
Abstract
Purpose
Epistaxis is a common complication of nasal intubation. Ease of insertion of the tracheal tube may be influenced by bevel orientation and tip bending. We examined ease of insertion and epistaxis with two tubes with different orientations and with or without a stylet to modify tip bending.
Methods
Two hundred patients scheduled to undergo oral or maxillofacial surgery were randomized into four groups according to method of nasal intubation used after induction of anesthesia. In one group, a Portex® tracheal tube was inserted with bevel facing left (Portex Group). In the second group, a Parker Flex-Tip® tube (Parker Group) was inserted with the bevel facing posteriorly, and in the last two groups, a stylet bent at 60° anteriorly was used with the Portex tube (Stylet-Portex Group) or Parker tube (Stylet-Parker Group). When the tube advanced without resistance, insertion was defined as “smooth”, and when resistance was encountered, insertion was defined as “impinged”. Severity of epistaxis was evaluated as none, mild, moderate, or severe.
Results
Smooth insertion was observed in 60% of patients in the Portex Group; 80% in the Parker Group; 100% in the Stylet-Portex Group; and 100% in the Stylet-Parker Group. Epistaxis was found in 50%, 24%, 20%, and 4% of patients, respectively. The styletted tip (difference: 30%; 95% confidence interval [CI]: 20.3 to 38.5; P < 0.0001) was found to improve ease of insertion. Both the posterior-facing bevel (difference: 21%; 95% CI: 9.0 to 32.1; P = 0.0005) and stylet (difference: 25%; 95% CI: 13.1 to 35.9; P < 0.0001) contributed significantly to absence of epistaxis.
Conclusions
Using a styletted tracheal tube with a posterior-facing bevel improves ease of insertion through the nasopharynx and decreases the severity of epistaxis during nasal intubation. Clinical trial registration number: UMIN Clinical Trials Registry (UMIN-CTR), UMIN000011327.
Résumé
Objectif
L’épistaxis est une complication courante de l’intubation nasale. La facilité d’insertion de la sonde trachéale pourrait être influencée par l’orientation du biseau et la courbure de l’extrémité. Nous avons étudié la facilité d’insertion et l’épistaxis avec deux sondes aux orientations différentes et avec ou sans stylet pour modifier la courbure de l’extrémité.
Méthode
Deux cents patients devant subir une chirurgie orale ou maxillo-faciale ont été aléatoirement répartis en quatre groupes selon la méthode d’intubation nasale utilisée après l’induction de l’anesthésie. Dans un groupe, une sonde trachéale Portex® a été insérée avec le biseau orienté vers la gauche (groupe Portex). Dans le deuxième groupe, une sonde Parker Flex-Tip® (groupe Parker) a été insérée avec le biseau orienté vers l’arrière, et dans les deux derniers groupes, un stylet plié à 60° vers l’avant a été utilisé avec une sonde Portex (groupe stylet-Portex) ou une sonde Parker (groupe stylet-Parker). Lorsque la sonde a cheminé sans résistance, l’insertion a été définie comme « facile », et lorsqu’il y a eu résistance, l’insertion a été définie comme « empiétée ». La gravité de l’épistaxis a été évaluée en tant que nulle, légère, modérée ou grave.
Résultats
On a observé une insertion facile chez 60 % des patients du groupe Portex, 80 % du groupe Parker, 100 % du groupe Stylet-Portex et 100 % du groupe Stylet-Parker. On a observé de l’épistaxis chez 50 %, 24 %, 20 % et 4 % des patients, respectivement. On a observé que la pointe avec stylet (différence: 30 %; intervalle de confiance [IC] 95 %: 20,3 à 38,5; P < 0,0001) améliorait la facilité d’insertion. Le biseau vers l’arrière (différence: 21 %; IC 95 %: 9,0 à 32,1; P = 0,0005) et la présence d’un stylet (différence: 25 %; IC 95 %: 13,1 à 35,9; P < 0,0001) ont contribué de façon significative à l’absence d’épistaxis.
Conclusion
L’utilisation d’une sonde trachéale avec stylet et biseautée vers l’arrière améliore la facilité d’insertion via le nasopharynx et réduit la gravité de l’épistaxis pendant une intubation nasale. Numéro d’enregistrement de l’étude clinique: Registre des études cliniques UMIN (UMIN-CTR), UMIN000011327.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Complications related to nasal intubation include epistaxis, fracture of the turbinates, and retropharyngeal injury. Epistaxis is the most common complication, usually resulting from abrasion of the nasal mucosa, including Kiesselbach’s area.1 This problem may be reduced by use of a vasoconstrictor, lubrication of the tracheal tube, use of a small tube, mechanical dilatation of the nasal cavity, or deliberate manipulation of intubation.1 Fracture of the turbinates, particularly the middle turbinate, may lead to traumatic avulsion and massive epistaxis, although this remains a rare complication.2,3 Strategies to enhance ease of insertion of the tube tip through the nasopharyngeal passage are thus essential to reduce nasopharyngeal bleeding.4
Various maneuvers, including thermosoftening the tubes and the telescoping catheter technique, have been proposed to facilitate easy passage through the nasal cavity and reduce epistaxis associated with nasal intubation.5-8 However, many of these methods are ineffective, expensive, or overly complicated. Simple, inexpensive, effective, and convenient methods for clinical anesthesia need to be proposed.7
We hypothesized that nasal bleeding might be prevented and passage of the tube through the nasopharynx might be smoother by facing the bevel toward the posterior nasopharyngeal wall and orienting the tube tip toward the oropharynx. Accordingly, this study was conducted to compare ease of insertion and epistaxis using two tubes with different bevel orientations, with or without a stylet that bends the tube tip in the anterior direction.
Methods
The study was carried out from April 2009 to March 2012 at Kagoshima University Medical and Dental Hospital in Kagoshima in Japan. The study protocol was approved by the Clinical Ethics Committee at Kagoshima University Medical and Dental Hospital (Kagoshima, Japan) (IRB #20-121, approved 12/26/2008), and written informed consent was obtained from all patients prior to participation.
Adult patients with American Society of Anesthesiologists (ASA) physical status class I or II were eligible for this study. Patients with a history of nasal surgery, trauma, recurrent epistaxis, blood dyscrasias, or coagulopathy were excluded from the study. Each patient was scheduled to undergo elective oral or maxillofacial surgery requiring nasal intubation under general anesthesia at Kagoshima University Medical and Dental Hospital.
The bevel of tracheal tubes most commonly used in clinical anesthesia is oriented either to the left or posteriorly. Also, the angle of the distal tip can be changed by inserting a curved stylet. Thus, based on the different bevel orientations and tip bending, patients were allocated into four groups as follows:
-
1.
Portex Group: Portex® tracheal tube (Smiths Medical International, Hythe, Kent, UK). The bevel faces to the left, and no stylet is inserted so the edge of the distal tip is straight. This is a standard left-bevelled tube.
-
2.
Parker Group: Parker Flex-Tip® tracheal tube (Parker Medical Englewood, CO, USA) The tip design differs from that of the Portex tracheal tube. The bevel faces posteriorly when inserted into the trachea, and the distal tip points towards the centre of the tube lumen. No stylet is inserted so the edge of the distal tip is straight. This is a posterior-facing bevel.
-
3.
Stylet-Portex Group: A malleable brass stylet 3 mm in diameter (Igarashi Ika Kogyo, Tokyo, Japan) was inserted into a Portex tube to flex the tube tip anteriorly by approximately 60°. The distal end of the stylet was positioned at the distal end of the cuff, and the bend in the tube was formed about 8 cm from the tip (Fig. 1A).
Fig. 1 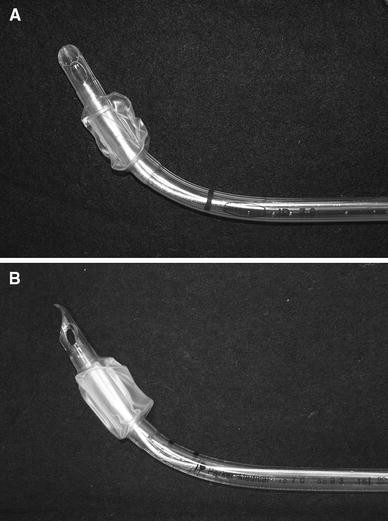
Stylet-Portex tube (A) and Stylet-Parker tube (B), both with a curved stylet to flex the tip anteriorly
-
4.
Stylet-Parker Group: In the same manner as in the Stylet-Portex Group, a stylet with an anterior bend was inserted into a Parker tube to flex the tube tip (Fig. 1B).

Each patient was allocated to one of the four groups differentiated by the direction of the bevel and the tube tip. Block randomization was performed with four groups of 50 patients, and an office staff member with no clinical involvement in the study inserted the group allocation into an opaque envelope and sealed the envelope. The envelope was opened at the induction of anesthesia. The anesthesiologist then prepared the assigned tracheal tube, and another anesthesiologist, unaware of tube assignment until intubation, inserted the tube.
Anesthesia was induced with intravenous propofol 1-2 mg·kg−1, and rocuronium 1 mg·kg−1 was administered intravenously for muscle relaxation. Oxygen and 3-5% sevoflurane were given via face mask. During mask ventilation, the patient’s nasal cavity was lubricated with 2% lidocaine jelly, and then a nasal examination was performed using cotton swabs with a vasoconstrictor to determine which nostril was broader. If conditions were the same on both sides, the right nostril was preferred for intubation. After the tracheal tube was lubricated with 2% lidocaine jelly, an anesthesiologist with more than five years of clinical experience gently inserted a tracheal tube (internal diameter [ID] 7.5 mm for males or 7.0 mm for females9 into the patient’s selected nostril. The tube, without thermosoftening pretreatment,8,10 was manipulated in a caudal direction to pass through the lower pathway along the nasal floor underneath the inferior turbinate,11 and then it was advanced through the nasal passage.
If the tube tip advanced into the oropharynx without resistance, insertion was defined as “smooth” and the tube was inserted into the trachea under direct laryngoscopy. In the Stylet-Portex and Stylet-Parker Groups, the curved stylet was withdrawn from the tube immediately after passage of the tube through the nasopharynx, and tracheal intubation was then performed. On the other hand, if resistance was encountered, insertion was defined as “impinged”, a mark was made on the tube corresponding to the depth of insertion into the nostril, and the distance between the tip and the mark was measured. This assessment of ease of insertion was made only on the first attempt, and no tube rotation against resistance was applied. If insertion was impinged, the tube was withdrawn from the nasal cavity, and reintubation was then performed using a different tube of the same type and other manipulations, including counterclockwise rotation of the tube or reinsertion into the other nostril.
Two independent anesthesiologists who did not observe the tube insertion assessed the severity of epistaxis using a laryngoscope immediately after and five minutes after the tube was passed through the nasal cavity. When the anesthesiologists’ evaluations differed, another anesthesiologist assessed the severity of epistaxis and decided the final score. Epistaxis was evaluated using four grades according to the following criteria: no epistaxis, no blood observed on either the surface of the tube or the posterior pharyngeal wall; mild epistaxis, blood apparent on the surface of the tube or posterior pharyngeal wall; moderate epistaxis, pooling of blood on the posterior pharyngeal wall; and severe epistaxis, a large amount of blood in the pharynx impeding nasotracheal intubation and necessitating urgent orotracheal intubation.8,12
Sample size
The results of our preliminary study revealed that the incidences of epistaxis in the Portex patients (the control group) and Stylet-Portex patients were 50% (four of eight) and 20% (two of ten), respectively. Based on the previous study by Morimoto et al.,10 our consensus was that the difference in these incidences was clinically relevant. Fisher’s exact test was used to determine sample size using α = 0.05 (two-sided), a power of 80%, which indicated that more than 44 patients would be required in each group assuming that the incidence of epistaxis would range between 20% and 50%. A total sample of 200 patients was therefore recruited for the four groups. Sample size calculations were carried out using PS: Power and Sample Size Calculation version 3.0.43 software (Vanderbilt University, TN, USA).
Statistical analysis
Study data are expressed as mean (standard deviation) or number of patients.
The incidence of smooth insertion through the nasopharynx and the severity of epistaxis were compared using the χ2 test or Fisher’s exact test if the number of observations obtained for analysis was small. The difference in the incidence, 95% confidence interval (CI), and P value were calculated. In the impinged tracheal tube, Student’s two-sample t test was used to analyze the distance between the tube tip and the mark on the tube.
Statistical analysis was performed using StatView version 5.0 and JMP® version 9.0.2 software (SAS Institute, Cary, NC, USA). P values < 0.05 were considered statistically significant. All tests are two-sided.
Results
Two hundred patients were randomized during April 2009 to March 2012, and the study ended because the target sample size of 200 had been reached at that time. All eligible patients agreed to participate and received their allocated intervention, and no patients were lost to follow-up. There were no missing data and no patients were excluded from the analysis. There was no crossover, and nasal intubation was performed in all patients using the assigned tracheal tube. No serious complications or traumatic events were encountered throughout the study, including turbinectomy and retropharyngeal laceration.
The baseline characteristics of the patients in the four groups were reasonably balanced (Table 1).
When a stylet was not used, resistance was encountered while advancing the tube into the nasal cavity in 40% (20 of 50) of patients in the Portex Group and 20% (ten of 50) of patients in the Parker Group (difference: 20%; 95% CI: 2.0 to 36.4; P = 0.029) (Tables 2, 3). On the other hand, in the Stylet-Portex and Stylet-Parker Groups, all tubes passed through the nasopharyngeal curve without resistance, and insertion was judged as smooth in all patients (Table 2). The tubes with a styletted tip were associated with a significantly smoother insertion than the tubes without a stylet (difference: 30%; 95% CI: 20.3 to 38.5; P < 0.0001) (Table 3).
When advancement of the tube through the nasopharynx was impinged, mean distance from the tube tip to the mark on the tube was 98 mm in the Portex Group and 109 mm in the Parker Group (Table 2, P = 0.006).
Nasal bleeding was observed in 50% (25 of 50) of patients in the Portex Group and 24% (12 of 50) of patients in the Parker Group (difference: 26%; 95% CI: 7.0 to 43.0; P = 0.006) (Tables 2 and 3). The incidences of mild, moderate, and severe epistaxis in the Portex Group were higher than in the Parker Group (Table 2).
The posterior-facing bevel was significantly associated with reduced epistaxis when compared with the left-facing bevel (difference: 21%; 95% CI: 9.0 to 32.1; P = 0.0005), and the styletted tip was significantly associated with reduced epistaxis when compared with the straight tip (difference: 25%; 95% CI: 13.1 to 35.9; P < 0.0001) (Table 3).
Discussion
The present study shows that, for nasal intubation, tracheal tubes with a posterior-facing bevel are associated with less epistaxis than standard tubes with a left-facing bevel. In addition, using an anteriorly curved stylet for both types of tubes made insertion even easier and produced less epistaxis.
The Parker tube is characterized by a posterior-facing bevel as well as the flexible and curved edge of the distal tip.13-16 When the tip of the Parker tube reached the curve of the nasopharynx, we presume that the bevel touched and slid along the posterior wall, as if the conventional tube were rotated 90° counterclockwise.17 The tip was thus able to pass smoothly along the curve of the nasopharynx (Fig. 2). At that time, the flexible and curved edge of the tip probably curled inward and a larger surface area of the tip came into contact with the mucous membrane, reducing the pressure exerted on the nasopharyngeal wall.18,19

Placement of the Stylet-Parker tube in the nasal cavity. The styletted Parker tube contributed to smooth insertion through the nasopharynx and reduction in the incidence of epistaxis due to anterior flexion of the distal tip, posterior-facing bevel, and flexible edge
In patients with impinged insertion in the Portex and Parker Groups, when resistance was encountered while advancing the tube into the nasal cavity, the distance from the distal tip to the nostril corresponded with the distance from the retropharyngeal wall to the nostril, suggesting that tube advancement stopped at the retropharyngeal wall.
In the Stylet-Portex and Stylet-Parker Groups, insertion of the tube was considered smooth in all patients and risk of epistaxis was lower than in the Portex and Parker straight tip groups. Hence, anterior flexion of the tube tip using a stylet is associated with considerably smoother insertion through the nasopharynx and reduced bleeding from the nasal cavity. When the styletted tube tip approached the curve of the nasopharynx, we presume that it easily turned with the curve as it advanced toward the oropharynx, consequently reducing damage to the nasopharyngeal mucosa.
A stylet is commonly used to turn the tube tip up toward the glottis as the tube tip advances toward the esophagus during orotracheal intubation. In this study, however, a curved stylet was used only to flex the distal tip of the tube anteriorly and was removed immediately after the tip was successfully inserted into the nasal cavity. Use of a stylet is generally considered dangerous in nasal intubation; however, the risk seems to depend on how the styletted tube is manipulated. The styletted tube was passed slowly through the inferior nasal meatus along the nasal floor and then advanced with discreet cephalad tilting of the proximal end of the tube. The stylet was carefully removed from the tube immediately after the tube tip passed through the nasal cavity. In our view, this gentle manipulation using a curved stylet facilitated the high success rate of smooth tube advancement. For 25 years, styletted tubes have been used safely at our hospital for nasal intubation in more than 5,200 patients scheduled for oral or maxillofacial surgery. A metal stylet was selected in our study because an overly soft stylet could not maintain the tip angle while the tube was advanced through the nasal cavity.
Several limitations to the present study must be considered when interpreting the results. First, preoperative evaluation of nasal anatomy was not performed by otolaryngologists, and postoperative complications in the nasal cavity, such as nasal pain or mucosal tearing, were not assessed. Second, the tube tips compared in this study were limited to only two designs. Evaluation of other tubes with different tip designs is needed. Additional studies are needed to address this limitation. Finally, the anesthesiologists who assessed epistaxis to define the severity of bleeding were able to see the tube tip and cuff during laryngoscopy; therefore, they would have been able to identify the design of the tube tip. Blinding the anesthesiologists to the tube design does not appear feasible, hence, the possibility of bias was not completely excluded.
In conclusion, a styletted tracheal tube with a posterior-facing bevel enhanced ease of insertion through the nasopharynx and reduced the risk of epistaxis during nasal intubation. The use of a stylet and a posterior-facing bevel can be implemented in adult patients requiring nasal intubation.
References
Hall CE, Shutt LE. Nasotracheal intubation for head and neck surgery. Anaesthesia 2003; 58: 249-56.
Williams AR, Burt N, Warren T. Accidental middle turbinectomy: a complication of nasal intubation. Anesthesiology 1999; 90: 1782-4.
Dost P, Armbruster W. Nasal turbinate dislocation caused by nasotracheal intubation. Acta Anaesthesiol Scand 1997; 41: 795-6.
Sim WS, Chung IS, Chin JU, et al. Risk factors for epistaxis during nasotracheal intubation. Anaesth Intensive Care 2002; 30: 449-52.
Seo KS, Kim JH, Yang SM, Kim HJ, Bahk JH, Yum KW. A new technique to reduce epistaxis and enhance navigability during nasotracheal intubation. Anesth Analg 2007; 105: 1420-4.
Watt S, Pickhardt D, Lerman J, Armstrong J, Creighton PR, Feldman L. Telescoping tracheal tubes into catheters minimizes epistaxis during nasotracheal intubation in children. Anesthesiology 2007; 106: 238-42.
Morimoto Y, Sugimura M, Hirose Y, Taki K, Niwa H. Nasotracheal intubation under curve-tipped suction catheter guidance reduces epistaxis. Can J Anesth 2006; 53: 295-8.
Kim YC, Lee SH, Noh GJ, et al. Thermosoftening treatment of the nasotracheal tube before intubation can reduce epistaxis and nasal damage. Anesth Analg 2000; 91: 698-701.
Dauphinee K. Nasotracheal intubation. Emerg Med Clin North Am 1988; 6: 715-23.
Agarwal A. Warming the tracheal tube and kinking. Can J Anesth 2004; 51: 96.
Ahmed-Nusrath A, Tong JL, Smith JE. Pathways through the nose for nasal intubation: a comparison of three endotracheal tubes. Br J Anaesth 2008; 100: 269-74.
Sanuki T, Hirokane M, Matsuda Y, Sugioka S, Kotani J. The Parker Flex-Tip™ tube for nasotracheal intubation: the influence on nasal mucosal trauma. Anaesthesia 2010; 65: 8-11.
Higueras J, Onrubia X, Sanchez de Meras A, Estruch M, Barbera M. Parker Flex-Tip tube for fibreoptic nasotracheal intubation in a case of lingual tonsil hypertrophy. Can J Anesth 2005; 52: 778-9.
Baraka A, Rizk M, Muallem M, Bizri SH, Ayoub C. Posterior-beveled vs lateral-beveled tracheal tube for fibreoptic intubation. Can J Anesth 2002; 49: 889-90.
Cywinski JB, Zura A, Doyle DJ. Unexpected obstruction of a Parker Flex-Tip™ tracheal tube in a patient with subglottic stenosis. Anesth Analg 2008; 106: 1924.
Kristensen MS. The Parker Flex-Tip tube versus a standard tube for fiberoptic oropharyngeal intubation: a randomized double-blind study. Anesthesiology 2003; 98: 354-8.
Asai T, Shingu K. Difficulty in advancing a tracheal tube over a fibreoptic bronchoscope: incidence, causes and solutions. Br J Anaesth 2004; 92: 870-81.
Xue FS, Xiong J, Yuan YJ, Wang Q. The Parker Flex-Tip™ tube for nasotracheal intubation. Anaesthesia 2010; 65: 417.
Prior S, Heaton J, Jatana KR, Rashid RG. Parker Flex-Tip and standard-tip endotracheal tubes: a comparison during nasotracheal intubation. Anesth Prog 2010; 57: 18-24.
Acknowledgement
The authors sincerely thank Tomofumi Hamada DDS, PhD, (Research Associate, Department of Oral Surgery, Kagoshima University Medical and Dental Hospital, Kagoshima, Japan) for help with the statistical analyses.
Funding
Financial support was provided solely by institutional sources.
Conflicts of interest
None declared.
Author information
Authors and Affiliations
Corresponding author
Additional information
Author contributions
Kazuna Sugiyama contributed to the conception and design of the study, conducted the study as leader, analyzed the data, and wrote and revised the manuscript. Yozo Manabe and Atsushi Kohjitani helped conduct the study, critically revised the article, and helped revise the manuscript. Yozo Manabe contributed to the acquisition and statistical analysis of the data. Kazuna Sugiyama and Atsushi Kohjitani reviewed the analysis of the data.
Rights and permissions
About this article
Cite this article
Sugiyama, K., Manabe, Y. & Kohjitani, A. A styletted tracheal tube with a posterior-facing bevel reduces epistaxis during nasal intubation: a randomized trial. Can J Anesth/J Can Anesth 61, 417–422 (2014). https://doi.org/10.1007/s12630-014-0156-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-014-0156-3