
Abstract
We investigated differences in sex responses in serum CK activity and renal function measured by glomerular filtration rate (GFR) after an exercise session. Twenty-two healthy and trained volunteers (11 males and 11 females) performed 17 resistance exercises with 3 × 12 repetitions in a circuit training fashion. Subjects provided blood samples prior to exercise session, and at 24, 48, and 72 h following exercise sessions for creatine kinase and creatinine. Twenty-four-hour urine samples were collected before and 72 h after the exercise. Estimate (e) GFR was obtained by using the Chronic Kidney Disease Epidemiology Collaboration equation adjusted for males and females. After the exercise session, males showed greater serum CK activity than females (p < 0.02), serum creatinine increased 31.3 % for males and 29.8 % for females, and urinary creatinine decreased on average 5.4 % for males and 0.6 % for females, with no significant differences (p > 0.05) between sex for serum and urinary creatinine. eGFR decreased significantly for males (~10 %) and females (~8 %), but also without a difference between the sexes (p > 0.05). The correlation between CK and eGFR was significant for males (r = −0.794; p = 0.003), and females (r = −0.8875; p < 0.001). A significant negative correlation between CK activity and the eGFR indice of renal function in both males and females was observed. Additionally, the renal function compromise was similar for both sexes, despite males presenting greater exercise-induced skeletal muscle damage when compared to females.
Similar content being viewed by others


Introduction
Exercise-induced muscle damage (EIMD) is evident from increased blood levels of muscle proteins such as creatine kinase (CK), lactate dehydrogenase (LDH), and myoglobin [1, 2]. Serum CK is cleared from the blood by the reticuloendothelial system, and myoglobin is cleared by the kidneys. This latter phenomenon can result in myoglobinuria which can cause damage to the kidney tubules, potentially resulting in acute renal failure especially in environmental conditions of heat stress and dehydration [1–3]. Furthermore, excessive muscle damage from physical activity can lead to renal failure, a clinical condition that has been termed exertional rhabdomyolysis (ERB) [2].
Serum CK activity has been studied extensively and is considered a qualitative marker for skeletal muscle damage [4–8]. Clarkson et al. [9] showed a strong correlation (r = 0.80, n = 203) between serum CK activity and serum myoglobin concentration after a damaging exercise session, but these findings indicated no compromise in renal function. These authors assessed renal function indirectly by measuring serum creatinine, blood urea nitrogen, potassium, osmolality, phosphorus, and uric acid, but did not assess the glomerular filtration rate (GFR).
GFR is considered the single best overall index of kidney function, and it is recommended for diagnosis and monitoring of kidney disease. This parameter can be obtained through estimation (e) by various formulas (eGFR) or through the measurement of creatinine clearance (Ccr), although use of Ccr has not been shown to improve the assessment of GFR over that provided by prediction equations [10, 11]. The change in GFR is important because, in a clinical setting, it is used to define a possible kidney compromise. For example, a decrease of ~50 % in GFR (<60 mL min−1) is considered evidence of kidney compromise, as in cases of ERB, and a decrease of 75 % is indicative of renal impairment [12].
Research findings suggest GFR may be a more sensitive indicator of potential renal problems after strenuous exercise which results in large increase of CK and myoglobin in the bloodstream. Specifically, Machado et al. [13] verified in active (non-athlete) females a strong and significant correlation between serum CK activity and eGRF variation (measured by four different formulas and creatinine clearance) after a strenuous workout. Colombini et al. [14] studied male professional cyclists during the Giro d’ Italia 3-week stage race and verified similar results [eGFR assessed by Chronic Kidney Disease Epidemiology Collaboration equation (CDK-EPI)].
As researchers, however, we are not aware of any study that has investigated the relationship between CK and eGFR according to the subject sex under controlled exercise conditions, which should be examined because of the previous reports about the protective effect of estrogen [15] against EIMD and inflammation [16–19], and about sex differences in renal hemodynamics [20]. Thus, the aim of this study was to investigate sex differences in serum CK activity and renal function after a resistance exercise session. We hypothesized that there would be a significant correlation between CK and eGFR whereby high post-exercise serum CK activity would be associated with greater decreases in eGFR in both males and females, but with a major impact in males.
Materials and methods
Subjects
Twenty-two trained subjects [11 males (age = 25 ± 3 years; height = 174 ± 4 cm; mass = 76.2 ± 4.4 kg) and 11 females (age = 27 ± 4 years; height = 160 ± 3 cm; mass 59.8 ± 7.3 kg)] volunteered to participate in the current study. To calculate the sample size, we used previously reported differences in eGFR between prior to and after 72 h of resistance exercise sessions [13, 14]. We calculated that 11 pairs of subjects were needed to detect this association with 2-tailed α = 0.05 and 1-β = 0.90. All subjects were healthy (i.e., no muscle, cardiovascular, or joint problems) and were not using ergogenic substances or any other drugs. Subjects underwent a physical examination by a physician and were further screened for any medications that might affect muscle damage or renal function. Subjects were excluded if they had a history or presence of muscle disease, diabetes mellitus, hypertension, or hyperthyroidism. All subjects had been participating in a structured training program (in the same fitness classes) for a minimum of 12 months with a mean frequency of three sessions per week. We utilized exercise-trained subjects because we wanted to simulate a “real life” situation which might occur when trained individuals perform unaccustomed strenuous exercise. The purpose and procedures were explained to the subjects and informed consent was obtained according to the Declaration of Helsinki and in accordance with the norms of the local Research Committee.
Experimental protocol
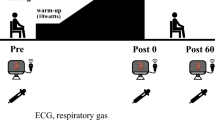
All subjects performed a 60-min resistance exercise session with 17 standardized exercises (Leg Press 45; Glut Kickback on Swiss Ball; Bench Press; One-legged Cable Kickback; Lunges; Cable Let pull down; Push Ups; Leg Curl; Fly; Pec Deck Fly; Pull over; Lever Seated Hip Abduction; Straight Led Deadlift; Cable Lateral Raise; Standing Calf Raise; Seated Calf Raise; Seated Biceps Curl). Standard exercise techniques were followed for each exercise [21]. All exercises were performed with 3 sets of 12 repetitions with personal choices in loading and in a circuit training fashion (with minimum rest intervals, <15 s). Each exercise set was composed of 12 complete movements (repetitions) of each exercise; an exercise “circuit” was one completion of all prescribed exercises in the program. When one circuit was completed, a subject then began the first exercise again for another circuit (3 circuits in total). The subjects had experience with performing these exercises and with the structured training program, but had never performed them with such short rest intervals between the exercises (i.e., <15 s). The short intervals between exercises were used to increase the magnitude of muscular stress and potential damage [22]. A Borg-CR10 rating of perceived effort [23] was used to check the effort made by subjects at the end of each circuit. The environmental conditions were verified and maintained constant throughout the exercise session (25 ± 1 °C and 70 ± 0 % relative air humidity). The subjects did not perform exercises for 96 h after the experimental session.
Blood collection and analysis
Subjects provided blood samples in a seated position from an antecubital vein via venipuncture in using serum tubes after 8 h overnight fast prior to the exercise session (PRE), and at 24, 48, and 72 h following the exercise session. Samples were allowed to clot for 30 min, and then centrifuged at 1,600g for 10 min. The serum was removed, and the serum CK activity was analyzed with an enzymatic method at 37 °C (CK-UV NAC-optimized; Biodiagnostica, Pinhais, Brazil) in a Cobas Mira Plus analyzer (Roche, Basel, Switzerland). Serum creatinine was measured with colorimetric assay (Biodiagnostica). The CK and creatinine analyses were made in triplicate and demonstrated high reliability (intraclass R = 0.89, 0.85, respectively). The coefficient of variation of the creatinine and CK assays were <3 %.
Urine collection and analysis
Before the exercise session, a 24-h urine sample was collected in 1,000-mL purpose-bottles. Bottles were kept cold during the collection period. Immediately after the return of the bottles, 50 mL of each whole urine sample were collected and stored at −70 °C before analysis for creatinine and uric acid. The same procedure (urine sample collection) was made 72 h after the first collection. Urinary creatinine and uric acid were determined by a validated automated colorimetric assay on a diagnostic auto-analyzer (Cobas Mira Plus analyzer; Roche, Germany).
Estimated Glomerular Filtration Rate (eGFR) was obtained by use of the Chronic Kidney Disease Epidemiology Collaboration equation (CDK-EPI) [eGFR = 144 × (0.993)Age × (Serum Creatinine (Scr)/0.7)−0.329 for female; eGFR = 141 × (0.993)Age × (Scr/0.9)−0.411 for male].
Statistical analyses
The difference between baseline serum CK and peak CK (at 48 or 72 h) was calculated (i.e., delta CK) and considered the principle outcome measure. To analyze the relationship between exercise-induced serum CK variations and eGFR, a linear regression bivariate analysis was applied and Spearman’s rank correlation coefficient (i.e., Spearman’s rho coefficient) and its respective p value was obtained. Spearman’s rank correlation coefficient was chosen because it is more appropriate to small sample size (10–100 samples) [24]. To compare serum CK activity over time, a 2 (sex) × 4 (sampling times) repeated ANOVA was utilized. Significant ANOVA results were followed by appropriate post hoc tests with Bonferroni corrections. Pre- versus post-blood and urinary creatinine, eGFR and urinary uric acid (UUA) were compared with a Student’s t test. The alpha level was set at <0.05 for a difference to be considered significant. Statistical analysis was completed using SPSS® 17.0 for Windows (LEAD Technologies, USA).
Results
The baselines of urinary and serum parameters are shown in Table 1.
Serum CK activity demonstrated a significant main effect for sex (p < 0.001) and for time (p < 0.001). Peak CK activity was significantly (t = −2.2; p = 0.018) greater in males (1142.8 ± 596.7 U L−1) than females (587.3 ± 566.7 U L−1), reaching its highest point 48 h following exercise. Figure 1 displays the serum CK activity following the exercise session in males and females.

Serum CK activity (mean ± SE) from females and males before and 24, 48 and 72 h after the exercise session. Asterisk 2 (sex) × 4 (sampling times) repeated ANOVA significant difference between women and men (p < 0.05)
The rating of perceived exertion increased significantly throughout the exercise (p < 0.01), but it was not different between the males and females (females: 6.1 ± 0.7, 6.5 ± 0.5, and 7.0 ± 0.0; Males: 5.5 ± 0.9, 6.1 ± 1.0, and 6.5 ± 0.9 Borg units after the first, second, and third circuits, respectively).
Indices of renal function changed after the exercise. For males and females, serum creatinine 72 h after the exercise session increased by 31.1 ± 21.3 % (p < 0.001) and 29.8 ± 13.9 % (p = 0.001), respectively, but without a difference between the sexes. UUA also increased by 34 ± 28.1 % (p < 0.02) and 24 ± 30.2 % (p < 0.02) after the exercise session for the males and females, respectively, but without a difference between the sexes. There was no observed significant time effect (i.e., pre- vs. 72 h measures) or sex differences in urinary creatinine (p = 0.249 for males and p = 0.374 for females) (Fig. 2). eGFR decreased in both sexes (10.0 ± 5.6 % for males, p < 0.001; and 7.9 ± 3.2 % for females, p < 0.001), but without significant differences between them (p > 0.05).

Percent change from baseline of serum (SCrn) and urinary creatinine (UCrn), urinary uric acid (UUA), and Estimated Glomerular Filtration Rate (eGFR) (mean ± SE) for males and females. Asterisk denotes a significant difference from baseline (p < 0.05)
Figure 3 shows the correlation relationship between the change in delta eGFR and the delta serum CK in both sexes (males n = 11; females n = 11). The Spearman’s rho coefficients were significant for males (r = −0.782; p = 0.004), and females (r = −0.745; p = 0.008).

Correlation between delta Serum CK activity and delta eGFR for females (black) and males (gray)
Discussion
This study showed a significant relationship between serum CK activity and the eGFR after strenuous exercise in male and female subjects. Additionally, we found that males showed a greater serum CK activity after exercise than females, but both sexes showed similar renal function decreases after exercise.
Sex influences on EIMD
Numerous studies have reported that estrogens may diminish exercise-induced muscle damage and inflammation [16–18, 25, 26]. This prophylactic effect is also reported to occur in other tissues such as cardiac muscle, liver, and nervous tissue [16, 25, 26], and have been attributed to the antioxidant and membrane stabiliser properties from estrogens [27]. Our results corroborate these previous findings, since our females showed lower serum CK activity following a damaging exercise, which is indicative of diminished EIMD.
Despite being a potential source of difference in the degree of serum CK activity, the greater muscle mass exhibited by males appears not to have been a source of any difference found, since no sex differences in serum CK activity were observed at the baseline measure. This is in accordance with Swaminathan et al. [28] who provided evidence that the lean body mass (i.e., major constituent is muscle) is not a major determinant of serum CK activity in healthy subjects.
Sex and renal function decreases after EIMD
Previous studies have shown that major increases in CK activity are associated with altered renal function by actions of myoglobin, which increases similarly to CK in the blood [1, 9]. For example, Clarkson et al. [9] reported a strong correlation between the increase of CK and myoglobin after unilateral eccentric elbow flexion exercise (i.e., 2 sets of 12 repetitions of biceps brachii lengthening contraction). However, despite the dramatic increases in CK and myoglobin (up to 80,550 U/L and 2,300 μg/L, respectively), these increases were not accompanied by serum creatinine elevation. In the present study, although the concentration of urinary creatinine did not demonstrate significant alterations, serum creatinine was increased significantly (~25 %). When we analyzed the eGFR (calculated using the serum creatinine), we found a significant reduction after the damaging resistance exercise. According to the “Clinical Practice Guidelines for Chronic Kidney Disease” [12], eGFR is a sensitive indicator of the filtration capacity of the kidneys and is a strong predictor of the time to onset of kidney failure as well as the risk of complications of chronic kidney disease. There was a reduction in eGFR calculated by the CDK-EPI equation, but it did not achieve values that were evidence of a kidney impairment (i.e., <60 mL min−1) [12]. The reduction in the values of eGFR appear to be due to a greater baseline eGFR found in trained individuals, as described in Lippi et al. [29]. Although the decrease we detected did not indicate a compromise in renal function, it may become clinically significant if this exercise activity is performed in a hot, humid environment and/or a person is somewhat dehydrated [1–3].
Machado et al. [13] showed a significant association between changes in serum CK activity and renal function after resistance exercise in females. Similar results were shown by Colombini et al. [14] studying males during the Giro d’ Italia 3-week stage race (21–22 days with more than 3,000 km covered and only 1 or 2 days of rest; athletes are submitted to very intense exercise effort, combining aerobic and anaerobic metabolism (particularly during mountain stages and time trials), but direct comparisons between these and the present study can not be made owing to the methodological differences that exist (i.e., differences in exercise features).
To the authors’ knowledge, the influence of sex on the relationship between CK and eGFR has not been reported in the literature, and so this is the first report on this topic. Our data clearly showed a relationship between CK elevation and reduced eGFR after physical exercise for both sexes. Moreover, despite the presence of higher serum CK activity after exercise, males showed similar eGFR decreases when compared to females. These findings provide some evidence that a different adaptive response to resistance exercise for males and females may exist, and paves the way for further studies aiming to identify the cellular–molecular features involved in this event.
References
Skenderi KP, Kavouras SA, Anastasiou CA, Yiannakouris N, Matalas A (2006) Exertional rhabdomyolysis during a 246 km continuous running race. Med Sci Sports Exerc 38:1054–1057
Warren JD, Blumbergs PC, Thompson PD (2006) Rhabdomyolysis: a review. Musc Ner 25:332–347
Ohta T, Sakano T, Igarashi T, Itami N, Ogawa T (2004) Exercise-induced acute renal failure associated with renal hypouricaemia: results of a questionnaire-based survey in Japan. Nephrol Dial Transpl 19:1447–1453
Stupka N, Lowther S, Chorneyko K, Bourgeois JM, Hogben C, Tarnopolsky MA (2000) Gender differences in muscle inflammation after eccentric exercise. J Appl Physiol 89:2325–2332
Chen TC, Hsieh SS (2001) Effects of a 7 day eccentric training period on muscle damage and inflammation. Med Sci Sports Exerc 33:1732–1738
Clarkson PM, Hoffman EP, Zambraski E, Gordish-Dressman H, Kearns A, Hubal M, Harmon B, Devaney JM (2005) ACTN3 and MLCK genotype associations with exertional muscle damage. J Appl Physiol 99:564–569
Clarkson PM, Hubal MJ (2002) Exercise-induced muscle damage in humans. Am J Phys Med Rehabil 81:S52–S69
Nosaka K, Newton M, Sacco P (2002) Muscle damage and soreness after endurance exercise of the elbow flexors. Med Sci Sports Exerc 34:920–927
Clarkson PM, Kearns AK, Rouzier P, Rubin R, Thompson PD (2006) Serum creatine kinase levels and renal function measures in exertional muscle damage. Med Sci Sports Exerc 38:623–627
Sokoll LJ, Russell RM, Sadowski JA, Morrow FD (1994) Establishment of creatinine clearance reference values for older women. Clin Chem 40:2276–2281
Myers GL, Miller WG, Coresh J, Fleming J, Greenberg N, Greene T, Hostetter T, Levey AS, Panteghini M, Welch M, Eckfeldt JH (2006) Recommendations for improving serum creatinine measurement: a report from the laboratory working group of the national kidney disease education program. Clin Chem 52:5–18
National Kidney Foundation-Kidney Disease Outcomes Quality Initiative (2000) Clinical practice guidelines for nutrition in chronic renal failure. Am J Kidney Dis 35:S1–S140
Machado M, Zini EN, Valadão SN, Amorim MZ, Barroso TZ, Oliveira W (2012) Relationship of glomerular filtration rate and serum CK activity after resistance exercise in women. Int Urol Nephrol 44:515–521
Colombini A, Corsetti R, Machado M, Graziani R, Lombardi G, Lanteri P, Banfi G (2012) Serum creatine kinase activity and its relationship with indices of renal function in professional cyclists during the giro d’ Italia 3 weeks stage race. Clin J Sports Med 22:408–413
Hatae J, Takami N, Lin H, Honda A, Inoue R (2009) 17beta-estradiol-induced enhancement of estrogen receptor biosynthesis via MAPK pathway in mouse skeletal muscle myoblasts. J Physiol Sci 59:181–190
Tiidus PM (1995) Can estrogens diminish exercise induced muscle damage? Can J App Physiol 20:26–38
Komulainen J, Koskinen SOA, Kalliokoski R, Takala TES, Vihko V (1999) Gender differences in skeletal muscle fibre damage after eccentrically biased downhill running in rats. Acta Physiol Scand 165:57–63
Tiidus PM (2011) Influence of estrogen on muscle plasticity. Braz J Biomot 4:143–155
Carter A, Dobridge J, Hackney AC (2001) Influence of estrogen on markers of muscle tissue damage following eccentric exercise. Hum Physiol 27:133–137
Safari T, Nematbakhsh M, Hilliard LM, Evans RG, Denton KM (2012) Sex differences in the renal vascular response to angiotensin II involves the Mas receptor. Acta Physiol 206:150–156
NSCA Certification Commission (2008) Exercise technique manual for resistance training, 2nd edn. Human Kinetics, Champaign
Machado M, Willardson JM (2010) Short recovery augments the magnitude of muscle damage in high responders. Med Sci Sports Exerc 42:1370–1374
Borg G (1988) Borg’s perceived exertion and pain scales. Human Kinetics, Champaign
Linton Marigold, Phillip S, Jr Gallo, Cheryl Logan A (1975) The practical statistician: simplified handbook of statistics. Brooks/Cole, Belmont
De Marinis E, Martini C, Trentalance A, Pallottini V (2008) Sex differences in hepatic regulation of cholesterol homeostasis. J Endocrinol 198:635–643
Wolf MR, Fragala MS, Volek JS, Denegar CR, Anderson JM, Comstock BA, Dunn-Lewis C, Hooper DR, Szivak TK, Luk HY, Maresh CM, Hakkinen K, Kraemer WJ (2012) Sex differences in creatine kinase after acute heavy resistance exercise on circulating granulocyte estradiol receptors. Eur J Appl Physiol 112:3335–3340
Kendall B, Eston R (2002) Exercise-induced muscle damage and the potential protective role of estrogen. Sports Med 32:103–123
Swaminathan R, Ho CS, Donnan SP (1988) Body composition and plasma creatine kinase activity. Ann Clin Biochem 25:389–391
Lippi G, Banfi G, Salvagno GL, Montagnana M, Franchini M, Guidi GC (2008) Comparison of creatinine-based estimations of glomerular filtration rate in endurance athletes at rest. Clin Chem Lab Med 46:235–239
Conflict of interest
No conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Amorim, M.Z., Machado, M., Hackney, A.C. et al. Sex differences in serum ck activity but not in glomerular filtration rate after resistance exercise: is there a sex dependent renal adaptative response?. J Physiol Sci 64, 31–36 (2014). https://doi.org/10.1007/s12576-013-0287-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12576-013-0287-2