
Summary
Purpose
In 1978, Drs. R Knill and A. Gelb published the results of a study to measure the effect of subanesthetic levels of halothane on the ability of fit volunteers to respond to sustained hypoxia, and to determine how long potentially hazardous levels of halothane persist after a brief non-complex surgical procedure in healthy patients. The purpose of this commentary is to highlight the historical context of their findings and the impact of their work on our modern day practice of anesthesia.
Principal findings
In six fit male volunteers, steady states of halothane reduced the ventilatory response to normocapnic hypoxemia (PETO2 40 mmHg) by ~ 50% at 0.05 MAC and by 70% at 0.10 MAC without affecting resting levels of ventilation. Subjects remained easily rousable and coherent with full memory of events. Symptoms of hypoxemia were markedly reduced or totally absent during hypoxic periods. In five patients recovering from dental procedures (mean duration 59 min), 0.10 MAC halothane levels persisted in the recovery room for approximately one hour.
Conclusions
Patients emerging from a brief (about one hour) halothane anesthetic, although appearing conscious, may have a hazardous degree of depression of the usually protective ventilatory response to hypoxemia for about one hour in the recovery room. Both the symptoms and signs of hypoxemia will be substantially reduced during this emergence phase, enhancing the risk that severe hypoxic episodes may go unrecognized.
Authors
Gelb AW, Knill RL.
Citation
Subanaesthetic halothane: Its effect on regulation of ventilation and relevance to the recovery room. Can Anaesth Soc J 1978; 25: 488-94.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Commentary
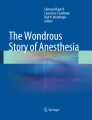
All high-impact research starts with a novel question that is important if proven true. The seminal article reviewed here arose from a challenge of the (then) commonly accepted view that our anesthetic agents were all safely out of the patient’s system by the time they appeared ready to leave the watchful context of the postanesthesia care unit. Following their observation of substantial depression of the compensatory ventilatory response to acute hypoxia in normal volunteers breathing subanesthetic concentrations of halothane,1 Drs. R. Knill and A. Gelb crafted a carefully designed study (reviewed here) to examine the response to sustained hypoxia, not just in healthy volunteers but in patients within the recovery room of an academic health sciences centre. They observed that levels of halothane that produce profound depression of this major protective compensatory mechanism persisted in patients for up to one hour following a one-hour halothane anesthetic, despite the patients’ apparent wakefulness (Figure).

Graph of the relative depression of three measures of ventilatory control at four concentrations of halothane. Zero depression indicates a response equal to the conscious state. 100% depression is a total absence of reflex compensation. Both baseline isocapnic ventilation and the ventilatory response to hypercapnea were minimally depressed at subanesthetic concentrations of halothane, being 50-75% depressed only at surgical depths of anesthesia. In sharp contrast, the ventilatory response to hypoxemia proved surprisingly sensitive, being ~ 50% depressed by 0.05 MAC halothane, ~ 70% depressed by 0.1 MAC halothane, and totally abolished at anesthetic concentrations. Levels of 0.1 MAC halothane persisted for about an hour after emergence from a brief one-hour halothane anesthetic. Reproduced with permission from Gelb AW, Knill RL. Subanaesthetic halothane: its effect on regulation of ventilation and relevance to the recovery room. Can Anaesth Soc J 1978; 25: 488-94
To appreciate the radical nature of this article and its clinical importance, one has to remember that, at the time of this investigation, pulse oximetry was unavailable in both the operating and recovery rooms of even the best-equipped centres. Up to that point, the carotid body receptors and their reflex pathways had been viewed as extremely rugged and labelled the “ultimum moriens” – the last to die. If the patient was responsive and coherent, it was generally expected that s/he would respond as needed to any episode of hypoxemia that might occur. This paper raised a red flag, warning us that patients with a PETO2 of 40 mmHg can have markedly reduced responses to sustained hypoxia for up to an hour after a brief halothane anesthetic without exhibiting symptoms. These data triggered a new era of investigation into factors impacting patient safety in the postoperative period.
Further studies examined the impact of both thiopentone2 and enflurane3 at anesthetic and subanesthetic doses. Dr. Knill then checked to see if painful stimuli reversed the observed depression of these crucial protective chemoreflexes. They didn’t.4
After finding similar depression of the ventilatory response to hypoxia with isoflurane,5 Dr. Knill moved on to investigate other factors that might also be impaired in that early postoperative period. The response both to acidemia and to the normal interaction of acidemia and hypoxemia were shown to be cut in half by residual 0.1% halothane and essentially abolished by light 1.0% concentrations. In short, the patient’s ability to compensate for any and all causes of acidemia that might occur (such as in patients with impaired renal function) became dangerously impaired.6
The potential impact of these seminal studies was initially recognized more by Dr. Knill than by the rest of the anesthesia research community. Dr. Knill went on to examine the time-course of respiratory depression associated with emerging postoperative pain control modalities (i.e., epidural morphine vs fentanyl)7 and to investigate postoperative sleep disturbances.8 In 1990, Dr. Knill challenged anesthesiologists to recognize that intense research activity over several decades had generated a wealth of information about the genesis and management of anesthesia-related complications during and immediately following anesthesia, while little effort was being invested in determining whether our anesthetics may be contributing to postoperative complications such as atelectasis, pneumonia, stroke, delirium, or myocardial infarction. All these complications were well-recognized to occur postoperatively, but neither surgeons nor anesthetists tended to view them as “their problem”, and as such, they had “fallen through the cracks” of academe. Dr. Knill challenged us to regard patient safety in the postoperative period as an issue for which we as anesthesiologists must take some responsibility.9
Dr. Knill’s published abstracts over the next five years reflect his concern for patient safety during the first postoperative week. He probed the relationship of sleep disturbances, hemodynamic instability, urine catecholamines, rises in myocardial enzymes, pain control methodologies, and the occurrence of delirium, as well as critical events in the recovery room. Dr. Knill’s sudden death in 1995 prevented many of the abstracts from maturing into full publications, but they did lay the groundwork for investigations by others. For example, by 1996, Dr. Georgiou et al. investigated whether the incidence and severity of postoperative hypoxemia during the first three nights following surgery could be decreased by using a total intravenous anesthesia technique instead of a volatile agent plus nitrous oxide.10
Indeed, intense research activity followed Dr. Knill’s 1978 article. Differences emerged among volatile agents, the biochemical basis of depression of the carotid body hypoxemic response was pursued, and the influence of wakefulness and/or variations of CO2 on the depressive effect of volatile agents on the body’s response to hypoxemia were investigated and reviewed, with both peripheral (carotid bodies) and central sites proving to be involved in the depression of the hypoxic ventilatory response by volatile anesthetic agents.11 Controversies were aired12 (and rebutted). The summative message became clear, i.e., unrecognized unanticipated hypoxemia can put patients at risk both in the recovery room and on the wards postoperatively. The contributing factors are multiple and vary unpredictably from patient to patient. It was about this time that pulse oximetry became a practical tool for the operating room, to be followed by the recovery room and other higher-intensity care areas in our hospitals. Throughout the 1980s, oximeters were large, clumsy, and prohibitively expensive tools for the pulmonary function laboratory and research labs. Part of Dr. Knill’s research legacy was his initiation of a line of investigation that increased our awareness of the widespread need for such a monitor outside our operating rooms.
The next field to reflect our dawning concern with the possible postoperative effects of our anesthetics was that of obstructive sleep apnea. Although the features of obstructive sleep apnea were described quite accurately by writers such as Shakespeare, the first medical description did not appear until 1966. It is no surprise that Dr. Knill’s 1978 paper plus four of his further investigations are referenced in Loadsman and Hillman’s 2001 review of anesthesia and sleep apnea,13 and his work continues to be viewed as foundational to our understanding of postoperative patient vulnerabilities.14,15 Currently, further sites of surprisingly delayed elimination of isoflurane have been identified in the mouse hippocampus for up to 24 hr.16 Whether the short-term memory impairment demonstrable at 24 hr has resulted from high intraoperative concentrations or whether trace amounts continue to impair brain function once neurons have been primed by higher levels requires further study. In any case, it is clear that the impact of our anesthetic agents persist long after apparent “emergence”.
The progressive extension of the Canadian Anesthesiologists’ Society motto –We watch closely those who sleep – into the postoperative period is a legacy of Drs. Gelb and Knill’s 1978 investigation and the subsequent research it triggered. It is part of the reason our departments now have names such as “Anesthesiology and Perioperative Medicine”, and our responsibility to our patients isn’t over at the end of our operating room list.
Key points
-
Patients emerging from a brief (about one hour) halothane anesthetic, although appearing conscious, may have a hazardous degree of depression of the usually protective ventilatory response to hypoxemia for about one hour in the recovery room.
-
Both the symptoms and signs of hypoxemia will be substantially reduced during the emergence phase, enhancing the risk that severe hypoxic episodes may go unrecognized.
-
Painful stimuli do not reverse the observed depression of these crucial protective chemoreflexes.
-
Unanticipated hypoxemia can put patients at risk both in the recovery room and on the wards postoperatively. The contributing factors are multiple, variable, and unpredictable from patient to patient.
References
Knill RL, Gelb AW. Ventilatory responses to hypoxia and hypercapnia during halothane sedation and anesthesia in man. Anesthesiology 1978; 49: 244-51.
Knill RL, Bright S, Manninen P. Hypoxic ventilatory responses during thiopentone sedation and anaesthesia in man. Can Anaesth Soc J 1978; 25: 366-72.
Knill RL, Manninen PH, Clement JL. Ventilation and chemoreflexes during enflurane sedation and anaesthesia in man. Can Anaesth Soc J 1979; 26: 353-60.
Lam AM, Clement JL, Knill RL. Surgical stimulation does not enhance ventilatory chemoreflexes during enflurane anaesthesia in man. Can Anaesth Soc J 1980; 27: 22-8.
Knill RL, Kieraszewicz HT, Dodgson BG, Clement JL. Chemical regulation of ventilation during isoflurane sedation and anaesthesia in humans. Can Anaesth Soc J 1983; 30: 607-14.
Knill RL, Clement JL. Ventilatory responses to acute metabolic acidemia in humans awake, sedated, and anesthetized with halothane. Anesthesiology 1985; 62: 745-53.
Knill RL, Clement JL, Thompson WR. Epidural morphine causes delayed and prolonged ventilatory depression. Can Anaesth Soc J 1981; 28: 537-43.
Knill RL, Moote CA, Skinner MI, Rose EA. Anesthesia with abdominal surgery leads to intense REM sleep during the first postoperative week. Anesthesiology 1990; 73: 52-61.
Knill RL. Clinical research in anaesthesia. Past accomplishments and a future horizon. Anaesthesia 1990; 45: 271-2.
Georgiou LG, Vourlioti AN, Kremastinou FI, Stefanou PS, Tsiotou AG, Kokkinou MD. Influence of anesthetic technique on early postoperative hypoxemia. Acta Anaesthesiol Scand 1996; 40: 75-80.
van den Elsen M, Sarton E, Teppema L, Berkenbosch A, Dahan A. Influence of 0.1 minimum alveolar concentration of sevoflurane, desflurane and isoflurane on dynamic ventilatory response to hypercapnia in humans. Br J Anaesth 1998; 80: 174-82.
Robotham JL. Do low-dose inhalational anesthetic agents alter ventilatory control? Anesthesiology 1994; 80: 723-6.
Loadsman JA, Hillman DR. Anaesthesia and sleep apnoea. Br J Anaesth 2001; 86: 254-66.
Chung SA, Yuan H, Chung F. A systemic review of obstructive sleep apnea and its implications for anesthesiologists. Anesth Analg 2008; 107: 1543-63.
Kaye AD, Hollon MM, Vadivelu N, et al. Postoperative apnea, respiratory strategies, and pathogenesis mechanisms: a review. J Anesth 2013; 27: 423-32.
Saab BJ, Maclean AJ, Kanisek M, et al. Short-term memory impairment after isoflurane in mice is prevented by the α5 γ-aminobutyric acid type A receptor inverse agonist L-655,708. Anesthesiology 2010; 113: 1061-71.
Funding sources
None.
Conflicts of interest
None declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Froese, A.B. From the Journal archives: Be alert to the risk of unexpected prolonged postoperative hypoxemia!. Can J Anesth/J Can Anesth 61, 379–382 (2014). https://doi.org/10.1007/s12630-013-0095-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-013-0095-4