
Abstract
Objective
Older adults are an increasing proportion of patients admitted to trauma services. Trauma in older adults’ results from many mechanisms of injury with the distribution of mechanisms of injury among older adults different than those of younger adults. The acute management of these injuries may determine the patients’ ability to return to independent living. It is known that prolonged immobilization of older patients results in deterioration of their functional status and increases the likelihood of hospital acquired complications, notably pneumonia, delirium, and loss of ambulation.
Design/Setting
We reviewed 213 patients aged 65 and older admitted to our trauma services who sustained cervical spine injuries that were either placed in c spine immobilization or were not to understand the outcomes associated with their mechanism of injury.
Results
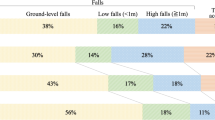
The youngest patients (65–74 years) were proportionately more likely to have sustained high energy injuries associated with motor vehicle crashes (36%) with a mortality rate of 11.5%. The oldest age group (> 85 years) had a higher mortality rate from falls from standing injuries (31%). Patients discharged with a collar were more likely to return to independent living. In addition, 96% of the patients that died in the acute care setting were not in cervical collar immobilization.
Conclusion
Patients under 85 years with a cervical spine injury should be placed in c-spine immobilization and aggressively managed with a multidisciplinary team approach. The older adult trauma population requires specialty care including rapid cervical spine evaluation and prescreening of functional status on admission. The NEXUS guideline should be enhanced for the older adult trauma population.
Similar content being viewed by others


References
Cohen, J.E., Human Population: The Next Half Century. Science, 2003. 302(5648): p. 1172–1175.
Colby, S.L. and J.M. Ortman, Projections of the size and composition of the US population: 2014 to 2060.
Spaniolas, K., et al., Ground level falls are associated with significant mortality in elderly patients. Journal of Trauma and Acute Care Surgery, 2010. 69(4): p. 821–825.
Brown, C.V.R., et al., A Comprehensive Investigation of Comorbidities, Mechanisms, Injury Patterns, and Outcomes in Older adult Blunt Trauma Patients. The American Surgeon, 2016. 82(11): p. 1055–1062.
Cooper, Z., et al., Mortality and Readmission After Cervical Fracture from a Fall in Older Adults: Comparison with Hip Fracture Using National Medicare Data. Journal of the American Older adults Society, 2015. 63(10): p. 2036–2042.
Jawa, R.S., et al., Spinal Fractures in Older Adult Patients Admitted After Low-Level Falls: 10-Year Incidence and Outcomes. Journal of the American Older adults Society, 2016: p. n/a-n/a.
Hanigan, W.C., et al., Odontoid fractures in elderly patients. Journal of Neurosurgery, 1993. 78(1): p. 32–35.
Moran, C., et al., Understanding post-hospital morbidity associated with immobilization of cervical spine fractures in older people using older adult medicine assessment techniques: A pilot study. Injury, 2013. 44(12): p. 1838–42.
Majercik, S., et al., Halo Vest Immobilization in the Elderly: A Death Sentence? The Journal of Trauma: Injury, Infection, and Critical Care, 2005. 59(2): p. 350–357.
Polin, R.S., et al., Nonoperative Management of Types II and III Odontoid Fractures: The Philadelphia Collar versus the Halo Vest. Neurosurgery, 1996. 38(3): p. 450–457.
Tashjian, R.Z., et al., Halo-vest immobilization increases early morbidity and mortality in elderly odontoid fractures. Journal of Trauma and Acute Care Surgery, 2006. 60(1): p. 199–203.
Committee, P.A., <Guidelines for Treatment of the Cervical Spine, eff 08-15-2009. pdf>. 2009. 8/15/2009.
Wilson, M.S., et al., Early predictors of mortality in older adult patients with trauma. Journal of orthopedic trauma, 2016. 30(9): p. e299–e304.
Perdue, P.W., et al., Differences in Mortality between Elderly and Younger Adult Trauma Patients: Older adult Status Increases Risk of Delayed Death. Journal of Trauma and Acute Care Surgery, 1998. 45(4): p. 805–810.
Morris, J.A., et al., Mortality in trauma patients: the interaction between host factors and severity. Journal of Trauma and Acute Care Surgery, 1990. 30(12): p. 1476–1482.
Hashmi, A., et al., Predictors of mortality in older adult trauma patients: a systematic review and meta-analysis. Journal of Trauma and Acute Care Surgery, 2014. 76(3): p. 894–901.
Friese, R.S., et al., Age and mortality after injury: is the association linear? European journal of trauma and emergency surgery, 2014. 40(5): p. 567–572.
Hollis, S., et al., The effect of pre-existing medical conditions and age on mortality after injury. Journal of Trauma and Acute Care Surgery, 2006. 61(5): p. 1255–1260.
Joseph, B., et al., Superiority of frailty over age in predicting outcomes among older adult trauma patients: a prospective analysis. JAMA surgery, 2014. 149(8): p. 766–772.
Kizilarshanoglu, M.C. et al., Is frailty a prognostic factor for critically ill elderly patients? Aging Clin Exp Res, 2017. 29: p. 247–255.
Jorgensen, R. and Brabrand, M, Screening of the frail patient in the emergency department: A systematic review. European Journal of Internal Medicine, 2017. 45: p. 71–73.
Lewis, E.T., et al., Which frailty scale for patients admitted via Emergency Department? A cohort study. Archives of Gerontology and Older adults, 2019. 80: p. 104–114.
MILZMAN, D.P., et al., Pre-existing Disease in Trauma Patients: A Predictor of Fate Independent of Age and Injury Severity Score. Journal of Trauma and Acute Care Surgery, 1992. 32(2): p. 236–244.
Grossman, M.D., et al., When is an elder old? Effect of preexisting conditions on mortality in older adult trauma. Journal of Trauma and Acute Care Surgery, 2002. 52(2): p. 242–246.
Copes, W.S., et al., The Injury Severity Score revisited. Journal of Trauma and Acute Care Surgery, 1988. 28(1): p. 69–77.
Yousefzadeh-chabok, S., et al., Comparison of Revised Trauma Score, Injury Severity Score and Trauma and Injury Severity Score for mortality prediction in elderly trauma patients. Ulus Travma Acil Cerrahi Derg, 2016. 22(6): p. 536–540.
Hoffman, J.R., et al., Validity of a Set of Clinical Criteria to Rule Out Injury to the Cervical Spine in Patients with Blunt Trauma. New England Journal of Medicine, 2000. 343(2): p. 94–99.
Blackham, J. & Benger, J. (2009). “Clearing” the cervical spine in conscious trauma patients. Trauma, 11 (2), 93–109.
Paykin, G., O’Reilly, G., Ackland, H.M., & Mitra, B. (2017). The NEXUS criteria are insufficient to exclude cervical spine fractures in older blunt trauma patients. Injury, 4(5), 1020–1024.
Mekata, K., et al., Cervical spine motion during swallowing. European Spine Journal, 2013. 22(11): p. 2558–2563.
Stambolis, V., et al., The Effects of Cervical Bracing Upon Swallowing in Young, Normal, Healthy Volunteers. Dysphagia, 2003. 18(1): p. 39–45.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest: The authors declare no conflict of interest. No funding was received for the research involved in the manuscript.
Ethical standard: This study was guided by the Saint Louis University Institutional Review Board#28203 following the ethical principles regarding all research involving humans as subjects, as set forth in the Ethical Principles and Guidelines for the Protection of Human Subjects of Reserach.
Rights and permissions
About this article

Cite this article
Moran, V., Pulliam, T., Rodin, M. et al. Cervical Injury Outcomes among Older Adults Admitted to an Inpatient Trauma Service. J Nutr Health Aging 25, 392–398 (2021). https://doi.org/10.1007/s12603-021-1589-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12603-021-1589-3