
Abstract
Introduction
The COVID-19 pandemic prompted public health teams across the world to emphasize case identification, contact tracing, and isolation in outbreak management strategies. Contact tracing was advanced by global access to mobile phones to develop and implement digital contact tracing (DCT) technology with the objective of increasing the rate of contact tracing while reducing the resources required.
Purpose
This study aimed to describe the DCT technology used during the COVID-19 pandemic across the world, and to identify differences and similarities between characteristics and uses.
Methods
This review followed the PRISMA (2020) guidelines for systematic reviews. Literature searches were conducted using Embase, MEDLINE, and PubMed and were restricted to English studies published between 2019 to 2023. Studies were excluded if they did not report findings for DCT during COVID-19, did not provide data for technology characteristics or outcomes, or were a study design listed for exclusion.
Results
Sixty one studies were included in the review producing results for 147 digital contact tracing technologies across 83 countries. The majority of digital contact tracing (DCT) technologies are government-owned (75.6%), primarily developed for COVID-19 tracing (96.4%). Bluetooth is the most favored technology (70%) used in their development, followed by GPS (30%) and QR codes (22%). Applications are the preferred platform (90.9%), with a few using applets (6.3%) and wearable devices (1.4%). Only 2 DCT technologies have achieved over 100 million downloads or uses (3.1%). Most DCTs fall into the 1–9.99 million downloads range (27.7%) and 10,000–99,999 downloads (20%). The majority of DCTs are voluntarily used by the population (63.6%), while 27.3% are mandated for use.
Conclusions
Digital contact tracing technologies were developed and implemented globally as a strategy in emergency outbreak management to reduce the spread of disease. This review describes the use of DCT across the world by identifying key features and characteristics that will serve as a lesson learned for improvement of existing DCT technologies for other emergency response outbreak management.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
The COVID-19 pandemic, caused by the SARS-CoV-2 virus, is a respiratory illness outbreak unlike the world had seen in recent history, and led to over 760 million cases and 6.9 million deaths between 2019 and 2023 [1, 2]. Public health teams worked tirelessly across the world testing a variety of solutions to reduce the effects of the ongoing threat. Outbreak response methods traditionally focus on case identification, halting transmission, surveillance, and isolation of cases; techniques that have been implemented and built upon from early century disease [3].
Contact tracing is an important tool for outbreak management as it assists in breaking chains of transmission to slow or stop the spread of a virus [4]. Traditional methods of contact tracing require manual efforts by teams of public health officials who trace the close contacts of identified index cases presenting with the disease of interest and provide support with the quarantine of contacts [4, 5]. Although traditional methods of emergency pandemic mitigation techniques were beneficial in fighting the evolving COVID-19 disease, many countries utilized information systems and technology, including smartphones, to take advantage of a world in which technology is an everyday part of life. In 2019, 65% of the global population were smartphone users, a statistic that aided public health response teams as digital contact tracing (DCT) applications and technology were incorporated into outbreak management [3].
DCT applications provide the unique opportunity to identify close contacts of positive COVID-19 cases without the work required to be performed by manual contact tracing teams which is demanding in time, effort, and relies heavily on the quantity and quality of information available [5]. Countries who elected to adopt DCT technology typically did so in the form of smartphone applications, websites, and wearable technology that provided the user with the status of infections in a specific location they had visited or sending exposure notifications (ENs) to close contacts of cases. Many DCT applications were built upon location-based technology including Bluetooth, GPS, QR Code, or a combination of these technologies [5, 6].
International stakeholders play an important role in the development of digital technologies for contract tracing. Go.Data is a digital tool used to combat the Ebola epidemic and it was developed by WHO in 2014 [7]. WHO and PAHO also had developed a multidisciplinary information hub to enable exchange of information on COVID-19 contact tracing protocol [8]. Other institutions, like CDC, conducted research focusing on requirements for digital contract tracing application to provide guidance for technical implementation of DCT [9]. This highlights the collaborative efforts aimed at sharing information and best practices for contact tracing protocols, underscoring the importance of global cooperation in addressing public health emergencies.
DCT has previously been used in other outbreaks including the use of the DCT platform for Polio in Nigeria which was implemented in 2017 using Geographic Information Systems and the use of Ebola Contact Tracing app in Sierra Leone as well as SORMAS (Surveillance, Outbreak Response Management and Analysis System) in Nigeria during the 2014–2016 Ebola epidemic [10,11,12,13]. Other technology related contact tracing effort that has been recorded includes the use of public surveillance cameras, the closed-circuit television (CCTV), in China and South Korea during the MERS outbreak in 2015 [14, 15].
DCT technologies uptake play a role in outbreak management. It was estimated that 60% uptake rates in the population have substantial effect on reducing the spread of disease and even lower numbers of 15% would still reduce infection and death rates [16,17,18,19]. To ensure that DCT technology'zz's uptake in the population reaches the desired numbers and is effective in outbreak management, we need to have a holistic understanding of the characteristics of DCT technology that is most suitable to be implemented for an emergency response outbreak.
This systematic review will provide analysis of the characteristics of the implemented DCT technologies during COVID-19 pandemic in order to better understand the potential use of technology for future outbreak response. An overview will describe the DCT features such as the origin, DCT system ownership, technology and platform type, as well as mandate status of the DCT technologies.
2 Methodology
2.1 Search strategy
The processes conducted for this review were based on the PRISMA guidelines. A systematic search was carried out using Embase (1974–2023), MEDLINE (1946–2023), and PubMed (-2023) databases on May 20th, 2023. Both Embase and MEDLINE were searched via Ovid, whereas PubMed was searched via NIH ncbi.nlm.nih. Two search strategies were created to be used for the different databases. The search terms used for the Embase and MEDLINE databases through OVID are “covid-19 or covid19 or sars-cov-2 or coronavirus or severe acute respiratory syndrome coronavirus”, “contact tracing or contact investigation or transmission tracing or contact with infect* or contact follow-up or case detection”, “mobile phone* or smartphone* or cell* phone or social media or phone app* or personal device or digital device), 1 and 2 and 3, “limit 4 to english language”, and “limit 5 to yr = ”2019-Current””. The search terms used for PubMed are “covid-19 or covid19 or sars-cov-2 or coronavirus or severe acute respiratory syndrome coronavirus” AND “contact tracing or contact investigation or transmission tracing or (contact adj3 infect*) or contact follow-up or case detection” AND “mobile phone* or smartphone* or cell* phone or social media or phone app* or personal device or digital device”.
Studies eligible for review were study that fit the following criteria; (i) digital technology used for public health contact tracing during COVID-19 pandemic; (ii) published between December 2019-May 2023; (iii) peer-reviewed published research including cross-sectional studies, cohort studies, case–control studies, case series, case reports, meta-analysis; (iv) primary or secondary outcomes report digital technology in the public health sector; (v) written in English language. Studies that are predominantly designed as dissertation, thesis, conference abstract, randomized control trials, background review, any type of expert opinion, letter to editor, commentary, pilot study, and modelling study; non contact tracing outcome; outcome not based on digital technology performance; written in non-english language were excluded from review process.
2.2 Selection process
The selection process ensured that duplication papers were removed before entering the reviewing stage. Multiple reviewers were used in the study selection phase to reduce error and possible selection bias. The first and second reviewers independently completed title and abstract screenings as well as the full text screening using EndNote20, Excel, and Google Sheets. Studies were screened in the title and abstract phase with inclusion and exclusion criteria, and if given information was not enough to decide, the study was forwarded to the full text screening for a more in-depth review. Studies meeting the inclusion criteria, reported data on the technology name, and one or more other categories during the full-text screening, were included in the final review. Studies identified for inclusion by both the first and second reviewer during screening stages were selected for the data extraction phase, and studies identified for exclusion by both reviewers were removed. Any discrepancies between the first and second reviewers were examined by a third reviewer, who used the final decision to reach a consensus between two reviewers.
2.3 Data collection and analysis
Data collection was conducted by the first reviewer from the sixty-one included studies which passed the screening phases. A template was developed using Microsoft Excel and Google Sheets to outline information needed to be extracted from these studies.
Each study was examined for data fitting each of the outcome categories, namely: i) name of the digital contact tracing technology; ii) DCT implementation location which consists of continent, country, and region; iii) year of DCT release; iv) DCT system ownership, categorized as government, private, and government-private collaboration; v) targeted user demographic, for health workers or for public; vi) purpose of technology development, categorized as developed for COVID-19 and repurposed; vii) type of technology used for location tracking such as Bluetooth, GPS, or QR codes; viii) type of platform for the DCT technology such as applications, websites, wearable devices; xi) mandate status, whether the app was government mandated or voluntary used, and other characteristics such as unique features, number of downloads, number of contacts identified, detection rate, and number of cases prevented. Information was not reported in all categories for each DCT technology and missing data was designated as not available.
3 Results
3.1 Study selection
The search of all three databases produced a total of 1,254 results, which were imported into EndNote20. From these results, 434 were duplicates and removed by both EndNote20 and manual assessment, leaving 820 to be screened for eligibility. The first phase of screening, by title and abstract, resulted in 683 records being excluded for either meeting exclusion criteria or not meeting inclusion requirements. The second phase of screening assessed the full text of each study and an additional 76 studies were excluded for one of six reasons: study design, results did not provide outcomes for technology and performance, not contact tracing, not digital contact tracing, and study not in English. An additional study was excluded because the full text could not be accessed. The resulting number of studies passing eligibility screenings and were available for extraction was 61 [5, 6, 16, 18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75]. Figure 1 shows a PRISMA [83] flow chart of the selection process during each stage.

PRISMA flowchart with results for screening process
3.2 Digital contact tracing technology characteristics
The studies reported 147 DCT technology apps, websites, and wearable technology. Of the 147 included, 11 were from Africa (7.5%), 54 from Asia (36.7%), 35 from Europe (23.8%), 36 from North America (24.5%), 3 from Australia/Oceania (2.0%), 5 from South America (3.4%), and 3 did not have an originating location identified (2.0%). Figure 2 depicts the coverage of digital contact tracing technology on a global scale by identifying the number of DCT technologies adopted per country.

Number of DCT technologies used per country
This map demonstrates that many countries adopted only one form of DCT technology, while several had two or three. India, China, and the United States of America have the highest populations in the world [14], and were the only countries to report more than four applications or other technology available for use. Data was collected on characteristics of technology reported on; the summary of these findings is reported in Table 1. A full report of characteristics for each DCT technology is included in the data analysis table (Online Resource 1).
Out of 147 DCT technologies reviewed, 67 DCTs were released in 2020, showing an effort to catch up with the peak of COVID-19 pandemic. Majority of the DCT technologies (65;75.6%) were developed and owned by the government, some are owned by private sectors (20; 23.3%) and only a miniscule amount is a collaborative effort of government and private sectors (1;1.2%). As a DCT technology, the purpose of the development matches the current outbreak, which is for COVID-19 tracing (53; 96.4%). The preferable type of technology used in development of DCT technology is bluetooth (70; 70%), followed by GPS (30; 30%) and QR codes (22; 22%). Application becomes the chosen platform for DCT technology (130; 90.9%), followed by applet (9; 6.3%) and wearable devices (2; 1.4%). There are only 2 DCT technologies that reached 100,000,000 downloads/uses (3.1%). Most of the DCTs had a number of uses ranging from 1,000,000 - 9,999,999 downloads (18; 27.7%) and 10,000 - 99,999 downloads (13; 20%). Considering the number of downloads, it is consistent with the result that only 6 of them are mandated to be used (6;27.3%) and the majority are voluntarily used by the population (14;63.6%).
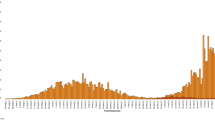
Studies reported the number of downloads and uses of DCT technologies as either a number or percentage of the study population. Percentage and population size were not reported for all studies at the time data was collected, therefore it is difficult to determine the exact number of downloads for numerous apps. The DCT which had the highest number of downloads was reported to be the Health Code apps from China which received 1.28 billion downloads country-wide between all provincial versions. As an individual DCT technology, the Aarogya Setu app launched by the Government of India received 216 million downloads. The number of downloads or uses of DCT organized by continent is shown in Fig. 3.

Number of Downloads or Uses by Continent
As seen in Fig. 3, four applications with download counts in Africa, Australia/Oceania, and South America reported results between 1,000,000 – 99,999,999 downloads. Europe reported downloads for 13 applications throughout countries to be between 10,000 – 99,999,999. Both Asia and North America received a much wider range of download/use of technology with Asia reporting ranges from 1,000 all the way up to 100,000,000 + for 16 technologies, and North America within the range of 1 to 99,999,999 for 29 applications.
In Figs. 4A & B, features of technologies were compared by continent to identify differences between regions and preferred technology used for DCT. Overall, 75.6% of the technology reported government DCT system ownership. Africa, Asia, and North America reported technology launched by both private and government bodies (n = 69, 80.2%), while Australia/Oceania, Europe, and South America only reported government affiliated applications (n = 14, 16.3%), and three (n = 3, 3.5%) were unidentified in location. North America reported the highest parentage of privately affiliated companies at 34.3% (n = 12) of North American DCT technologies. Three technologies were reported as privately affiliated with unknown originating locations. Technology types were broken into 4 categories: Bluetooth, GPS, QR code, and other. In general, in general, the most adopted technology type was Bluetooth, followed by GPS and QR code. Applications that reported more than one type of technology used were included in all appropriate categories. Multiple technology types were reported in all continents excluding South America, which had results of technology type for only one of the five applications included in the review, and therefore reported only the use of Bluetooth. Europe and North America heavily favoured Bluetooth technology with fewer DCT applications utilizing GPS, QR Code, or other technology. Africa, Asia, and Australia/Oceania used a variety of Bluetooth, GPS, QR Codes, and other technology types.

A DCT system ownership by continent, B Technology type by continent, C Technology platform by continent, D Area coverage by continent
Technology platforms were examined across the continents and findings are reported in Fig. 4C. Overall, applications were the most used DCT technology platform. North America reported a small percentage of SSO (single sign-on) identification methods used for DCT, the majority done through smartphone applications. Asia reported slightly less percentages of DCT technology using apps, but use of Applets accessed through already existing applications as well as wearable devices and websites. Africa, Australia/Oceania, Europe, and South America reported the sole use of smartphone applications for digital contact tracing. Three applications were identified without corresponding locations. The area of coverage per technology was also collected and reported upon in Fig. 4D. Most technologies in all continents, excluding North America, reported coverage country-wide and a few were applied across multiple countries. Of the applications launched for each European country, many reported the ability to be used in surrounding countries. North America reported very different results as most technology in the United States of America provided coverage by state or county, and Canada received provincial coverage from two of the three applications reviewed.
4 Discussion
This review identified 147 digital contact tracing technology implemented in 83 countries across the world. There was a global implementation of technology that reached every continent, but fewer DCT technologies were available in Africa and South America than any other continents. Countries without reported technology correlate with nations of less developed status, and those with more numerous available DCT technologies were of those most highly populated [76, 77]. Applications and other technology used within Asia reported the highest number of downloads and uses, followed by Europe, North America, South America, Australia/Oceania, and Africa.
Although China’s Health Code application system was the only technology to receive uptake of over 80% of the population, other technologies reported over the recommended 60% threshold, and most DCT technology received more than the recommended 15% of population minimum. Mandate status may correlate with the increased number of downloads and uses, as those which were deemed mandatory for use did not report results with low number of uses. Privacy and ethical issues have been raised as a possible deterrent to uptake of DCT technology within the public [78].
DCT technology was generally affiliated with government rather than private institutions. Although governments may have partnered with private companies to develop the technology, those which were approved or owned by government departments were considered affiliated with a country’s governmental body.
Not all applications and wearable devices used more than one form of technology type, but many applications used Bluetooth the primary proximity indicator within DCT and incorporated the use of GPS, QR Codes, and other technologies to assist with accuracy. Bluetooth technology was typically used to trace contacts by identifying other Bluetooth compatible phones through signals ranging 6 feet or less for more than 15 min [35, 79]. Signal transmissions were commonly described as “handshakes” between Bluetooth compatible devices [46]. QR Codes were multifaceted in its applications, finding different uses between a variety of apps. Select applications used QR Codes in facilities, venues, and borders, requiring users to scan a code with their app, logging visits by individuals with their key personal information [80]. Other applications generated QR Codes to provide personalized health status, vaccination status, and travel passes [45].
Smartphone applications were reported as the most used platform of technology for DCT world-wide and by a large margin. Wearable technology was implemented in countries which had already adopted smartphone applications to include those who did not have access to their application. Singapore provided wearable devices, called tokens, which complimented the TraceTogether application to address technical and privacy concerns hindering the uptake of the DCT technology [81]. This helps to reduce inequalities in populations and close gaps caused by lack of access to smartphones which are compatible with these technologies [24].
Lastly, the majority of DCT technologies were implemented countrywide, allowing for more contacts to be traced with movement of cases and health populations. Many European countries offered applications, which could still be used in neighbouring countries allowing for better digital contact tracing efforts to be conducted. Liu reported this feature in apps including, but not limited to, HOIA, #OstaniZdrav, Corona-Warn-App, CoronaMelder, and Koronavilkku [82]. However, this was not the case within the United States of America which based the coverage of their applications on state lines rather than as a country overall. If applications do not correspond with those in other states, travellers pose additional risks to spreading disease with the ability to digitally trace.
4.1 Strength and limitations
This study provides a comprehensive perspective on the implementation of digital contact tracing technologies used during covid-19. By reviewing 147 DCT technologies across 83 countries, this study also covers the analysis of prominent characteristics of DCT technology that influence its adoption, providing valuable insights to enhance understanding towards effective contact tracing efforts. There are limitations identified within this review. Only studies which were reported in the English language were included leaving the possibility of quality data being excluded, especially with many of the technologies covering countries which do not use English as an official language. Additionally, many studies were limited and did not provide information for several of the characteristics of interest. Although the selection process was designed to reduce bias, quality assessments for individual studies were not conducted, leaving room for other biases to be overlooked, and it is noted that publication bias may exist within the studies available. It is important to review the differences and similarities summarized in this review between DCT technologies to understand how different technological, and political factors relating to mandate status, may play a role in their performance. Outbreaks will continue to threaten public health so by utilizing the information gathered within this systematic review, DCT developers and government institutions can prepare and identify changes that may be made to existing technology prior to when it is needed next. Further research should be conducted to determine the effectiveness of DCT in contact tracing methods and outbreak management as this review was unable to collect the required data to make analyses.
5 Conclusions
The COVID-19 pandemic posed a serious global public health threat that opened opportunities for advanced technology to be implemented in outbreak management strategies. This systematic review focus on landscape of digital contact tracing (DCT) technologies deployed during the COVID-19 pandemic. Findings showed a global disparity in DCT availability, with fewer implementations observed in Africa and South America compared to other continents, indicating a correlation with the level of economic development and population density. Notably, government affiliation predominated in the development and deployment of DCT technologies, with mandates potentially influencing uptake rates.
Technologically, Bluetooth emerged as a primary proximity indicator within DCT, often augmented by GPS, QR codes, and other tools to enhance accuracy. Smartphone applications emerged as the most utilized platform for DCT worldwide, although efforts to bridge technological disparities were evident through the introduction of wearable devices in regions lacking smartphone access, as seen in Singapore. Moving forward, further research is warranted to assess the effectiveness of DCT in contact tracing and outbreak management. This study provides a comprehensive analysis of digital contact tracing technology during the COVID-19 pandemic, highlighting global implementation across 83 countries. By leveraging the findings of this study, policymakers, DCT developers, and public health officials can proactively prepare and refine existing technologies to address future public health crises, thereby contributing to the global effort to combat infectious diseases.
Data availability
The data sets generated during and/or analysed during this study are available from the corresponding author on reasonable request.
Abbreviations
- DCT:
-
Digital Contact Tracing
- GPS:
-
Global Positioning System
- QR Code:
-
Quick Response Code
- SSO:
-
Single Sign On
- GIS:
-
Geographic Information System
- GSM:
-
Global System for Mobile communication
- ODK:
-
Open Data Kit
- Power BI:
-
Microsoft Power Business Intelligence
- ENs:
-
Exposure Notification
References
Chen J. Novel statistics predict the COVID-19 pandemic could terminate in 2022. J Med Virol. 2022;94(6):2845–8. https://doi.org/10.1002/jmv.27661.
World Health Organization: WHO. Coronavirus disease (COVID-19). World Health Organization: WHO. 2023. https://www.who.int/news-room/fact-sheets/detail/coronavirus-disease-(covid-19). Accessed 15 Aug 2023.
Budd J, Miller BS, Manning EM, et al. Digital technologies in the public-health response to COVID-19. Nat Med. 2020;26(8):1183–92. https://doi.org/10.1038/s41591-020-1011-4.
World Health Organization. Coronavirus disease (COVID-19): Contact tracing. https://www.who.int/. 2021. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-covid-19-contact-tracing. Accessed 22 Aug 2023.
Mazza C, Girardi D, Gentile L, Gaeta M, Signorelli C, Odone A. Public health effectiveness of digital contact tracing in the COVID-19 pandemic: A systematic review of available data. Acta Biomedica Atenei Parmensis. 2021;92(S6):e2021439–e2021439. https://doi.org/10.23750/abm.v92iS6.12237.
Golinelli D, Boetto E, Carullo G, Nuzzolese AG, Landini MP, Fantini MP. Adoption of Digital Technologies in Health Care During the COVID-19 Pandemic: Systematic Review of Early Scientific Literature. J Med Internet Res. 2020;22(11): e22280. https://doi.org/10.2196/22280.
World Health Organization: WHO. Tracking COVID-19: Contact Tracing in the Digital Age. World Health Organization: WHO. 2020. https://www.who.int/news-room/feature-stories/detail/tracking-covid-19-contact-tracing-in-the-digital-age. Accessed 16 Mar 2024.
PAHO. Contact Tracing Knowledge Hub. Pan American Health Organization. https://www.paho.org/en/contact-tracing-knowledge-hub. Accessed 16 Mar 2024.
CDC. CDC - Mining Project - Mobile Applications for Digital Contact Tracing - NIOSH. Centers for Disease Control and Prevention. 2023. https://www.cdc.gov/niosh/mining/researchprogram/projects/project_digitalcontacttracing.html. Accessed 18 Mar 2024.
Bode M, Craven M, Leopoldseder M, Rutten P, Wilson M. Molly Bode. McKinsey & Company. 2020. https://www.mckinsey.com/industries/public-sector/our-insights/contact-tracing-for-covid-19-new-considerations-for-its-practical-application. Accessed 20 Oct 2023.
Akpan GU, Bello IM, Touray K, et al. Leveraging Polio Geographic Information System Platforms in the African Region for Mitigating COVID-19 Contact Tracing and Surveillance Challenges: Viewpoint (Preprint). JMIR Publications Inc. 2020. https://doi.org/10.2196/preprints.22544. Accessed 20 Oct 2023.
Danquah LO, Hasham N, MacFarlane M, et al. Use of a mobile application for Ebola contact tracing and monitoring in northern Sierra Leone: a proof-of-concept study. BMC Infect Dis. 2019;19(1). https://doi.org/10.1186/s12879-019-4354-z.
Tom-Aba D, E. Toikkanen S, Glöckner S, et al. User Evaluation Indicates High Quality of the Surveillance Outbreak Response Management and Analysis System (SORMAS) After Field Deployment in Nigeria in 2015 and 2018. In: German Medical Data Sciences: A Learning Healthcare System: Proceedings of the 63rd Annual Meeting of the German Association of Medical Informatics, Biometry and Epidemiology (Gmds e.V.) 2018 in Osnabrück, Germany – GMDS 2018. IOS Press; 2018:233–237. https://ebooks.iospress.nl/publication/50064. Accessed 28 Oct 2023.
Kang M, Song T, Zhong H, et al. Contact Tracing for Imported Case of Middle East Respiratory Syndrome, China, 2015. Emerg Infect Dis. 2016;22(9):1644–6. https://doi.org/10.3201/eid2209.152116.
Park YS, Lee C, Kim KM, et al. The first case of the 2015 Korean Middle East Respiratory Syndrome outbreak. Epidemiology and Health. 2015;37(e2015049): e2015049. https://doi.org/10.4178/epih/e2015049.
Grill E, Eitze S, De Bock F, et al. Sociodemographic characteristics determine download and use of a Corona contact tracing app in Germany—Results of the COSMO surveys. PLoS ONE. 2021;16(9): e0256660. https://doi.org/10.1371/journal.pone.0256660.
Min-Allah N, Alahmed BA, Albreek EM, et al. A survey of COVID-19 contact-tracing apps. Comput Biol Med. 2021;137(October 2021, 104787):104787. https://doi.org/10.1016/j.compbiomed.2021.104787.
O’Callaghan ME, Abbas M, Buckley J, et al. Public opinion of the Irish “COVID Tracker” digital contact tracing App: A national survey. Digit Health. 2022;8. https://doi.org/10.1177/20552076221085065.
Seto E, Challa P, Ware P. Adoption of COVID-19 Contact Tracing Apps: A Balance Between Privacy and Effectiveness. J Med Internet Res. 2021;23(3): e25726. https://doi.org/10.2196/25726.
Mandil A, Mabry R, Milani B, Nour M, Afifi M, Abdel-Ghani K. Mapping of health innovations in response to the COVID-19 pandemic in Eastern Mediterranean and selected Arab Countries. East Mediterr Health J. 2022;28(2):130–43. https://doi.org/10.26719/emhj.22.028.
Mbunge E. Integrating emerging technologies into COVID-19 contact tracing: Opportunities, challenges and pitfalls. Diabetes Metab Syndr. 2020;14(6):1631–6. https://doi.org/10.1016/j.dsx.2020.08.029.
Min-Allah N, Alahmed BA, Albreek EM, et al. A survey of COVID-19 contact-tracing apps. Comput Biol Med. 2021;137: 104787. https://doi.org/10.1016/j.compbiomed.2021.104787.
Müller A, Cau A, Muhammed S, et al. Digital mHealth and Virtual Care Use During COVID-19 in 4 Countries: Rapid Landscape Review. JMIR Formative Research. 2022;6(11): e26041. https://doi.org/10.2196/26041.
Liu M, Zhou S, Jin Q, Nishimura S, Ogihara A. Effectiveness, Policy, and User Acceptance of COVID-19 Contact-Tracing Apps in the Post–COVID-19 Pandemic Era: Experience and Comparative Study. JMIR Public Health Surveill. 2022;8(10): e40233. https://doi.org/10.2196/40233.
Akpan GU, Bello IM, Touray K, et al. Leveraging Polio Geographic Information System Platforms in the African Region for Mitigating COVID-19 Contact Tracing and Surveillance Challenges: Viewpoint. JMIR Mhealth Uhealth. 2022;10(3): e22544. https://doi.org/10.2196/22544.
Fan Y, Wang Z, Deng S, Lv H, Wang F. The function and quality of individual epidemic prevention and control apps during the COVID-19 pandemic: A systematic review of Chinese apps. Int J Med Informatics. 2022;160: 104694. https://doi.org/10.1016/j.ijmedinf.2022.104694.
Hogan K, Macedo B, Macha V, Barman A, Jiang X. Contact Tracing Apps: Lessons Learned on Privacy, Autonomy, and the Need for Detailed and Thoughtful Implementation (Preprint). JMIR Publications Inc. 2021. https://doi.org/10.2196/preprints.27449. Accessed 24 Aug 2023.
Mahr D, Bloch M. Digital risk distribution and COVID-19: How contact tracing is promoted as a solution to equilibrate public health and economic prosperity during pandemics. DIGITAL HEALTH. 2022;8:205520762210850. https://doi.org/10.1177/20552076221085068.
Panchal M, Singh S, Rodriguez-Villegas E. Analysis of the factors affecting the adoption and compliance of the NHS COVID-19 mobile application: a national cross-sectional survey in England. BMJ Open. 2021;11(8): e053395. https://doi.org/10.1136/bmjopen-2021-053395.
Thomas MJ, Lal V, Baby AK, Rabeeh VPM, James A, Raj AK. Can technological advancements help to alleviate COVID-19 pandemic? a review. J Biomed Inform. 2021;117: 103787. https://doi.org/10.1016/j.jbi.2021.103787.
John Leon Singh H, Couch D, Yap K. Mobile Health Apps That Help With COVID-19 Management: Scoping Review. JMIR Nursing. 2020;3(1):e20596. https://doi.org/10.2196/20596.
Voo TC, Ballantyne A, Ng CJ, et al. Public acceptability of COVID-19 control measures in Singapore, Hong Kong, and Malaysia: A cross-sectional survey. Int J Infect Dis. 2022;120:51–8. https://doi.org/10.1016/j.ijid.2022.04.021.
Davalbhakta S, Advani S, Kumar S, et al. A Systematic Review of the Smartphone Applications Available for Corona Virus Disease 2019 (COVID19) and Their Assessment Using the Mobile App Rating Scale (MARS). Cold Spring Harbor Laboratory; 2020. https://doi.org/10.1101/2020.07.02.20144964. Accessed 24 Aug 2023.
Simmhan Y, Rambha T, Khochare A, et al. GoCoronaGo: Privacy Respecting Contact Tracing for COVID-19 Management. J Indian Inst Sci. 2020;100(4):623–46. https://doi.org/10.1007/s41745-020-00201-5.
Jha V, Bassi A, Arfin S, John O. An overview of mobile applications (apps) to support the coronavirus disease 2019 response in India. Indian J Med Res. 2020;151(5):468. https://doi.org/10.4103/ijmr.ijmr_1200_20.
Alanzi T. A Review of Mobile Applications Available in the App and Google Play Stores Used During the COVID-19 Outbreak. J Multidiscip Healthc. 2021;14:45–57. https://doi.org/10.2147/jmdh.s285014.
Pandit JA, Radin JM, Quer G, Topol EJ. Smartphone apps in the COVID-19 pandemic. Nat Biotechnol. 2022;40(7):1013–22. https://doi.org/10.1038/s41587-022-01350-x.
Sharma N, Basu S, Sharma P. Sociodemographic determinants of the adoption of a contact tracing application during the COVID-19 epidemic in Delhi, India. Health Policy and Technology. 2021;10(2): 100496. https://doi.org/10.1016/j.hlpt.2021.02.003.
Sujarwoto S, Augia T, Dahlan H, Sahputri RAM, Holipah H, Maharani A. COVID-19 mobile health apps: an overview of mobile applications in Indonesia. Front Public Health. 2022. https://doi.org/10.3389/fpubh.2022.879695.
Vahidi H, Taleai M, Yan W, Shaw R. Digital Citizen Science for Responding to COVID-19 Crisis: Experiences from Iran. Int J Environ Res Public Health. 2021;18(18):9666. https://doi.org/10.3390/ijerph18189666.
Ishimaru T, Ibayashi K, Nagata M, et al. Industry and workplace characteristics associated with the Use of a COVID-19 contact tracing app in japan: a nation-wide employee survey. Cold Spring Harbor Laboratory. 2021. https://doi.org/10.1101/2021.04.01.21254744. Accessed 24 Aug 2023.
Ishimaru T, Ibayashi K, Nagata M, et al. Factors Associated with Acceptance of a Digital Contact Tracing Application for COVID-19 in the Japanese Working-Age Population. Cold Spring Harbor Laboratory. 2021. https://doi.org/10.1101/2021.10.28.21265601. Accessed 24 Aug 2023.
Salathé M, Althaus CL, Anderegg N, et al. Early Evidence of Effectiveness of Digital Contact Tracing for SARS-CoV-2 in Switzerland. Cold Spring Harbor Laboratory. 2020. https://doi.org/10.1101/2020.09.07.20189274. Accessed 24 Aug 2023.
Al-Kuwari MG, Ali Al Nuaimi A, Semaan S, Gibb JM, AbdulMajeed J, Al Romaihi HE. Effectiveness of Ehteraz digital contact tracing app versus conventional contact tracing in managing the outbreak of COVID-19 in the State of Qatar. BMJ Innovations. 2022;8(4):255–60. https://doi.org/10.1136/bmjinnov-2021-000879.
Huang Z, Guo H, Lee YM, Ho EC, Ang H, Chow A. Performance of Digital Contact Tracing Tools for COVID-19 Response in Singapore: Cross-Sectional Study. JMIR Mhealth Uhealth. 2020;8(10): e23148. https://doi.org/10.2196/23148.
Lai SHS, Tang CQY, Kurup A, Thevendran G. The experience of contact tracing in Singapore in the control of COVID-19: highlighting the use of digital technology. Int Orthop. 2020;45(1):65–9. https://doi.org/10.1007/s00264-020-04646-2.
Thomas R, Michaleff ZA, Greenwood H, Abukmail E, Glasziou P. Concerns and Misconceptions About the Australian Government’s COVIDSafe App: Cross-Sectional Survey Study. JMIR Public Health Surveill. 2020;6(4): e23081. https://doi.org/10.2196/23081.
Vogt F, Haire B, Selvey L, Kaldor J. Effectiveness of Digital Contact Tracing for COVID-19 in New South Wales, Australia. Cold Spring Harbor Laboratory. 2021. https://doi.org/10.1101/2021.11.18.21266558. Accessed 24 Aug 2023.
Chand SS, Chand AA, Chand KK. The use of careFiji app for contact tracing during the COVID-19 pandemic: Digital gap and challenges faced in Fiji. Int J Surg. 2021;92: 106023. https://doi.org/10.1016/j.ijsu.2021.106023.
Ali ZS, Dang H. Factors impacting the use of the NZ COVID Tracer application in New Zealand". Smart Health. 2022;24: 100278. https://doi.org/10.1016/j.smhl.2022.100278.
Howell BE, Potgieter PH. COVID-19 contact-tracing smartphone application usage—The New Zealand COVID Tracer experience. Telecommunications Policy. 2022;46(8): 102386. https://doi.org/10.1016/j.telpol.2022.102386.
Kouliaridis V, Kambourakis G, Chatzoglou E, Geneiatakis D, Wang H. Dissecting contact tracing apps in the Android platform. PLoS ONE. 2021;16(5): e0251867. https://doi.org/10.1371/journal.pone.0251867.
Walrave M, Waeterloos C, Ponnet K. Reasons for Nonuse, Discontinuation of Use, and Acceptance of Additional Functionalities of a COVID-19 Contact Tracing App: Cross-Sectional Survey Study (Preprint). JMIR Publications Inc. 2021. https://doi.org/10.2196/preprints.22113. Accessed 24 Aug 2023.
Piotto S, Di Biasi L, Marrafino F, Concilio S. Evaluating Epidemiological Risk by Using Open Contact Tracing Data: Correlational Study (Preprint). JMIR Publications Inc.; 2021. https://doi.org/10.2196/preprints.28947. Accessed 24 Aug 2023.
Ter Haar W, Bodriesz J, Venekamp RP, et al. The Epidemiological Impact of Digital and Manual Contact Tracing on the SARS-CoV-2 Epidemic in the Netherlands: Empirical Evidence. Cold Spring Harbor Laboratory. 2023. https://doi.org/10.1101/2023.04.27.23289149. Accessed 24 Aug 2023.
van Gend JE, van’t Klooster JWJR, Bolman CAW, van Gemert-Pijnen JEWC. The dutch covid-19 notification app: lessons learned from a mixed methods evaluation among end users and contact-tracing employees. JMIR Form Res. 2022;6(11):e38904. https://doi.org/10.2196/38904.
Shrivastava SR, Shrivastava PS. Exploring the scope and utility of digital proximity tracing in the effective containment of COVID-19 infection: A narrative review. Germs. 2022;12(2):276–82. https://doi.org/10.18683/germs.2022.1329.
O’Donnell CA, Macdonald S, Browne S, et al. Widening or narrowing inequalities? The equity implications of digital tools to support COVID-19 contact tracing: A qualitative study. Health Expect. 2022;25(6):2851–61. https://doi.org/10.1111/hex.13593.
Rodríguez P, Graña S, Alvarez-León EE, et al. A population-based controlled experiment assessing the epidemiological impact of digital contact tracing. Nat Commun. 2021;12(1). https://doi.org/10.1038/s41467-020-20817-6.
von Wyl V, Höglinger M, Sieber C, et al. Drivers of Acceptance of COVID-19 Proximity Tracing Apps in Switzerland: Panel Survey Analysis. JMIR Public Health Surveill. 2021;7(1): e25701. https://doi.org/10.2196/25701.
Lewis D. Contact-tracing apps help reduce COVID infections, data suggest. Nature. 2021;591(7848):18–9. https://doi.org/10.1038/d41586-021-00451-y.
Pepper C, Reyes-Cruz G, Pena AR, et al. Understanding Trust and Changes in Use After a Year With the NHS COVID-19 Contact Tracing App in the United Kingdom: Longitudinal Mixed Methods Study. J Med Internet Res. 2022;24(10): e40558. https://doi.org/10.2196/40558.
Wymant C, Ferretti L, Tsallis D, et al. The epidemiological impact of the NHS COVID-19 app. Nature. 2021;594(7863):408–12. https://doi.org/10.1038/s41586-021-03606-z.
Gao G, Lang R, Oxoby RJ, et al. Drivers of downloading and reasons for not downloading COVID-19 contact tracing and exposure notification apps: A national cross-sectional survey. PLoS ONE. 2022;17(7): e0269783. https://doi.org/10.1371/journal.pone.0269783.
Oyibo K, Morita PP. The effect of persuasive design on the adoption of exposure notification apps: quantitative study based on COVID alert. JMIR Form Res. 2022;6(9):e34212. https://doi.org/10.2196/34212.
Baumgart DC. Digital advantage in the COVID-19 response: perspective from Canada’s largest integrated digitalized healthcare system. npj Digit Med. 2020;3(1). https://doi.org/10.1038/s41746-020-00326-y.
Blacklow SO, Lisker S, Ng MY, Sarkar U, Lyles C. Usability, inclusivity, and content evaluation of COVID-19 contact tracing apps in the United States. J Am Med Inform Assoc. 2021;28(9):1982–9. https://doi.org/10.1093/jamia/ocab093.
Bair H, Wanger JD, Shah NR. A Brief History of Exposure Notification During the COVID-19 Pandemic in the United States, 2020–2021. Public Health Rep. 2022;137(2_supp):23S-28S. https://doi.org/10.1177/00333549221099533.
Aronoff-Spencer E, Nebeker C, Wenzel AT, et al. Defining key performance indicators for the California COVID-19 exposure notification system (CA Notify). Public Health Rep. 2022;137(2):67S-75S. https://doi.org/10.1177/00333549221129354.
Gellert GA, Kelly SP, Hsiao AL, et al. COVID-19 surge readiness: use cases demonstrating how hospitals leveraged digital identity access management for infection control and pandemic response. BMJ Health & Care Informatics Online. 2022;29(1): e100680. https://doi.org/10.1136/bmjhci-2022-100680.
Chen T, Baseman J, Lober W, et al. WA Notify: the planning and implementation of a Bluetooth exposure notification tool for COVID-19 pandemic response in Washington State. Online J Public Health Inform. 2021;13(1). https://doi.org/10.5210/ojphi.v13i1.1169.
Huang Z, Tay E, Wee D, Guo H, Lim HYF, Chow A. Public Perception of the Use of Digital Contact-Tracing Tools After the COVID-19 Lockdown: Sentiment Analysis and Opinion Mining. JMIR Formative Research. 2022;6(3): e33314. https://doi.org/10.2196/33314.
Rekanar K, Buckley J, Buckley S, et al. Sentiment analysis of user feedback on the HSE contact tracing app. research square platform LLC. 2020. https://doi.org/10.21203/rs.3.rs-96174/v1. Accessed 23 Aug 2023.
Segal CD, Lober WB, Revere D, Lorigan D, Karras BT, Baseman JG. Trading-off privacy and utility: the Washington State experience assessing the performance of a public health digital exposure notification system for coronavirus disease 2019. J Am Med Inform Assoc. 2022;29(12):2050–6. https://doi.org/10.1093/jamia/ocac178.
Ussai S, Pistis M, Missoni E, et al. “Immuni” and the National Health System: Lessons Learnt from the COVID-19 Digital Contact Tracing in Italy. Int J Environ Res Public Health. 2022;19(12):7529. https://doi.org/10.3390/ijerph19127529.
Country classification. In: World Economic Situation and Prospects 2014. UN; 2014:143–150. https://www.un.org/en/development/desa/policy/wesp/wesp_current/2014wesp_country_classification.pdf. Accessed 24 Aug 2023.
Sharma S, Singh G, Sharma R, Jones P, Kraus S, Dwivedi YK. Digital health innovation: exploring adoption of COVID-19 digital contact tracing apps. IEEE Trans Eng Manag. Published online 2022:1–17. https://doi.org/10.1109/tem.2020.3019033/.
Trivedi A, Vasisht D. Digital contact tracing. ACM SIGCOMM Computer Communication Review. 2020;50(4):75–81. https://doi.org/10.1145/3431832.3431841.
Miller JS, Bonacci RA, Lash RR, et al. COVID-19 Case Investigation and Contact Tracing in Central Washington State, June–July 2020. J Community Health. 2021;46(5):918–21. https://doi.org/10.1007/s10900-021-00974-5.
Mbunge E, Fashoto SG, Batani J. COVID-19 Digital Vaccination Certificates and Digital Technologies: Lessons from Digital Contact Tracing Apps. SSRN Electronic Journal Published online. 2021. https://doi.org/10.2139/ssrn.3805803.
Lee T, Lee H. Tracing surveillance and auto-regulation in Singapore: ‘smart’ responses to COVID-19. Media International Australia. 2020;177(1):47–60. https://doi.org/10.1177/1329878x20949545.
Röhrig R, Beißbarth T, König J. German Medical Data Sciences 2021: Digital Medicine: Recognize - Understand - Heal: Proceedings of the Joint Conference of the 66th Annual Meeting of the German Association of Medical Informatics, Biometry, and Epidemiology E.V. (Gmds) and the 13th Annual Meeting of the TMF - Technology, Methods, and Infrastructure for Networked Medical. IOS Press; 2021. https://ebooks.iospress.nl/volume/german-medical-data-sciences-a-learning-healthcare-system-proceedings-of-the-63rd-annual-meeting-of-the-german-association-of-medical-informatics-biometry-and-e. Accessed 30 Oct 2023.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Acknowledgements
We would like to thank Denes Stefler, Aradhna Kaushal, and Emma Beard at the University College London for their guidance on development of topic, methodology, and stakeholder involvement.
Funding
All authors did not receive funding for the creation of this manuscript.
Author information
Authors and Affiliations
Contributions
Nicole Irwin led the study design, conducted search strategy, performed paper screening for abstract and full text review, and carried out data analysis. Dewi Nur Aisyah built the paper concept and supported the development of methodology. Fauziah Mauly Rahman performed paper screening for abstract and full text review, as well as built the first draft of the paper. Logan Manikam validated the study and critically revised the manuscript content. Nicole Irwin had primary responsibility for the final content. All authors read and contributed to reviewing the study data, the manuscript design, and the approval of the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study is a systematic review. We declare that the data collected for this paper do not require ethical approval as no individual data are presented.
Conflict of interest
The authors declare no potential conflicts of interest with respect to the research, authorship and publication of this paper.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Irwin, N., Aisyah, D.N., Rahman, F.M. et al. Digital contact tracing technology in the COVID-19 pandemic: a systematic review. Health Technol. (2024). https://doi.org/10.1007/s12553-024-00857-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12553-024-00857-4