Bala I, Gulati A. Comparison of fasting gastric volume using ultrasound in diabetic and non-diabetic patients in elective surgery: an observational study. Indian J Anaesth 2020; 64: 391–6.
Strid H, Simrén M, Stotzer PO, Abrahamsson H, Björnsson ES. Delay in gastric emptying in patients with chronic renal failure. Scand J Gastroenterol 2004; 39: 516–20.
Chang JE, Kim H, Won D, et al. Ultrasound assessment of gastric content in fasted patients before elective laparoscopic cholecystectomy: a prospective observational single-cohort study. Can J Anesth 2020; 67: 810–6.
Soenen S, Rayner CK, Horowitz M, Jones KL. Gastric emptying in the elderly. Clin Geriatr Med 2015; 31: 339–53.
Kupfer RM, Heppell M, Haggith JW, Bateman DN. Gastric emptying and small-bowel transit rate in the elderly. J Am Geriatr Soc 1985; 33: 340–3.
Brogna A, Ferrara R, Bucceri AM, Lanteri E, Catalano F. Influence of aging on gastrointestinal transit time. An ultrasonographic and radiologic study. Invest Radiol 1999; 34: 357–9.
Madsen JL, Graff J. Effects of ageing on gastrointestinal motor function. Age Ageing 2004; 33: 154–9.
Bouvet L, Barnoud S, Desgranges FP, Chassard D. Effect of body position on qualitative and quantitative ultrasound assessment of gastric fluid contents. Anaesthesia 2019; 74: 862–7.
Cubillos J, Tse C, Chan VW, Perlas A. Bedside ultrasound assessment of gastric content: an observational study. Can J Anesth 2012; 59: 416–23.
Perlas A, Mitsakakis N, Liu L, et al. Validation of a mathematical model for ultrasound assessment of gastric volume by gastroscopic examination. Anesth Analg 2013; 116: 357–63.
Perlas A, Davis L, Khan M, Mitsakakis N, Chan VW. Gastric sonography in the fasted surgical patient: a prospective descriptive study. Anesth Analg 2011; 113: 93–7.
Yu K, Ke MY, Li WH, Zhang SQ, Fang XC. The impact of soluble dietary fibre on gastric emptying, postprandial blood glucose and insulin in patients with type 2 diabetes. Asia Pac J Clin Nutr 2014; 23: 210–8.
Gomes PC, Caporossi C, Aguilar-Nascimento JE, Candido da Silva AM, Tavares de Araujo VM. Residual gastric volume evaluation with ultrasonography after ingestion of carbohydrate- or carbohydrate plus glutamine-enriched beverages: a randomized, crossover clinical trial with healthy volunteers. Arq Gastroenterol 2017; 54: 33–6.
Jian WL, Zhang YL, Xu JM, et al. Effects of a carbohydrate loading on gastric emptying and fasting discomfort: an ultrasonography study. Int J Clin Exp Med 2017; 10: 788–94.
Popivanov P, Irwin R, Walsh M, Leonard M, Tan T. Gastric emptying of carbohydrate drinks in term parturients before elective caesarean delivery: an observational study. Int J Obstet Anesth 2020; 41: 29–34.
Hellström PM, Samuelsson B, Al-Ani AN, Hedström M. Normal gastric emptying time of a carbohydrate-rich drink in elderly patients with acute hip fracture: a pilot study. BMC Anesthesiol 2017; https://doi.org/10.1186/s12871-016-0299-6.
Kaska M, Grosmanová T, Havel E, et al. The impact and safety of preoperative oral or intravenous carbohydrate administration versus fasting in colorectal surgery--a randomized controlled trial. Wien Klin Wochenschr 2010; 122: 23–30.
Järvelä K, Maaranen P, Sisto T. Pre-operative oral carbohydrate treatment before coronary artery bypass surgery. Acta Anaesthesiol Scand 2008; 52: 793–7.
Hausel J, Nygren J, Lagerkranser M, et al. A carbohydrate-rich drink reduces preoperative discomfort in elective surgery patients. Anesth Analg 2001; 93: 1344–50.
Wang ZG, Wang Q, Wang WJ, Qin HL. Randomized clinical trial to compare the effects of preoperative oral carbohydrate versus placebo on insulin resistance after colorectal surgery. Br J Surg 2010; 97: 317–27.
Wainwright TW, Gill M, McDonald DA, et al. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Acta Orthop 2020; 91: 3–19.
van Noort HH, Eskes AM, Vermeulen H, et al. Fasting habits over a 10-year period: an observational study on adherence to preoperative fasting and postoperative restoration of oral intake in 2 Dutch hospitals. Surgery 2021; 170: 532–40.
Hussain R, Nazeer T, Aziz NH, Ali M. Effects of fasting intervals on gastric volume and pH. Pak J Med Health Sci 2011; 5: 582–6.
Patil MC, Prajwal B. Randomised clinical trial to compare ultrasonography guided gastric volume in patients after overnight fasting and after ingestion of clear fluids two hours before surgery. Indian J Clin Anaesth 2020; 7: 509–13.
Author contributions
Hyun-Jung Shin contributed to the conception and design of the study; collection, analysis, and interpretation of the data; drafting of the manuscript; critical revision; and final approval. Bon-Wook Koo contributed to the development of methodology, statistics, analysis, and final approval. Dongsik Lim contributed to the development of methodology, data analysis, data interpretation, revision of manuscript, and final approval. Hyo-Seok Na contributed to the conception and design of study, critical revision, and final approval.
Disclosures
None.
Funding statement
The authors received no financial support.
Editorial responsibility
This submission was handled by Dr. Stephan K. W. Schwarz, Editor-in-Chief, Canadian Journal of Anesthesia/ Journal canadien d’anesthésie.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shin, HJ., Koo, BW., Lim, D. et al. Ultrasound assessment of gastric volume in older adults after drinking carbohydrate-containing fluids: a prospective, nonrandomized, and noninferiority comparative study. Can J Anesth/J Can Anesth 69, 1160–1166 (2022). https://doi.org/10.1007/s12630-022-02262-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-022-02262-9