
Abstract
Ghrelin and adiponectin have been found in breast milk and are considered to take part in the regulation of growth and energy metabolism of infants. Our aims were to determine ghrelin and adiponectin levels in breast milk and serum samples of mothers and their infants, and to investigate the relationship between their levels and anthropometry of newborn infants during early postnatal life. Total and active ghrelin and adiponectin levels were studied in breast milk, and the serum samples of 25 healthy lactating women and their healthy fullterm infants were taken at the 1st and 4th months of life. Anthropometric measurements of infants were also performed during the study period. Breast milk and infant serum active ghrelin levels were found to be significantly increased at the 4th month of life compared with 1st month levels (p < 0.05). Maternal serum total ghrelin and infant serum adiponectin levels were found to be significantly reduced at the 4th month of life (p < 0.05). Breast milk active ghrelin levels were higher than the infant and maternal serum active ghrelin at the 1st and 4th months (p < 0.05). There was a negative significant correlation between the level of infant serum active ghrelin levels and BMI of infants at the 1st month. A positive significant correlation was found between the level of 1st month infant serum adiponectin levels and weight gain of infants during the study period. Fourth month infant serum adiponectin were also positively correlated with weight and BMI of infants at the 4th month and the weight gain during study period. There was a positive significant correlation between the level of 4th month breast milk active ghrelin and weight gain of infants during the study period. Ghrelin and adiponectin are involved in postnatal growth of infants. Ghrelin in breast milk also seems to be related to the growth of infants during early postnatal life. The sources of these peptides in breast milk are probably both maternal serum and breast tissue itself.
Similar content being viewed by others


Introduction
Ghrelin, which is a novel 28 amino acid peptide hormone produced mainly by fundus of the human stomach and epsilon cells of the pancreas, stimulates secretion of growth hormone as the ligand for the growth hormone secretagogue receptor, and increases hunger though its action on hypothalamic feeding centers [1]. It has been suggested that ghrelin has a significant role in the growth and development of infants [2–6].
Adiponectin is a 244 amino acid protein, mainly produced by adipose tissue, which modulates a number of metabolic processes, including glucose regulation and fatty acid catabolism [7]. Adiponectin level is inversely correlated with body fat percentage in adults, while the association in infants and young children is less clear [8, 9]. Weight reduction significantly increases circulating levels [10]. The role of adiponectin on the growth of infants during early postnatal life growth is not clear.
Breast milk also contains a variety of bioactive substances such as hormones and growth factors in addition to macro- and micronutrients [11]. It has been suggested that these factors in breast milk may have long-term effects on growth, development, and overall health into adulthood [12]. Recently, ghrelin and adiponectin have also been discovered in breast milk, probably have a significant role in the regulation of appetite, carbohydrate/lipid metabolism, and energy balance of infants [13–15]. However, there are only a few studies investigating the relationship between the growth of infants and both ghrelin and adiponectin in breast milk, while the effects of these peptides on growth and their source in breast milk is still a controversial issue.
In this study; ghrelin and adiponectin levels have been studied in breast milk, and infant and maternal serum to investigate whether there is any relationship between their levels and postnatal growth of the infants, and to determine the source of these peptides in breast milk.
Subjects and methods
The study protocol was approved by the local Ethical Committee. Informed consent has been obtained from all parents of infants before the study.
Subjects
Twenty-five healthy lactating non-obese women, with a mean age of 24 ± 0.95 years, who had full-term natural deliveries, and their infants were included in the study. However, during the study period, 6 mothers and their infants were excluded from analysis because of an unwillingness to attend the research, and for this reason, 19 mothers and their infants were evaluated at the 4th month.
No mother had a history of abdominal surgery or gastrointestinal disease or took any medication prior to the period of sample collection. All infants were delivered at term (between 37 and 40 weeks) and born after an uneventful pregnancy by normal delivery. Infants who had neonatal disease, fever, chronic illness or current pathology compromising growth, or were partially breastfeeding were excluded from the study.
At the 1st and 4th months of life, anthropometric measurements including weight and length were performed, and breast milk and infant and maternal serum ghrelin and adiponectin concentrations were determined. The primary outcome measure of our study was to evaluate the relationship between serum, breast milk ghrelin, adiponectin concentrations, and anthropometric parameters of the infants. We evaluated the correlation between ghrelin, adiponectin concentrations, and infant age, weight, and length, and finally investigated the difference in ghrelin and adiponectin concentrations between males and females.
Anthropometric measurements
At the 1st and 4th months of life, weight was measured on a Seca Medical 334 baby scale. Crown-to-heel length was measured to the nearest millimeter on a recumbent infant board by two trained people using a Harpenden Infant Measuring Table. Body mass index (BMI) was calculated as body weight (kg)/square of length (m2). Weight gains during the study period were also calculated.
Breast milk and blood samples
Breast milk samples by hand expression just before breastfeeding, and fasting venous blood samples of infants and mothers, were collected between 0800 and 1000 hours at the 1st and 4th months of life. All milk and blood samples were immediately placed on ice. Blood samples were centrifuged within 30 min at 2,000g for 10 min at 4°C. Breast milk and serum samples were stored at −80°C until they were analyzed for ghrelin and adiponectin. One set of serum and milk samples was acidified, by adding 1 N HCl (10% of volume; pH ~3–4) to stabilize the labile side chain of active ghrelin and to prevent a rapid deacylation of ghrelin, as recommended. Milk samples were thawed for 2 h in the refrigerator and vortexed continuously to ensure sample uniformity. Skim milk was prepared by centrifugation of whole milk at 3,000g for 10 min at 4°C to separate milk fat from the liquid phase. The fat layer was removed, and the aqueous phase was assayed.
Assays
Ghrelin assay
The serum and milk active ghrelin (AGHR) concentrations were determined by radioimmunoassay [Ghrelin (Active) RIA, GHRA-88HK; Linco Research, MO, USA], the serum and milk total ghrelin (TGHR) concentrations were determined by radioimmunoassay [Ghrelin (Total) RIA, GHRT-89HK; Linco Research;] using a polyclonal antibody that recognizes octanoylated and nonoctanoylated ghrelin and I 125 ghrelin as a tracer molecule. The detection limits of the kits were 93 pg/mL for TGHR and 7.8 pg/mL for AGHR when a 100 μL sample size used. The results were evaluated according to pg/mL.
Adiponectin assay
Serum and milk adiponectin concentrations were determined by an enzyme-linked immunosorbent assay (Human Adiponectin ELISA, EZHADP-61 K; Linco Research). Sensitivity limit for this assay is 0.78 ng/ml for Human Adiponectin (20 μl sample size). The appropriate range of the assay is 1.56 to 100 ng/ml Human Adiponectin (20 μl sample size). The results were evaluated according to ng/mL.
Statistical analysis
The analysis was conducted with SPSS software (v.15.0 for Windows; SPSS, Chicago, IL, USA). All quantitative data were presented as the mean ± standard deviations. Statistical comparisons were made using non-parametric Kruskal–Wallis ANOVA and Mann–Whitney U tests. Simple correlations were assessed by Spearmen’s correlation coefficients. The test values of p < 0.05 were considered as significant.
Results
The mean TGHR, AGHR, and adiponectin concentrations in the 1st and 4th months are presented in Tables 1 and 2. Breast milk and infant serum AGHR levels were found to be significantly increased at the 4th month of life compared with the 1st month (p < 0.05). On the other hand, maternal serum TGHR and infant serum adiponectin levels were found to be significantly reduced at the 4th month of life (p < 0.05). TGHR and adiponectin levels of breast milk and maternal serum were not significantly different at the 1st and 4th months of life (p > 0.05). However, breast milk AGHR levels were higher than the infant and maternal serum AGHR at the 1st and 4th months (p < 0.05). No significant correlations could be found among breast milk, infant and maternal serum TGHR, AGHR, and adiponectin levels (p > 0.05).
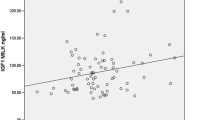
The correlations between breast milk and infant serum AGHR, TGHR, and adiponectin levels and anthropometric parameters of infants are shown in Tables 3 and 4. There was a negative significant correlation between the level of infant serum AGHR levels and BMI of infants at the 1st month of life. (r = −0.41, p = 0.048). A positive significant correlation was found between the level of 1st month infant serum adiponectin levels and weight gain of infants during the study period. (r = 0.53; p = 0.020). Fourth month infant serum adiponectin were also positively correlated with weight and BMI of infants at the 4th month and weight gain during the study period (r = 0.61, p = 0.006; r = 0.71, p = 0.001; r = 0.81, p = 0.001, respectively).
There was a positive significant correlation between the level of 4th month breast milk AGHR and weight gain of the infants during the study period (r = 0.51, p = 0.025).
Discussion
It is well known that ghrelin is involved in the regulation of body weight, and the role of ghrelin on infant growth has been well-documented in a few studies [2–5]. Savino et al. [4] observed a negative correlation between serum ghrelin concentrations and infant weight gain. In another study, a positive correlation between serum ghrelin concentrations and infant weight, height circumferences, and length in the 1st month of life has been reported [2]. Yis et al. [6] suggested that higher serum ghrelin in breast-fed infants might have played a role in their faster growth during the first 3 months of age. We also determined a negative significant correlation between the level of infant serum AGHR levels and BMI of infants at the 1st month of life in the present study.
There are only a few studies investigating the relationship between infant growth and serum adiponectin levels in the literature. It has been reported that cord blood adiponectin inversely associated with weight gain in the 1st month of life [8]. Serum adiponectin levels have also been found to be positively correlated with birth weight and length [16]. In this study, a positive significant correlation has been found between 1st month infant serum adiponectin levels and weight gain of infants during the study period. Fourth month infant serum adiponectin levels were also positively correlated with weight and BMI of infants at the 4th month and weight gain during the study period. These results show that the serum adiponectin may also have an important role in infant growth during early postnatal life.
The possible role of breast milk leptin on early infant growth has been investigated in a few studies, and it has been suggested for short-term control of food intake and long-term control of energy balance and body weight regulation [17–20]. Detection of leptin receptors in intestine epithelial cells suggests that leptin could pass from milk to infant blood, supporting these findings [21]. Despite the detection of ghrelin and adiponectin in breast milk and their receptors in gastric epithelial cells of human, there is no sufficient study investigating the relationship between breast milk ghrelin and adiponectin and infant growth of breast-fed infants during early postnatal life [22, 23]. Aydin et al. [15] found that increases in ghrelin levels in colostrum, transitional and mature milk paralleled infant growth. In our recent study, we showed that the colostrum TGHR was negatively correlated with BMI and weight of the infants at birth, while there was no significant correlation with colostrum adiponectin [24]. In this study, a positive significant correlation has also been detected between the level of 4th month breast milk AGHR concentrations and weight gain of infant during the study period. We think that these findings might be evidence of the effect of ghrelin in breast milk on infant growth. It can be speculated that the amount of ghrelin in breast milk might be physiologically provided (synthesized by mammary epithelial cells or passed to breast milk from the serum of mother) in relation to the need and the state of the infant beginning from birth as suggested for leptin.
We could not determine any relationship between adiponectin levels in breast milk and growth parameters of the infants. Further longitudinal investigations are needed, especially during the early lactation period, to clarify the effects of breast milk adiponectin on growth, appetite, and regulation of nutrition of infancy and childhood obesity.
In our study, mother serum and breast milk TGHR levels were found to be reduced during 1–4 postpartum lactation months. In contrast, mother serum and breast milk AGHR levels were found to be increased during 1–4 postpartum lactation months. Both AGHR and TGHR are present in various tissues, milk, and blood, where they have important physiological roles. One of the main differences between these two forms is that only TGHR can pass the blood–brain barrier. In terms of milk ghrelin, however, the “active” form is physiologically more important for infant development [25]. TGHR is not totally inactive, has an influence on cell proliferation and adipogenesis, and counteracts the metabolic action of AGHR. Therefore, it was important to determine whether concentrations of both AGHR and TGHR in breast milk vary at different stages of lactation during the entire period of the first 6 months of lactation [26].
The source of peptides in breast milk is still a controversial issue. Kierson et al. [14] reported that ghrelin levels in breast milk were higher than the maternal plasma, and suggested that mammary epithelial cells were able to produce ghrelin mRNA. However, Aydin et al. reported that ghrelin was present in colostrum, and transitional and mature milk in increasing amounts, and that the maternal plasma AGHR levels were significantly higher than that of breast milk after delivery, suggesting ghrelin in breast milk might come from plasma [5]. Martin et al. [13] reported that the concentration of adiponectin in breast milk is much lower than the serum levels. In this study, TGHR and adiponectin levels of breast milk and maternal serum were not found to be significantly different, and no significant correlations could be found between breast milk, infant and maternal serum TGHR, AGHR, and adiponectin levels. If these findings are taken into consideration, it can be suggested that breast tissue is able to synthesis some peptides such as ghrelin and adiponectin. However, we also found that AGHR levels in breast milk were higher than the maternal serum levels at the 1st and 4th months of life, and significantly increases in both breast milk and maternal serum AGHR levels have been detected during the study period, which indicates that at least part of the ghrelin in human milk originates from the mother’s plasma. We think that the differences in results between present and previous studies may be related to the kit used to measure AGHR in the breast milk. There is no commercial milk ghrelin assay kit. Thus, Groschl et al. [27] showed different levels for the breast milk ghrelin using different kits.
In conclusion; we think that ghrelin and adiponectin may play an important role in the postnatal growth of infants. Ghrelin in breast milk also seems to be related to the growth of infants during early postnatal life. The sources of these peptides in breast milk are probably both maternal serum and breast tissue itself. However, more studies are required to clarify the role of ghrelin and adiponectin in breast milk in early human development. Also, more longitudinal studies are needed to better understand the possible long-term consequences of these peptides in further life.
References
Kojima M, Kangawa K (2005) Ghrelin: structure and function. Physiol Rev 85:495–522
Savino F, Grassino EC, Fissore MF, Guidi C, Liguori SA, Silvestro L, Oggero R, Miniero R (2006) Ghrelin, motilin, insulin concentration in healthy infants in the first months of life: relation to fasting time and anthropometry. Clin Endocrinol 65:158–162
Onal EE, Cinaz P, Atalay Y, Turkyilmaz C, Bideci A, Akturk A, Okumus N, Unal S, Koc E, Ergenekon E (2004) Umbilical cord ghrelin concentrations in small- and appropriate-for-gestational age newborn infants: relationship to anthropometric markers. J Endocrinol 180:267–271
Savino F, Liguori SA, Fissore MF, Oggero R, Silvestro L, Miniero R (2005) Serum ghrelin concentration and weight gain in healthy term infants in the first year of life. J Pediatr Gastroenterol Nutr 41:653–659
Savino F, Fissore MF, Liguori SA, Grassino EC, Guidi C, Oggero R, Silvestro L, Miniero RJ (2007) Serum ghrelin concentration, fasting time and feeding in infants. J Pediatr Endocrinol Metab 20:1027–1033
Yis U, Ozturk Y, Sisman AR, Uysal S, Soylu OB, Buyukgebiz B (2010) The relation of serum ghrelin, leptin and insulin levels to the growth patterns and feeding characteristics in breast-fed versus formula-fed infants. Turk J Pediatr 52:35–41
Savino F, Petrucci E, Nanni G (2008) Adiponectin: an intriguing hormone for paediatricians. Acta Paediatr 97:701–705
Ukkola O, Santaniemi M (2002) Adiponectin: a link between excess adiposity and associated comorbidities? J Mol Med 80:696–702
Mantzoros CS, Rifas-Shiman SL, Williams CJ, Fargnoli JL, Kelesidis T, Gillman MW (2009) Cord blood leptin and adiponectin as predictors of adiposity in children at 3 years of age: a prospective cohort study. Pediatrics 123:682–689
Coppola A, Marfella R, Coppola L, Tagliamonte E, Fontana D, Liguori E, Cirillo T, Cafiero M, Natale S, Astarita C (2008) Effect of weight loss on coronary circulation and adiponectin levels in obese women. Int J Cardiol 134:414–416
Hamosh M (2001) Bioactive factors in human milk. Pediatr Clin North Am 48:69–86
Savino F, Liguori SA (2008) Update on breast milk hormones: leptin, ghrelin and adiponectin. Clin Nutr 27:42–47
Martin LJ, Woo JG, Geraghty SR, Altaye M, Davidson BS, Banach W, Dolan LM, Ruiz-Palacios GM, Morrow AL (2006) Adiponectin is present in human milk and is associated with maternal factors. Am J Clin Nutr 83:1106–1111
Kierson JA, Dimatteo DM, Locke RG, Mackley AB, Spear ML (2006) Ghrelin and cholecystokinin in term and preterm human breast milk. Acta Paediatr 95:991–995
Aydin S, Aydin S, Ozkan Y, Kumru S (2006) Ghrelin is present in human colostrum, transitional and mature milk. Peptides 27:878–882
Inami I, Okada T, Fujita H, Makimoto M, Hosono S, Minato M, Takahashi S, Harada K, Yamamoto T (2007) Impact of serum adiponectin concentration on birth size and early postnatal growth. Pediatr Res 61:604–606
Ucar B, Kirel B, Bor O, Kilic FS, Dogruel N, Aydogdu SD, Tekin N (2000) Breast milk leptin concentrations in initial and terminal milk samples: relationships to maternal and infant plasma leptin concentrations, adiposity, serum glucose, insulin, lipid and lipoprotein levels. J Pediatr Endocrinol Metab 13:149–156
Miralles O, Sanchez J, Palou A, Pico C (2006) A physiological role of breast milk leptin in body weight control in developing infants. Obesity (Silver Spring) 14:1371–1377
Dundar NO, Anal O, Dundar B, Ozkan H, Caliskan S, Buyukgebiz A (2005) Longitudinal investigation of the relationship between breast milk leptin levels and growth in breast-fed infants. J Pediatr Endocrinol Metab 18:181–187
Doneray H, Orbak Z, Yildiz L (2009) The relationship between breast milk leptin and neonatal weight gain. Acta Paediatr 98:643–647
Morton NM, Emilsson V, Liu YL, Cawthorne MA (1998) Leptin action in intestinal cells. J Biol Chem 273(40):26194–26201
Takeshita E, Matsuura B, Dong M, Miller LJ, Matsui H, Onji M (2006) Molecular characterization and distribution of motilin family receptors in the human gastrointestinal tract. J Gastroenterol 41:223–230
Yoneda K, Tomimoto A, Endo H, Lida H, Sugiyama M, Takahashi H, Mawatari H, Nozaki Y, Fujita K, Yoneda M, Inamori M, Nakajima N, Wada K, Nagashima Y, Nakagama H, Uozaki H, Fukayama M, Nakajima A (2008) Expression of adiponectin receptors, AdipoR1 and AdipoR2, in normal colon epithelium and colon cancer tissue. Oncol Rep 20:479–483
Dundar NO, Dundar B, Cesur G, Yilmaz N, Sutcu R, Ozguner F (2010) Ghrelin and adiponectin levels in colostrum, cord blood and maternal serum. Pediatr Int 52:622–625
Aydin S, Geckil H, Karatas F, Donder E, Kumru S, Kavak EC, Colak R, Ozkan Y, Sahin I (2007) Milk and blood ghrelin level in diabetics. Nutrition 23:807–811
Ilcol YO, Hizli B (2007) Active and total ghrelin concentrations increase in breast milk during lactation. Acta Paediatr 96:1632–1639
Groschl M, Uhr M, Kraus T (2004) Evaluation of the comparability of commercial ghrelin assays. Clin Chem 50:457–458
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Cesur, G., Ozguner, F., Yilmaz, N. et al. The relationship between ghrelin and adiponectin levels in breast milk and infant serum and growth of infants during early postnatal life. J Physiol Sci 62, 185–190 (2012). https://doi.org/10.1007/s12576-012-0193-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12576-012-0193-z