
Abstract
Purpose
Physically demanding activities at the nursing bed are a key factor in the overwork of nursing staff and play a major role in the development of musculoskeletal disorders. The heavy back strain plays a significant part in this. Technical aids such as robotic assistance systems have the potential to minimize this overload during nursing activities. In the present work, we have investigated the relief potential of a supporting robotic assistance system developed in the AdaMeKoR project. An exploratory study design was developed to assess the relief potential of the robotic system for nurses during the care action of repositioning from the supine position to the sitting position at the edge of a nursing bed under kinaesthetic principles.
Methods
The study was conducted in March 2022 with a total of 21 nursing professionals participating. Safety precautions at this stage of the robot’s development made it necessary to use a 40 kg patient simulator instead of having a human act as the patient. Each participant performed the repositioning three times in the conventional manner and three times with the robotic-assistance. The conventional and the robotic-assisted task execution was compared using different perspectives of analysis. From a sensory perspective, ground reaction forces and electromyography data were collected and analyzed. A kinaesthetic perspective was added using 3D-video data which was analyzed by professional kinaesthetics trainers. A third perspective was added by collecting the subjective workload experiences of the participants.
Results
While participants’ self-assessment based on a NASA-TLX questionnaire suggests more of a physical and psychological strain from using the robot, electromyography shows a 24.41% reduction in muscle activity for left back extensors and 7.99% for right back extensors. The kinaesthetic visual inspection of the study participants also allows conclusions to be made that the robot assistance system has a relieving effect when performing the nursing task.
Conclusions
The conducted study suggests that overall the robotic-assistance has the potential of relieving nurses of partial physical exertion during mobilization. However, the different focuses of analysis show varying results in regard to external, i.e. sensor data and expert analysis, compared to internal, i.e. the nurses, perspectives. Going forward, these results have to be further expanded to get more robust analyses and insights on the interdependencies of subjective factors contributing to the experience of workload. In view of the fact that robotics for nursing is still a relatively new field and there are various lessons to be learned regarding the conceptualization of studies and corresponding evaluations, our approach of combining perspectives of analysis allows for a more differentiated view of the subject at hand.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Nursing is an interactional and mostly interactive work, where a cooperative relationship is established which consists of communicational-emotional as well as physical work [1]. While research regarding concrete nursing actions should always consider this complexity, specific problems deserve focused attention. One such issue can be seen in the physical strains nurses have to deal with regularly across most care settings. The prevalence of body ailments among nurses is a well-investigated phenomenon and it is evident that physical demands are reported more often for nurses than for other professions [2, 3]. Compared to other occupational groups, nursing professions experience more days of absence due to illness. In Germany, for example, the main causes among nursing staff in nursing homes are mostly musculoskeletal disorders (24.6%) [4]. A major source of physical strains in nursing comes from actions related to mobilization and transfer processes, which are common tasks performed in nursing [5]. These actions often stress the lumbar region, resulting in low back pain (LBP) as a musculoskeletal disease [6]. This process can be attributed to the high loads experienced during mobilization and transfer of patients. From a physiological point of view, the maximum load that can still be classified as harmless to health is reduced with age [7]. For men, the limit value at age 20 is 5.4 kN and is reduced to a maximum of 2.2 kN by the age of 60 years [7]. For women, the limit is 4.1 kN at age 20 and reduced to 1.8 kN by the age of 60 years [7]. The loads occurring during the most common nursing activities at the nursing bed were biomechanically quantified for the lower back at the transition L5-S1 of the spine. On average, moving a patient (60–80 kg) conventionally to the bed’s head while standing at the bed’s long side leads to a compressive force of 6.7 kN on L5-S1 [8], which exceeds the biomechanical limit and tends to have a damaging effect, leading to chronic LBP in the worst case. Depending on the scenario (limited musculature of the caregiver, high weight of the patient), the effects can be much more severe. These mobilizations have to be performed several times a day.
Next to these direct effects, high physical strains in nursing have far-reaching consequences on an institutional and societal level. For example, it was shown that back pain constitutes a central factor for sick leaves for nurses and also that nurses are affected by issues like disc damages more often than average [9]. Furthermore, high physical demand was shown to be a significant factor for nurses leaving the profession [10].
Combining these factors with the already immense shortage of skilled nurses, the need for action to maintain health is evident. With regard to the reduction of physical strain during patient mobilization, different strategies can be found. On the one hand, some are linked to specific ways of movements [11]. An example of a widely distributed concept is that of kinaesthetics [12]. This concept is based on attentive movement patterns and the self- and situational-awareness of the acting person. On the other hand, there is a great range of devices designed to relieve nurses of the necessity of exerting high physical efforts or corresponding adverse movements, typical examples being lifters or slide boards [13].
With technological advancements in various fields, there also seem to be connectable concepts for mobilization devices for nursing. One of the latest technical areas, which promises innovations in this context is the field of robotics [14]. The underlying idea is that robots, having a degree of autonomous capacity, could support the mobilization process in an overall favourable way by improving the rigid procedures of conventional devices.
Since we focus on physical relief in the caregiving context, we do not provide an overview of developments in social robotics or other assistive robotics, which can also be used for support in nursing care [15]. One of the best-known robots for physical assistance in the care context is the Robot for Interactive Body Assistance (RIBA), with the potential to carry patients weighing up to 60 kg out of bed [16]. The prototype, developed in Japan, is controlled by a tactile interface. Another example is the so-called “Robotic Nursing Assistant” with the potential to lift and carry patients of up to 227 kg [17]. Another assistance system is the piggyback nursing robot, which a patient leans on with his or her chest when sitting at the edge of the bed and is moved into a stable position so that transport is possible [18]. While the systems above all provide physical relief in general, they are all comparable to intelligent patient lifts in their mode of action. The primary focus is on transferring patients out of or into bed; repositioning individual body parts in the care bed is not presented. Only the system called ROBERT comes close to this, but here the focus lies on rehabilitation. This system consists of a lightweight robot on a mobile platform which can be moved to the patient’s bedside and used for physical therapy by running individual trajectories for the patient’s movement therapy [19].
However, physical support through robotic assistance is not only present in nursing. In the industrial context, for example, there are several applications of exoskeletons that have a direct influence on the human body and facilitate work. Work in an industrial context often requires that unhealthy or strenuous postures have to be held for extended periods of time. In such cases, the use of passive exoskeletons can provide measurable relief, for example for the lower [20, 21] or upper extremities [22, 23]. These assistance systems provide direct support for the musculature, thus relieving the user.
In our research we try to fill the identified research gap in nursing care by combining transfer assistance and repositioning support within the nursing bed, especially since the highly stressful forces - as already shown above - mainly occur during the repositioning tasks in the nursing bed.
Our setup, consisting of a nursing bed with an attached robot assistance system and sensors for perception, biosignal and biomechanical analysis [24,25,26], combines the robot system’s support with basic concepts from kinaesthetics to provide physical relief while training the movement sequences at the same time.
The development of robots for nursing is a complex and new field, with various exploratory research to be done. With nursing at its core seen as interactional and relationship work, the idea of implementing robots comes along with a variety of requirements for standards of reasoning, including but not limited to perspectives from nursing, technical and occupational sciences, ethics and legal studies as well as actors from the direct care practice [1, 27]. In addition to an interdisciplinary theoretical discourse accompanying the development process, among fundamental requirements for the legitimacy of (the development of) robotics for nursing are assessments by the care practitioners and a proven effect of its usage [27]. About the application considered here, these latter requirements are current objectives in the development process and frame the central aim of this article. This leads to the following main research questions: (1) To what extent is it possible to identify an objective and/or subjective relief potential in robot-assisted mobilization? In addition, the following sub-question was also formulated: (2) What conclusions can be drawn/lessons can be learned from a multi-perspective assessment of a relief potential for future evaluations?
With this aim, an exploratory study design was developed to assess the ergonomic relief potential of the proposed robot system. The study aimed at the assessment of the physical loads during a conventional mobilization compared to a robotic-supported mobilization. The analysis was based on a data triangulation of three distinct perspectives – sensor data, expert appraisals as well as the self-perception of nurses.
2 Methods
2.1 Data collection: study procedure
The study was conducted over three consecutive days in March 2022 at the Assistance Systems and Medical Device Technology department of the Carl von Ossietzky University of Oldenburg with the participation of the Department of Nursing Science of the University of Osnabrück and the AdaMeKoRFootnote 1 project coordination of Johanniter Unfall-Hilfe.
In detail, each day followed the same structure, split into five main parts. Initially all participants (nurses - for more information see sample and results) were given a theoretical input about the project as well as the study design and the schedule for the day. Afterwards, the attendees participated in a kinaesthetics course, led by two professional kinaesthetics trainers. Here, the participants learned theoretical and practical input about the basics of kinaesthetics and the mobilization process with a focus on the tasks to be performed in the subsequent tests in the care laboratory (see Fig. 1) with different sensor system explained in more detail in the “Data Collection: Instruments” subsection [28]. Specifically, this task was to mobilize a patient simulator weighing approximately 40 kg from the supine position in the middle of the bed to the edge of the bed into a sitting position. Next, the participants successively performed three recorded conventional mobilizations of the patient simulator. Afterwards, each study participant was instructed to fill out a paper-based assessment (NASA-TLX - for more information see Data Collection: Instruments) about their subjective workload during the mobilization. Following a break, the participants received a second kinaesthetics course. This time the focus was on performing the same mobilization process but with the support of a second person that would imitate the movements the robot would make. Subsequently, each participant performed a second mobilization, this time around with the support of a lightweight robot assistance system (KUKA LBR iiwa7 R800) as in Fig. 1. After a demonstration of the robotic movements, each participant again performed three recorded mobilizations of the patient simulator. Afterwards, the subjective work load assessment was again filled out for this second performance. When all participants had finished recording each day was closed with a short discussion round including everyone involved.

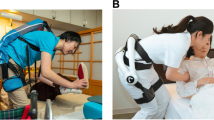
Overview of the laboratory environment with hardware used to conduct the study described in this paper. A 40 kg weighing patient simulator in a nursing care bed (A) is used for the activity to be examined. A lightweight robot arm system (model KUKA LBR iiwa7 R800) is attached to the bed and used for the robot-supported variant of the study task (B). The scene is detected by two 3D depth cameras (C). A force measuring plate (D) is used to measure the ground reaction forces during the task. The robot is controlled by a computer setup with visualization (E). The muscle activity of the study participants is measured with an electromyograph (F) during the task performance. A modified padded end effector is used for the interaction between patient simulator and robot (G)
2.2 Sample
Nurses from all over Germany were approached and recruited for study participation via digital recruitment. Two criteria were set as obligatory for inclusion: participants had to (1) be active registered nurses and (2) agree to the terms and conditions of the study and data management (see below). Work experience as well as prior experience with kinaesthetics were set as desirable but not necessary.
2.3 Mobilization task
During the task execution with the robot’s help, the study participants first place the right leg of the patient simulator and then get ready to move the simulator into the stable lateral position. The study participant prepares the patient simulator to get in contact with the light weight robot’s end effector (first phase). As they do, the lightweight robot arm moves to the patient simulator’s shoulder and cooperatively applies a force so that support is provided when turning (second phase). The robot stops with the patient simulator in a stable lateral lying position and remains there, stabilizing the patient simulator so that the study participant can move the simulator’s legs to the correct position without difficulty to perform the final step of the movement. (third phase) After preparation, the final support movement is then initiated, during which the robot stabilizes the patient simulator’s back as it is raised, thus serving as a support to the rear. Once the patient simulator is sitting upright and stabilized by the robot at the edge of the bed, the process is complete (fourth phase). During the mobilization task without the robot, the first phase is excluded because there is no contact between robot and patient simulator.
2.4 Data collection: instruments
Multiple sensors (force measuring plate, 3D depth cameras and a surface electromyograph) as well as a paper-based questionnaire were used to evaluate potential physical unloading and to measure the subjective physical and psychological stress.
With regard to the sensors, there are several specifications to be made. First, electromyography (EMG) sensors from the manufacturer Delsys were used for the analysis of muscle activity (model Trigno Avanti). This sensor is wireless and can record EMG signals at a maximum frequency of 4370 Hz. In addition, the sensors have built-in inertial measurement units (IMUs), which means that the acceleration and position of the sensors used can also be recorded, although the sampling rates here are lower than for the EMG signals. Two sensors were attached to the back extensor (erector spinae left, ESL, and erector spinae right, ESR) of each study participant prior to performing the actual recordings. Before the actual sensor attachments, the skin was prepared, i.e. the region was shaved, degreased with alcohol and then lightly abraded to maximize the signal transmission capability [29].
Second, a force measuring plate (FMP) was used as a further sensor channel for the evaluation. This allows the detection of ground reaction forces in order to record the forces dissipated through the ground. In this way, movements and loads can be compared between the individual movement cycles. The AccuPower model from the AMTI company was used, which can record forces and moments in all three axes at a frequency of 200 Hz. The study participants stood on the FMP positioned in front of the nursing bed while performing the selected movement. At the beginning, end and between each trial the participants had to jump on the FMP to make synchronisation between all sensors possible.
In addition, two 3D depth cameras were positioned behind the nursing bed during the study to capture the movement of the study participants while allowing synchronization of all sensor channels during processing. The cameras captured the scene at 30 frames per second.
Finally, the robot assistance system itself should be mentioned. The assistance system is a modified care bed equipped with lightweight robot manipulators of the model KUKA LBR iiwa7 R800. Each robot stands on a base socket, which was attached to the bed frame and can also be repositioned along the bed frame. Since grasping actions are not suited for patient handling in the nursing care context, only pushing support movements are to be performed. For that, a modified robot end effector with a palm-sized polyethylene attachment was developed, allowing for padded support. A basic impedance controller is used, which provides a compliant behaviour. For the movement a pose controller is utilized. During the robot-assisted motions, the robot travels along a pre-defined trajectory with support points, but can yield to some degree due to the underlying impedance controller. The movement between these support points is triggered by a human operator.
The system’s hardware infrastructure has been discussed previously [30] in detail but will be outlined in the following. Each KUKA LBR iiwa7 R800 comes with a control unit, which is in our case connected to a computer running the Robot Operating System [31] via the Fast Robot Interface. This computer is connected to the main computer, which is running a simulated environment in Unity [32] based on the real surroundings recorded by several connected sensors (e.g. Azure Kinect 3D depth cameras for body tracking data, EMG sensors for muscle activity and the force torque sensor data of the robots). Within this environment, pose commands for movement are sent back to the robot control unit based on the sensor data and decision making. The inverse kinematics for the robot movement are solved via BioIK [33]. In general, the robot’s trajectories are either predefined based on model behavior or manually adjusted by the user through hand guiding. For the study, the contact points between the robot and the patient simulator were discussed in advance with the kinaesthetics experts in preparation for the workshops introducing the study participants to the subject matter.
As already mentioned, next to the sensor systems a questionnaire for assessing the participants subjective work load was used. For this we utilized the NASA Task Load Index (NASA-TLX), which since its development in 1988 has already been used in various domains and for heterogenous activities [34]. The NASA-TLX itself consists of six subscales with each focusing on a different aspect of work load. The subscales include „Mental Demands”, „Physicals Demands”, „Temporal Demands”, „Effort”, „Performance” and „Frustration”, each of which has to be rated. Here, each scale ranged from 0 (i. e. low demand or good performance) up to 10 (i. e. high demand or bad performance), with 0.25 steps being possible.
2.5 Data analysis
For the analysis, three distinct perspectives of analysis were used, namely sensor data, expert appraisals and the self-perception of the study participants. (1) The first part of the data analysis in the study dealt with the actual data acquisition during the performance of the nursing activity of repositioning at the nursing bed. For this purpose, the ground reaction forces, robot data, muscle activities and bodytracking data were recorded during the execution of the nursing activity. All data were manually synchronized by recorded jumps on the FMP, as this jump can be seen in all human-related sensor data. The robot data were synchronized with the initial patient simulator contact, which is visible in the camera data. The raw EMG sensor data for ESL and ESR recorded at 1259 Hz were processed by filtering. First, a 4th degree band-pass filter with a high-band frequency of 20 Hz and a low-band frequency of 450 Hz was applied to the data to minimize the high frequency noise. Afterwards, a low pass filter with a frequency of 6 Hz was applied. The cleaned signal was used for the following comparisons. For the FMP data, the raw data was used. However, the weight of the subjects was subtracted in the z-direction in each case, so that there is no offset in the data. For the video and depth image data, the body tracking model from Microsoft was used to capture the posture. The force-moment sensor data recorded by the robot was also analyzed as raw data and not further smoothed since the noise was minimal. For the comparison of the data, on the one hand, the subjects were considered individually in the comparison between conventional and robot-assisted task execution, and the individual results of the subjects represent an averaging of the successful trials. Additionally, an averaging of the entire data across all subjects was determined and used for the overall comparison. It should also be mentioned that the individual axes of the sensor channels were considered individually, so that for the FMP a division into x-, y- and z-axis was performed. The entirety of the data was then used to quantify the physical relief that might occur.
(2) The second part of the analysis aimed at the comparison of the subjectively perceived stress levels of the participants. For this step, the NASA-TLX scales were analyzed using descriptive statistics in Windows Excel. First, the data for each participant was digitalized for both the assessment of the conventional as well as the robot-supported mobilization. Afterwards, the results were grouped corresponding to each mobilization process, whereby both the NASA-TLX overall result and the subscales were assessed. For the analysis of the overall assessment the values of the six subscales were added so that it could range from 0 (no/minimal stress) to 60 (maximum stress). The split analysis of specific subscales and the overall assessment is in accordance with the work of Hart [34].
(3) The third part of the analysis aimed at an external assessment from an expert point of view. This subanalysis was primarily performed by two professional kinaesthetics trainers using the 3D-video data. To set up a basis for this, a heuristic evaluation form was designed in cooperation of the main authors and the kinaesthetics trainers. The first part of this form consisted of a rating of the observed physical stress from one to ten, with ten being maximum physical stress. The second part was based on a kinaesthetics interaction assessment – which itself could not be used in its entirety because of the mobilization of a simulator. This second part consisted of notes on particularities in (a) the intrinsic movement of the participants, (b) the handling of the patient simulator including observations regarding the human-robot interaction when applicable and (c) other observations. In the process, the two experts graded all individual mobilizations with and without the robot aid along the aforementioned heuristic. Initially, this was done separately by the experts. Afterwards, these results were compared and merged. In cases of diverging results in the observation, a consensus was made through discussion. The resulting data was then analyzed using descriptive statistics in Windows Excel.
In total, this three-step process allowed to get distinct analytical perspectives of the physical burden during the mobilization process and the potential stress reduction from the robot aid.
3 Results
3.1 General characteristics
In total 21 registered nurses participated in the study, with 16 female and 5 male participants. The average age of the participants were 49.3 years (21–62 years) and had 25.9 years work experience in nursing (1–43 years). The participants’ average height was at 1.72 m (1.58–1.92 m) and the average weight at 78.04 kg (50–125 kg). Regarding prior kinaesthetic experience, 11 participants indicated experience beyond a basic course, 5 stated to have done a basic course and 5 stated to have almost no experience with the concept.
While the total of 21 participated in the study, not all data were usable for the evaluation. Due to technical difficulties, three datasets of participants performing the robot-supported mobilization could not be recorded. The analyzed data had to be further reduced by excluding trials where human-robot cooperation was not executed in a sufficient way, leading to a final amount of 15 evaluable study participant sensor datasets and 54 individual 3D-videos for the experts’ analysis.
3.2 Sensor data
In the following, the sensor data recorded during the study are described and visualized. In the considered movement of placing the patient simulator on the edge of the bed, we put a focus on the last movement phase, namely the movement of raising from the side-length to the sitting position. The synchronized time series data for the movement with and without robot support for one study participant is presented in Fig. 2. In addition, the structure and sequence of the scenario can be also seen.

The plots show the exemplary sensors result plots of a study participant during one conventional (C) and one robot-supported (RS) trial for all three or four phases shown above. The yellow phase shows the time for the docking of the end effector. In the blue phase, the patient simulator is brought from the supine to the lateral position. In the red phase, the legs are prepared. In the green phase, the raising process from the lateral position to the seated position takes place. The ground reaction forces of the force measuring plate (FMP) are on the top, the muscle activity (EMG) of the lower back extensor (ESR, ESL) are shown in the middle and the robot-supported trial also provides robot force data depicted on the bottom. During robot support, lower sensor values for the ground reaction forces and muscle activity were registered
The figure shows the exemplary sensor data of one study participant for one complete repositioning process in two different variations, namely the conventional (left) and the robot-supported variant (right). The movement process itself was divided into different phases, which are visualized by different background colors. The yellow area spans the time period where the study participant slightly lifted the torso of the patient simulator to allow the robot to dock. This phase is only present as the first phase in the measurements with the robot. The blue phase shows the repositioning from the supine to the lateral position of the patient simulator. Further on, the red phase shows the process of preparing the patient simulator for the final movement, e.g. by putting the legs into the correct position. In the green and final phase, the patient simulator was positioned from the stable lateral position to the upright sitting position at the edge of the bed, completing the process.
In Fig. 3, the FMP and EMG results of all study participants are visualized based on the recorded data in the aforementioned green phase. These bar plots show the mean and standard deviation of the performed trials for all study participants (S1 – S15) and for both variations, namely the conventional patient simulator repositioning (red) and the repositioning supported by the robot (blue). For the FMP, the ground reaction forces (GRF) are shown for each individual axis in the three upper graphs. The orientation of the axis is shown in Fig. 1.
For the FMP data, an average value of -10.62 N with a standard deviation of 25.52 N was measured for the x-axis during conventional performance. For the y-axis, the value is -32.96 N with a standard deviation of 32.95 N. On the z-axis, the average value is 25.53 N with a standard deviation of 41.45 N. For the robot-assisted variant, in turn, the x-axis force value shows a value of 16.98 N with a standard deviation of 18.30 N, the y-axis a value of -27.19 N with a standard deviation of 26.57 N, and finally the z-axis an average value of 26.01 N with a standard deviation of 30.02 N.
The EMG results show the results for each individual muscle, which are ESR and ESL in this context. In addition, the average over all participants for each execution variant is also shown.
During the conventional execution, the EMG showed an average value of 17.2 µV for the muscular load of the ESL with a standard deviation of 8.9 µV. For the muscle ESR, in turn, the average value was 7.5 µV with a standard deviation of 3.9 µV. For the robot-assisted variant, the average value for the muscle ESL was 13.0 µV with a standard deviation of 7.0 µV. For the ESL muscle, the value was 6.9 µV with a standard deviation of 2.7 µV.

This figure visualizes the results of all study participants where the human-robot cooperation succeeded during the task of repositioning the patient simulator to the bed’s edge. The ground reaction force results of the force measuring plate (FMP GRF) for all three axes (x, y, z) and the lower back extensor’s muscle activity (EMG ESR & EMG ESL) are shown individually and also as an overall average value. Both mean and standard deviation are displayed
3.3 Questionnaire results
In total, 21 NASA-TLX questionnaire for the conventional mobilization process and 17 scales for the mobilization with the robot support were filled out, the 4 remaining questionnaires were incomplete and thus could not be used for the overall analysis. The overview including both assessments is depicted in Table 1. For the conventional mobilization the mean total score was 16.39 with a standard deviation of 6.18. The highest subscale score was for the “Perceived Performance” with a mean of 3.75 and a standard deviation of 2.04, while the lowest score was for “Mental Demands” with a mean of 1.64 with a standard deviation of 1.38. In regard to the subscales associated with physical activity, the mean score for the subscale “Physical Demands” was at 3.14 with a standard deviation of 1.64 and for the subscale “Effort” at 3.36 with a standard deviation of 1.71.
Looking at the results regarding the robot-supported mobilization, the mean total score was at 21.24 with a standard deviation of 8.26. Again, the highest and lowest subscale scores were for the “Perceived Performance” with a mean of 4.66 with a standard deviation of 1.93 and “Mental Demands” with a mean of 2.4 with a standard deviation of 1.34. The mean score for the “Physical Demands” was at 3.32 with a standard deviation of 2.05 and at 3.93 with a standard deviation of 2 for the “Effort” subscale.
3.4 Kinaesthetics analysis
A total of 63 videos of all 21 participants’ conventional mobilizations and 54 videos of 17 participants’ robot-supported mobilizations were assessed by the kinaesthetics experts and the resulting data were analyzed by the main authors. The videos were captured by the 3D depth camera system used during the study. The kinaesthetics experts visually assessed the physical exertion of the study participants based on the camera footage and their experience. Similar to the NASA-TLX questionnaire used, the number 0 was classified as low physical load and the number 10 as high physical load. The appraisal of the conventional process showed a mean value of 3.92 with a standard deviation of 0.98, a median of 4, a minimum of 2 and a maximum of 7. The robot-supported mobilization on the other hand showed a mean of 2.67 with a standard deviation of 1.2, a median of 3, a minimum of 1 and a maximum of 6. Looking at the kinaesthetics interaction assessment, various observations regarding the manner of as well as the success of the human-robot-interaction could be made. One theme emerging from this appraisal is the importance of temporal coordination. Both cases with the robot acting too fast as well as the participants beginning the movement too quickly were observed, which resulted in non-optimal usage of the support and consequently a higher physical stress rating was given. Furthermore, cases of non-optimal interactions resulting from the positioning of the end effector could be identified. Another observation was made in regard to the way the robot support was used respectively. The participants adapted their movements. Here, different approaches could be identified, where some participants mainly used the robot as a static support during the lateral positioning of the simulator, which gave them time to take the legs out of the bed, while others also managed to use the robot dynamically during the sitting up motion.
4 Discussion
The results of this study show important implications regarding the potential reduction of physical load in the field of nursing care by the usage of a supporting robot system paired with basics of the kinaesthetics concept in mobilization processes in nursing. Comparing the individual results, it is noticeable that the mobilization processes were assessed differently by the external (i.e. sensor-based and experts observations) compared to the internal (i.e. subjective stress experience) points of view. The sensor-based results show a stress reduction in both the EMG data as well as the average peak forces due to the reduced standard deviation during the robot-supported mobilization. This is affirmed by the kinaesthetic experts’ results, which also depict that the physical stress during the mobilization with the robot-support is considered to be less than during the conventional mobilization process. Whereas, the appraisals of the participants differ from these results as the respective scales show that the robot-supported mobilization process, while itself not indicating excessive load, was assessed with a higher subjective stress level in all regards in comparison to the conventional mobilization process. Looking at these results, it is important to note the focus of the individual assessments. While the external appraisals focus on conclusions about the observed physical effort, the NASA-TLX scale includes factors, which can only be assessed by the performing individuals. As already mentioned above, it is in line with the NASA-TLX creators to look at the subscales, which in this case allows for a direct comparison of the results of the sensor-based and experts assessments with the subscale of “Physical Demands”. Interestingly, this subscale shows the lowest difference in mean values, with just a slight increase from the conventional to the robot-supported mobilization (see Table 1). Considering the shown physical stress relief in the external assessments, it would be relevant to check whether the subjective assessment of the physical exertion correlates with other factors of the NASA-TLX like temporal demands or frustration, where the gap between the conventional and robot-supported mobilization was clearly greater appraised. This would require a larger sample size.
Additionally, FMP and EMG data were recorded during the mobilization process. A clear evaluation of the FMP results in the x- and y-axis direction is relatively difficult to interpret, since it is not possible to directly speak of a physical unloading here because of a missing reference such as gravity in the z-axis. What can be said directly, however, is that the movement behaviour of the study participants changed as a result of using the robot. In the x-axis, for example, there was a shift from negative to positive x-values on average (see Fig. 3), with a reduction in standard deviation. This can be explained by the fact that the robot acts as a support on the opposite side, resulting in a counterforce away from the direction of the bed. There are no significant changes in the forces along the y-direction, as the motion in both conventional and robot-assisted variants do not differ much from each other, although the reduced standard deviation would be worth mentioning. For the values measured in the z-direction, the values are similar on average, although this is also very dependent on the individual subjects. While some subjects experience a strong relief in the z-direction, no negative or significant changes can be seen in other subjects. A positive aspect is that the maximum force peaks were reduced by the robot assistance, which according to the literature has a strong influence on the health of the lumbosacral disc. The result is most likely not as critical as it would be with a normal or overweight patient due to the relatively light patient simulator with 40 kg because the robot could otherwise expend much more force and has not come close to its force limits. This fact made the difference between the conventional and the robot-supported trials smaller.
In contrast to the results of the ground force plate, the differences in muscle activity are more visible. On average, the left part of the back extensor (ESL) was activated 24.41% less during the robot-assisted variant, while the right part (ESR) was activated 7.99% less. Despite the results of the FMP, a relief can be observed on the muscular level during the performed movements in the back-extensor area with robot assistance. It is also possible that a shift in muscle activity in the body has taken place due to the slight adjustment of the movement pattern and that the leg muscles are used more, which is also a positive result in principle for the overall ergonomics.
In summary, from a muscular point of view, a relief could be observed in the area of the back extensor during robot-assisted execution of the repositioning task. From a kinaesthetic perspective, the robot can be integrated into the movement process as a stabilizing element, although the concrete interaction methodology still needs to be defined. Moreover, it is a consideration that the robot should analyze the mobilization process and offer the most reasonable support variant depending on the current situation. This situational awareness of the robot must be addressed technically in future work.
In addition to this studies main focus of exploring the physical relief potential of the robotic system, it is particularly relevant in research contexts to critically reflect on the potential effects of using this and other corresponding systems against a broader background. Since corresponding reflections require a high degree of complexity and thus dedicated attention, the topic can only be touched upon here. From a nursing science perspective, a central aspect of reflection is the question of whether robotics is conducive to the delivery of “good care” or whether it hinders or even prevents it [1]. In recent years, there have been different approaches to corresponding reflection frameworks (e.g. [35,36,37]). Exemplary arguments in the discourse can be found on the one hand on the basis of correspondingly negative scenarios of a possible substitution of human care [38]. On the other hand, there are also conceptions that present the competent and reflective use of assistive technologies as an explicitly caring characteristic of nurses [39].
5 Limitations
Our study has to be critically reflected regarding a couple of aspects. First, a total of 21 participants is a relatively small sample size. The COVID-19 situation and corresponding regulations in Germany (contact restrictions) have complicated the acquisition process in both the institutional preparations of an on-site testing as well as the availability of nurses, as the working conditions in nursing practice are even more challenging than usually. However, our study was deliberately designed under an exploratory paradigm, in which different methods of data collection and analysis were combined as to not only get preliminary findings about the potential of ergonomic stress relief but to also gain insights about our approach of data triangulation in the evaluation of a robot-support system for nursing. With this in mind, the sample size allowed us to create a balance between pragmatically manageable amounts of data and analysis at an appropriate depth while also leaving room for lessons to be learned about the study setup. Furthermore, the process of mobilising a patient simulator of about 40 kg rather than a real person and the limited mobility of the patient simulator compared to a real human must be noted as limitations. In addition to the limitations this creates regarding the closeness to real physiological conditions (e.g. the weight and mobility of real patients), it also is a comprehensive reduction of the interactional part of nursing. These factors also remain true, but the handling of a patient simulator was a necessary safety precaution at this stage of the robot’s development. Nonetheless, the results have to be viewed in light of this reduction of the real nursing processes. Lastly, the exclusion of some datasets has to be mentioned. From a technical perspective, a synchronous operation between the robot and the caregiver is essential. As some instances of failed human-robot-interactions only became clear in the analysis of the video data, it was necessary to exclude some datasets of participants to get a clearer result of the potential of the robotic support. The fact that the interaction did not work out as intended in some cases is a motivation for further developments. Especially the optimization of the interaction methods as well as the situational awareness of the robot system are planned for future work.
6 Conclusion
Robotics for nursing is a relatively new and complex interdisciplinary field in which there are still various lessons to be learned in terms of both the concrete development of the technology as well as the conceptualisation of studies for corresponding evaluations. Researchers are obliged to check the efficacy and usefulness of the robot systems from different perspectives while they are still under development. In this article, an approach to integrate these factors into an exploratory study design was made. With respect to the perspectives of both nurses themselves as well as experts in the field of mobilization next to sensor-based data, we chose to approach the question of the potential stress relief of a robot system with a multi-perspective data collection and analysis. Referring to our main research question, it can be noted, that from an external point of view, the robot use case is able to achieve a reduction of the physical stress in this particular mobilization process. With regard to physical support, the results of the present research coincide with the results of domain-unrelated support systems in that a positive effect is evident with regard to user-centered physical relief. But also, the internal (i. e. the nurses’) point of view, with the indications of a somewhat higher load, must be taken seriously. Subsequently, a detailed analysis of the subjective stress experience shows to be beneficial as it can provide information about individual factors impacting the assessment. The approach of integrating expert perspectives into the analysis proved to be a valuable addition in the evaluation of the robot use case, as this allowed for a genuinely professional assessment and expansion of the interpretation of the other datasets. The most prominent argument here being that the slowing down of the mobilization process can be attributed positively as it allows for more attentive actions. This aspect becomes even more interesting in light of the discussion of the increasingly efficiency-driven caring contexts. While it is not the intention to suggest that robotics is an instrument for averting this trend, findings of this kind might give impulses for the broader discourse of pros and cons of robotics in nursing. Concluding, our findings show indications of a physical stress relief in a robot-supported mobilization, while it has also to be pointed out, that the way of assessing data in this context can vary between external and internal perceptions. The chosen procedure of data triangulation proved to be valuable as it allowed for the combination of not only sensor-based but also multi-perspective subjective and experts assessments of the mobilization process. A next step will be to integrate the lessons learned into an adapted study design in which a larger sample size has to validate the implications found here.
Notes
“An Adaptive Multi-Component Robot System for Nursing Care” (Ein adaptives Mehrkomponenten-Robotersystem für die Pflege). For more information see http://adamekor.de/ and https://www.pflege-und-robotik.de/adamekor/.
References
Hülsken-Giesler M, Remmers H. Robotische Systeme für die Pflege: Potenziale Und Grenzen Autonomer Assistenzsysteme aus pflegewissenschaftlicher sicht. Göttingen: V&R unipress; 2020.
Schmucker R. Arbeitsbedingungen in Pflegeberufen: Ergebnisse Einer Sonderauswertung Der Beschäftigtenbefragung Zum DGB-Index Gute Arbeit. In: Jacobs K, Kuhlmey A, Greß S, Klauber J, Schwinger A, editors. Pflege-Report 2019. Mehr Personal in Der Langzeitpflege – Aber woher? Berlin, Germany: Springer; 2020. pp. 49–60.
Melzer M. Arbeitssituation Und Gesundheit Beruflich Pflegender. In: BAuA, editor. Stressreport Deutschland 2019: Psychische Anforderungen, Ressourcen Und Befinden. Dortmund, Germany: Bundesanstalt für Arbeitsschutz und Arbeitsmedizin; 2020. pp. 136–45.
Rothgang H, Müller R. Barmer Pflegereport 2020. Berlin, Germany: BARMER; 2020.
Yassi A, Lockhart K. Work-relatedness of low back pain in nursing personnel: a systematic review. Int J Occup Environ Health. 2013;19(3):223–44.
Yoshimoto T, Oka H, Fujii T, Kawamata K, Kokaze A, Koyama Y, Matsudaira K. Survey on chronic disabling low back pain among care workers at nursing care facilities: a multicenter collaborative cross-sectional study. J Pain Res. 2019;12:1025–32.
Jäger M. „Revidierte Dortmunder Richtwerte-Empfehlungen Zur Maximalbelastung Des Unteren Rückens Beim Handhaben Von Lasten auf basis Der Kompressionsfestigkeit Isolierter Wirbelsäulensegmente. editor. Arbeit interdisziplinär analysieren – bewerten –gestalten: 65. Kongress Der Gesellschaft für Arbeitswissenschaft. Dresden, Germany: GfA-Press; 2019. n.pag. Gesellschaft für Arbeitswissenschaft.
Jäger M, Jordan C, Theilmeier A, Wortmann N, Kuhn S, Nienhaus A, Luttmann A. Analyse Der Lumbalbelastung Beim Manuellen Bewegen Von Patienten Zur Prävention biomechanischer Überlastungen Von Beschäftigten Im Gesundheitswesen. Zentralblatt für Arbeitsmedizin. Arbeitsschutz Und Ergonomie. 2014;64(2):98–112. https://doi.org/10.1007/s40664-013-0010-4.
Drupp M, Meyer M. Belastungen Und Arbeitsbedingungen Bei Pflegeberufen-Arbeitsunfähigkeitsdaten und ihre Nutzung Im Rahmen eines Betrieblichen Gesundheitsmanagements. In: Jacobs K, Kuhlmey A, Greß S, Klauber J, Schwinger A, editors. Pflege-Report 2019. Mehr Personal in Der Langzeitpflege – Aber woher? Berlin, Germany: Springer; 2020. pp. 23–47.
Mazurenko O, Gupte G, Shan G. Analyzing US nurse turnover: are nurses leaving their jobs or the profession itself. J Hosp Adm. 2015;4(4):48–56.
Brinkmann A, Kowalski C, Lau S, Meyer O, Diekmann R, Hein A. Chair squat performance as a potential predictor for nurses’ physical capabilities in ergonomic patient transfers. Sci Rep. 2023;13:2825. https://doi.org/10.1038/s41598-023-29968-0.
Gattinger H. Development and evaluation of two instruments to assess nursing staff’s competence in mobility care based on kinaesthetics. 2017. https://www.utupub.fi/bitstream/handle/10024/144030/AnnalesD1310Gattinger.pdf?sequence=1&isAllowed=y. Accessed 8 March 2023.
Berman A, Snyder SJ, Levett-Jones T, Burton P, Harvey N. Skills in clinical nursing. Melbourne, Vic.: Pearson Australia; 2017.
Brinkmann A, Fifelski-von Böhlen C, Lau S, Meyer O, Diekmann R, Hein A. Providing physical relief for nurses by Collaborative Robotics. Sci Rep. 2022;12:8644. https://doi.org/10.1038/s41598-022-12632-4.
Nieto Agraz C, Pfingsthorn M, Gliesche P, Eichelberg M, Hein A. A survey of robotic systems for nursing care. Frontiers in Robotics and AI. 2022;(9). https://www.frontiersin.org/articles/10.3389/frobt.2022.832248/full. Accessed 8 March 2023.
Mukai T, Hirano S, Nakashima H et al. Development of a nursing-care assistant robot RIBA that can lift a human in its arms. In: 2010 IEEE/RSJ International Conference on Intelligent Robots and Systems. Taipei, Taiwan; 2010:5996–6001.
Ding J, Lim Y-J, Solano M et al. Giving patients a lift-the robotic nursing assistant (RoNA). In: 2014 IEEE International Conference on Technologies for Practical Robot Applications (TePRA). Woburn, MA, USA; 2014:1–5.
Liu Y, Guo S, Yin Y, Jiang Z, Liu T. Design and compliant control of a piggyback transfer robot. J Mech Rob. 2022;14(3).
Chan A. A technical report on a novel robotic lower limb rehabilitation device - is ROBERT® a cost-effective solution for rehabilitation in Hong Kong? Hong Kong Physiotherapy Journal. 2022;42(2):75–80.
Luger T, Seibt R, Cobb TJ, Rieger MA, Steinhilber B. Influence of a passive lower-limb exoskeleton during simulated industrial work tasks on physical load, upper body posture, postural control and discomfort. Appl Ergon. 2019;80:152–60.
Siedl SM, Mara M. Exoskeleton acceptance and its relationship to self-efficacy enhancement, perceived usefulness, and physical relief: a field study among logistics workers. Wearable Technol. 2021;2:e10.
Schroeter F, Kähler ST, Yao Z, Jacobsen T, Weidner R. Cognitive effects of Physical Support systems: a study of resulting effects for tasks at and above Head Level using exoskeletons. In: Schüppstuhl T, Tracht K, Henrich D, editors. Annals of Scientific Society for Assembly, Handling and Industrial Robotics. Berlin, Heidelberg: Springer; 2020. pp. 149–59.
Ralfs L, Peck T, Weidner R. Laboratory-based evaluation of exoskeletons in an overhead Assembly Task. In: Schüppstuhl T, Tracht K, Fleischer J, editors. Annals of Scientific Society for Assembly, Handling and Industrial Robotics 2022. Cham: Springer; 2023. pp. 203–14.
Kowalski C, Brinkmann A, Fifelski-von Böhlen C, Gleiche P, Hein A. A rule-based robotic assistance system providing physical relief for nurses during repositioning tasks at the Care Bed. Int J Intell Rob Appl. 2022. https://doi.org/10.1007/s41315-022-00266-8.
Fifelski-von Böhlen C, Brinkmann A, Fudickar S, Hellmers S, Hein A. Technology-based education and training system for nursing professionals. Springer Commun Comput Inform Sci. 2022. https://doi.org/10.1007/978-3-031-20664-1_7.
Hellmers S, Brinkmann A, Fifelski-von Böhlen C, Lau S, Diekmann R, Hein A. Posture and mechanical load Assessment during Patient transfers. SN Comput Sci. 2022. https://doi.org/10.1007/s42979-022-01263-1.
Maibaum A, Bischof A, Hergesell J, Lipp B. A critique of robotics in health care. AI Soc. 2022;37:467–77.
Brinkmann A, Fifelski C, Lau S, Kowalski C, Meyer O, Diekmann R, Isken M, Fudickar S, Hein A. The AAL/Care Laboratory-a healthcare prevention system for caregivers. Nanomaterials and Energy. 2020;9(1):27–38.
Hermens HJ, Freriks B, Merletti R, et al. European recommendations for surface electromyography. Roessingh Res Dev. 1999;8(2):13–54.
Kowalski C, Brinkmann A, Hellmers S, Fifelski-von Böhlen C, Hein A. Comparison of a VR-based and a rule-based robot control method for assistance in a physical human-robot collaboration scenario. In: 2022 31st IEEE International Conference on Robot and Human Interactive Communication (RO-MAN); 2022:722–728.
Quigley M, Gerkey B, Conley K, Faust J, Foote T, Leibs J, Berger E, Wheeler R, Ng A. ROS: an open-source Robot Operating System. ICRA workshop on open source software. Japan: Kobe; 2009. p. 5.
Juliani A, Berges VP, Teng E, Cohen A, Harper J, Elion C, Goy C, Gao Y, Henry H, Mattar M, Lange D. Unity: A general platform for intelligent agents. https://arxiv.org/pdf/1809.02627.pdf. Accessed 8 March 2023.
Starke S, Hendrich N, Zhang J. Memetic evolution for generic full-body inverse kinematics in robotics and animation. IEEE Trans Evol Comput. 2018;23(3):406–20.
Hart SG. NASA-task load index (NASA-TLX); 20 years later. Proceedings of the Human Factors and Ergonomics Society Annual Meeting. 2006;50(9):904–908.
van Wynsberghe A. Designing robots for care: care centered value-sensitive design. Sci Eng Ethics. 2013;19(2):407–33.
Coeckelbergh M. Artificial agents, good care, and modernity. Theor Med Bioeth. 2015;36(4):265–77.
Seefeldt D, Hülsken-Giesler M. Pflegeethik Und Robotik in Der Pflege. In: Monteverde S, editor. Handbuch Pflegeethik – Ethisch denken und handeln in den Praxisfeldern Der Pflege. Stuttgart: Kohlhammer; 2020. pp. 217–84.
Sharkey A, Sharkey N. Granny and the robots: ethical issues in robot care for the elderly. Ethics Inf Technol. 2012;14(1):27–40.
Locsin RC. Technological competency as caring in nursing: a model for practice. Indianapolis: Sigma Theta Tau International Honor Society of Nursing; 2005.
Acknowledgements
This work was funded by the German Ministry for Education and Research (BMBF) within the research project AdaMeKoR (grant 16SV8531).
The authors have disclosed that they have no significant relationships with, or financial interest in, any commercial companies pertaining to this article.
Funding
This work was funded by the German Ministry for Education and Research (BMBF) within the research project AdaMeKoR (grant 16SV8531).
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Jonathan Levin Behrens, Christian Kowalski, Anna Brinkmann, Maren Asmussen-Clausen and Karina Jürgensen. The first draft of the manuscript was written by Jonathan Levin Behrens and Christian Kowalski. All authors commented on previous versions of the manuscript and made substantial contributions. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. This study design was approved by the Commission for Research Impact Assessment and Ethics of the Carl von Ossietzky University of Oldenburg (Drs.EK/2021/113).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent to publish
The authors affirm that human research participants provided informed consent for publication of the images in Fig. 2.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Behrens, J.L., Kowalski, C., Brinkmann, A. et al. Physical relief potential through robot-assisted mobilization in nursing care: an exploratory study. Health Technol. 13, 1011–1023 (2023). https://doi.org/10.1007/s12553-023-00795-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12553-023-00795-7